Article Text

Statistics from Altmetric.com
P195 THORACIC ULTRASOUND: COMPETENCY AND TRAINING STRATEGIES WITHIN OUR REGION
1L. M. Jones, 1A. B. Hardy, 2J. Hogg. 1St James’s University Hospital, Leeds, UK, 2Pinderfields General Hospital, Wakefield, UK
Introduction A recent National Patient Safety Agency (NPSA) alert1 highlighted the risks of chest drain insertion using the Seldinger technique and strongly advised thoracic ultrasound (TUSS) be undertaken prior to drain insertion. This study aims to identify the range of TUSS competency in our region as well as investigating local strategies for obtaining the necessary equipment and training.
Method To ascertain the local availability of TUSS an online questionnaire was sent to a consultant at each hospital in the region.
Results All of the hospitals responded. Four of 12 hospitals (33%) had an ultrasound machine within the respiratory department and three hospitals (25%) had a machine available within the hospital but in another department. Of the 12 hospitals, seven (58%) had a lead clinician for thoracic ultrasound. 34% of senior doctors in respiratory departments had attended an ultrasound course (0–86%). Three consultants within the region, but no registrars, have achieved level 1 competency in performing TUSS. In four hospitals TUSS was supervised by radiologists, two hospitals had radiographer supervision, two had respiratory consultants with level 1 USS competency and one hospital had consultants without competency. In three hospitals TUSS was not supervised (fig 1). Three hospitals had secured funding for an ultrasound training course from their trust. One hospital used the NPSA alert to obtain this. Two respondents commented on difficulty in obtaining funding for a formal training programme; indeed, one hospital quoted that they had been told it was “not a management priority” but had developed a strategy for informal training. Seven hospitals did not have a strategy in place or funding at this time.

Supervision of thoracic ultrasound.
Conclusions At present there is a significant variability in availability of TUSS within respiratory departments and there is a need to standardise training strategies and opportunities to obtain competencies in the region. Given problems with management support and funding opportunities, locally determined solutions are required in the short term but there is a need for regional leadership on the issue. In light of the recent NPSA alert, there is an urgent need for investment in TUSS training and machine availability within hospitals.
References
P196 HAS TRAINING FOLLOWING THE NPSA ALERT IMPROVED THE SAFETY OF SELDINGER CHEST DRAIN INSERTION?
C. M. Hallsworth, H. Walters, C. W. H. Davies, G. V. Robinson. Respiratory Medicine, Royal Berkshire NHS Foundation Trust, Reading, UK
Background The National Patient Safety Agency (NPSA) alerted physicians to the potential risks of Seldinger chest drain insertion in May 2008. The deadline for implementing changes to improve safety was 17 November 2008. Training and assessment of doctors inserting these drains (by two respiratory consultants and the use of a manikin) started in our institution (a large DGH of 1017 beds where <50% of respiratory patients are managed on the respiratory ward) in October 2008.
Methods Data were collected on all patients in whom a Seldinger chest drain was inserted between September 2008 and February 2009. Drain complications were divided into major (death, empyema, significant haemorrhage and lung injury) and minor (all others, including the need for a second drain), with subgroup analysis dependent on the drain insertion location (respiratory ward or other) and pre and post junior doctors’ training.
Results A total of 94 drains were inserted, data are available on 93. 35 drains were for pneumothorax, 58 for effusion; 37 (39%) drains were inserted on the respiratory ward. Potentially unsafe insertion techniques including position outside the safe triangle and without ultrasound was higher for drains inserted off the respiratory ward (11% vs 5%, p = 0.47). The complication rate was higher for drains inserted off the respiratory ward, including two empyemas and one lung injury (55% vs 35%, p = 0.21). Drains “fell out” or blocked more often (45% vs 16%, p<0.01) and second drains were needed more frequently off the respiratory ward (23% vs 5%, p = 0.02). Following junior doctor training, written consent improved off the respiratory ward, but only to 31%; involvement of the respiratory team in drain insertion increased from 14% to 34% (table 1).
