Article Text

Abstract
Background: Epidemiological studies suggest that dietary intake of vitamins A, C and E may be associated with the occurrence of asthma. A systematic review and meta-analysis was conducted in accordance with MOOSE guidelines to determine whether vitamins A, C and E, measured as dietary intakes or serum levels, are associated with asthma.
Methods: MEDLINE, EMBASE, CINAHL, CAB abstracts and AMED (up to November 2007), conference proceedings and bibliographies of papers were searched to identify studies of asthma, wheeze or airway responsiveness in relation to intakes and serum concentrations of vitamins A, C and E. Pooled odds ratios (OR) or mean differences (MD) with 95% confidence intervals (CI) were estimated using random effects models.
Results: A total of 40 studies were included. Dietary vitamin A intake was significantly lower in people with asthma than in those without asthma (MD −182 μg/day, 95% CI −288 to −75; 3 studies) and in people with severe asthma than in those with mild asthma (MD −344 μg/day; 2 studies). Lower quantile dietary intakes (OR 1.12, 95% CI 1.04 to 1.21; 9 studies) and serum levels of vitamin C were also associated with an increased odds of asthma. Vitamin E intake was generally unrelated to asthma status but was significantly lower in severe asthma than in mild asthma (MD −1.20 μg/day, 95% CI −2.3 to −0.1; 2 studies).
Conclusions: Relatively low dietary intakes of vitamins A and C are associated with statistically significant increased odds of asthma and wheeze. Vitamin E intake does not appear to be related to asthma status.
Statistics from Altmetric.com
Diet has been widely implicated in the aetiology of cardiovascular disease1 2 and other disorders, but the role of diet in the aetiology of respiratory diseases is less clearly defined. Over the past 15 years many observational epidemiological studies have reported associations between diet and asthma, and particularly for the antioxidant vitamins A, C and E. However, randomised controlled trials of vitamin supplementation in asthma thus far have been inconclusive.3–6 In view of this apparent inconsistency between the observational and experimental data,7 we have attempted to determine the magnitude of the overall associations of these vitamins estimated by the observational studies by carrying out a systematic review and meta-analysis to provide pooled quantitative estimates of the likely magnitude of the effect of dietary intake and blood levels of antioxidant vitamins on a range of measures of asthma and asthma severity.
METHODS
Systematic review methods
A comprehensive search of the MEDLINE (1950 to November 2007), EMBASE (1980 to November 2007), CINAHL (1982 to November 2007) and AMED (1985 to November 2007) was conducted to identify all published comparative epidemiological studies assessing the relation between antioxidant vitamins and asthma status. Search terms were selected under guidance from the Centre for Reviews and Dissemination and the Airways Group Specialist search terms.8 Reference lists from identified relevant studies and previous reviews were scanned and checked for further studies. Abstracts were identified through searching CAB abstracts database (1973 to November 2007) and American Thoracic Society conferences (2003–2007). No language restrictions were applied.
The exposures of interest were measures of dietary intake or of objective levels of vitamins in body fluids of the antioxidant vitamins A, C and E. The primary outcome measure used was asthma (physician-diagnosed, self-reported physician-diagnosed or defined as exercise-induced bronchospasm/constriction); secondary outcomes included wheeze, airway reactivity and asthma severity. Studies using spirometry or symptoms of cough and breathlessness as their main outcomes were excluded as these outcomes are likely to be relatively non-specific to asthma.
Two authors (SA and JL-B) reviewed the titles and then the abstracts, excluding irrelevant papers after each stage. Disagreements were resolved by discussion. The full text of the remaining papers was sought and the following exclusion criteria applied: reviews, duplicated studies, those without relevant outcomes and those in which no quantitative results or p values were presented, inability to source the text. Included studies were assessed for methodological quality using the Newcastle-Ottawa Scale for Quality Assessment (NOS).9 The median score of 6 was used to distinguish moderate and high quality studies from poorer quality studies.
Statistical analysis
Data were extracted independently by two authors (SA and JL-B). Dichotomous outcomes are presented as odds ratios (OR) with 95% confidence intervals (CI) and continuous outcomes are presented as mean differences (MD) with 95% CI. Conversions of biochemical units of measurement for the exposures were performed where necessary to allow for comparisons of units across studies.10 Where exposure was expressed in quantiles, vitamin levels are expressed as high or low, typically representing a comparison of the lowest with the highest exposure categories.
