Article Text

Statistics from Altmetric.com
P211 SAFETY AND TOLERANCE OF NEBULISED ADC4022 (LOW-DOSE THEOPHYLLINE) IN HEALTHY VOLUNTEERS AND COPD PATIENTS
S. Snape, J. C. Fox, M. F. Fitzgerald, N. J. C. Snell. Argenta Discovery Ltd, Harlow, UK
Background Chronic obstructive pulmonary disease (COPD) and severe asthma are considered to be relatively corticosteroid-resistant; this is hypothesised to be due to reduced histone deacetylase (HDAC) activity which, in preclinical studies, can be upregulated by low-dose theophylline.1 We have administered nebulised low-dose theophylline (ADC4022) to healthy volunteers (HV) and patients with COPD; here we present the safety, tolerance and pharmacokinetic findings from these studies.
Methods Study 1: a randomised, placebo-controlled, single rising dose (12.5 mg and 20 mg) and multiple-dose (12.5 mg twice daily up to 5 days) study in HV. Subsequently the 12.5 mg twice daily dose was studied in combination with placebo or inhaled budesonide. In total, 28 HV were exposed to ADC4022.2 Study 2: a 4-week double-blind randomised comparison of nebulised ADC4022 12.5 mg twice daily or placebo, both in combination with nebulised budesonide 1 mg twice daily, in 91 patients with moderate-severe COPD.
Results Safety: ADC4022 was well tolerated in both studies. In the HV study no adverse events (AEs) were considered drug-related. There were no clinically significant changes in lung function or laboratory parameters. In the COPD study there was a similar incidence of side effects and laboratory abnormalities in the active and placebo groups; only one serious AE occurred (pneumonia in an ADC4022 subject, considered unrelated to drug). FEV1 declined in placebo patients but was maintained in ADC4022 patients (p = 0.045). In HV, theophylline was measurable in the blood within 15 min of nebulisation. After 5 days’ dosing median Tmax was 0.25 h and mean Cmax 0.191 mg/l (range 0.112–0.346). In 10 COPD patients, median Tmax was 0.5 h, mean Cmax 0.323 mg/ (range 0.122–0.603), mean T1/2 8.9 h.
Discussion Nebulised ADC4022 appeared to be safe and well tolerated both in HV and COPD patients. Plasma theophylline concentrations were far below those usually associated with systemic side effects (>10 mg/l).3 Evidence of clinical benefit and anti-inflammatory effects has been shown in study 2,4 and further clinical studies are planned.
P212 FAST ONSET OF EFFECT OF ACLIDINIUM BROMIDE, A NOVEL LONG-ACTING MUSCARINIC ANTAGONIST, IN PATIENTS WITH COPD
1J. Vestbo, 2C. Vogelmeier, 3J. Creemers, 4A. Ribera, 4E. Garcia Gil. 1Medicines Evaluation Unit, Manchester, UK, 2Department of Internal Medicine, University of Marburg, Marburg, Germany, 3Catharina Ziekenhuis, Eindhoven, The Netherlands, 4Almirall R&D, Barcelona, Spain
Introduction Aclidinium bromide is a novel long-acting inhaled muscarinic antagonist in development for the treatment of chronic obstructive pulmonary disease (COPD). Phase II studies have shown that aclidinium provides rapid and sustained bronchodilation in patients with COPD. The aim of this study was to assess the rate of onset of bronchodilation with aclidinium compared with placebo and tiotropium in patients with moderate to severe COPD.
Methods This was a double-blind double-dummy multicentre crossover study in COPD patients with a post-bronchodilator forced expiratory volume in 1 s (FEV1) ⩾30% and <60% predicted. The study comprised three 1-day treatment periods separated by 5–7 days’ washout. In each period, patients received single doses of aclidinium 200 μg (via Genuair, a new multidose dry powder inhaler), tiotropium 18 μg (via HandiHaler) or placebo (via Genuair and HandiHaler). Serial spirometry was conducted over 3 h post-dose. The primary variable was the percentage of patients with an increase in FEV1 of ⩾10% above baseline at 30 min post-dose. Other assessments included relative change from baseline in FEV1 over 3 h post-dose, normalised AUC0–3 h FEV1 and change in perception of dyspnoea.
Results A total of 115 patients entered the study. Significantly more patients had an increase in FEV1 of ⩾10% above baseline at 30 min with aclidinium and tiotropium vs placebo (49.5% and 51.8% vs 13.8%; p<0.0001). At 30 min the relative change from baseline in FEV1 was significantly higher for aclidinium and tiotropium vs placebo (12% and 11% vs 3%; p<0.0001). At all time points (10 min to 3 h post-dose), a higher relative change from baseline in FEV1 was observed in patients treated with aclidinium and tiotropium compared with placebo (p<0.01). Normalised AUC0–3 h FEV1 was significantly above placebo (p<0.0001) with aclidinium (0.127 l) and tiotropium (0.110 l). Aclidinium and tiotropium improved the perception of dyspnoea at all time points measured.
Conclusion The bronchodilatory effect of aclidinium was observed from 10 min post-dose. Aclidinium had an onset of action and magnitude of effect similar to tiotropium during the first 3 h post-dose.
This study was supported by Laboratorios Almirall SA, Barcelona, Spain.
P213 A PHASE III STUDY EVALUATING ACLIDINIUM BROMIDE, A NOVEL LONG-ACTING ANTIMUSCARINIC, IN PATIENTS WITH COPD: ACCLAIM/COPD I
1P. W. Jones, 2P. Chanez, 1A. Agusti, 3H. Magnussen, 4L. Fabbri, 5C. Caracta, 6E. Garcia Gil. 1St George’s, University of London, London, UK, 2Université de la Mediterranée AP-HM, Marseille, France, 3Hospital Grosshansdorf, Grosshansdorf, Germany, 4University of Modena and Reggio Emilia, Modena, Italy, 5Forest Research Institute, New Jersey, USA, 6Almirall R&D Centre, Barcelona, Spain
Introduction We investigated the long-term efficacy and safety of the novel long-acting inhaled muscarinic antagonist aclidinium bromide in patients with moderate to severe chronic obstructive pulmonary disease (COPD).
Methods Patients were randomised in a double-blind fashion (3:1 ratio) to receive aclidinium 200 μg or placebo once daily via the Genuair inhaler (a multidose dry powder inhaler) for 52 weeks. The primary endpoint was trough forced expiratory volume in 1 s (FEV1) at 12 weeks and 28 weeks. Other endpoints included time to first exacerbation and health-related quality of life (HRQL) as measured by the St George’s Respiratory Questionnaire (SGRQ), and improvement in dyspnoea as measured by the Transitional Dyspnoea Index (TDI) at 52 weeks.
Results We examined 843 patients, 627 treated with aclidinium and 216 treated with placebo. At 12 and 28 weeks, aclidinium significantly improved trough FEV1 by 61 and 67 ml, respectively, compared with placebo (both p<0.001); this effect was then maintained over 1 year. More patients receiving aclidinium had clinically relevant improvements in SGRQ total score (⩾4 units; 48.1% vs 39.5%; p = 0.025) and TDI focal score (⩾1 unit improvement 56.4% vs 38.0%; p<0.0001 based on OR) over 1 year compared with placebo. In contrast, aclidinium did not alter the time to first moderate or severe exacerbation (hazard ratio 1.0; 95% CI 0.72 to 1.33; p = 0.89). Aclidinium was well tolerated, with 57% and 59% of patients reporting adverse events in the aclidinium and placebo groups, respectively. The incidence of anticholinergic adverse events was low: dry mouth was reported by 1.0% and 0.9% of patients in the aclidinium and placebo groups, respectively.