Conclusion Seldinger chest drain insertion complication rates remain high, despite the NPSA alert and the new training and assessment of junior doctors. All major complications occurred in drains inserted on the non-respiratory ward. Minor complications fell following doctor training, but remain higher on the non-respiratory ward. The use of ultrasound remains low. Ongoing training and assessment of junior doctors is needed, ideally with the majority of chest drains managed by respiratory specialists.
P197 ATTAINING LEVEL 1 CHEST ULTRASOUND COMPETENCY: PROGRESS OF THE DELEGATES WHO ATTENDED THE BASIC THORACIC ULTRASOUND SKILLS FOR CHEST PHYSICIANS COURSE (2005–9)
A. R. Guhan, S. Kluzek, A. Saha, J. Fletcher, A. Bapu, G. Naisby. The James Cook University Hospital, Middlesbrough, UK
Introduction Chest ultrasound (CUS) examination before any intervention in patients with pleural effusion (PPE) is becoming accepted as best practice among chest physicians (CPs) in the UK. A recent national web-based survey by two of the authors (AG and GN) revealed that 92% of current respiratory trainees (RTs) in the UK wanted CUS training included in their curriculum. As with any skill, adequate training is essential prior to safe independent practice. Training guidelines are available from the Royal College of Radiologists (RCR) for CPs to attain basic (level 1) CUS competency (BCUS-C) that lists both theoretical and practical training requirements. Important among these are acquiring basic ultrasound and CUS theory and formal introduction to the principles of practical CUS that the trainee could subsequently develop under Training Mentor Supervision (TMS). Currently, such training opportunities are limited in the UK. Since June 2005 our institution has organised a Basic Thoracic Ultrasound Skills course for CPs twice a year, aimed at addressing the RCR training requirements, with close to 190 delegates from across the UK attending to date. We were interested to learn about their subsequent progress in CUS training and of any hurdles/difficulties they faced in their path to attain BCUS-C.
Method In mid-July 2009 we invited all the delegates whose contact details were available (n = 161) to participate in a web-based questionnaire survey (http://www.kwiksurveys.com/online-survey.php?surveyID = IBEMI_9e5adac4), specifically asking each delegate whether he/she has attained BCUS-C since attending our course, (if yes) how long this took, did they have TMS, who their mentor was (radiologist/CP?) and what they perceived as important hurdles in their training path.
Results At the time of abstract submission we had 56 (35%) responses, 46% of whom were either consultants or final year trainees. 10 (18%) had attained BCUS-C, requiring approximately 4–6 months to do this, working in units seeing 2–4 PPE/week; 29% had not “got started”. Only 66% had TMS, the majority from radiologists. Difficulty accessing an ultrasound machine (27%) and TMS (40%) remain major hurdles. Those in units with dedicated pleural disease clinics appear to attain BCUS-C sooner.
Conclusions Important hurdles remain in the CP’s CUS training pathway, despite completing our CUS introductory course.
P198 CHEST DRAIN INSERTION TRAINING USING SIMULATION: WEST MIDLANDS DEANERY MODULE
T. R. Naicker, C. Dave, M. Menon, D. T. McLeod. Sandwell and West Birmingham Hospitals NHS Trust, Birmingham, UK
Introduction Modernising Medical Careers (MMC) stipulates that chest drain insertion (Seldinger) is one of the core competences for all medical trainees by ST2 level. Currently there is no formal training in chest drain insertion included in MMC. The West Midlands Deanery is addressing this by funding a research project looking at simulation training in chest drain insertion using a novel porcine rib model.
Structure of Training and Assessment The module consists of both training and assessment. The training is divided into theory and practical; trainees are sent a web link to the BTS guidelines 2 weeks prior to the training day which is reviewed in tutorial format on the training day. Hands-on familiarisation with the Seldinger kit, drain insertion and securing is achieved using porcine ribs mounted on a resin cast of human thorax (fig 1). The face validity of the model was tested over a period of 1 year on both respiratory and non-respiratory trainees before being used in the module. Knowledge is assessed by using six chest radiograph-based questions, each an example of common scenarios. Practical skills are marked using two types of scoring systems; generic scoring was based on direct observed procedures (DOPs) forms and a check list scoring was marked by two respiratory SpRs on a video recording of the trainee’s performance.

