Article Text

Abstract
Background: There is an increasing understanding that extreme preterm birth carries a risk of long-term pulmonary sequelae. A study was undertaken to investigate if, and in what way, neonatal factors were associated with subsequent abnormalities on pulmonary high-resolution CT (HRCT) scanning and if pulmonary function was related to these abnormalities.
Methods: HRCT scanning and pulmonary function tests were performed less than 2 weeks apart in 74/86 eligible subjects (86%) born at a gestational age of ⩽28 weeks or with a birth weight of ⩽1000 g within a defined area in Western Norway in 1982–5 (n = 42) or 1991–2 (n = 32). Mean age at examination was 18 and 10 years, respectively. HRCT scans were interpreted by a paediatric radiologist blinded to the clinical data using a structured system allowing scores from 0 to 50.
Results: Lung parenchymal abnormalities were found in 64 subjects (86%), the median (interquartile range) score being 3.0 (1.75–5.0) points. Prolonged neonatal requirement for oxygen treatment predicted poor outcome, and an increase of 100 days increased the average HRCT score by 3.8 points (p<0.001). There was also a positive association of the severity of pulmonary function abnormalities with the extent of HRCT abnormalities, exemplified by the relation between forced expiratory volume in 1 s and total HRCT score (β = −0.090; p<0.001).
Conclusions: In area-based cohorts of long-term survivors of extremely preterm birth, prolonged neonatal requirements for oxygen treatment predicted subsequent structural abnormalities on HRCT scans and in pulmonary function, and these two outcome measures were interrelated.
Statistics from Altmetric.com
Over the past three decades the survival rates for extremely preterm neonates have increased significantly from <10% to >80% in developed countries.1–3 Despite major advances in treatment, the reported incidence rates for bronchopulmonary dysplasia (BPD) have remained largely unchanged,4 and BPD is currently an important cause of chronic lung disease in children and young adults.4–6 There is reason to believe that even subtle damage to the lung parenchyma in early life may be a precursor for chronic obstructive pulmonary disease (COPD) in adulthood.7 Concerns about long-term outcome for subgroups of BPD survivors were raised as early as in 1990,8 and have also been expressed in more recent studies.1 Large cohorts of these pioneer subjects are about to reach adulthood, allowing thorough assessment of long-term outcomes. In addition to prematurity as such, we still do not fully understand the association between different neonatal factors, events or treatment with pulmonary changes in later life.
We have previously reported on airway abnormalities and pulmonary hyperinflation as well as high-resolution CT (HRCT) findings for two area-based birth cohorts of extremely preterm neonates followed for up to 20 years.9–11 Although there is good evidence to suggest an association of prolonged neonatal oxygen requirements with decreased pulmonary function later in life,6 11 12 similar data for structural lung sequelae are sparse. In the present study we therefore investigated associations between perinatal factors and subsequent structural abnormalities on pulmonary HRCT scans in childhood and early adulthood. We also examined the association between pulmonary function and HRCT findings at follow-up.
METHODS
Subjects
Of the 130 subjects born at a gestational age ⩽28 weeks or with a birth weight ⩽1000 g during the two inclusion periods in 1982–5 (first birth cohort) and 1991–2 (second birth cohort), all survivors (n = 86) were invited to participate in this study performed in 2001–2. Five eligible preterm individuals could not participate and seven declined to have an HRCT scan performed, leaving 74 subjects (86%) available for the present study. All preterm individuals were born within a defined region in Western Norway and medical care was provided at the only neonatal intensive care unit in the region (Haukeland University Hospital). Perinatal medical data were accessed from hospital charts and relevant background data from a standardised questionnaire. BPD was classified as suggested by Jobe and Bancalari13—that is, mild or moderate/severe BPD according to requirement for supplemental oxygen at a postnatal age of ⩾28 days or at a postmenstrual age of ⩾36 weeks, respectively. Neonatal characteristics of the preterm population are provided in table 1 and their lung function data at follow-up are shown in table 2. These results are presented and discussed in detail elsewhere.11 Briefly, preterm individuals had airway obstruction, airway hyperresponsiveness and pulmonary hyperinflation, which increased with increasing severity of BPD.