Conclusions This study demonstrates that aclidinium 200 μg significantly improves lung function, health-related quality of life and dyspnoea in patients with moderate to severe COPD. Due to the low incidence of COPD exacerbations in the study, no differences were observed between aclidinium and placebo. Aclidinium is well tolerated with a low incidence of dry mouth.
This study was supported by Laboratorios Almirall SA, Barcelona, Spain and Forest Laboratories, New York, USA.
P214 IS REVIEW IN THE CHEST CLINIC OR GP SURGERY ADVANTAGEOUS? CLUES FROM THE 2008 UK COPD AUDIT
1R. A. Stone, 2J. M. Potter, 2D. Lowe, 2N. A. Pursey, 2R. J. Buckingham, 3C. M. Roberts. 1Musgrove Park Hospital, Taunton, UK, 2The Royal College of Physicians, London, UK, 3Whips Cross University Hospital, London, UK
The 2008 UK COPD Audit comprised five elements, one being a survey completed by 2864 patients hospitalised with exacerbation and reported at www.rcplondon.ac.uk/copd. We have now undertaken further analysis of the data, examining particular subgroups within the survey population. We wished to identify any differences in responses of groups who were being reviewed in either chest clinics (n = 440), at their GP surgeries (n = 814), in both settings (n = 727) or neither of these (n = 706), and the data reported represent a summary of the salient points (table 1).
Attendance at both clinic and surgery seemed advantageous over review in one or other setting, and particularly compared with neither. Thus, understanding of COPD was highest in the group attending both chest clinic and surgery (91%) but lowest in those attending neither (77%). The group attending both clinic and surgery had the highest receipt of rescue medication compared with those attending neither (30% vs 16%), greater awareness of changes in sputum at exacerbation (62% vs 48%), a higher proportion of written plans for managing flare-up (32% vs 17%) and explanation about medication (94% vs 71%).
The population attending both chest clinic and surgery may be different fro, that attending neither, however: 32% live alone (vs 43%), 42% use oxygen (vs 24%), 62% use nebulisers (vs 38%) and 31% use both oxygen and nebulisers (vs 17%). 75% of patients reviewed in clinic and surgery had been admitted with COPD in the previous year compared with 53% of those receiving neither and exacerbation frequency was much greater in the former, 93% describing flare-ups a number of times a year compared with 75%. 70% of the reviewed group sought telephone advice compared with 40%; this suggests the COPD may be more severe and less stable in those attending for review.
We conclude that these patient-reported data, albeit in a selected group of hospitalised cases, suggest beneficial effects of a joint approach to COPD care across primary and secondary care, perhaps via improved management of the disease in its totality. Although the data suggest patients not attending for review have less favourable care, this group may have a different profile of disease.
P215 MICROBIAL CONTAMINATION OF HOME NEBULISERS USED BY COPD PATIENTS
1S. Jarvis, 1R. J. Shiner, 2C. P. Thomas, 2S. Goonesekera, 3R. Haffenden, 2A. Abdolrasouli, 1P. W. Ind. 1Department of Respiratory Medicine, Imperial College Healthcare NHS Trust, London, UK, 2Department of Microbiology, Imperial College Healthcare NHS Trust, London, UK, 3Hammersmith and Fulham PCT, Community Respiratory Services, London, UK
Introduction Domiciliary nebulisers are widely used in chronic obstructive pulmonary disease (COPD). Nebuliser contamination has been shown in patients with cystic fibrosis and asthma. Nebuliser cleaning practice has not been assessed in COPD patients who are often elderly, with severe disease and multiple co-morbidities. We investigated microbial colonisation of home nebulisers and examined efficacy of local cleaning instructions.
Methods Nebulisers (n = 44) from COPD patients, mean age 71 years (range 40–93) were swabbed at the time of routine equipment change by the community respiratory service. Cultures were taken from facemasks/mouthpieces, chambers and tubing as returned by patients (pre-washing). After a controlled washing regime and air-drying following local trust guidelines, nebulisers (except tubing) were re-cultured (post-washing). Nebuliser cleaning frequency was established from individual patients.
Results 32/44 (72.7%) nebulisers showed bacterial contamination with heavy growth in chambers (>200 colonies per plate); 19 grew organisms including coagulase-negative staphylococci, alpha-haemolytic streptococci, Bacillus species, diphtheroids, non-pathogenic oropharyngeal Neisseria species and Candida species. Potentially pathogenic organisms colonised 13/44 (29.5%) nebulisers and included Staphylococcus aureus (n = 1) and gram-negative bacteria (n = 10) (including Pseudomonas aeruginosa, Klebsiella pneumoniae, Escherichia coli, Serratia liquefaciens, Proteus mirabilis, multi-resistant Enterobacter cloacae) and filamentous fungus Fusarium oxysporum (n = 1). Of the 44 nebulisers, only 3 were cleaned “after each use”; 7 were cleaned “once a day” and 8 had “never” been cleaned. Of the nebulisers contaminated with pathogenic organisms, 4 had “never” been cleaned (30.7%) while 2 (15.3%) were cleaned “after each use”. Mean (SD) age of patients who had “never” cleaned their nebuliser was 76 (7) vs 61 (19) years in the group who “cleaned after each use”. Post-washing cultures showed eradication of most organisms except coagulase-negative staphylococci and gram-negative organisms, which remained at >100 colonies/plate (fig 1).
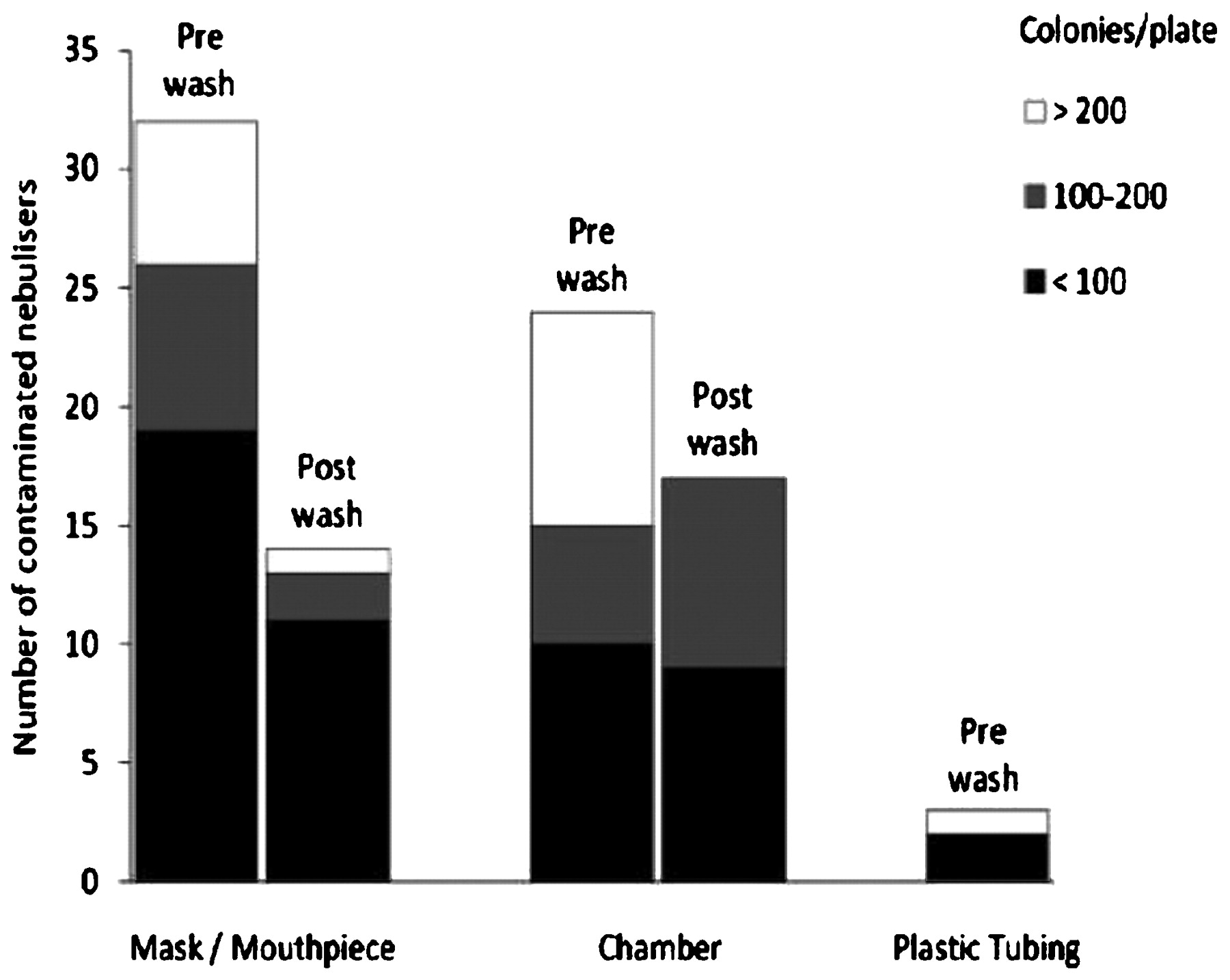
Microbial colonisation of nebuliser components pre- and post-washing.