Results We have so for trained 75 core medical trainees with a pass rate of 97%. The two candidates who did not pass will retake the module. The feedback has been overwhelmingly positive with the training considered to be realistic. The trainees felt it has significantly improved their skills as well as confidence, and openly stated that they would recommend it to their colleagues.
Conclusions The West Midlands Deanery Chest drain training module is effective in the training of doctors and can be adapted to suit local needs. We have demonstrated that it is possible to train and assess the core medical trainees in chest drain insertion and recommend that respiratory departments embrace the use of simulation models to train the next generation of physicians.
P199 COLLABORATION BETWEEN RESEARCHERS AND PATIENTS IN DEVELOPMENT OF A COPD RESEARCH PROGRAMME
1J. W. Dodd, 2H. Persaud, 1J. R. H. Archer, 1S. A. Srivastava, 1P. W. Jones, 1E. H. Baker. 1St George’s University of London, London, UK, 2On behalf of the Patient Advisory Group, St George’s University of London, London, UK
Background Public and patient involvement in research is a UK priority and may be consultative, collaborative or patient-led. We report on a collaborative project between researchers and patients with chronic obstructive pulmonary disease (COPD) to develop a COPD research programme.
Methods Patients attending a COPD research clinic were invited to join a “patient advisory group”. Meetings are held every 2 months and follow a semi-structured informal “round table” format. At the initial meeting the concept of collaboration was introduced and patients were asked to address general questions about COPD research. At subsequent meetings participants worked collaboratively with researchers to develop specific research proposals.
Results To date the patient advisory group has met three times and been attended by 19 COPD patients. Issues addressed by the participants include: the worst thing about having COPD; patient priorities for COPD research; barriers to patient involvement in research; recruitment; measuring benefits of treatment; safety issues and risk assessment; participant comfort during studies (table 1). Participants have contributed specifically to the design of two new research protocols.
Discussion Collaboration between researchers and COPD patients has raised awareness of patient priorities and needs, improved protocol design and provided new ideas for recruitment and retention into studies. Patient involvement in research also strengthens applications to ethics committees and funding bodies. As our current group comprises patients who are highly motivated to participate in research, their opinions may not reflect those of the COPD community as a whole. Future plans include widening access to patient involvement in research through the St George’s COPD Research Enterprise (SCORE), patient representation on study steering groups and patient involvement in study recruitment.
P200 ASSESSMENT OF PSYCHOSOCIAL PROBLEMS AND DISABILITY IN COPD PATIENTS IN PRIMARY CARE
J. Upton, C. Loveridge, M. Fletcher. Education for Health, Warwick, UK
Introduction In chronic obstructive pulmonary disease (COPD) the prevalence of clinical depression ranges between 10% and 42%. In primary care, COPD patients are increasingly cared for by nurses. Here we measured the frequency nurses undertook the assessment of psychosocial problems and disability. We also investigated the relationship between this with the level of nurse training and whether the practice ran a designated respiratory clinic.
Methods Lead COPD nurses, based at 500 randomly selected UK general practices, were invited to participate. Nurses self-reported the frequency they performed key tasks (scored on a 4-point Likert-type scale), their COPD-related training and whether they ran a designated respiratory clinic. The relationship between the frequency these tasks were performed and the level of training and presence of a respiratory clinic was tested using the χ2 test.
Results 368 nurses completed the COPD questionnaire (74%). 349 ran follow-up consultations. 51% of nurses (95% CI 45% to 56%) reported “always” or “often” assessing psychosocial problems. 48% (95% CI 42% to 53%) reported “always” or “often” assessing disability using a validated scale. Nurses without accredited training and nurses in practices without a designated respiratory clinic were statistically significantly less likely to report “always” or “often” performing these tasks (table 1).
Conclusion Psychosocial problems are infrequently assessed during nurse-led primary care consultations, particularly when patients are not seen in a respiratory clinic or by nurses without accredited training. This may be due to time constraints, lack of knowledge or the exclusion of this task from the Quality Outcomes Framework. Nurses also infrequently assessed disability using a validated scale. This may improve following the recent inclusion of this task in the Quality Outcome Framework. Measures should be put in place to overcome barriers to the performance of key tasks overlooked by primary care nurses.