Meta-analyses were performed to calculate weighted effect measures across studies using random effects models. Heterogeneity between the studies was assessed using I2,11 and if levels of heterogeneity (I2 >75%) existed, then meta-analyses were not performed. Subgroup analyses relating to methods of asthma diagnosis, adult versus children and methodological quality of the studies were conducted to explore reasons for moderate levels of heterogeneity (I2 >50%). Analysis was performed using Review Manager 4.2.9 (Version 4.2 for Windows, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2003); p values <0.05 were considered statistically significant. The systematic review was carried out in accordance with the MOOSE guidelines.12
RESULTS
Overview of included studies
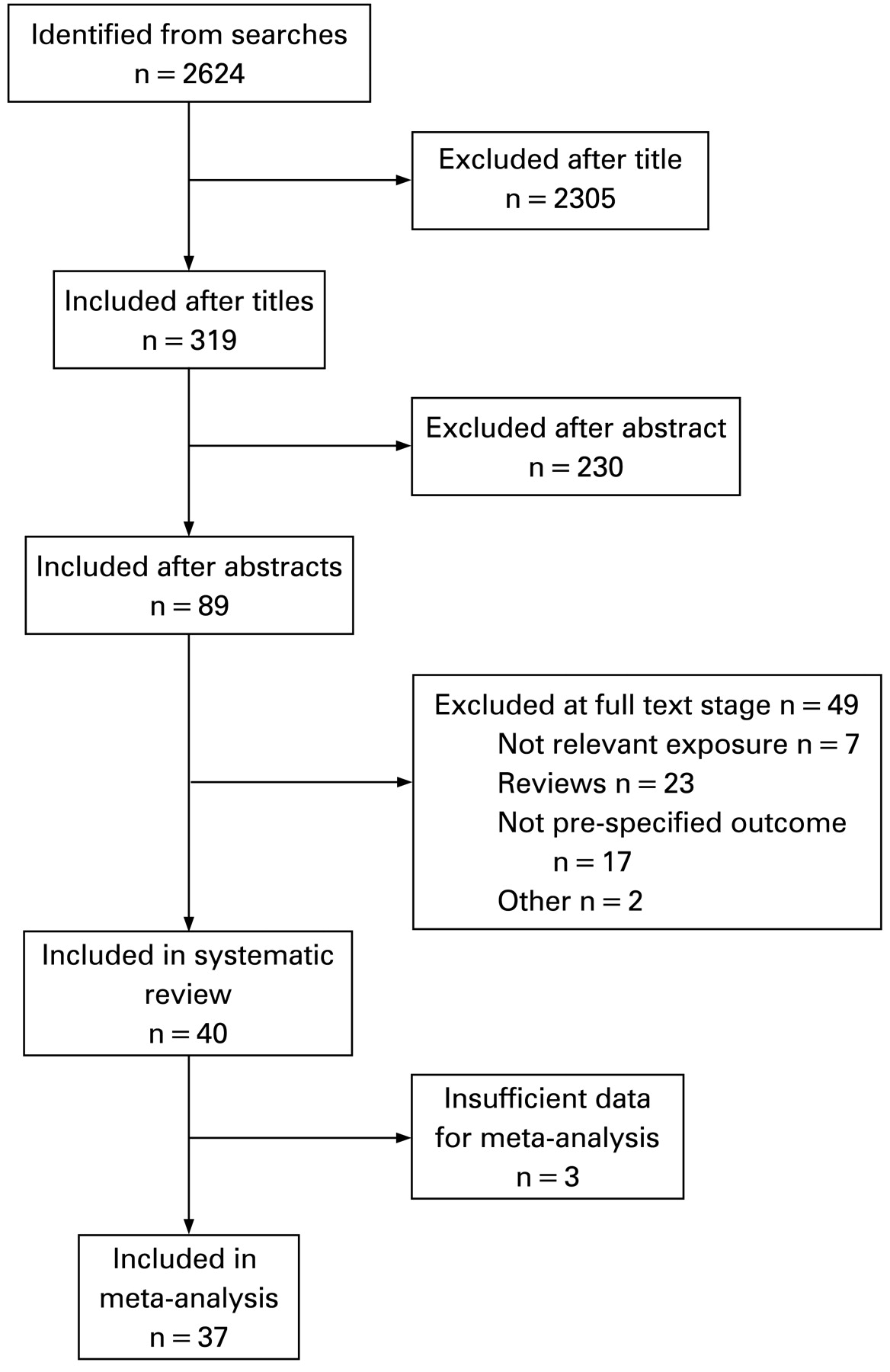
From an initial 2624 papers and abstracts identified from the literature searches, 89 had potentially eligible abstracts and 40 met the selection criteria (table 1, fig 1). Twenty-three of these assessed asthma as an outcome,13–35 9 assessed wheeze,36–44 5 assessed both asthma and wheeze,45–49 2 assessed airway reactivity50 51 and 1 assessed both asthma and airway reactivity.52 Twenty-six of the papers studied the effects of measures of dietary intake;16–19 23 25 27 29 31 32 34–38 40–45 47 49–52 23 studied biochemical levels in serum or plasma13–15 17 18 20 21 23 24 26–28 30 31 33 34 36 37 39 42 46 48 50 and 1 assessed the effects of antioxidant levels in sputum.22 Further information about the individual studies is presented in the online supplement.

Flow chart for identifying studies.
Methodological quality of the studies
The NOS scores for the 40 studies ranged from 3 to 9, with a median of 6; 26 of the 40 studies (65%) were scored as being of moderate or high level (⩾6) methodological quality.
Dietary intake and serum levels of vitamin A
Overall, 21 papers reported the association of vitamin A or its components on one or more of the outcome measures,15–18 24 25 27–29 31 35 36 38–40 48 51 52 of which 11 papers assessed exposure to vitamin A,15–17 19 20 24 34 36 39 43 45 10 assessed β-carotene,17 18 25 31 36 38 39 48 51 52 2 assessed α-carotene,17 18 6 assessed retinol25 28 36 40 51 52 and 4 assessed carotene.29 31 35 40 The results for β-carotene, α-carotene, retinol and carotene are presented in the online supplement.
Asthma as the outcome
Self-reported dietary intake was significantly reduced in asthma by 182 μg/day (95% CI −288.42 to −75.25; I2 = 0%; 3 studies; fig 2). Pooled serum levels were also reduced in asthma (4 studies; all high quality and ascertained asthma using physician diagnosis), though not to the point of statistical significance (by 0.17 μmol/l (95% CI −0.36 to 0.02); I2 = 59%; fig 2). However, the direction of the association seemed to differ between adults and children, with pooled serum levels being significantly reduced in the two studies in children (MD −0.25 μmol/l, 95% CI −0.40 to −0.10; fig 2).

Dietary intake (μg/day) and serum levels (μmol/l) of vitamin A and asthma. Mean differences relate to the difference in mean dietary intakes or serum levels of vitamin A. Squares are the difference in means between people with asthma and those without asthma, and bars represent 95% confidence intervals (CI). Negative mean differences indicate lower levels seen in subjects with asthma than in those without asthma. Arrows on the end of bars indicate that the limits are beyond the scale presented.
