Article Text

Statistics from Altmetric.com
CLINICAL PRESENTATION
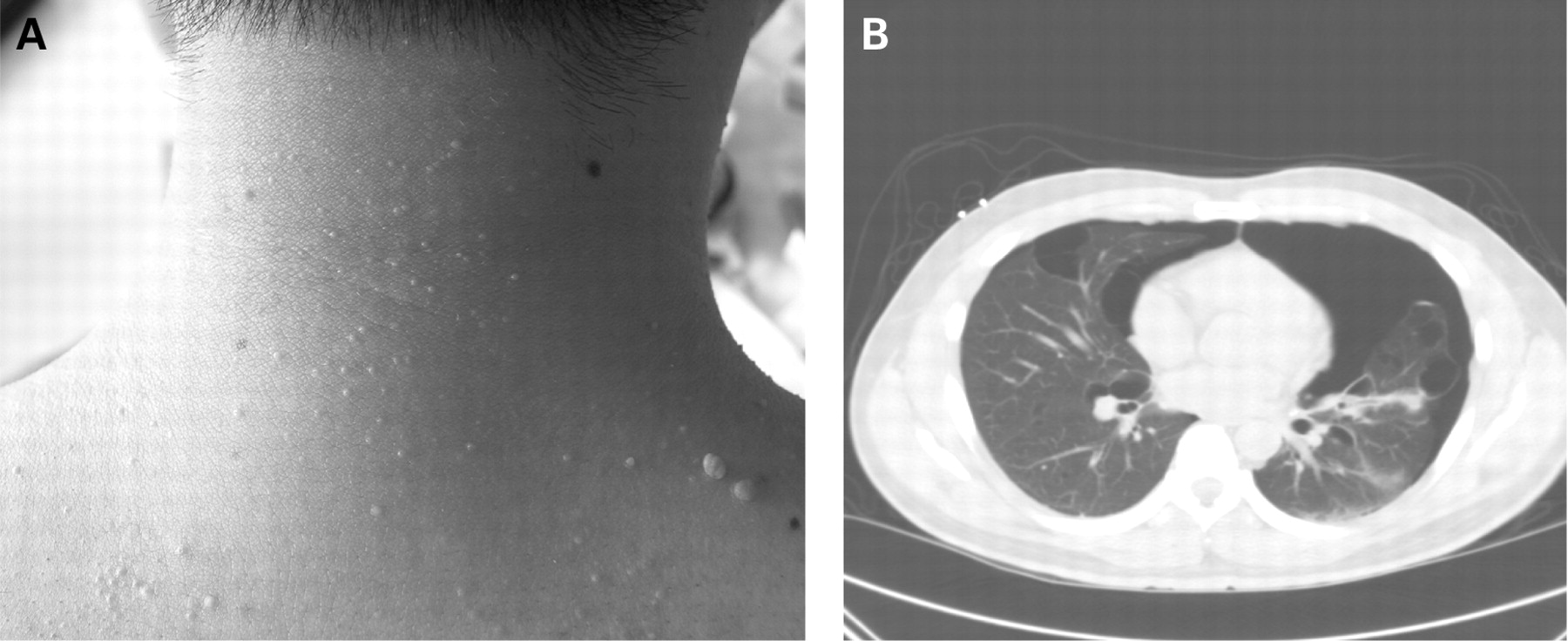
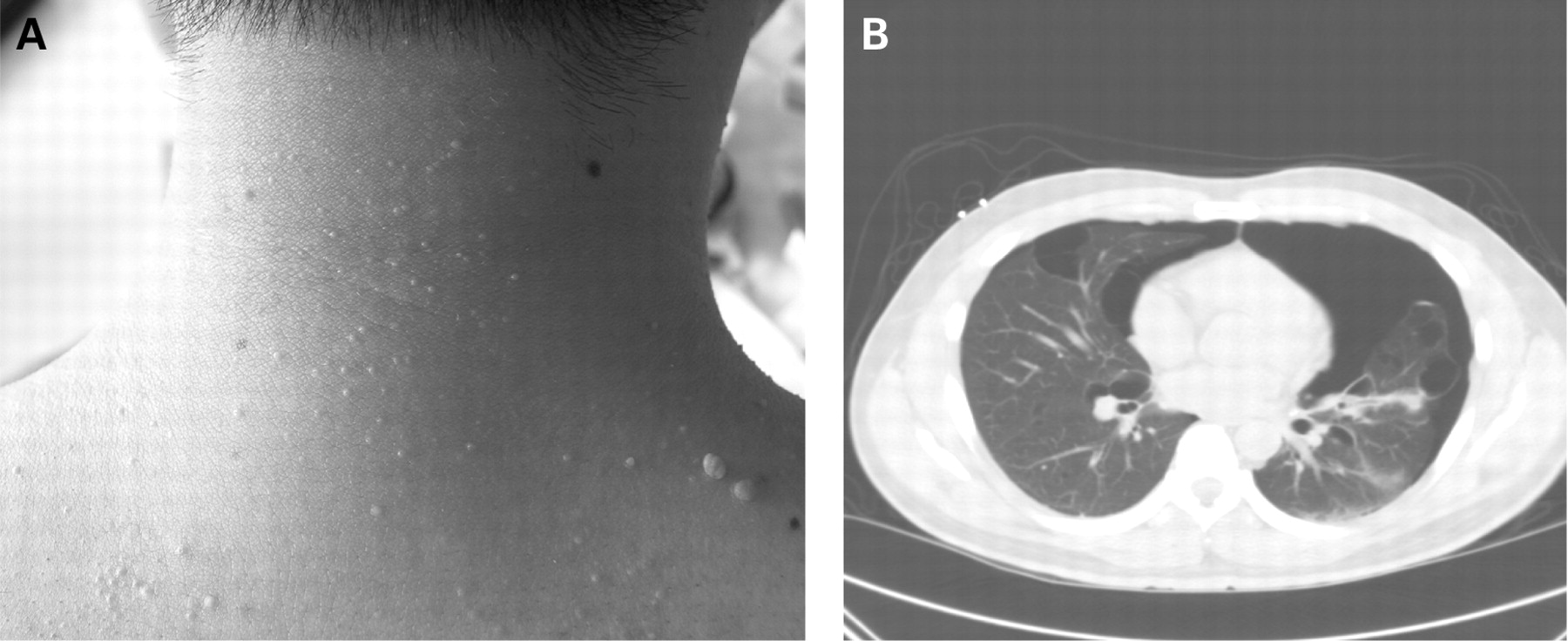
A 36-year-old non-smoking Korean man presented to the emergency room with bilateral pleuritic chest pain and mild dyspnoea on exertion. His review of systems was negative. He had multiple family members across three generations with “lung disease”. His physical examination was notable for a normal body habitus, left greater than right diminished breath sounds, hypertympany of the left thorax and many small (2–3 mm) papular lesions on his neck, chest and upper back (fig 1A). These had been present since about the age of 30 years and over the last 6 years the number of lesions had steadily increased with some larger lesions on his upper back. An initial chest radiograph showed a small right and a large left pneumothorax. In addition to the pneumothoraces, a CT scan demonstrated multiple bilateral, basilar and peripheral predominant thin-walled cystic parenchymal lesions (fig 1B).
{kind=link}
(A) Papular lesions on the upper back and neck. (B) CT scan of the chest showing bilateral pneumothoraces and basilar and peripheral predominant thin-walled cystic lesions.
Bilateral chest tubes were placed with resolution of the right pneumothorax. Owing to a persistent left-sided air leak, the patient underwent video-assisted thoracoscopic surgery with resection of multiple cystic lesions and a mechanical pleurodesis. Lung pathological examination demonstrated benign intraparenchymal thin-walled cysts which were negative for organisms and immunohistochemical stains (CD1a, HMB-45, S-100 and smooth muscle actin).
QUESTIONS
What is the diagnosis and what diagnostic test confirmed this diagnosis?
See page 457.
This case was submitted by:
Footnotes
Competing interests: None.
Patient consent: Obtained.