P201 USE OF A SIMPLE QUESTIONNAIRE TO MEASURE KNOWLEDGE OF OXYGEN PRESCRIBING AT INDUCTION FOR THE F1 YEAR
P. C. Deegan. Royal Liverpool and Broadgreen University Hospitals Trust, Liverpool, UK
Introduction The development of the BTS Guidelines on Emergency Oxygen use has highlighted the need for sensible prescribing of oxygen. Little is known about the level of knowledge of F1 doctors as they start their first post.
Methods All new F1 doctors are given a lecture on practical oxygen prescribing as part of their induction programme (end of July/beginning of August). They are asked to complete an anonymised questionnaire prior to the start of the lecture which includes the following questions (free text, not MCQ): percentage of oxygen in air (Q1); what the abbreviation Fio2 means (Q2); main types of oxygen delivery device (looking for nasal cannulae, venturi mask, partial rebreather/non-rebreather mask, Q3); starting %O2 for an acutely breathless COPD patient (Q4); normal ranges for ABG data (Q5); target oxygen saturation when giving supplemental oxygen (Q6).
Results The results for five consecutive years (2004–8) are summarised in table 1 as percentages of respondents giving specified answers. Table 1 also includes the percentage of respondents giving safe replies to all six questions (ie, safe to prescribe oxygen on the wards). The apparent improvement in some areas in 2008 could possibly be explained by the F1s having had a lecture on “Respiratory Scenarios” immediately prior to the lecture on oxygen prescribing.
Conclusion Results show that there are significant gaps in the knowledge of junior doctors with regard to oxygen prescribing as they complete their undergraduate training. Having a lecture on oxygen prescribing at induction helps, but there is still a need to emphasise these issues in the undergraduate curriculum. Continuing Education is also needed as part of a Trust Policy on Oxygen Prescribing.
P202 OXYGEN PRESCRIBING IN A DISTRICT GENERAL HOSPITAL: AN AUDIT, RE-AUDIT AFTER EDUCATIONAL SESSIONS AND MODIFIED OXYGEN PRESCRIPTION PROFORMA
M. L. Harley, A. J. Wickham, R. G. Francis, J. A. Hughes. Kent and Sussex Hospital, Tunbridge Wells, UK
Introduction and Objectives Oxygen is a widely used medication across all specialties but, despite national guidelines, prescribing is poor. This is important because of the number of side effects of oxygen therapy. This study aimed to assess the accuracy of oxygen prescribing and whether prescriptions are followed and altered in view of clinical response. The audit standard, derived from the British Thoracic Society (BTS) guideline for emergency oxygen use in adults, is that “100% of patients have accurate oxygen prescription with a target saturation range”.
Method The standard BTS emergency oxygen audit proforma was used to assess all adult patients in non-critical care environments in a district general hospital setting. A multi-time point survey was completed and re-audited over two 2-month periods approximately 8 months apart. The re-audit was completed following three formal educational sessions and informal nurse-led ward-based teaching.
Results 1454 patients were assessed in the two audit periods. 14% (n = 206) of patients were using or prescribed oxygen. In the initial audit only 14% of patients had a formal oxygen prescription with target saturation, the majority of which were met. 63% of patients were not using the prescribed oxygen delivery system. In the re-audit, 23% had a formal oxygen prescription and a further 26% had another clear instruction for oxygen use. 75% of patients with a target saturation met this. Fewer patients (43%) were using a different oxygen delivery system from that prescribed.
Conclusions Oxygen prescribing improved following multiple education sessions suggesting a moderate benefit. Alteration of oxygen prescriptions in view of clinical response did not change following education sessions; this could be improved by using a modified BTS oxygen prescribing proforma (table 1), allowing more area for changes. This new proforma is being considered for integration into a South East Thames regional drug chart. Bedside oxygen posters, made in conjunction with medical devices companies, should be displayed in all ward areas to improve understanding and help engender a change in attitude among medical staff towards oxygen prescribing.