Asthma severity as the outcome
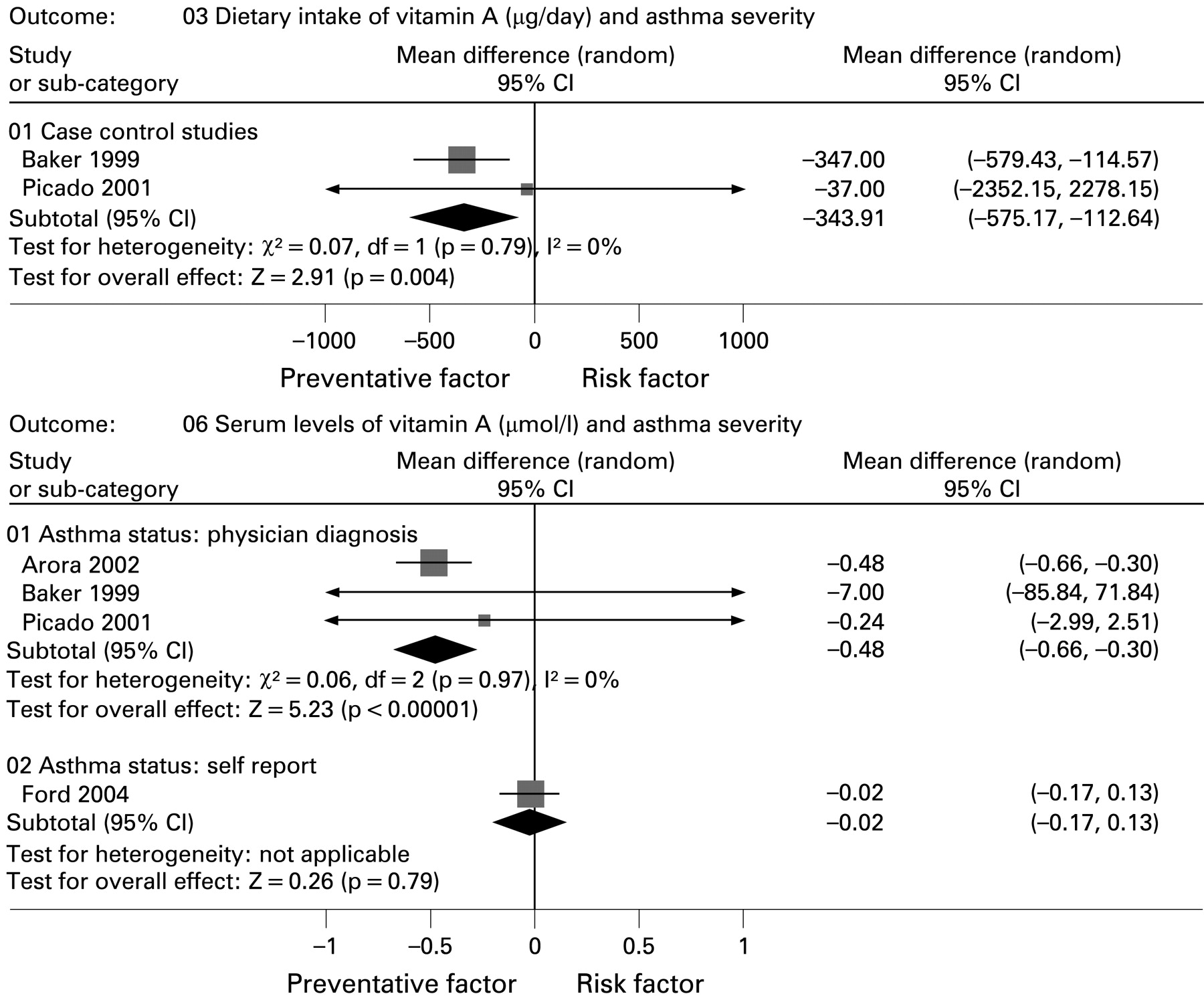
Cases of severe asthma had significantly lower dietary intakes of vitamin A (MD −344 μg/day (95% CI −575.17 to −112.64; I2 = 0%; 2 studies; fig 3) than cases of mild disease. Results of the four studies assessing serum levels showed extreme heterogeneity (I2 = 80%) so a pooled analysis was not carried out; however, a subgroup analysis suggested that physician-diagnosed cases of severe asthma (all studies of lower quality and conducted in adults) had significantly lower serum levels of vitamin A (MD −0.48 μmol/l, 95% CI −0.66 to −0.30; I2 = 0%; 3 studies; fig 3) than cases of mild disease. No relation was seen for self-reported severity of asthma (all conducted in children and of higher quality) (MD −0.02, 95% CI −0.17 to 0.13; 1 study; fig 3).
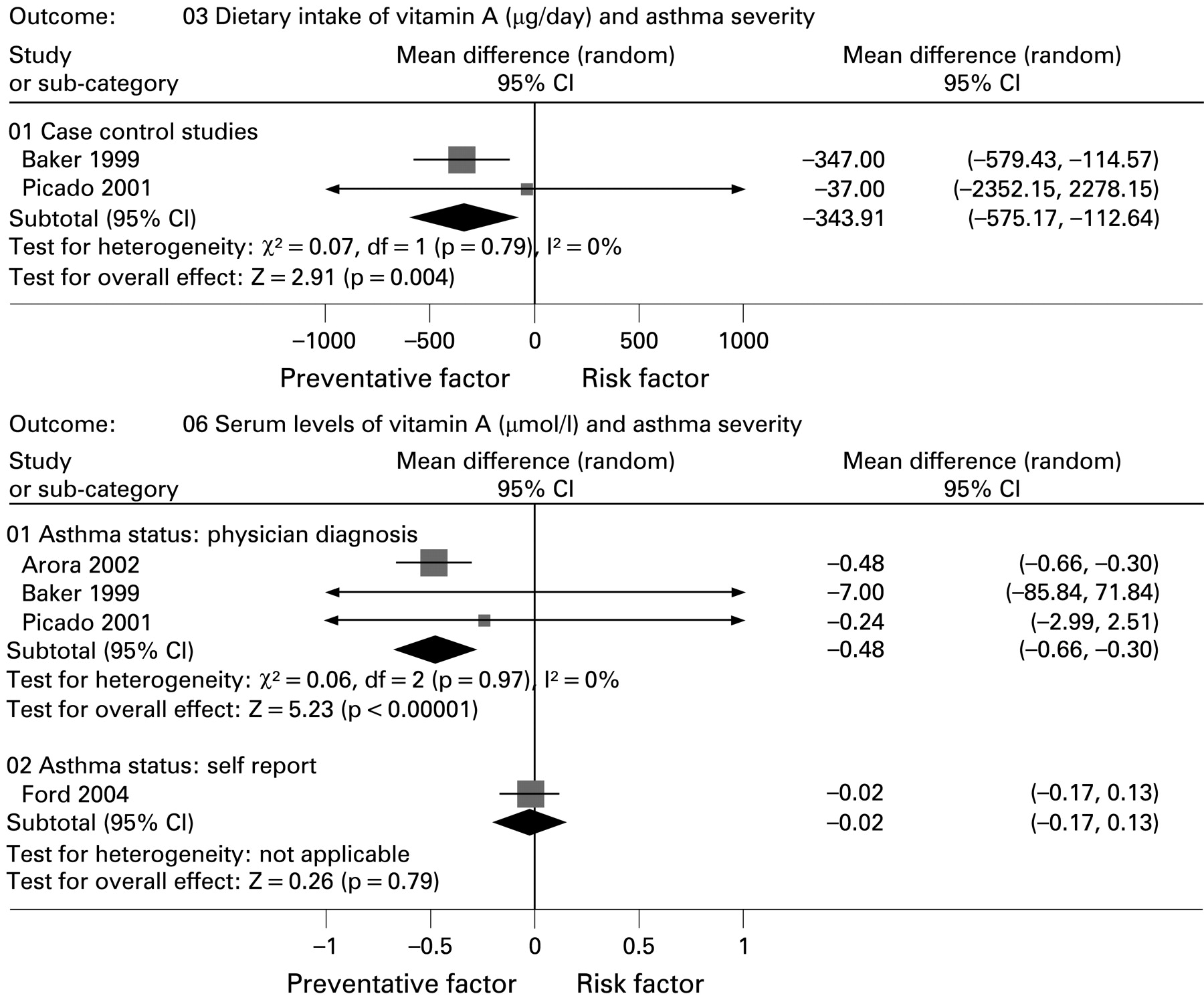
Dietary intake (μg/day) and serum levels (μmol/l) of vitamin A and asthma severity. Mean differences relate to the difference in mean dietary intakes or serum levels of vitamin A. Squares are difference in means between people with severe asthma and those without severe asthma, and bars represent 95% confidence intervals (CI). Negative mean differences indicate that lower levels are seen in people with severe asthma than in those with mild asthma. Arrows on the end of bars indicate that the limits are beyond the scale presented.
Wheeze as the outcome
Although no association was seen between low dietary intakes of vitamin A and wheeze (OR 0.58, 95% CI 0.29 to 1.16; 1 study), low serum levels were significantly associated with a 24% decreased odds of wheeze (95% CI 0.63 to 0.92; 1 study).
Airway reactivity as the outcome
No significant associations were seen for total dietary intake of vitamin A (MD 0.02, 95% CI −0.08 to 0.12 per doubling intake).43
Dietary intake and serum levels of vitamin C
A total of 32 papers reported the association with vitamin C.13 14 16 17 19 21–23 25 27–30 32–43 45–49 51 52
Asthma as the outcome
Low levels of dietary vitamin C intake were associated with a significant increase in the relative odds of asthma (OR 1.12, 95% CI 1.04 to 1.20; I2 = 0%; 9 studies; fig 4). Meta-analysis of studies reporting serum vitamin C levels and the odds of asthma was not carried out because of extreme levels of heterogeneity (I2 = 94%; 2 studies; both studies were of moderate to high quality and used self-reported asthma diagnosis); however, individual studies showed that low levels of serum vitamin C were associated with increased odds of asthma (OR 1.01, 95% CI 1.00 to 1.02 per 1 μmol/l increase;35 OR 1.22, 95% CI 1.11 to 1.33).48

Dietary intakes (mg/day) of vitamin C and asthma. Odds ratios relate the ratio of odds of low dietary levels of vitamin C in people with asthma compared with those without, and bars represent 95% confidence intervals (CI). Odds ratios <1 indicate that lower dietary levels of vitamin C are seen in people with asthma than in those without asthma. Arrows on the end of bars indicate the limits are beyond the scale presented.
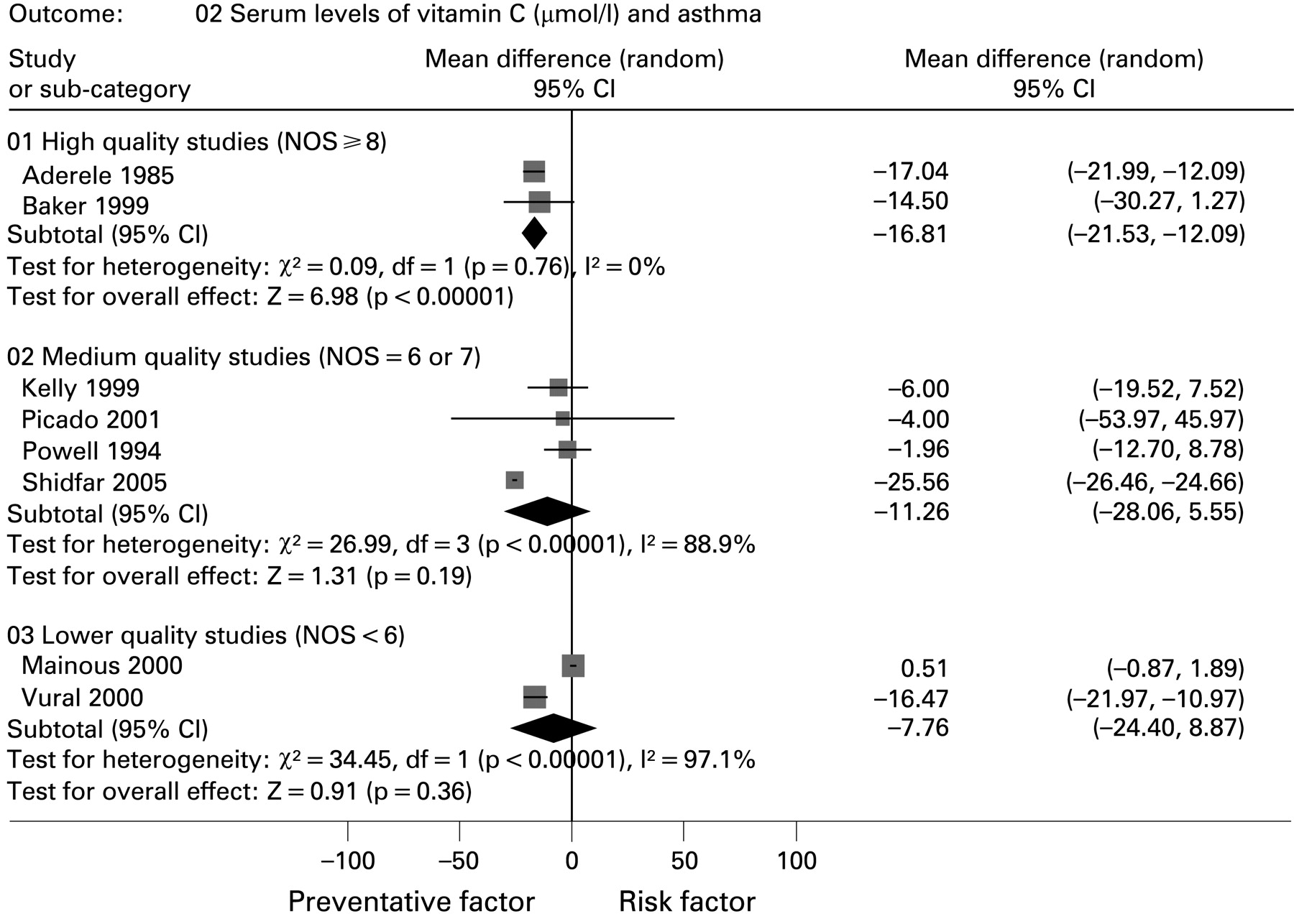
The mean dietary intake of vitamin C was not significantly different in people with asthma compared with those without asthma (MD −8.62 mg/day, 95% CI −19.77 to 2.53; I2 = 19%; 5 studies). Pooled analyses of mean serum levels of vitamin C and asthma status could not be performed owing to high levels of heterogeneity (I2 = 100%; 9 studies), primarily relating to one study14 in which extremely high levels of vitamin C were seen in the control group (mean 272.54 μmol/l). A sensitivity analysis restricted to high-quality studies (NOS ⩾8) excluded this finding14 and revealed that people with asthma had mean serum levels that were significantly lower (by 16.8 μmol/l, 95% CI −21.5 to −12.1; I2 = 0%; 2 studies), while non-significant reductions were seen in moderate and lower quality studies (fig 5). Subgroup analyses based on age (adult: I2 = 99.5%, 6 studies; children: I2 = 84%, 2 studies) and method of asthma ascertainment (physician-diagnosed: I2 = 88%, 6 studies; self-reported: 1 study; unknown method: 1 study) indicated that these factors did not explain any of the observed heterogeneity.

Serum levels (μmol/l) of vitamin C and asthma. Mean differences relate to the difference in mean serum levels of vitamin C. Squares are differences in mean between people with asthma and those without asthma and bars represent 95% confidence intervals (CI). Negative mean differences indicate that lower levels are seen in people with asthma than in those without asthma. Arrows on the end of bars indicate the limits are beyond the scale presented.
Asthma severity as the outcome