Neonatal history and treatment
Mean (SD) birth weight was 1014 (193) g and 933 (204) g and mean (SD) gestational age was 27.3 (1.4) weeks and 26.7 (1.7) weeks in the first and second birth cohorts, respectively. In the first inclusion period 39% of the admitted infants died in the neonatal department compared with 27% in the second (p = 0.157).
The senior medical staff responsible for major decisions was largely the same for both periods. Weaning from supplemental oxygen was based on transcutaneous measurements in the 1980s and oximetry in the 1990s. Exogenous surfactant (Exosurf) was available to the second birth cohort and was administered to 15 subjects (47%), in essence as prescribed for selective administration in the Osiris trial.14 Routines for administration of postnatal corticosteroids were similar for the two inclusion periods.
HRCT protocol and interpretation
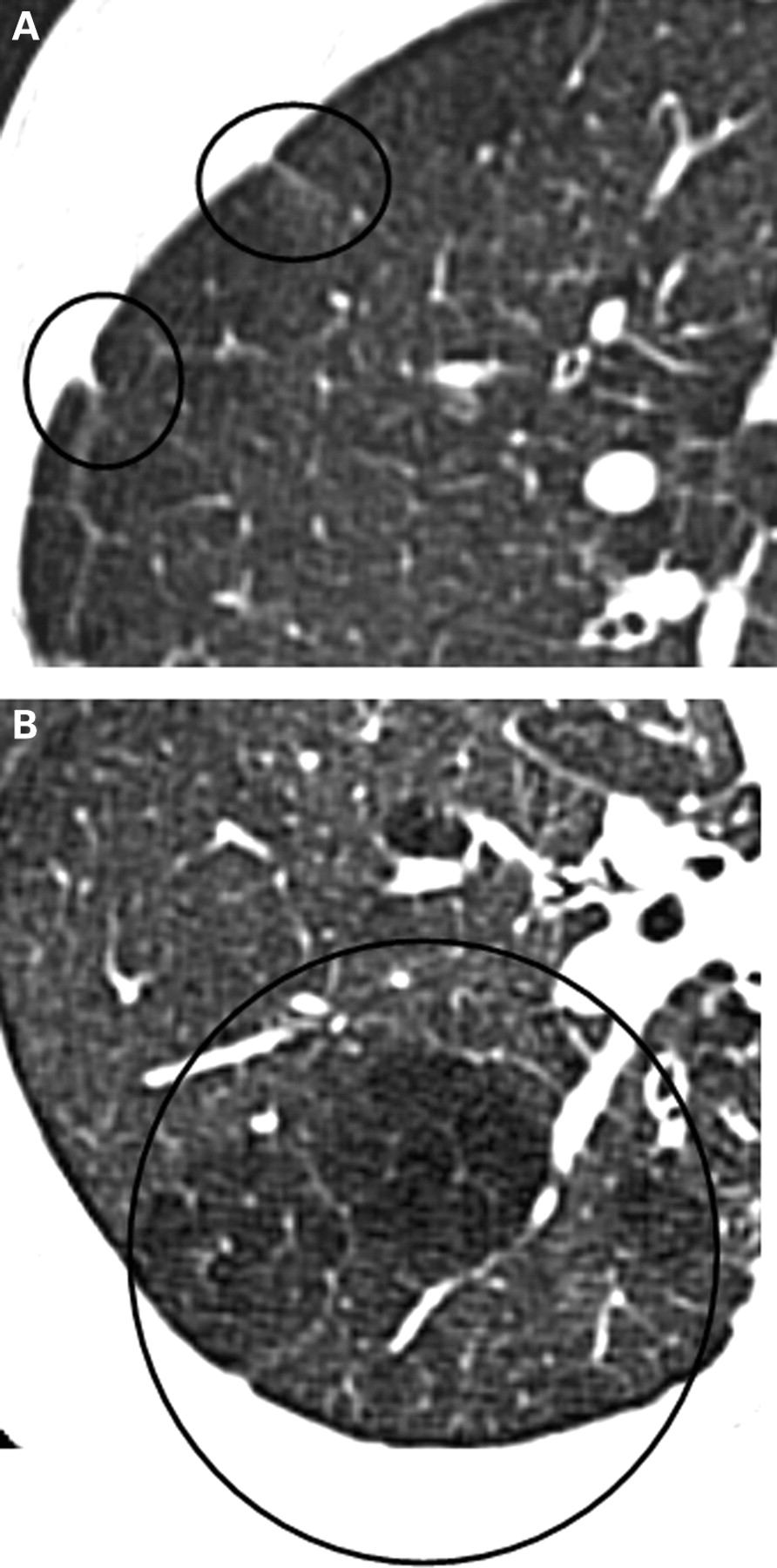
The HRCT scans were performed on a General Electric Hi Speed Advantage CT (Milwaukee, USA), obtaining 1.25-mm sections at 10 mm intervals in inspiration and at 20 mm intervals in expiration. All scans were interpreted independently by two paediatric radiologists according to a structured scoring scheme. Each lung segment was scored for the presence or absence of the following variables: linear and subpleural triangular opacities (fig 1), decreased lung attenuation (on inspiration and/or expiration, fig 1), bronchial wall thickening, bronchus-to-artery-diameter ratio, bullae, emphysema, collapse/consolidation and bronchiectasis. This initial scoring system was robust, with weighted kappa values for the total HRCT score of 0.87 (interobserver) and 0.88 (intraobserver).9 A slightly simplified version was used in the present study. The original segmental lung maps from the second reading of observer number 2 (SMA) were re-evaluated. Each lobe (lingula included) was scored according to either the presence (1) or absence (0) of each of the abovementioned variables in any lung segment belonging to that particular lung lobe. Linear and triangular opacities were merged into one variable (ie, the presence of either in any lung segment within a lobe implied a score of 1 for that particular lobe). There was one exception; lungs containing a subsegmental collapse/consolidation were scored as 1 and lungs with segmental involvement were scored as 2 (table 3). This system gave a minimum score of 0 (normal) and a maximum score of 50.
{kind=link}
High-resolution CT findings in an 11-year-old boy showing (A) linear and subpleural triangular opacities and (B) hypoattenuated area.