Conclusions Most COPD patients did not wash their nebuliser as directed. The recommended washing process under laboratory conditions was ineffective at eradicating coliforms and coagulase-negative staphylococci, which may adhere to surfaces via biofilms. Biofilm-associated bacteria demonstrate antibiotic resistance and are increasingly recognised to cause infections. A causal relationship between nebuliser contamination and clinical infection or exacerbations was not studied and requires further work. The various challenges regarding nebuliser-cleaning practices need to be addressed.
P216 ATTITUDES OF CLINICAL STAFF TOWARDS INPATIENT OXYGEN PRESCRIBING
D. Nazareth, K. Nguyen, H. Tan, P. Deegan. Royal Liverpool University Hospital, Liverpool, UK
Background Oxygen supplementation is effective and relatively safe when used correctly, but can be dangerous if used incorrectly. The BTS guidelines on emergency oxygen (October 2008) recommend the safe prescription and administration of all medical oxygen. The Royal Liverpool University Hospital introduced a Trust-wide oxygen prescribing policy in 2005. Several audits have shown that not all patients receiving oxygen have an oxygen prescription (consistently <75%) and not always correctly applied (wrong Fio2, wrong device). This study attempts to identify possible factors and attitudes that influence staff in their approach to oxygen prescribing.
Methods A self-administered questionnaire was used. Some questions were of a yes/no format. However, the majority were on a 6-point scale (1 = strongly disagree and 6 = strongly agree) with answers grouped as disagree (1–2) and agree (5–6) for comparative purposes.
Results Questionnaires were completed by 86 medical staff (67 (78%) junior doctors). Although 84 respondents (98%) were aware that oxygen should be prescribed, only 54 (64%) were aware of guidelines (51 (61%) Trust and 16 (19%) BTS). Regarding oxygen prescribing, 57 (72%) agreed that it ensured patient safety and was good clinical management, and 55 (70%) indicated that this should not be left to nursing staff. However, 75 (87%) gave responses to questions exploring reasons why oxygen may not be prescribed (see table 1) and only 28 (36%) welcomed ward pharmacists’ input. Additionally, 15 (19%) felt that guidelines interfered with clinical practice and freedom to make decisions.
“When I do not prescribe oxygen, it is because”
Conclusions Most staff are aware that oxygen needs prescribing but there is a significant proportion who are unaware of guidelines. Failure to start a prescription seems to be related more to staff forgetting rather than to a feeling it will generate extra work. Pharmacists’ input would be helpful in this regard, but there seems to be some resistance to this measure. There is also a small proportion who appear to be resistant to the idea of prescribing oxygen for a variety of reasons and these attitudes will need to be addressed in educational and training programmes.
P217 IMPROVED HEART RATE VARIABILITY AFTER LONG-TERM OXYGEN THERAPY IN HYPOXIC PATIENTS WITH COPD
1K. E. Lewis, 2J. A. Annandale, 3M. J. Lewis. 1Swansea School of Medicine, Swansea, UK, 2Respiratory Unit, Prince Philip Hospital, Llanelli, UK, 3School of Human Sciences, Swansea University, Swansea, UK
Introduction The exact mechanisms by which long-term oxygen therapy (LTOT) increases survival in hypoxic patients with chronic obstructive pulmonary disease (COPD) are unknown. Reduced heart rate variability (HRV) is associated with sudden cardiac death. We wanted to see if HRV is influenced by LTOT in hypoxic COPD patients.
Methods A pilot interventional cohort study. Ten hypoxic non-smoking stable COPD patients (7 men, mean age 73.9±7.2 years) underwent Holter ECG monitoring (Spacelabs Del Mar Reynolds, UK) for a 24-hour period before and after LTOT, prescribed for 28 days for 16 h/day according to standard guidelines.1 All subjects had resting arterial oxygen tension increased to >8 kPa with no change in arterial carbon dioxide tension on LTOT. HRV was quantified during the morning, afternoon, evening and night periods using recommended measures.2 Subjects also had physical activity/energy expenditure monitoring (SenseWear Pro3 Monitor; Bodymedia Inc, USA) but had no other changes in treatment.
Results Patterns of variation in HRV over 24 h were similar before and after LTOT and similar to healthy controls, suggesting that COPD patients have a generally normal pattern of autonomic nervous system control. HRV was increased (indicating a favourable physiological change) during the morning and night following LTOT (table 1), despite no changes in activity/energy expenditure.
Pre-LTOT vs post-LTOT HRV
Conclusions An increase in HRV following LTOT (in the absence of altered activity levels) provides tentative evidence that LTOT directly modifies heart rate control in COPD. Improvements in HRV occurred mainly during the morning, possibly after using LTOT during the night.
References
P218 ACCURACY OF OXYGEN FLOW METERS IN A SECONDARY RESPIRATORY SERVICE (WARDS AND HIGH DEPENDENCY UNITS) AT A LONDON HOSPITAL
1P. I. Suppiah, 2S. M. S. Smith, 2S. E. Elkin. 1School of Medicine, Imperial College London, London, UK, 2Chest and Allergy, Imperial College Healthcare NHS Trust, St Mary’s Hospital, London, UK
Introduction Accuracy of oxygen flow for titration is imperative for the clinical treatment of hypoxaemia associated with respiratory disorders and other life-threatening diseases. Patients with chronic obstructive pulmonary disease (COPD) exacerbations require accurate titrations of oxygen at varying flow rates and concentrations. This study sought to determine if the oxygen flow meters used at a London hospital were accurate.
Methods An observational study of oxygen flow meters in circulation for clinical use in either a ward or unit. Flow meters were tested at five different flow rates settings (15, 10, 4, 2 and 1 l/min) using three different delivery devices (simple face mask, nebuliser mask and nasal cannulae). All tests were conducted in a closed setting using a digital measuring device.