Similar dietary intake (MD −16.13 mg/day, 95% CI −41.02 to 8.76, I2 = 0%; 2 studies) and serum levels (MD −5.41 μmol/l, 95% CI −14.17 to 3.35; I2 = 67%; 4 studies) of vitamin C were seen between severe and non-severe asthma.
Wheeze as the outcome
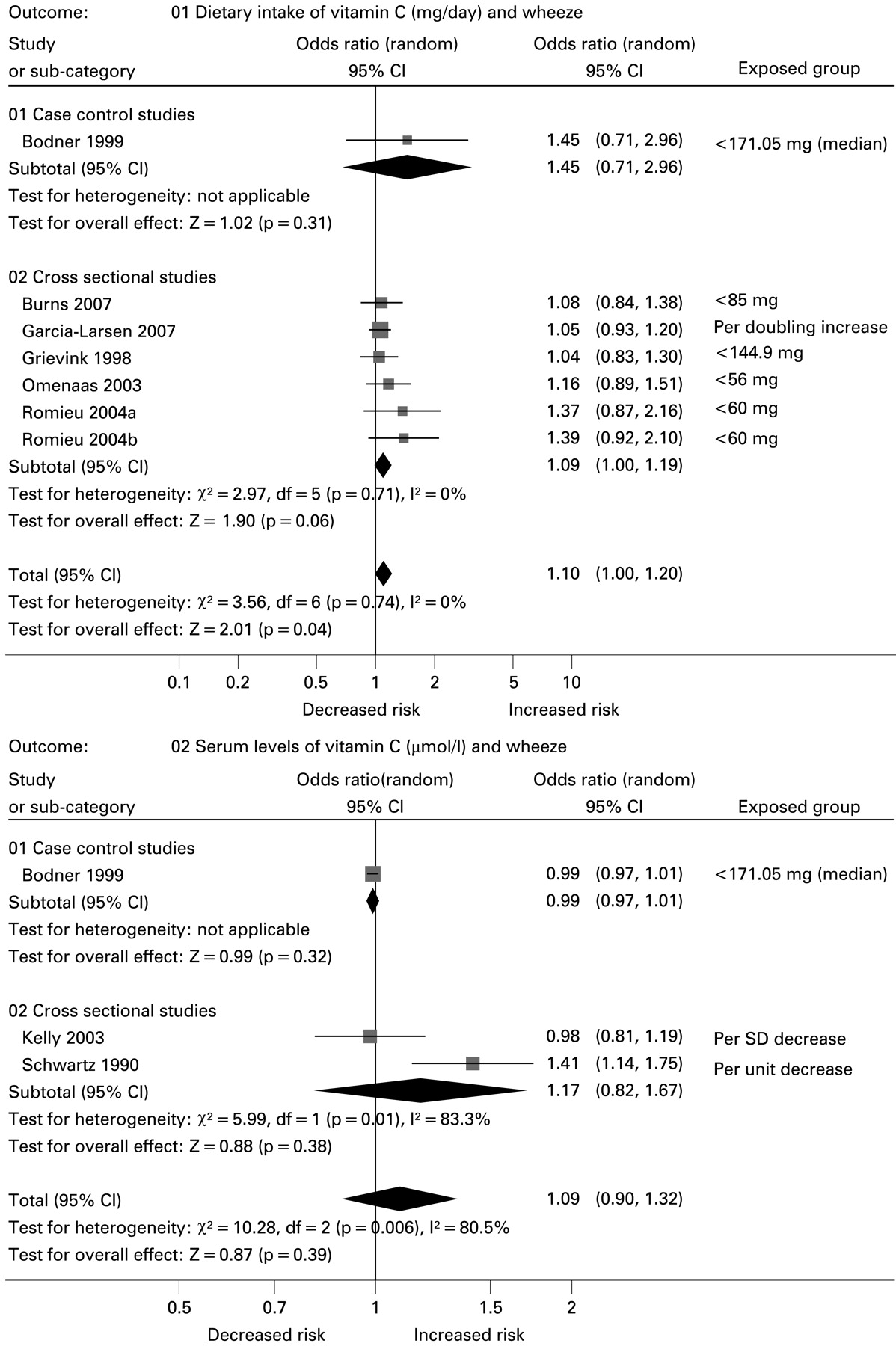
An increased odds of wheeze was associated with lower dietary intakes of vitamin C (OR 1.10, 95% CI 1.00 to 1.20; p = 0.04 I2 = 0%; 6 studies; fig 6). Extreme levels of heterogeneity were seen between the studies that assessed serum levels of vitamin C and the odds of wheeze (3 studies; I2 = 81%), therefore pooled analyses were not performed. All three studies were of moderate to high quality and assessed wheeze using self-reported questionnaire; however, a subgroup analysis based on age found that no effect was present in adults (OR 0.99, 95% CI 0.97 to 1.01; I2 = 0%; 2 studies), but a significant 41% increase in the odds of wheeze was seen in the study that included participants of all ages (95% CI 1.14 to 1.75).42 Additionally, mean dietary intake (MD 4.70 mg/day, 95% CI −26.6 to 36.0; 1 study) and mean serum vitamin C (MD 0.06 μmol/l, 95% CI −1.00 to 1.12; I2 = 0%; 2 studies) were similar in people with and without wheeze.
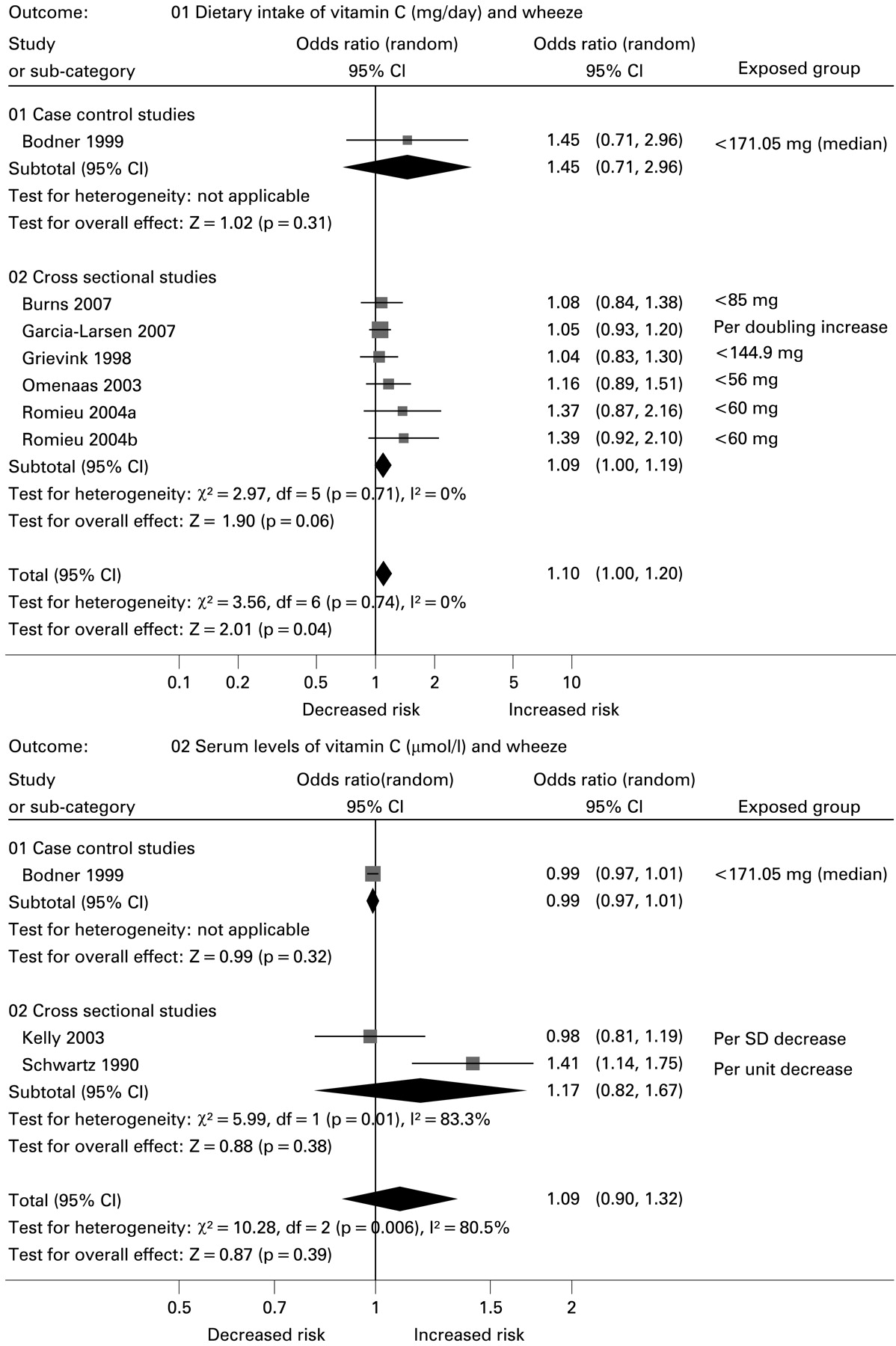
Dietary intake (mg/day) and serum levels (μmol/l) of vitamin C and wheeze. Odds ratios relate the ratio of odds of low dietary intake or serum levels of vitamin C in people with wheeze compared with those without, and bars represent 95% confidence intervals (CI). Odds ratios <1 indicate that lower levels of vitamin C are seen in people with wheeze than in those without wheeze. Arrows on the end of bars indicate the limits are beyond the scale presented.