Pulmonary function tests
Pulmonary function tests were performed within 2 weeks of the HRCT scan. Maximal flow-volume loops and static lung volumes were measured with Vmax 22 and Autobox 6200, respectively (SensorMedics, Yorba Linda, USA), applying standard quality criteria.15 Forced expiratory volume in 1 s (FEV1), forced expiratory flow at 50% and at 25–75% of forced vital capacity (FEF50 and FEF25–75), total lung capacity (TLC), residual lung volume (RV) and the ratio RV/TLC were recorded and the values expressed as percentages of predicted.16 17
Statistical methods
Lung function data were normally distributed while HRCT scores were not. Group comparisons were done with statistical tests as appropriate (Student t test for lung function data and Mann-Whitney U-test for HRCT scores). The results are reported as means or median values (or both), as appropriate. Simple linear regression analyses were used to study relationships between HRCT scores (response variable) and accessible neonatal variables (antenatal cigarette exposure, antenatal maternal infection, antenatal treatment with corticosteroids, treatment with exogenous surfactant, gestational age at birth, birth weight, closing of a persistent ductus arteriosus, postnatal treatment with corticosteroids, number of days with intermittent positive pressure ventilation, number of days with oxygen treatment). Clinically, we know that that most of these neonatal variables are colinear and we therefore performed a backward stepwise multiple linear regression analysis for total HRCT score. The analysis included those factors from the neonatal period that were significantly related to total HRCT score in simple regression models. Analyses of interaction effects were used to assess if the influence from the examined neonatal variables differed between the two birth cohorts.18 Relationships between HRCT scores (response variable) and lung function data (FEV1, FEF50, FEF25–75 and RV/TLC) were studied in simple linear regression models. The results are reported as determination coefficients (R2) and regression coefficients (β). R2×100 estimates the percentage of the variability in an outcome variable (eg, total HRCT score) being explained by one or several explanatory variable(s) (eg, FEV1) and the adjusted R2 estimates the variance explained “per estimated coefficient” in a multiple linear regression model. The β value illustrates the numerical change in an outcome variable, when one explanatory variable changes one unit and other variables are kept unchanged. All statistical tests were performed at a 5% significance level.