Modified BTS oxygen prescribing proforma
P203 AN AUDIT OF THE EFFECT OF OXYGEN PRESCRIPTION CHARTS ON CLINICAL PRACTICE
M. Wijesinghe, K. Perrin, R. Beasley. Medical Research Institute of New Zealand, Wellington, New Zealand
Introduction and Objectives The BTS guideline for emergency oxygen use in adult patients recommends that every hospital should have a designated oxygen section on the drug chart on which oxygen should be prescribed and a target oxygen saturation range stated. The purpose of this audit was to investigate whether the introduction of a new drug chart with an oxygen prescription section would improve hospital-wide prescription, administration and monitoring of oxygen therapy.
Methods An initial audit was undertaken of all patients in our tertiary referral hospital, excluding the neonatal unit, paediatric ward, psychiatric ward, emergency department and intensive care unit. The hospital records and observation charts of patients receiving oxygen were reviewed and information on monitoring prior to starting therapy, prescription, and monitoring and titration while receiving oxygen was recorded. Criteria were set to assess whether prescription, assessment, monitoring and titration of oxygen were adequate. A second audit, using identical methodology, was then conducted 6 months following the introduction of a new drug chart, with a specific oxygen prescription section on the front of the chart.
Results 610 and 566 patients were audited in 2007 and 2008, respectively. The results are shown in table 1.
Conclusions An oxygen prescription section on hospital drug charts improved the prescription of oxygen but did not improve clinical practice. Additional strategies are required to improve the administration of oxygen therapy in hospitals.
P204 CONSULTANT-LED SPECIALIST COMMUNITY COPD CLINIC: DOES IT WORK?
N. Diar Bakerly, J. A. Roberts. Salford PCT, Salford, Lancashire, UK
Introduction Services provided in secondary care can be expensive and inflexible, particularly if it covers large geographical area as patients often find it difficult to travel. This may cause inequality in access to services including outpatients. Our PCT commissioned a consultant-led specialist community COPD clinic to provide easy access to clinic. We present data from the first 12 months of this service.
Methods A community COPD clinic was introduced once weekly (one session). The clinic is delivered by a consultant respiratory physician and respiratory nurse consultant in three venues (rotating). Referral criteria were developed and included a chest radiograph and spirometry prior to referral. The clinic was widely advertised to clinicians in primary and secondary care with its aims clearly defined, and that is to deal mainly with severe or difficult-to-diagnose COPD. The clinic was added to the electronic Choose and Book system.
Results A total of 203 patients were seen. 117 (58%) were new patients and the remaining were follow-ups or transfers of care from secondary care clinics. New patients’ characteristics are shown in table 1. Average waiting time from referral was 30.2 days. 65% of patients were referred from primary care, 18% from secondary care and 13% from the integrated COPD team. 97 (83%) patients had COPD as the primary diagnosis (21 mild; 45 moderate; 31 severe). Only 8 (6%) patients did not have COPD, with 3 referrals considered inappropriate. 26 (22.2%) of new patients required extra tests including blood tests, full pulmonary function tests and CT scans; however, most blood tests were conducted in general practice.
Conclusions Community COPD clinics are an alternative to secondary care-based clinics and provide easy access to specialist advice. Approximately one in five patients required further secondary care-based tests. Inappropriate referrals to these clinics do not appear to be a problem. These clinics may therefore have a role in the management of patients with COPD.
P205 BTS BRONCHOSCOPY TRAINING SURVEY 2009
I. A. Du Rand, R. A. Lewis. Worcestershire Royal Hospital, Worcester, UK
Objectives Following changes in the European Working Time Directive compliant working patterns, time for training in all specialties has been reduced. Numbers of bronchoscopies and competency levels are an indicator of training in this important aspect of respiratory medicine. Our objective was to assess bronchoscopy training with the use of a questionnaire.
Methods The authors designed and undertook an online national survey on behalf of the BTS of all respiratory SpRs in the UK to establish trainees’ training opportunities, exposure and competencies in flexible bronchoscopy. Trainees were asked to self-report competencies for various aspects of bronchoscopy.