Airway reactivity as the outcome
Three heterogeneous studies conducted in adults43 51 52 reported the relation between dietary intake of vitamin C and airway reactivity as measured using methacholine challenge. Two studies found evidence of a significant increase in airway reactivity with lower levels of vitamin C (OR 7.14; 95% CI 1.92 to 25.0;51 MD −0.12, 95% CI −0.22 to −0.03 per doubling in intake),43 but no association was seen in the other study (OR 1.04, 95% CI 0.76 to 1.43).52
Dietary intake and serum levels of vitamin E
Twenty-four studies reported the association with vitamin E levels,16 17 21 22 24 25 27–29 31 32 34–36 38–40 43–45 48 49 51 52 of which 4 assessed α-tocopherol in particular.21 28 31 36
Asthma as the outcome
Pooled analyses could not be performed to assess the relation between mean dietary intake (I2 = 81%; 5 studies) or mean serum levels (I2 = 90%; 6 studies) of vitamin E and asthma due to extreme heterogeneity. All of the studies that measured mean dietary intake of vitamin E were of moderate to high quality and conducted in adults, and therefore only subgroup analyses based on ascertainment of asthma status were conducted. Significantly lower mean levels of dietary vitamin E were associated with asthma in studies which used physician diagnoses (MD −1.91 mg/day, 95% CI −2.51 to −1.31; I2 = 0%; 4 studies; fig 7), however no effect was seen for self reported asthma status (MD −0.20 mg/day; 95% CI −0.72 to 0.32; 1 study; fig 7). All of the studies that measured serum levels of vitamin E were of high quality, so subgroup analyses based on age and ascertainment of asthma were conducted. Age did not explain the observed heterogeneity (adults: MD 3.12, 95% CI −2.53 to 8.76, I2 = 89%, 4 studies; children: MD 0.00, 95% CI −0.02 to 0.02, I2 = 0%; 2 studies), and no significant difference in mean serum vitamin E levels were seen with asthma in studies which used physician diagnoses (MD 0.10 μmol/l, 95% CI −1.17 to 1.37; I2 = 47%; 5 studies; fig 7). However, significantly increased levels of vitamin E were seen in the study which did not define asthma status (MD 9.10 μmol/l, 95% CI 6.34 to 11.86; 1 study; fig 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Dietary intakes (mg/day) and serum levels (μmol/l) of vitamin E and asthma. Mean differences relate to the difference in mean dietary intake or serum levels of vitamin E. Squares are differences in mean between people with asthma and those without asthma, and bars represent 95% confidence intervals (CI). Negative mean differences indicate that lower levels are seen in people with asthma than in those without asthma. Arrows on the end of bars indicate the limits are beyond the scale presented.
No relation was seen between the odds of asthma and lower dietary intakes of vitamin E (OR 1.23, 95% CI 0.90 to 1.69; I2 = 74%; 6 studies) or serum levels of vitamin E (OR 1.04, 95% CI 0.91 to 1.19; 1 study). All of the studies of the relation between dietary intake of vitamin E and the odds of asthma (6 studies) used self-reported ascertainment of asthma. A subgroup analysis of these studies showed a non-significant trend towards an increased odds of asthma with lower levels of dietary vitamin E (adults: OR 1.25, 95% CI 0.93 to 1.67; p = 0.13; I2 = 53%; 4 studies); however, studies were too heterogeneous for comparisons in children (I2 = 91%; 2 studies). A subgroup analysis based on quality of the studies did not explain any of the observed heterogeneity between the 6 studies (moderate to high quality: I2 = 84%, 3 studies; low quality: I2 = 63%, 3 studies).
Asthma severity as the outcome
Significantly lower dietary intake was seen in those with severe asthma (MD −1.20 μg/day, 95% CI −2.29 to −0.11; I2 = 0%; 2 studies) but there was no difference in mean serum levels (MD −0.34 μmol/l, 95% CI −3.79 to 2.94; I2 = 31.5%; 3 studies) compared with those with less severe disease.
Wheeze as the outcome
Similar levels of dietary intakes of vitamin E were seen in people with wheeze and those without (MD 0.80 μg/day, 95% CI −0.23 to 1.83; 1 study). No relation was seen between the odds of wheeze and lower serum levels (OR 1.08, 95% CI 0.88 to 1.30; 1 study) or lower levels of dietary intake (OR 0.90, 95% CI 0.68 to 1.20; I2 = 66%; 5 studies).
Airway reactivity as the outcome
No association was seen between the risk of airway reactivity and lower dietary intakes of vitamin E (OR 1.06, 95% CI 0.48 to 2.38; I2 = 39%; 2 studies; MD −0.08, 95% CI −0.26 to 0.09 per doubling intake; 1 study).