RESULTS
Neonatal characteristics and lung function data are given in tables 1 and 2. Pathological findings were demonstrated in 64 subjects (86%). Most of the observed pathology was relatively minor with linear/triangular opacities constituting the majority, seen in 82% of the cases and contributing 64% to the total score. Hypoattenuated areas in inspiration were seen in 14% and hypoattenuated areas in expiration were seem in 26% of the cases. The mean (SD) total HRCT score for the whole group was 3.6 (3.0) points (range 0–13). The median (interquartile range, IQR) score was 3.0 (1.75–5.0) points. A higher score was found for the 1982–4 birth cohort than for those born during 1991–2 (mean 4.0 vs 3.2), however the difference was not statistically significant (p = 0.075). There was no significant difference according to gender, with mean scores of 4.2 for boys and 3.1 for girls (p = 0.181).
Relationship between neonatal factors and HRCT findings
In linear regression models, neither age at examination nor birth cohort significantly predicted total HRCT score at examination. Numerically, the number of days with oxygen treatment seemed to be of higher importance in the 1991–2 birth cohort than in the 1982–5 cohort, explaining 43% and 23%, respectively, of the variability in total HRCT score (R2 = 0.425; p<0.001 vs R2 = 0.228; p = 0.002). However, this difference was not statistically significant (test of interaction, p = 0.267). The effects from the various examined neonatal variables on the total HRCT score did not differ significantly between the two birth cohorts (tests of interaction).
Compared with subjects without BPD or with only mild BPD (n = 53), subjects with a history of moderate or severe BPD (n = 21) had a significantly higher total HRCT score (mean 3.0 vs 5.2, p = 0.009) as well as more opacities (p = 0.035) and hypoattenuated areas (p = 0.007).
Intrauterine cigarette exposure, evidence of maternal infection, antenatal treatment with corticosteroids and treatment with exogenous surfactant were unrelated to HRCT findings at follow-up in simple regression models and when tested with non-parametric group comparisons (Mann-Whitney U test). In simple regression models, gestational age at birth was associated with total HRCT score (β = −0.721; 95% confidence interval (CI) −1.144 to −0.297; p = 0.001)—that is, one week longer pregnancy reduced the total HRCT score by 0.7 points. Birth weight was also associated with the total HRCT score (β = −0.004; 95% CI −0.007 to −0.001; p = 0.013)—that is, an increase in birth weight of 100 g reduced the total HRCT score by 0.4 points. A neonatal history of an artificially closed ductus arteriosus was associated with increased total HRCT score (β = 1.962; 95% CI 0.573 to 3.350; p = 0.006). Postnatal treatment with corticosteroids significantly predicted increased scores for the most common HRCT findings, and the total HRCT score increased by 4 points in the treated group (β = 4.182; 95% CI 2.511 to 5.852; p<0.001). The number of days with ventilator treatment was associated with the total HRCT score (β = 0.114; 95% CI 0.066 to 0.163; p<0.001)—that is, 10 ventilator days increased the total HRCT score by 1.1 points. Increased number of days with oxygen treatment predicted an increase in the total HRCT score as well as more opacities and hypoattenuated areas. Four weeks of oxygen treatment increased the total HRCT score at follow-up by 1 point (β = 0.038; 95% CI 0.025 to 0.052; p<0.001).
Neonatal variables that were significantly associated with the total HRCT score were included in a backward stepwise linear regression analysis. The final model contained only two variables significant at the 5% level: number of days with oxygen treatment (β = 0.029; 95% CI 0.012 to 0.045) and number of days with ventilator treatment (β = 0.060; 95% CI 0.005 to 0.115). This model explained 33.3% of the variability in total HRCT score (adjusted R2 = 0.330, p<0.001). When the number of days with ventilator treatment was omitted from the model, the number of days with oxygen treatment still explained 31% of the variability in total HRCT score (R2 = 0.307, p<0.001), thus appearing the single most important explanatory variable after adjustment for other colinear neonatal variables.
