Article Text

Statistics from Altmetric.com
P131 MODELLING THE IMPACT OF INHALED DRUG PARTICLE SIZE OF SALBUTAMOL ON BRONCHODILATOR RESPONSE USING ARTIFICIAL INTELLIGENCE
1M. de Matas, 1Q. Shao, 2M. Biddiscombe, 3H. Chrystyn, 2P. J. Barnes, 1O. S. Usmani. 1Institute of Pharmaceutical Innovation, University of Bradford, Bradford, UK, 2Imperial College London and Royal Brompton Hospital, London, UK, 3School of Pharmacy, University of Huddersfield, Huddersfield, UK
Introduction We have previously shown that artificial neural networks (ANN) can be used to generate in vitro-in vivo correlation (IVIVC) models to predict the bronchodilator response (BR) to inhaled salbutamol (SB) delivered by polydisperse aerosols from dry powder inhalers and nebulisers in asthmatic subjects.1 BR was highly dependent on aerodynamic drug particle size (APS).
Objectives ANN software was therefore used in this study to model in vitro and in vivo data from 18 mild-moderate asthmatics receiving monodisperse (uniform drug particle sizes) SB aerosols of 1.5, 3 and 6 μm MMAD in a cumulative dosing schedule of 10, 20, 40 and 100 μg.2 The intention of this strategy was to explore the impact of APS on BR using accurate clinical aerosol science data and construct a model able to predict in vivo clinical outcomes in individual patients.
Methods Input variables to the model were APS, body surface area (BSA), age, pre-treatment forced expiratory volume in 1 s (FEV1)%predicted, forced vital capacity (FVC), cumulative emitted drug dose and bronchodilator reversibility to SB 200 μg metered dose inhaler (REV). These factors were used by the model to predict the BR (%ΔFEV1) at 10 (T10) and 20 (T20) min after receiving each of the four doses for each particle size. Predictability of the model was assessed using unseen data.
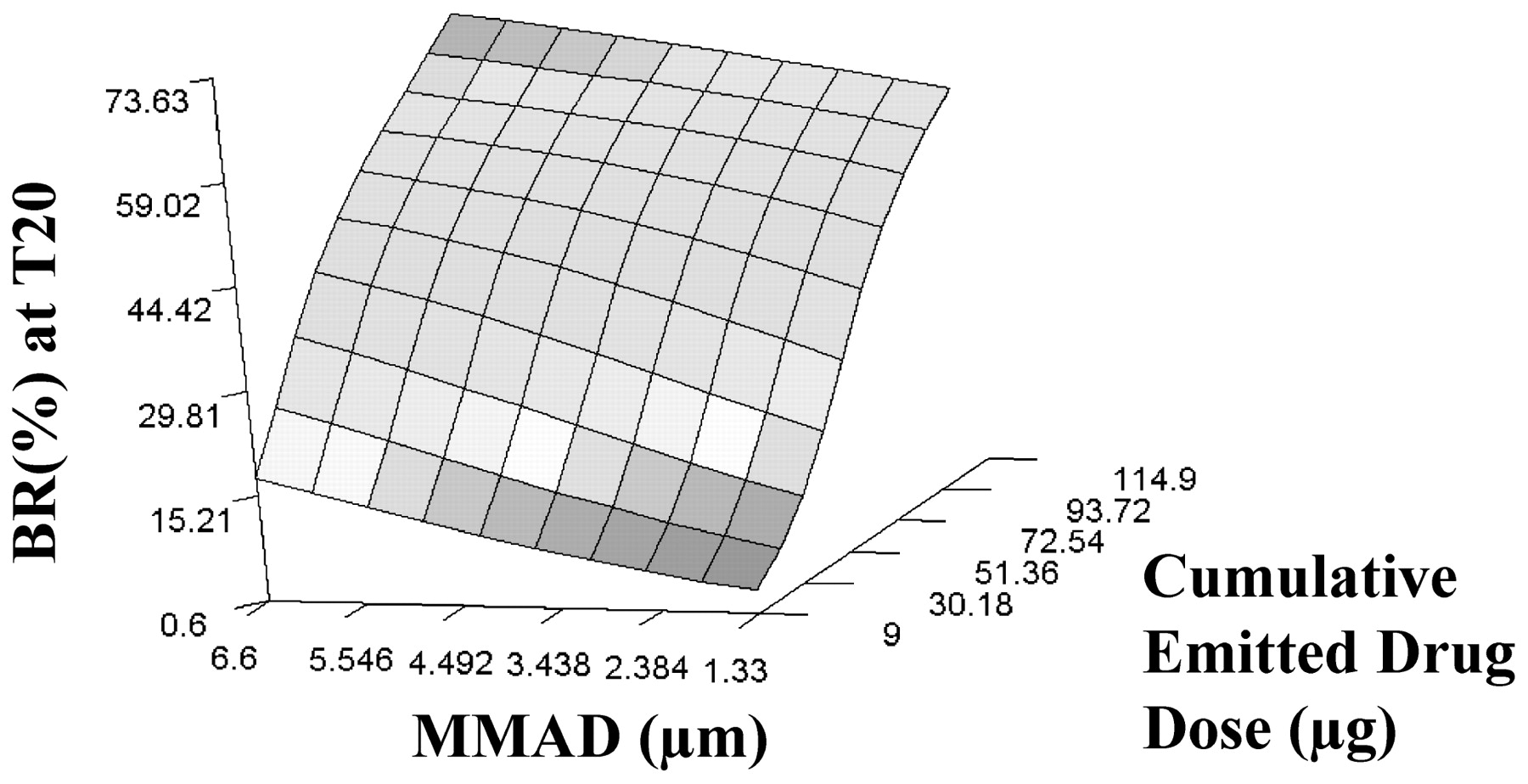
Results Generated models reliably predicted in vivo performance (BR) in individual subjects with coefficients of determination (R2) ⩾0.8. The average error between predicted and observed BR for individual subjects (unseen data) was <4.5% across the cumulative dosing regimen. Increases in APS and drug dose gave improved BR (%ΔFEV1) (fig 1). Models showed trends towards improved response in younger patients and those having greater REV.