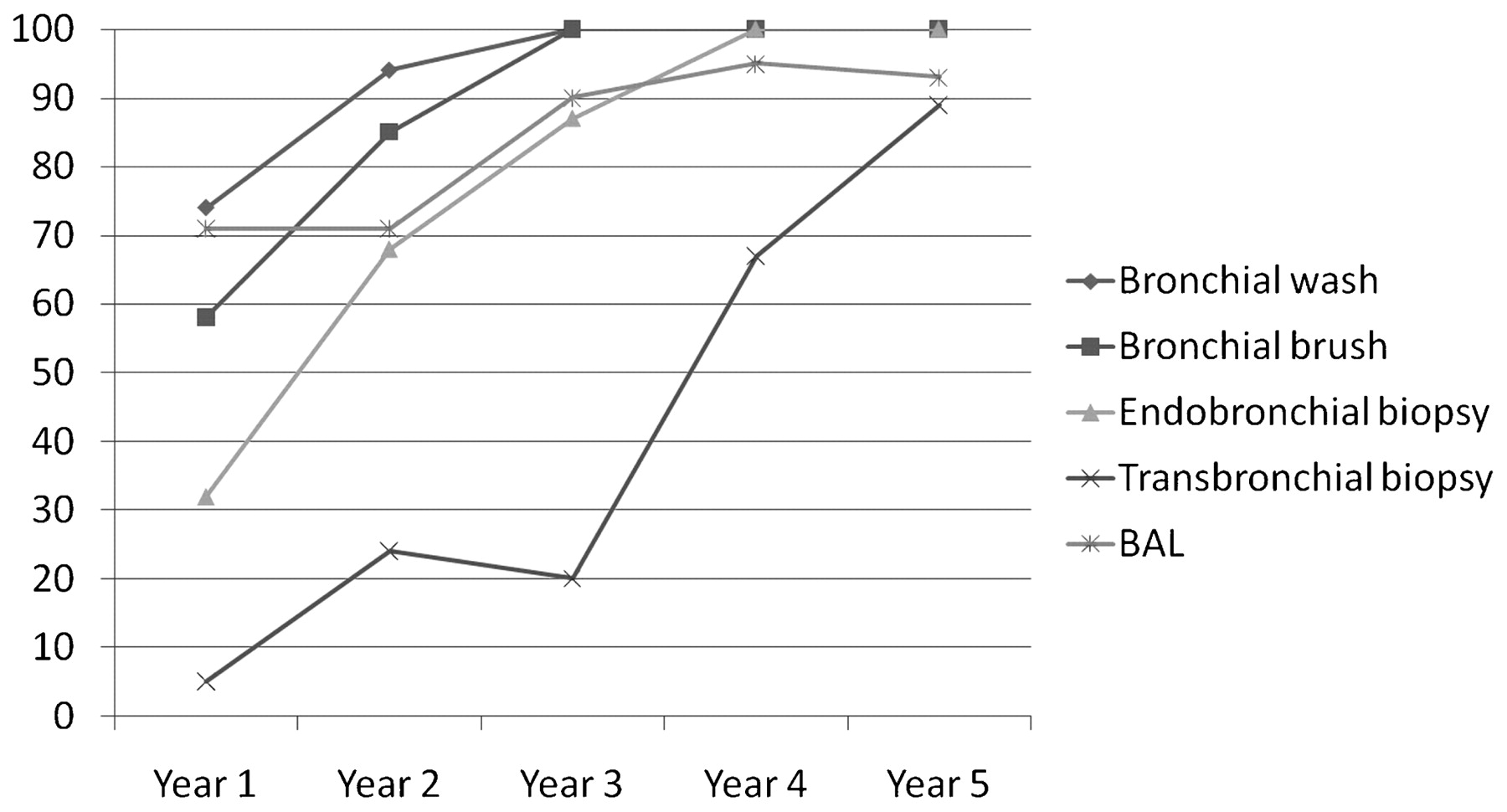
Results 224 replies represented 48% of potential recipients of the questionnaire. The majority of trainees (52%) were scheduled to attend one bronchoscopy list per week. Full shift rotas caused 46% trainees to miss at least one bronchoscopy list per month. The majority of trainees (88%) had performed 200 bronchoscopies by their fourth year. From the self-reported competency responses we were able to derive “learning curves” for various procedures by analysing competencies by the different years of SpRs in training. For bronchial lavage and brush, trainees feel competent after the second year; competency in more complex procedures takes longer (fig 1). Only 30% of trainees record their diagnostic rates for bronchoscopies. 68% of trainees are satisfied with their training in bronchoscopy. The opportunities to train in interventional bronchoscopy are limited and centred round specialist centres. Few trainees feel competent in interventional procedures at the end of training.