DISCUSSION
This systematic review and meta-analysis of the evidence on antioxidant vitamin intake and asthma status shows a consistent negative association between overall dietary vitamin A intake and the odds of asthma and severe asthma, although findings for wheeze were less consistent. The mean deficit of 182 μg vitamin A per day in people with asthma relates to 26% and 30% of the latest recommended daily intakes of vitamin A for men and women, respectively.54 Additionally, most of the studies assessing the association found mean levels of vitamin A in people with asthma were below the recommended daily intakes. Vitamin A intake was lower in people with severe asthma than in those with less severe asthma by the equivalent of about half the recommended daily amount (50% in men and 57% in women). The results for the specific types of vitamin A (retinol, α-carotene, total carotenoids and carotene) did not generally reach statistical significance at the 5% level; however, there was a tendency for increased serum β-carotene levels to be associated with reduced odds of asthma.
For vitamin C we found evidence of an increase of approximately 12% in the odds of asthma associated with lower levels of intake of vitamin C. Results from individual studies also suggested that mean serum levels tended to be lower in people with asthma. These findings were generally supported by the results for wheeze and airway reactivity; however, associations with asthma severity were not conclusive. Measures of vitamin E were, however, generally unrelated to asthma status, although significantly lower mean dietary intakes (by approximately 2 mg/day, about 20% of the daily recommended intake of vitamin E) were seen in studies of people with physician-diagnosed asthma.
These findings contrast with those of a recent meta-analysis of published studies55 which found no significant association between dietary antioxidant intake and asthma or lung function. However, this meta-analysis searched only for studies in adults published in English language journals and listed in only one electronic database, and the meta-analyses were based on a combined outcome of asthma or wheeze. The present study was conducted with higher methodological rigor, in accordance with the MOOSE guidelines,12 used more comprehensive sources and search strategies and, where possible, validated search terms.8 56 57
One concern relating to our analysis is that the methods used to ascertain levels of the antioxidant vitamins (either through dietary intake, plasma and serum or sputum levels) were inconsistent over the range of the studies included. Even within a particular type of ascertainment such as food frequency questionnaires, substantial variation existed between the methods used and the periods covered by the questionnaire, some assessing dietary intake over the last 12 months and some over 6 months. In addition, due to the design of the majority of studies included in the review, the levels of antioxidant vitamins were assessed after the onset of asthma. The use of both food frequency questionnaires and of biological levels to estimate dietary intake have recognised strengths and weaknesses, but a major strength of questionnaires is that they measure typical dietary patterns over several months and, while the quantitative estimates of intake they provide are relatively imprecise, their ranking of intake is more representative58 and therefore suitable for combination in the meta-analysis of quantile effects. Biochemical levels offer the advantage of objectivity but often reflect only relatively recent intake and may also be subject to homeostatic or other metabolic or excretory influences that distort the relation between biological level and dietary intake. For example, levels of vitamin C in peripheral blood show relatively little variation between intakes above the minimum recommended daily intake59 and are therefore less representative of between-subject differences in intake than questionnaire measures. Thus, while dietary and serum measures are correlated for vitamin A,60 vitamin C61 and vitamin E62 and, in particular, strong correlations have been reported for antioxidant vitamins in people with asthma,61 these methodological differences are still likely to cause some discrepancy in the observed relations between diet and disease.
Most of the studies we analysed did not report adjusted results, so the results from our analyses are primarily based on crude estimates which were either extracted or estimated from these studies and so are subject to the unadjusted effects of confounding factors such as age,26 63 socioeconomic status,13 35 smoking,36 64 body mass index,47 the effects of correlated intakes of other antioxidant vitamins and, in particular for vitamin E, the effects of total cholesterol and lipid levels. The most common factors adjusted for in the included studies were age (23 studies), sex (18 studies), smoking (active or passive, 16 studies) and social class (12 studies); only 6 studies adjusted for the effects of other antioxidant vitamins in their analyses.
Overall, our findings from this systematic review and meta-analysis indicate that low levels of vitamin C intake and—to a lesser extent—vitamin A are consistently associated with asthma risk to a degree that, if causal, would be sufficient to be clinically relevant. These findings are plausible, given the recognised anti-inflammatory and antioxidant actions of these vitamins.50 However, these conclusions have not been supported by the limited data available from randomised clinical trials of dietary supplementation with vitamin C for which a recent Cochrane review concluded that there is no appreciable effect.3 One explanation for this discrepancy would be that the observational data are systematically flawed by biases leading to spurious results from meta-analyses,65 and particularly publication bias. We attempted to minimise the effects of publication bias by performing comprehensive searches that included “grey” literature; however, we were unable to formally test for publication bias due to the small numbers of studies included in the meta-analyses. Another possibility is that the observed relation between nutrient intake and disease is not causal but arises from correlation with other causally-related nutrients or non-dietary exposures. Alternatively, the observation may reflect a causal association arising from dietary intakes during early life that tend to track into adulthood, or from more sustained periods of intake than have been tested in randomised trials to date. Reverse causation is also a potential explanation, particularly in severe asthma,34 but there is no evidence that this occurs in the milder disease that predominated in the studies analysed.
The epidemiological evidence thus suggests that vitamins A and C are linked to asthma. Epidemiological studies and meta-analyses are useful for identifying association between exposures and diseases65 but cannot reliably establish causation. Further investigations are necessary to account for the observed associations using well-designed randomised controlled trials of vitamin supplementation in asthma. Trials of vitamin C supplementation to date have been disappointing; whether the effect of vitamin A will prove more important to clinical management or whether the observed associations with diet are due to confounding effects will only be resolved by further clinical trials.
REFERENCES
Supplementary materials
Web only appendix 64;7:610-19
Files in this Data Supplement:
Footnotes
See Editorial, p 560
▸ Further information is published online only at http://thorax.bmj.com/content/vol64/issue7
Funding: This study was internally funded by the University of Nottingham. The study sponsor had no role in the study design; in the collection, analysis, and interpretation of the data; in the writing of the report; or in the decision to submit the paper for publication.
Competing interests: None.
Linked Articles
- Editorial
- Editorial