{kind=link}
Response surface plot showing typical relationships between aerodynamic particle size (MMAD) and cumulative emitted drug dose on bronchodilator response (BR) at 20 min after inhalation (T20) of monodisperse aerosols.
Conclusions ANN models were able to accurately predict the in vivo BR for inhaled monodisperse SB aerosols in individual patients from knowledge of APS, drug dose and subject characteristics. These data confirm our previous findings that APS can be used to discriminate predictably between aerosols giving different BR. ANN therefore have the potential to be applied across a range of inhaled drugs to generate IVIVC models, thus limiting human and animal experiments.
P132 IN VITRO VALIDATION OF RADIOLABELLED INHALED CORTICOSTEROID FOR IN VIVO LUNG DELIVERY USING GAMMA SCINTIGRAPHY
1M. F. Biddiscombe, 2S. Meah, 3R. Sadler, 2P. J. Barnes, 2O. S. Usmani. 1Nuclear Medicine, Royal Brompton Hospital and National Heart and Lung Institute, Imperial College London, London, UK, 2Airways Disease Section, Royal Brompton Hospital and National Heart and Lung Institute, Imperial College London, London, UK, 3GlaxoSmithKline, Ware, UK
Introduction Gamma scintigraphy (GS) of the lungs can considerably enhance our knowledge of the deposition of inhaled drug aerosols in vivo. Most lung deposition studies use polydisperse aerosols (aerosols produced from current clinical inhaler devices) that deliver a coarse spray of particles with many different sized drug particles, which are unable to accurately investigate the relationship between clinical airway effects and inhaled drug particle size. Monodisperse aerosols are a fine mist formulation comprising drug particles of uniform size that enable the precise regional airways targeting of inhaled drug within the lungs and allow detailed investigation of the effects of drug particle size.
Objectives We describe a method to “tag” monodisperse fluticasone propionate (FP) aerosols using radiolabel (Tc-99m) and determine in vitro whether FP and Tc-99m were correctly matched for different drug particle sizes using an Andersen Cascade Impactor (ACI).
Methods FP nebules were mixed with ethanol and Tc-99m and delivered to a Spinning Top Aerosol Generator to generate radiolabelled monodisperse aerosols. FP aerosols of particle size 1.5 μm, 3 μm, 6 μm MMAD were sampled using an ACI at an inhaled flow of 28 l/min. Radioactive counts were measured using a gamma camera. FP drug concentration was determined using HPLC.
Results Percentage FP deposition and radioactive counts (R) were well matched on all ACI stages (particle size ranges given) for the three monodisperse aerosol distributions (table 1, N = 3 experiments each). The ratios of FP%/R% were constant on each ACI stage (particle size range) for each monodisperse aerosol size.
Conclusions Our in vitro experiments show monodisperse FP drug aerosols can be successfully radiolabelled and that the radiolabel does not alter the particle size distribution of the drug formulation. This validation allows for future precise in vivo scintigraphic investigations, using monodisperse aerosols, of the perceived clinical importance of targeting inhaled corticosteroid formulations to different lung regions in different disease states and severities.
P133 IMPLICATIONS OF NOT WELL-CONTROLLED ASTHMA: UK RESULTS FROM A EUROPEAN SURVEY
1J. Foo, 2L. Rice, 2K. Annunziata, 1G. D. Castillo. 1GlaxoSmithKline, Paris, France, 2Consumer Health Sciences International, Princeton, USA
Introduction and Objectives A European patient survey in 2006 showed that the majority of treated asthma patients (55%) are poorly controlled.1 A 2008 survey2 aimed to reassess the level of asthma control in Europe. We investigated if asthma control in the UK had improved and the implications for patients and clinicians of rescue use of ⩾2 puffs/week.
Methods A detailed population-based cross-sectional survey carried out in 2008 in France, Germany, Italy, Spain and UK was administered to a sample of individuals drawn from an internet panel. The Asthma Control Test (ACT)3 was used to assess level of control: at least well-controlled (ALWC) asthma (score 20–25) and not well-controlled (NWC) asthma (score ⩽19). The SF-12 questionnaire was used to assess health-related quality of life.
Results Of 15 000 UK respondents, 1523 were diagnosed asthma patients (mean age 45.3 years). 1362 (89.4%) of asthma respondents were receiving treatment for asthma. Of these, 697 (51.2%) were NWC in 2008 compared with 45% in 2006.1 590 (84.7%) of the NWC patients used rescue medication ⩾2 puffs/week. Table 1 compares NWC and ALWC patients.
Conclusions The level of asthma control in the UK has not improved since 2006.1 NWC patients experienced significantly more night-time awakenings and visited their physician more frequently than those with ALWC asthma. Furthermore, these patients were less able to perform physical (eg, housework, sports) and social activities. This survey suggests that rescue medication use of ⩾2 puffs/week is a useful way of identifying NWC patients for further assessment (eg, using validated tools such as ACT) to ensure that these patients are optimally managed and treated according to BTS/SIGN guidelines, with the goal of improving quality of life and asthma control in the UK.
Asthma Control Test is a trademark of QualityMetric Inc. GlaxoSmithKline purchased the survey data from Consumer Health Sciences International.