{kind=link}
{kind=link}
{kind=link}
Procedure competencies. Self-reported competencies for each year of training indicating “learning curves” for common procedures performed during bronchoscopy. The y-axis represents the percentage of trainees with 90% competency. The x-axis represents the completed years of training.
Conclusions We have found that, at the end of 5 years’ training, most trainees have obtained competency in all aspects of bronchoscopy apart from interventional procedures. There are clearly learning curves for each individual aspect of bronchoscopy; the more complex the procedure, the longer it takes to be competent. From our survey it appears that the full 5 years’ training and 200 bronchoscopies are needed for self-reported competency. Interventional bronchoscopy training will need to be restructured to ensure competent interventional bronchoscopists in the future. This survey has important implications for the training recommendations for current and future SpRs in respiratory medicine.
P206 SELF-MANAGEMENT IN ASTHMA AND COPD
I. Younis, N. J. Roberts, M. R. Partridge. Imperial College, London, UK
Background Self-management (SM) improves outcome in long-term conditions. SM is strongly recommended in asthma guidelines. In chronic obstructive pulmonary disease (COPD) the evidence in favour is increasing. Use is poorly implemented in asthma with only a few studies as to why. Less is known about healthcare professionals views’ about SM in COPD.
Methods A questionnaire study of healthcare professionals views’ on SM plans in asthma and COPD was sent to respiratory SpRs and consultants in North London and a GP+nurse in 31 GP practices in one PCT. This abstract summarises the quantitative results.
Results 54/176 questionnaires were returned from 18/55 GPs, 13/41 nurses, 13/63 SpRs and 10/17 consultants. Over 90% of respondents agreed/strongly agreed with the British asthma guideline recommendation on SM. Two-thirds occasionally and 10% never issued action plans. Respondents reported discussing SM with 76% of their patients. GPs estimated that 34% of patients received plans; consultants estimated the highest (70%). 90% believed that patients should receive a plan during a hospital admission. 25% of doctors reported undertaking SM education with patients compared with 61.5% of nurses. 80% occasionally/never asked to see a patient’s plan which they had not issued. 52% believed they had witnessed improved outcomes using SM, of which 75% always/sometimes gave plans to patients. Nurses most commonly issued asthma plans (61.5%) compared with SpRs (38.5%) and GPs (27.8%). Overall, 18/54 (33%) of respondents felt they lacked confidence constructing an asthma plan, of which 8/18 (44%) were GPs and 6/18 (33%) were nurses. 80% of respondents strongly/agree with NICE recommendation on SM in COPD but 40% did not feel plans were as valuable as in asthma. 54% discussed COPD SM with patients. Respondents believed 40% of patients received COPD plans with higher levels reported by consultants (67%). Again nurses issue most of the plans (69.2% vs 61.5% in asthma), but GPs were more involved in SM in COPD (50%) than in asthma (33.3%).
Conclusions Despite strong support for guideline recommendation, implementation was patchy. Consultants reported greater involvement but, overall, nurses were the most likely to give action plans. A third lack confidence in completing an action plan. In COPD there was greater GP involvement.
P207 DECLINING RESPIRATORY CLINICAL ACADEMICS: A MODEL FOR REVERSING THE TREND?
O. S. Usmani, E. M. Watson, S. N. Meah, M. E. Hodson, J. A. Mitchell. National Heart and Lung Institute, Imperial College London, London, UK
Introduction Recent publications reinforce the crisis in both respiratory1 and cardiovascular2 academic medicine that will threaten future clinical research. Attracting young clinicians forms a cornerstone in reversing the decline in academia.3 The National Heart and Lung Institute (NHLI) at Imperial College London is a leading postgraduate research centre in Europe committed to research, development and education in heart and lung medicine.
Objectives We have established a clinical research fellows training initiative (CRFTI) to attract, encourage and support clinical trainees interested in undertaking postgraduate research. The CRFTI aims to (1) match potential fellows with appropriate supervisors to their research interests; (2) support the process of writing grant/fellowship applications; (3) advise on regulatory, intellectual, statistical and financial considerations; and (4) guide interview technique.
Methods We planned a session on “Higher Degrees” as part of the Respiratory Specialist Registrar NW Thames training programme. A pre-session questionnaire (Pre-Q) was sent to all trainees in order to tailor the session to their needs. Questions asked whether trainees planned to do research, their reasons, advice they needed and, for those who had undertaken research, what advice they would give. Pre-Q informed us to direct initial talks on funding opportunities, choosing supervisors, deanery issues and job prospects. Feedback was undertaken with a post-session questionnaire (Post-Q) to guide future talks and role of CRFTI.
Results 18/44 trainees (41%) responded to the Pre-Q where 39% (7/18) had previously undertaken and 62% (11/18) were planning research. Responses are grouped into themes listed by the number of times cited (table 1).
Conclusions Trainees require the necessary information at an early stage of their career to provide them with an informed decision to undertake research. Importantly, following our session, several trainees were considering undertaking research having previously felt they lacked “academic capability”. The CRFTI is actively supporting 9/34 attending trainees (26%) towards research fellowships and will develop a website resource. We hope the initial experiences of our focused initiative may be a helpful model for other academic institutions to consider.
Details on CRFTI/questionnaires are available from o.usmani@imperial.ac.uk (Respiratory Lead) and emma.watson@imperial.ac.uk (Research Manager).
P208 UK RESPIRATORY TRAINEES’ VIEWS ABOUT IMPLEMENTING E-LEARNING INTO POSTGRADUATE TRAINING
S. F. Smith, N. J. Roberts, M. R. Partridge. Imperial College, London, UK
Background We have previously shown good acceptance of e-learning by undergraduates but more guarded acceptance by those in the first 3–4 years after graduation. This study specifically investigates respiratory SpRs’ views about implementing e-learning into their postgraduate education.
Methods Semi-structured telephone interviews with specialist respiratory registrars were undertaken to discuss their views about medical postgraduate training and e-learning. Calls were recorded and interviews transcribed and themed.
Results 13 trainees took part (age 34±3 years; 11F, 2M). Ten (77%) were British medical school graduates and 6 (46%) graduated before 2000. All of the trainees stated that they had either minimal or no exposure to e-learning as undergraduates. All had internet access at home and 10 (77%) used the internet for educational purposes for 2–4 h per week. Three (23%) downloaded educational material to an iPod and 46% spent 2–4 h updating their knowledge per week. Nine (69%) thought that e-learning should be embedded into the training programme, although some suggested that initial piloting and training were required. Responses were varied (0–50%) when asked how many training days could be replaced by e-learning. Maintaining the social interaction of training days was emphasised, and need to use the full teaching day without gaps was highlighted. The ideal length of an e-module was thought to be <2 h (54%). Five (38.5%) suggested 2–4 h, but dependent on the topic and whether users could interrupt the module without loss. Nine (69%) thought that e-modules should be a compulsory component of postgraduate certification and, if this was put in place, 12 (92%) would complete the modules at home. Lack of free uninterrupted study time made e-learning difficult to complete at work. Specific diseases, bronchoscopic anatomy, physiology, lung function, radiology and interpretation of results were suggested as areas which would lend themselves to delivery via e-learning.
Conclusions Overall, postgraduates seem receptive to the positive benefits of using e-learning as part of their postgraduate training. However, the social interaction and face-to-face teaching on study days were highlighted as important. Most were willing to undertake e-learning in their own time, but as an adjunct rather than a replacement for training days.