Association of HRCT findings with lung function tests
When studied with simple linear regression models, all of the assessed lung function variables (FEV1, FEF50 and FEF25–75 and the ratio RV/TLC) were significantly associated with linear/triangular opacities and with total HRCT score (table 4). Reducing FEV1 (expressed as percentage predicted) by 20 units implied an increase in total HRCT score of 1.8 points (β = −0.090; 95% CI −0.14 to −0.04; p<0.001). Twenty-one preterm individuals (28%) had hypoattenuated areas on inspiration and/or expiration images. Subjects with hypoattenuated areas had significantly lower FEV1 than those without hypoattenuated areas (mean FEV1 80.9% vs 89.8%, p = 0.040). No statistical difference was demonstrated between the two groups for mean FEF50 (74.0% vs 81.0%; p = 0.289) and the ratio RV/TLC (22.8 vs 22.2; p = 0.772).
DISCUSSION
Pulmonary HRCT abnormalities were demonstrated in 86% of the children or adolescents born extremely preterm, most of the findings being relatively minor with linear/triangular opacities being the most typical (seen in 82%). Neonatal BPD and prolonged requirement for oxygen treatment appeared to be the major neonatal predictors for the observed HRCT changes at ages 10 or 18 years. Lung function abnormalities were associated with pathology on pulmonary HRCT scans.
The strengths of this study were the population-based design and the high follow-up rate of 86%. Selection bias is considered unlikely since Haukeland University Hospital provides the only neonatal intensive care unit within the area under investigation. Furthermore, no major differences in baseline characteristics were seen for the cases excluded from the study compared with those included. Two birth cohorts were studied, born approximately 7–8 years apart. To the benefit of all preterm children, but particularly the most immature and vulnerable infants, substantial improvements in treatment had occurred during this time interval. A tendency for increased survival rates in the second birth cohort combined with lower birth weight and gestational age indicate a possible recruitment of new and more immature survivors in the last birth cohort. One may envisage two possible long-term consequences from this scenario: fewer sequelae due to better treatment or more sequelae due to survival of more vulnerable individuals. Interestingly, we observed a non-significant trend for fewer structural pulmonary sequelae in the most recent birth cohort, illustrated by a mean total HRCT score of 3.2 compared with 4.0 in the 1982–5 birth cohort. It cannot readily be established in this study whether or not this numerical difference reflects a true improvement or whether the two birth cohorts are, in fact, similar because of a relatively low power caused mainly by a high degree of individual differences, with a consequently wide range of distribution (mean (SD) total HRCT score 3.6 (3.0)). With this knowledge at hand, we have in retrospect calculated that the lower detection limit of this study for differences between the two birth cohorts was approximately 2 points for total HRCT score, providing a significance level of 0.05 and 80% power. Subanalyses of putative associations between particular neonatal variables and particular HRCT subscores would be even more difficult to interpret. Larger multicentre studies or meta-analyses are required to investigate these issues.
A slightly revised procedure for calculating the HRCT scores was used in this study compared with a previous presentation of these same subjects.9 First, linear and triangular opacities were merged into one entity as these findings may be difficult to distinguish and may also reflect similar pathology. Second, we opted to base the scores on findings in the different lung lobes instead of lung segments. This made the scoring process less complex, reducing the risk of inaccuracies. Furthermore, the highest attainable score of this revised version becomes more evident to an uninvolved clinician. Formal reliability testing was not felt to be required as the revised version is fully based on the previous and more complex method.
Histopathological findings after extremely preterm birth typically include abnormal alveolarisation, disturbed vascularisation and altered elastic and fibrous interstitial networks.19–23 This again may change the peribronchiolar support, elastic recoil and small airway resistance and lead to decreased expiratory flow rates.24 25 The reduced maximal expiratory flow rates (FEV1, FEF50 and FEF25–75) observed in our study may be explained within this conceptual framework. Further, the observed association between low flow rates and HRCT changes suggests that the radiographic findings, although subtle, reflect some fundamental aspect of the pulmonary sequelae from extremely preterm birth.
