Article Text

Abstract
Background: The effect of low-dose CT screening for lung cancer on smoking habits has not been reported in large randomised controlled trials.
Methods: This study evaluated the effect on smoking habits of screening with low-dose CT at 1-year follow up in the Danish Lung Cancer Screening Trial (DLCST), a 5-year randomised controlled trial comprising 4104 subjects; 2052 subjects received annual low-dose CT scan (CT group) and 2052 received no intervention (control group). Participants were healthy current and former smokers (>4 weeks since smoking cessation) with a tobacco consumption of >20 pack years. Smoking habits were determined at baseline and at annual screening. