Article Text

Statistics from Altmetric.com
A 29-year-old woman was transferred to our unit with a diagnosis of bronchial carcinoid tumour. She complained of chest pain, dyspnoea, cough and haemoptysis. She smoked 20 cigarettes per day and denied any history of tuberculosis, histoplamosis or occupational exposure and her family history was strongly positive for cancer. She had undergone a contrast-enhanced CT scan of the chest in the endocrinology unit which showed a partially calcified mass in the left hilum (fig 1A, arrow). Further pulmonary scintigraphy with 111In-octreotide showed a concentration of the isotope in the left hilar region (fig 1B, arrow) and a positron emission tomographic scan with 18F-FDG (FDG-PET) showed that the mass had an uptake suggestive of bronchial carcinoid tumour (fig 1C, arrow). Carcinoembryonal antigen (CEA) and tissue-specific polypeptide (TSP) levels were 7.9 ng/ml (normal 0–4) and 122.0 U/l (normal 0–80), respectively. Fibreoptic bronchoscopy revealed a pedunculated mass which bled easily occluding the left upper bronchus (fig 1D), and a CT-guided fine needle aspiration of the mass yielded inconclusive results. The patient underwent a left superior lobectomy with mediastinal lymphadenectomy. At gross examination, the mass measured 2.5 cm and appeared solid and pale. The histological diagnosis was broncholithiasis of the left upper bronchus (fig 2). One year later the patient is in good health with no sign of recurrence.

(A) CT scan showing the mass in the left hilar region (arrow). (B) Concentration of 111In-octreotide in the same region (arrow). (C) FDG-PET scan showing lesion in the left hilar region (arrow). (D) The bleeding mass at bronchoscopy.

{kind=link}
{kind=link}
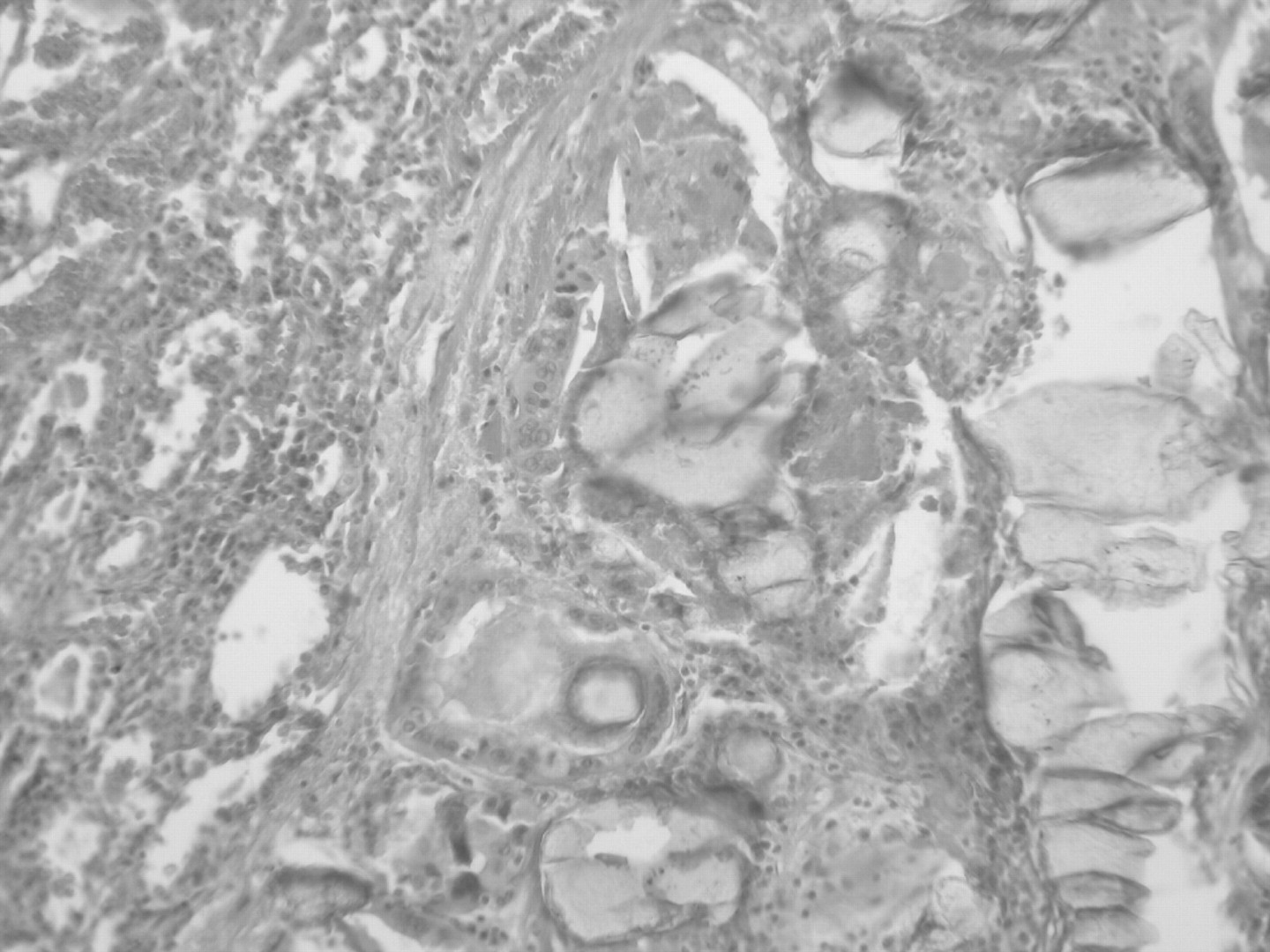
Histiocytes with foreign body reaction, rare giant cells and calcific lesions. Lymphocytes with reactive fibrous tissue can be seen at the periphery of the lesion.
It is noteworthy that the mass showed significant FDG activity on the PET scan1 and concentration of 111In-octreotide on scintigraphy. Furthermore, the values of CEA and TSP were abnormally high, and bronchoscopy revealed an easily bleeding mass suggestive of bronchial carcinoid tumour.
Broncholithiasis is a rare disease with varying clinical presentations.2 Despite its rarity, it should also form part of the differential diagnosis of pulmonary opacities with high FDG uptake on PET and concentration of In-octreotide on pulmonary scintigraphy.
Learning points
Broncholithiasis as a diagnostic possibility is rarely considered in patients with calcified granulomas on chest radiographs or chronic cough.
To prevent serious complications such as massive haemoptysis and fistula with the oesophagus or mediastinum, immediate treatment is essential.
Footnotes
Patient consent: Obtained.