The neonatal history of extreme preterm individuals varies considerably, some being relatively benign while, in others, neonatologists are faced with major challenges from nearly all organ systems. In these tiny patients, most medical problems tend to be interrelated and have some impact on ventilation and gas exchange. We know, for instance, that a neonate born with a low birth weight after a short gestation who develops respiratory distress and a wide open ductus arteriosus is likely to be exposed to prolonged mechanical ventilation, postnatal corticosteroids, some procedure to close the patent ductus arteriosus and prolonged oxygen treatment. The long-term effects of particular neonatal factors are therefore difficult to discern due to co-linearity between the explanatory variables.
Clearly, pulmonary outcome from premature birth is related to gestational age at birth and to birth weight.26 27 In simple regression analyses in this study, these variables were also related to the total HRCT score. We also observed a strong association between postnatal treatment with corticosteroids and HRCT findings. Grischkan et al28 reported a similar association with subsequent development of asthma. In this context, one must bear in mind that this treatment is used to facilitate extubation in infants with the most severe lung disease. In a stepwise multiple regression model including a series of potential explanatory variables, the number of days with oxygen treatment and the number of days with ventilator treatment explained 33.3% of the variability in total HRCT score, supporting the view that the most traumatised neonates are those most prone to develop long-term sequelae.
Prolonged requirements for oxygen treatment have previously been identified as an important explanatory variable for functional lung abnormalities.10–12 This study provides evidence that this association is present also for structural lung sequelae as evident on HRCT scanning. Whether or not this is a noxious effect of oxygen per se is unknown. Certainly, prolonged requirements for supplemental oxygen may represent the “final common output” of a series of events, inducing a statistical—but not necessarily a causal—relation to outcome. However, an independent noxious effect from oxygen is not biologically implausible. Both scenarios may be true—that is, prolonged requirements may be a marker of lung injury already present as well as a causal factor for additional lung injury. Whatever role oxygen supplementation may play, prolonged requirements appear to be a prognostic indicator for subsequent functional and structural abnormalities in these infants.
Only a few studies have reported the HRCT findings in long-term survivors of preterm birth,29–34 of which only two address the associations between HRCT findings and neonatal factors and lung function.31 32 In a study by Mahut and colleagues,31 which included 41 toddlers aged between 10 and 20 months with a history of neonatal BPD and uncontrolled respiratory symptoms, pathological HRCT findings were reported in all cases with a higher prevalence of opacities and hyperlucent areas than in our study. Their findings of prolonged neonatal oxygen treatment predicting later HRCT abnormalities, as well as the positive association between HRCT pathology and reduced lung function, are consistent with our findings. Wong and colleagues reported pulmonary emphysema on HRCT images in 16 out of 19 ex-preterm individuals who had a neonatal history of oxygen requirements at 36 weeks gestation and were examined at the age of 18–26 years.32 However, their cohort was highly selected, constituting 19 subjects (14%) from a cohort consisting of 133 subjects.
Bancalari et al reported that the fraction of infants able to breathe room air at 36 weeks was relatively similar over a wide range of gestational ages.4 Since infants born after a short gestation require longer periods of oxygen therapy to reach 36 weeks than more mature infants, increased survival in the most immature group seems to occur at the cost of prolonged exposure to oxygen treatment. Although not statistically significant, prolonged treatment with oxygen seemed to be more important for total HRCT score in the 1991–2 birth cohort than in the 1982–5 cohort. If prolonged oxygen exposure is a principal explanatory factor for subsequent functional as well as structural abnormalities of the lungs, one may reason that increased survival of the most immature infants may occur at the cost of an increased risk of long-term pulmonary sequelae.
In conclusion, in area-based cohorts of 10–18-year-old subjects born extremely preterm in the 1980–90s, evidence of structural lung injury was observed on HRCT images in 86% of the subjects, the majority of the pathology being relatively minor linear or subpleural opacities. A neonatal history of prolonged requirements for oxygen treatment predicted subsequent structural abnormalities on the HRCT scan, as well as lung function abnormalities. Structural and functional pulmonary abnormalities were significantly associated with each other, suggesting that these outcome categories are related and possibly connected to similar neonatal traumas.
Acknowledgments
The authors are indebted to Professor Trond Markestad for his enthusiasm and valuable comments.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: The Regional Committee for Medical Research Ethics approved the study. Informed written consent was obtained from participating subjects and parents.