Results 81 flow meters (FM) were tested. Using a simple mask, FM inaccuracies (%) exponentially increased with a decrease in flow rate (13%, 15 l/min; 20%, 10 l/min; 53%, 4 l/min; 72%, 2 l/min; 79%, 1 l/min). Using nasal cannulae, inaccuracies were found (23%, 15 l/min; 28%, 10 l/min; 56%, 4 l/min; 70%, 2 l/min; 82%, 1 l/min). Using a nebuliser mask, a similar pattern was seen (17%, 15 l/min; 28%, 10 l/min; 49%, 4 l/min; 78%, 2 l/min; 83%, 1 l/min). Flow meters were also analysed by brand, with specific brands being indicative of older equipment having more flow rate errors. The error pattern was consistent across the three delivery devices.
Conclusions A large proportion of flow meters were inaccurate and did not meet the manufacturer’s standard, especially at low flow settings. The clinical impact of these inaccuracies is unknown. A multicentre study is being undertaken to confirm these findings.
Clinical implications of lung infection
P219 ATTEMPTED ERADICATION OF PSEUDOMONASAERUGINOSA IN NON-CYSTIC FIBROSIS BRONCHIECTASIS WITH ORAL CIPROFLOXACIN MONOTHERAPY
A. Jones, J. Stowell, M. Nizbet, R. Wilson. Royal Brompton Hospital, London, UK
Background In patients with non-CF bronchiectasis, colonisation with Pseudomonas aeruginosa (PA) is associated with increased hospital admissions, reduced quality of life and increased mortality. At our centre we screen sputum samples from clinic and at first isolation of PA we attempt eradication, initially with oral ciprofloxacin monotherapy when sensitive. The aim of this study is to determine the success rate of this strategy and any factors associated with successful eradication.
Methods A case note review of all patients identified as having a first isolate of PA between 2003 and 2007 was undertaken. Those patients were reviewed for clinical parameters, lung function, microbiology and clinical outcomes.
Results 43 patients were identified. Mean age at first isolation was 54.79 (±17.81) years, 19 (44%) were male. Six patients (14%) were successfully treated and remained free of PA after 12 months; of these, 3 patients (7%) remained free of PA for the entire time of follow-up. Successful eradication at 12 months was significantly associated with male sex (p = 0.004) and non-mucoid phenotype (p = 0.04). Age at first isolation of PA was also shown to be significant with the successfully eradicated group being older (62.5 vs 53.5 years, p = 0.01). There was no relationship between forced expiratory volume in 1 s (as a marker of severity) and treatment success. No association was found between successful eradication and underlying cause for bronchiectasis, smoking history, steroid use or sinusitis. In 5 patients unsuccessfully eradicated, the PA developed ciprofloxacin resistance. All patients who were successfully eradicated had never had a hospital admission prior to colonisation with PA compared with 14 patients (38%) who were unsuccessful.
Conclusions Eradication of PA with oral ciprofloxacin has a low rate of success, but having a non-mucoid phenotype of PA and being male is significantly associated with an improved chance of eradication. It is likely that people who have a first isolate of PA at an older age have less severe disease and, as such, an improved rate of eradication. A non-mucoid phenotype may reflect recent colonisation and this emphasises the importance of regular screening of sputum for PA.
P220 SYSTEMIC MANIFESTATIONS OF BRONCHIECTASIS
1N. S. Gale, 2J. M. Duckers, 3M. Munnery, 1S. Enright, 3J. R. Cockcroft, 2C. E. Bolton, 2D. J. Shale. 1School of Healthcare Studies, Cardiff University, Cardiff, UK, 2Department of Respiratory Medicine, University Hospital Llandough, Cardiff, UK, 3Wales Heart Research Institute, Cardiff University, Cardiff, UK
Background Bronchiectasis is characterised by inflammation and airways injury which lead to loss of airways function, this being associated with an increased risk of cardiovascular disease (CVD) in healthy individuals and subjects with airways obstruction.1 Increased aortic pulse wave velocity (aPWV) (a predictor of cardiovascular risk) and loss of bone mineral density (BMD) have been reported in chronic obstructive pulmonary disease,2 but extrapulmonary manifestations have not been well studied in bronchiectasis. We hypothesised that patients with bronchiectasis would have increased aPWV and reduced BMD.
Methods We studied 20 (4 male) clinically stable patients with bronchiectasis and 20 age-, sex- and smoking-matched controls, all without prior evidence of CVD. In all subjects we determined aPWV, blood pressure (BP), forced expiratory volume in 1 s (FEV1) and systemic inflammation (interleukin-6, IL6). All participants had fat-free mass index (FFMI) and BMD determined by DXA scan, and exercise capacity by the 6-minute walk distance (6MWD).
Results Median age of patients was 65 years (range 42–80) and 62 years (36–69) for controls. aPWV, heart rate and IL6 were greater in patients, while 6MWD was lower compared with controls (p<0.05, table 1). In all subjects aPWV related to age (r = 0.694), FEV1% (r = −0.552), log10IL6 (r = 0.389), systolic BP (r = 0.329) and 6MWD (r = −0.454) (all p<0.05). The BP, BMI, FFMI and BMD were similar between patients and controls (p>0.05).
Conclusions Patients with bronchiectasis have increased aPWV and systemic inflammation and reduced exercise capacity, which indicate a greater risk of CVD. However, BMD was not reduced in this group. Further studies are required to investigate this further and to determine the long-term effects of the haemodynamic alterations.
P221 STREPTOCOCCUS PNEUMONIAE INFECTION: ENHANCED PREDICTION OF SURVIVAL BEYOND PNEUMONIA SEVERITY SCORING
L. Varatharajan, A. Draper, S. Akhtar, A. Higton, K. Gajee, F. Chua. St George’s Hospital NHS Trust, London, UK
Rationale Pneumococcal infections can produce severe pneumonic disease, often with bacteraemic (invasive) complications. We postulated that evaluating patient attributes, in addition to calculating pneumonia severity and acute physiological derangement, would improve the prediction of patient survival.
Methods A retrospectively identified cohort of 114 patients (64 M, 50 F; age range 22–98 years, median 59) who presented with infective symptoms and tested positive for urinary pneumococcal antigen between October 2006 and August 2008 was studied. In addition to CURB(−65) and APACHE II scores, pre-morbid functional status, radiological findings and microbiological results were assessed. Associations with survival and death within 30 days were determined. Multiple variables were analysed using logistic regression analysis.
Results In this cohort, 16/114 (14%) inpatient deaths were recorded (among whom six patients were transferred to ICU, including four for endotracheal intubation). Pneumococcal bacteraemia was detected in 17/114 (14.9%) cases. Of the variables examined, decreased pre-admission mobility was significantly associated with 30-day mortality (odds ratio (OR) 4.54; p = 0.028) when adjusted for pneumonia severity. Further adjustment for concomitant all-type cancer increased the OR to 13.18 (p = 0.032). Area-under-the-curve of receiver operating characteristics for (CURB(−65) + mobility + cancer) was 0.81 (95% CI 0.71 to 0.91). In contrast, the extent of radiological abnormality had poor discriminatory value for mortality. APACHE II score of <9 strongly correlated with survival at 30 days as shown by Pearson χ2 test (p = 0.003). This cut-off was 100% sensitive at predicting mortality; in the remaining 75 cases with APACHE II scores ⩾9 the death rate was 19%. Stratification by CURB(−65) revealed a 30-day survival rate of >95% for scores 0–1; scores of 3 and 4 were associated with mortality rates of 14.3% and 41.7%, respectively.
Conclusion Physiological scoring clarifies the severity of acute illness and assigns mortality significance to patients with pneumococcal sepsis. Additional assessment of specific pre-morbid factors may enhance predictive modelling and influence clinical decision-making, particularly when considering escalatory measures or, conversely, when setting treatment limits. Pre-hospitalisation mobility appears to be an important factor; however, adjustment for age and co-morbidities requires further evaluation. We propose validating our findings in a larger cohort, ideally with prospective scrutiny.
