Article Text

Statistics from Altmetric.com
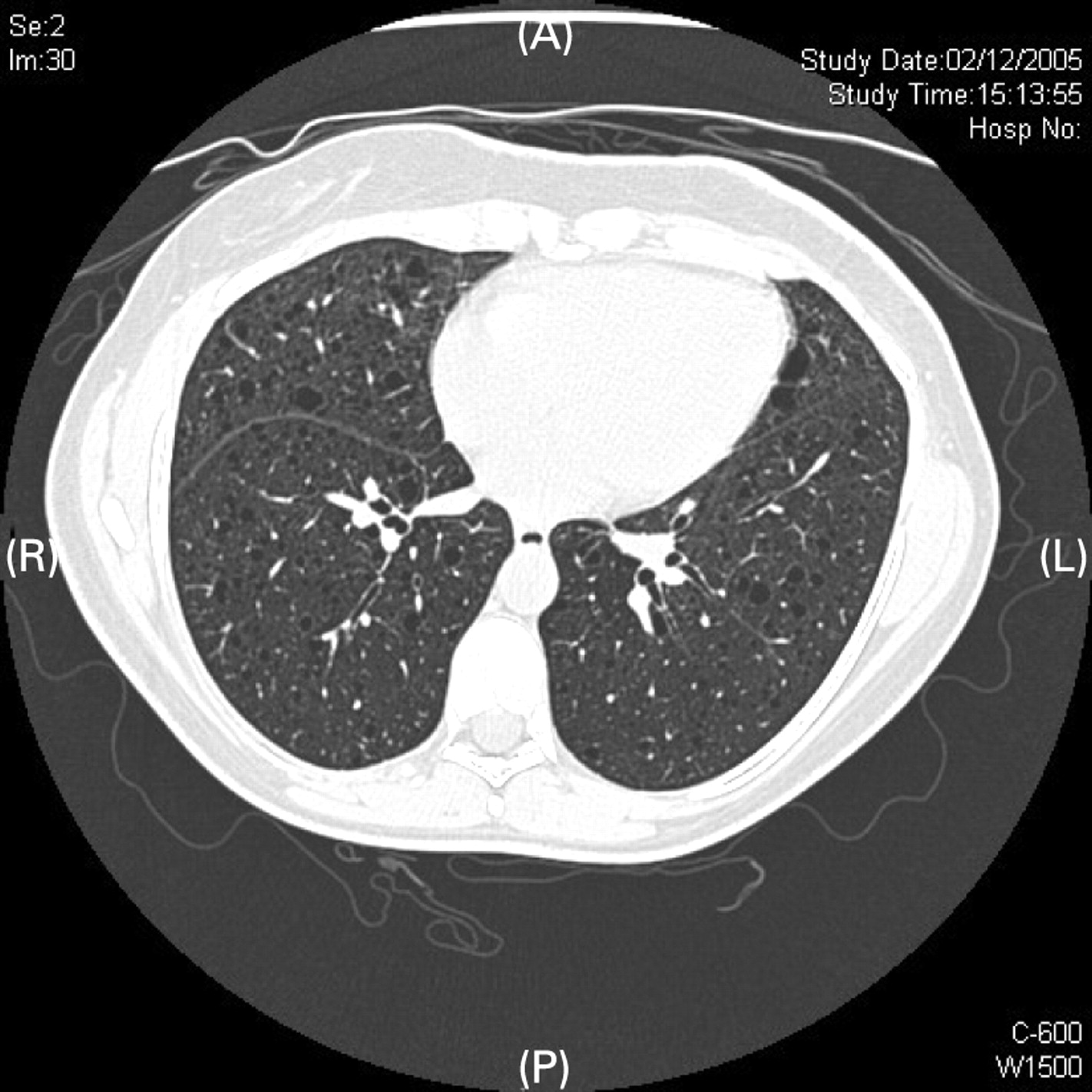
A 39-year-old nulliparous woman became breathless after a caesarean section. CT pulmonary angiography (fig 1) showed no filling defect but cysts, small bilateral effusions and thickened interlobular septa were visible consistent with a possible diagnosis of lymphangioleiomyomatosis (LAM). An open lung biopsy performed 11 months later showed that the lung parenchyma contained scattered cysts of various sizes with proliferative smooth muscle bundles in the cyst walls staining for smooth muscle actin and HMB45, which confirmed a diagnosis of LAM.

CT pulmonary angiography showing cysts, small bilateral effusions and thickened interlobular septa.
It is thought that the interstitial infiltrates were secondary to LAM. Cardiac failure may have a similar CT appearance, but the patient had no risk factors apart from recent pregnancy, improved with no anti-failure medication and did not have lung crepitations when auscultated in the immediate postoperative period.
A follow-up CT scan of the thorax 14 months later (fig 2) showed that the reticular shadowing and pleural effusions had disappeared.
{kind=link}
{kind=link}
Follow-up CT scan of the thorax.
DISCUSSION
An 11-fold increase in the incidence of chylous effusions and pneumothoraces in LAM during pregnancy has been described.1
Learning points
Lymphangioleiomyomatosis (LAM) may present for the first time in pregnancy.
Lymphatic infiltration in LAM may regress post partum.
REFERENCE
Footnotes
Competing interests: None.
Patient consent: Obtained.