P222 PROINFLAMMATORY POTENTIAL OF PSEUDOMONAS AERUGINOSA IN MACROPHAGE MODELS: IMPORTANCE OF CLINICAL ORIGIN?
1L. A. Borthwick, 2J. Perry, 1A. J. Fisher, 1A. De Soyza, 1S. S. Sunny. 1Newcastle University, Newcastle upon Tyne, UK, 2Freeman Hospital, Newcastle upon Tyne, UK
Introduction Pseudomonas aeruginosa is the primary cause of respiratory infection in cystic fibrosis (CF) patients and has a propensity for establishing a chronic form of infection. Persistent infection leads to prolonged inflammation, resulting in considerable morbidity and mortality. Prior research suggests that there may be strain-to-strain variations in proinflammatory potentials of bacteria depending on its clinical origin. Many studies have, however, used limited strain numbers or laboratory strains.
Aim To determine whether differences in proinflammatory potential existed between clinical isolates of CF-derived and non-CF-derived P aeruginosa and Haemophilus influenzae (which is generally associated with less severe clinical pathology than P aeruginosa).
Methods THP-1 and PMA-differentiated U937 macrophage-like cells were stimulated with whole cell lysates (WCL) of CF P aeruginosa (n = 8), non-CF P aeruginosa (n = 9) and H influenzae (n = 7) for 24 h. Interleukin (IL)8, IL1β and tumour necrosis factor (TNF)α release was measured by ELISA. Macrophage viability was assessed by FACS.
Results In both THP-1 and U937 cells, stimulation with WCL induced no significant cell death. In U937 cells, CF-derived P aeruginosa strains induced significantly less release of cytokines than non-CF strains (IL8: 1341 ng/ml±37 vs 1548 ng/ml±38, p<0.01; IL1β: 1413 pg/ml±60 vs 1708 pg/ml±108, p = 0.04; TNFα: 7910 pg/ml±319 vs 10247 pg/ml±294, p<0.01). Conversely, when THP-1 cells were used, no significant difference was observed between CF and non-CF strains (p>0.05). However P aeruginosa strains induced significantly more cytokine release than H influenzae strains from THP-1 cells (IL8: 67330 pg/ml±3893 vs 51754 pg/ml±3136, p<0.01; IL1β: 1288 pg/ml±73 vs 843 pg/ml±73, p<0.01; TNFα: 2833 pg/ml±254 vs 1428 pg/ml±151, p<0.01). No significant difference was observed when all P aeruginosa strain lysates were compared with H influenzae lysates as stimulants of U937 cells (p>0.05).
Conclusion There is variation across strains of P aeruginosa attributable to the clinical source of the strain. This provides support for the hypothesis that bacteria can adapt to their surroundings in a way that alters their proinflammatory potential. However, the extent to which this can manifest itself in the in vivo setting depends on which macrophage line used. Prior literature should be interpreted with caution.
P223 EFFECTS OF TEMPERATURE AND HUMIDITY ON ADULT ADMISSIONS WITH COMMUNITY ACQUIRED PNEUMONIA
J. Micallef, R. Callus, J. Mamo, S. Montefort. Mater Dei Hospital, Birkirkara, Malta
Introduction Epidemiologists have long recognised an association between climate and infectious diseases. Pneumonia tends to peak in the cold winter months. Previous studies looking at the influences of meteorology on the incidence of pneumonia have postulated that sudden differences in temperature and humidity are a possible reason for the development of pneumonia.
Aim To determine whether there is a relationship between fluctuations in temperature and humidity and the number of hospital admissions with community acquired pneumonia.
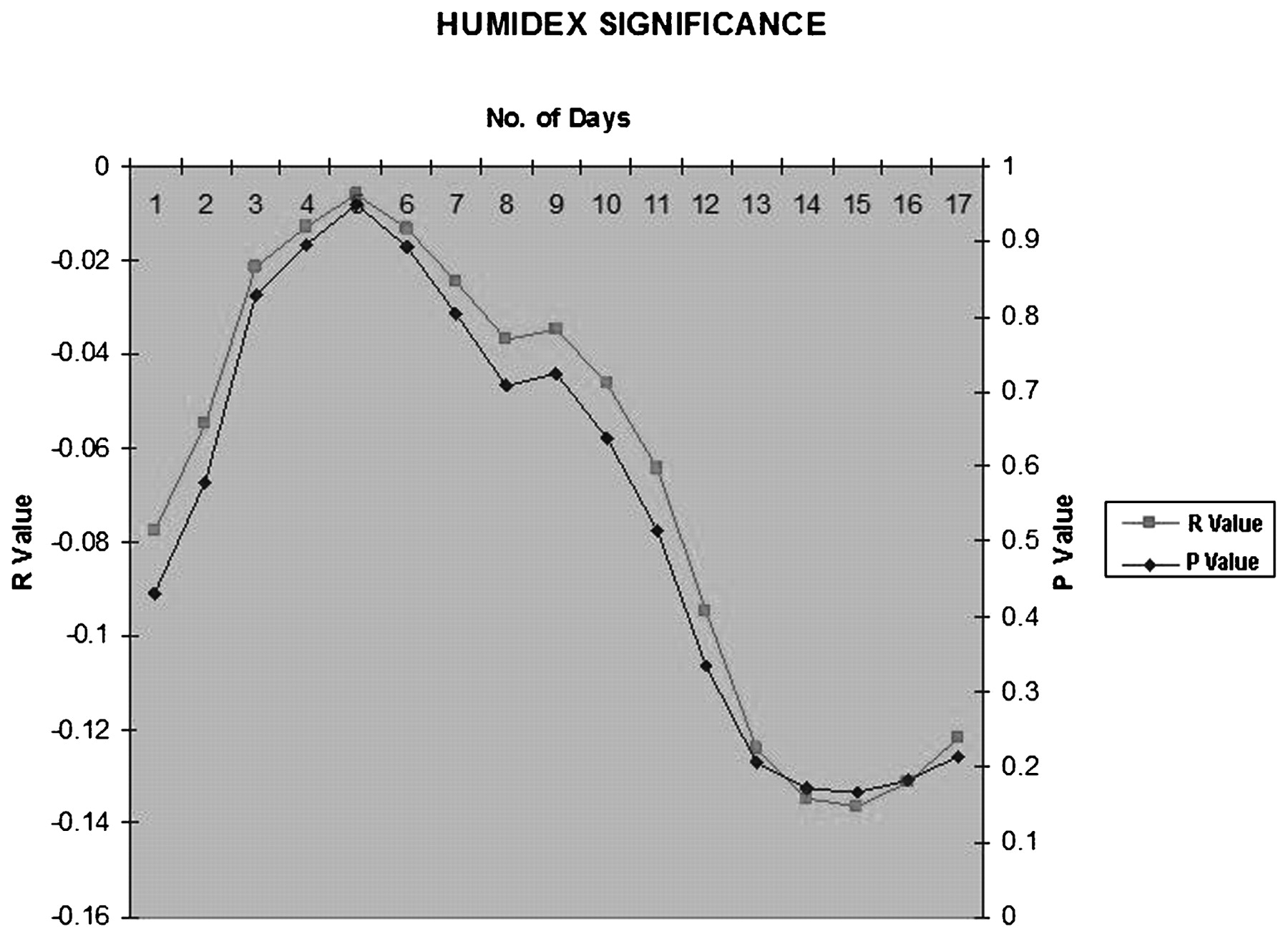
Method All adult patients with radiological and clinical evidence of community acquired pneumonia admitted at the University Hospital were included in a prospective study. The study was conducted over 15 consecutive weeks (105 days) between 1 December 2008 and 15 March 2009. These are the coldest winter months in a small island with a population of around 500 000 inhabitants with a single main university hospital. The daily minimum and maximum temperatures and humidities were obtained from the National Meteorological Office. These were used to calculate a daily Humidex value. This is used by the Meteorological Service of Canada as a calculation of perceived environmental temperature. Humidex = (air temperature) + h with h = (0.5555)*(e –10.0) and e = 6.11 * exp [5417.7530 * ((1/273.16) − (1/dewpoint in Kelvin))]. The results were then compared with the daily pneumonia admissions using STATA statistical program.
Results A total of 196 patients admitted over the study period had radiological evidence of pneumonia. Due to the small numbers, the correlation between temperature and humidity did not show any statistically significant levels. The statistical program STATA showed an increased risk of admission from days 8 to 14 (p = 0.17). A graphical representation of temperatures and humidity shows an increase in admissions 1 week after a visible decrease in the average daily temperature (fig 1). This shows a degree of correlation which is not significant on statistical analysis.
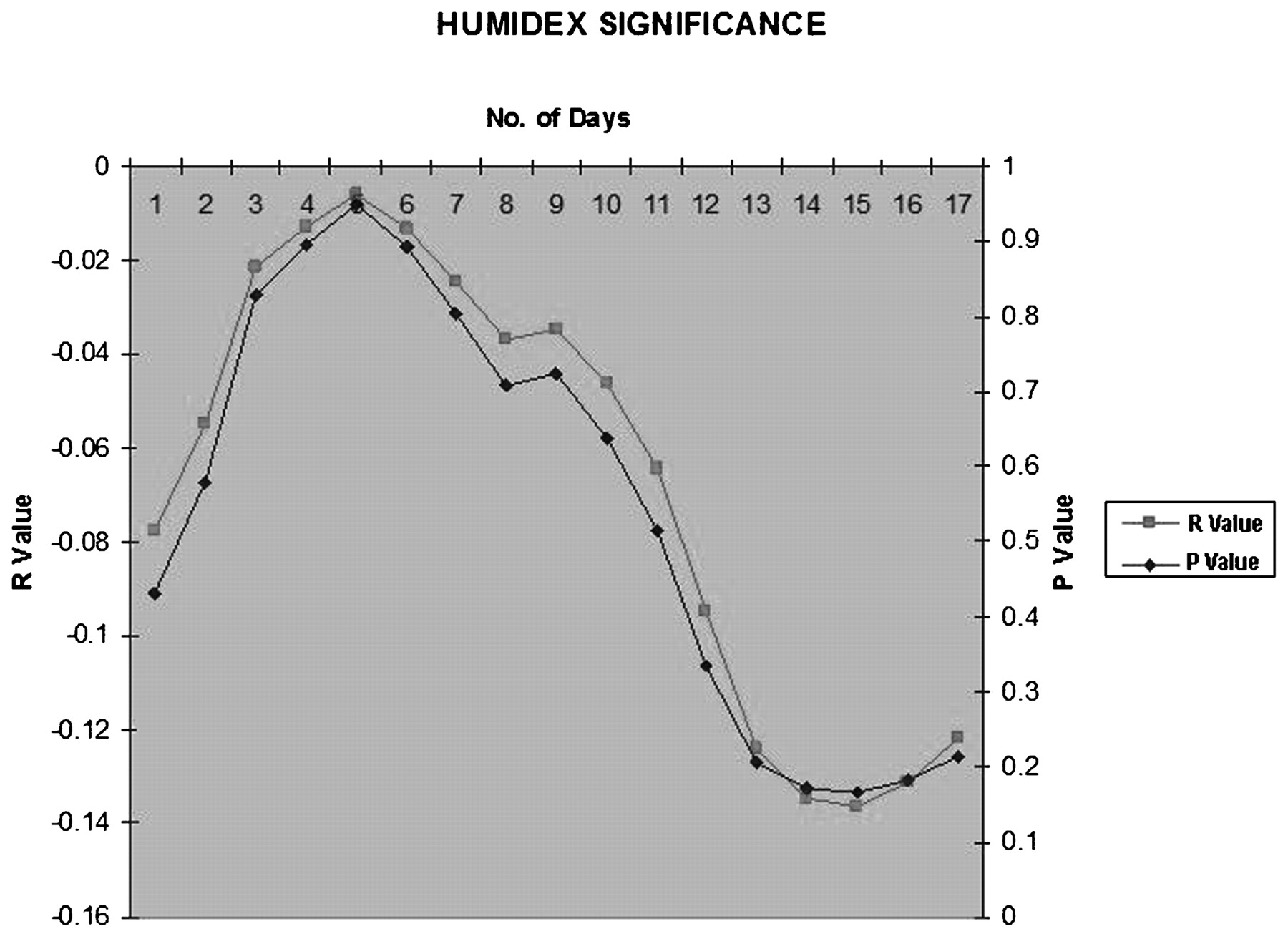
Conclusion Winter with its low temperatures alone does not appear to be the sole reason for the development of community acquired pneumonia in an island population. Sudden fluctuations in meteorological conditions may help predict an increase in hospital admissions. Further studies with a larger sample population are required.
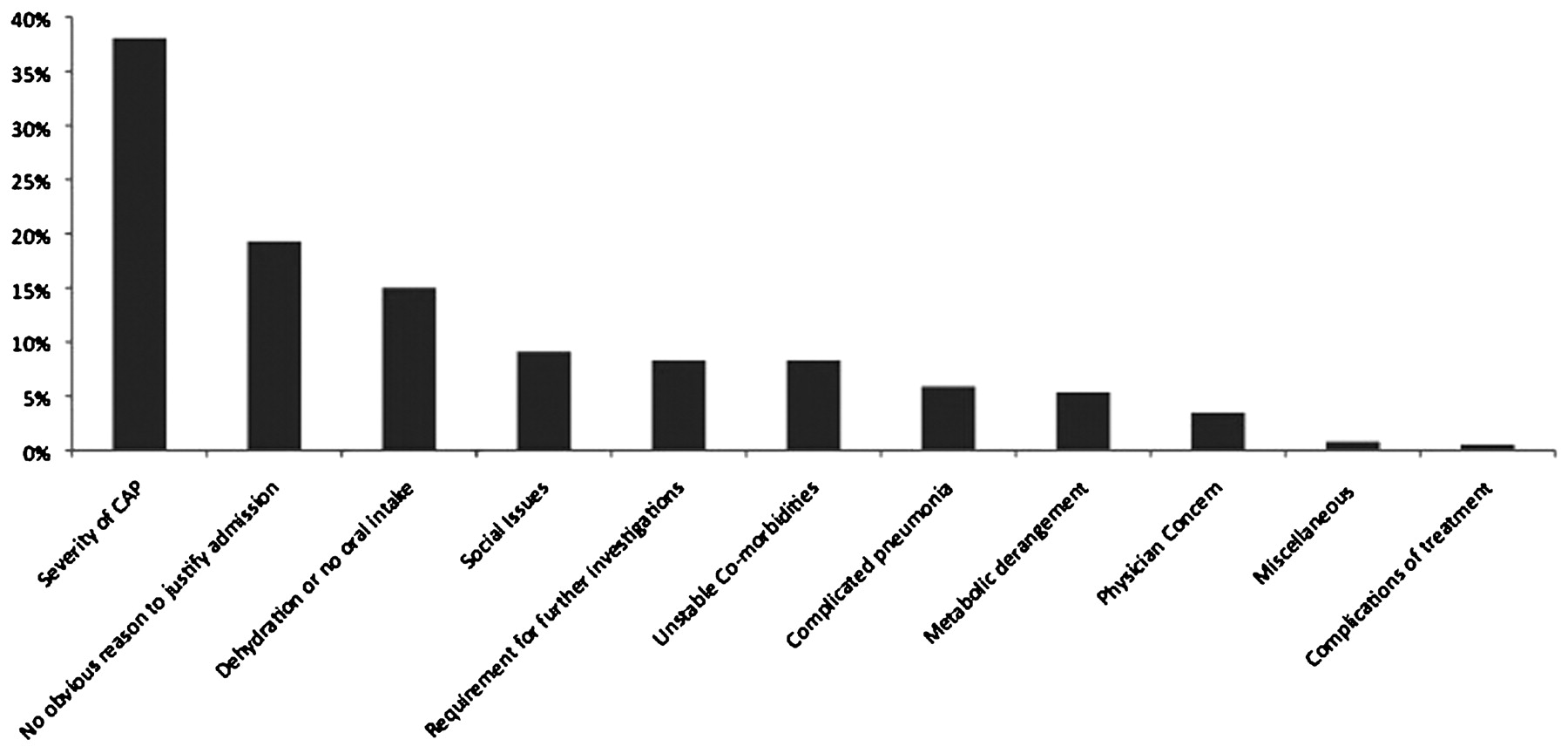
P224 REASONS FOR HOSPITALISATION IN PATIENTS WITH COMMUNITY ACQUIRED PNEUMONIA WITH LOW CURB65 SCORES AND THEIR OUTCOME
1G. Choudhury, 1J. D. Chalmers, 1P. Mandal, 1A. R. Akram, 1M. P. Murray, 2P. M. Short, 1A. Singanayagam, 1A. T. Hill. 1Royal Infirmary of Edinburgh, Edinburgh, UK, 2Ninewells Hospital and Medical School, Dundee, UK
Introduction The BTS Community Acquired Pneumonia (CAP) guidelines recommend that patients at low risk of mortality using the CURB65 score (0–1) could be managed as outpatients. Despite this, many are hospitalised. The aim of our study was to investigate why low-risk patients with CAP were admitted to hospital and to look at the outcome.
Methods We retrospectively reviewed case records for CAP patients admitted with low CURB65 scores (0–1) enrolled in a prospective observational study of CAP conducted from Jan 2005 to Jan 2008. The main reasons for admission to hospital (⩾12 h of hospital stay) were classified by two independent investigators and a consensus reached. Outcomes were need for mechanical ventilation and/or inotropic support (MV/IS) and 30-day mortality.
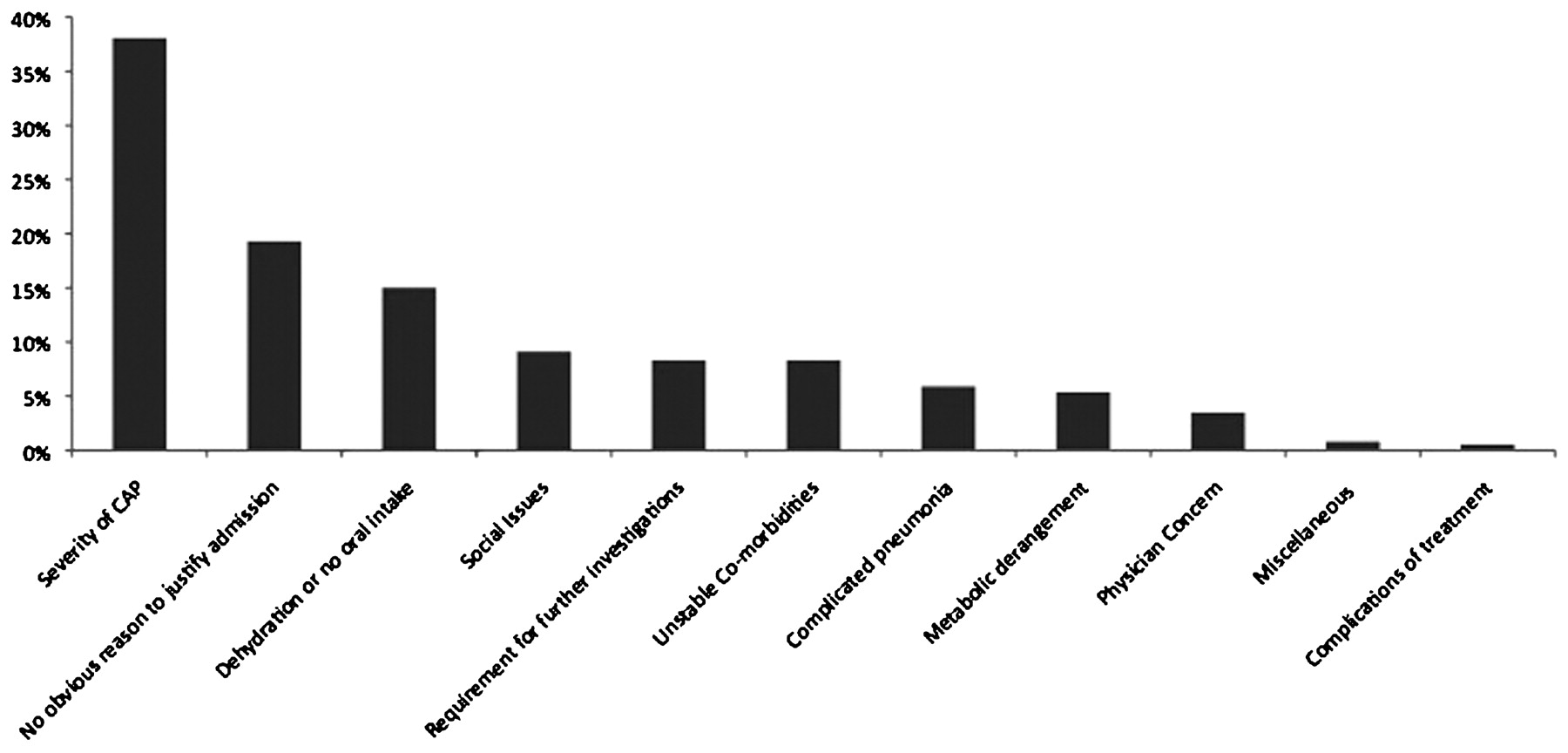
Results 1249 patients were referred to hospital with CAP. 503 patients were classified into CURB65 group 0–1. 130 patients were discharged (within 12 h) from this group, median age 50 years (IQR 36–65). 373 patients with CURB65 0 or 1 were admitted to hospital, median age 56 years (39–65). The reasons for hospital admission are shown in fig 1. The most common reason for hospitalisation was severity of CAP not measured by CURB65. Patients who were admitted had increased frequency of multilobar chest radiographic involvement (9.9% in admitted patients vs 0% discharged, p<0.0001) and higher C-reactive protein (CRP) levels (CRP ⩾100 mg/l in 59.2% vs 32.3%, p<0.0001). There was also increased frequency of patients with COPD and chronic cardiac disease in those that were admitted (COPD 17.7% vs 8.5%, p = 0.01; chronic cardiac disease 11.5% vs 4.6%, p = 0.02). MV/IS was required for 2.4% in those that were admitted compared with 0% in those that were discharged. 30-day mortality was 2.8% in those that were admitted compared with 0.8% in those that were discharged. In patients with no clear reason for admission, none needed MV/IS and one died.
{kind=link}
{kind=link}
{kind=link}
Severity of pneumonia included oxygen dependence, haemodynamic instabilities, severe pleurisy not controlled by simple analgesia, severe breathlessness. Metabolic derangements included diabetic complications, electrolyte disturbances such as hyponatraemia and hyperkalaemia. Physician concern entails all those situations where physician pre-empted potential complications (eg, empyema).
Conclusion The majority of low-risk patients with CAP presenting to hospital have legitimate reasons to justify hospitalisation. This study therefore supports the need for clinician assessment as an adjunct to CURB65 score. A further 18% of hospitalised patients, however, could have been managed as outpatients.
P225 ANTIBIOTICS FOR EXACERBATIONS OF NON-CF BRONCHIECTASIS: WHEN, WHY AND WHAT DO RESPIRATORY PHYSICIANS PRESCRIBE AND FOR HOW LONG?
J. G. Macfarlane, A. T. Hill. Respiratory Department, Royal Infirmary of Edinburgh, Edinburgh, UK
Introduction The aim of this national study was to explore the views of consultant respiratory physicians on the duration of antibiotics required for an acute exacerbation of non-CF bronchiectasis (AEB).
Methods This report summarises the first 100 results of a national survey sent to all UK consultant respiratory physicians. The survey assessed features used to diagnose an AEB requiring antibiotics, factors influencing a longer antibiotic course, as well as choice and duration of antibiotics.
Results Diagnosing an AEB requiring antibiotics: Respiratory physicians use symptoms, invariably in combination, to diagnose an AEB. These most commonly included increase in sputum purulence (99%) and sputum volume (85%); also dyspnoea (59%), cough (45%). They uncommonly use changes in lung function (18%), chest signs (2%) or fever (5%). Choice of antibiotic: If no previous sputum microbiological results were known, 93% of physicians treated with amoxicillin, coamoxiclav or doxycycline in mild bronchiectasis (67%, 20% and 6% ,respectively), with only 1% using a fluoroquinolone. In severe bronchiectasis, just 59% used amoxicillin or coamoxiclav (38% and 21%, respectively) and 33% used a fluoroquinolone. Duration of antibiotic course and sputum microbiology: The decision to prescribe more than 7 days of antibiotics for an AEB was influenced by: a history of ⩾3 exacerbations per year (57%), degree of sputum volume (34%) or purulence (30%), respiratory co-morbidity (30%), physicians’ usual practice (20%), patient preference or experience (15%), age ⩾65 years (11%). Table 1 shows that physicians were more likely to prescribe a prolonged course of antibiotics (>7 days) if Pseudomonas aeruginosa or enteric gram negative bacilli were present compared with other bacteria in both mild and moderate/severe bronchiectasis (p<0.0001 and 0.008, respectively). Patients with moderate/severe bronchiectasis were more likely to receive a prolonged course than those with mild disease (p<0.0001).
Duration of antibiotics prescribed by respiratory physicians for acute exacerbations of mild vs moderate/severe bronchiectasis with different sputum microbiology
Conclusions These results demonstrate the considerable variability in the management of AEB. Diagnosis is based mainly on symptoms, not examination or lung function. The duration of antibiotics is guided by a range of patient symptoms and history, but also by physician habit and the results of sputum microbiology and severity of underlying disease.
P226 DEVELOPMENT OF AN ADULT “CYSTIC FIBROSIS SWINE FLU TRIAGE SERVICE” IN A LONDON TERTIARY REFERRAL CENTRE
D. J. Dhasmana, K. Dack, K. Gyi, M. E. Hodson, D. Bilton. Department of Cystic Fibrosis, Royal Brompton Hospital, Royal Brompton and Harefield NHS Trust, London, UK
Introduction and Objectives Swine-origin influenza virus (SOIV) pandemic continues to spread with increasingly epidemic proportions in the UK, and in London in particular. Careful management strategies must be developed in secondary and tertiary care where inpatients and staff are susceptible. Cases are predicted to rise in the autumn and appropriate validated triage measures should be sought in anticipation of this.
Methods We have initiated such a service for all adult patients with cystic fibrosis (CF) with suspect SOIV which includes a dedicated mobile hotline number, telephone advice, attendance of those at risk and admission of those found to require further inpatient care. Several clinical, microbiological and radiological parameters have been prospectively recorded. Each patient was given a “flu score” of 0–6 according to pandemic flu screening criteria, with one point for each of fever, cough/sore throat, myalgia, vomiting/diarrhoea, headache, rhinorrhoea.
Results Early data show that the majority of CF patients develop a mild and self-limiting illness which can be safely managed at home without attendance. Current data are as follows: 101 phone calls; 24 patients given Tamiflu, 1 pregnant woman given Relenza; 7 attendances of which 5 led to admission; of attendances 3/6 were positive for influenza A by nasopharyngeal aspirate (NPA) including 2 later confirmed H1N1 by RNA PCR and 1 still pending; 1 NPA was negative and the final 2 were of inadequate quality for analysis although throat swabs in these latter 2 cases were negative. Antibiotics were additionally prescribed in 24 patients, intravenously in 6 cases. 2 patients had been issued Tamiflu by their GP with “sick contacts” but were themselves asymptomatic. Assessment of the service is ongoing at the time of reporting and analysis of further biochemical parameters including C-reactive protein, lymphocyte count and vitamin D are in process. Early analyses of “flu score” data suggest 4/6 stratifies those highly likely to have SOIV and that would require inpatient interventions.
Conclusions SOIV remains a major concern in London in secondary and tertiary care where inpatients with significant clinical morbidity are at risk. The service to date appears to offer a safe and effective vehicle through which patients with CF can receive a level of intervention appropriate to their needs.
P227 PROCALCITONIN: A USEFUL MARKER OF SYSTEMIC BACTERIAL SEPSIS?
1V. Patil, 2J. B. Morjaria, 1F. DeVilliers, 2K. S. Babu. 1Inverclyde Royal Hospital, Greenock, UK, 2Southampton General Hospital, Southampton, UK
Introduction Appropriate identification and monitoring of bacterial sepsis is pivotal for best patient outcomes. Procalcitonin (PCT) is a pro-hormone of calcitonin released in response to bacterial infections. PCT concentrations of <0.5 ng/l suggest low-risk bacterial sepsis, levels between >0.5 and <2 ng/l suggest possibility of systemic sepsis and levels of >2.0 ng/l indicate high risk.
Aims We have previously examined the role of a semi-quantitative PCT test and found that 50% of the patients with PCT levels ⩾2 ng/l had positive cultures. However, this test provided insufficient information on the response to treatment. The current study examined the usefulness of a quantitative PCT assay in bacterial sepsis, comparing it with the gold standard (ie, cultures and other markers, namely total white cell (WC) and neutrophil counts and C-reactive protein (CRP)).
Methods PCT assays performed using VIDAS-BRAHMS-PCT (a one-step immunoassay sandwich method using fluorescent detection) was compared with paired blood/fluid (peritoneal and pleural) cultures. Positive bacterial cultures from sputum, urine and tracheal aspirate were excluded as these are less likely to indicate systemic sepsis.
Results We obtained paired data on 99 patients. There were no significant differences in the total WC or neutrophil counts between the two groups of 74 subjects with negative cultures and 25 with positive cultures. However, there were significant differences in the CRP and PCT levels between the two groups (p = 0.04 and p<0.001, respectively). 13 of those with culture positive results had isolates of gram positive organisms while 3 had gram negative isolates and the rest had a mixed flora. Receiver operator curve analysis reported that a PCT value of 2.42 ng/ml had a sensitivity and specificity of 84% and 64.9%, while a CRP of 150 mg/l had 69.6% sensitivity and 52.9% specificity. Their combined specificity was 83.5%.
Conclusion PCT in combination with CRP is a useful marker of systemic bacterial sepsis. Elevation in PCT levels is more likely to be due the presence of gram positive organisms. In patients with suspected systemic sepsis with inconclusive/awaiting culture results, PCT assays may have a crucial role in initiating antibiotic therapy.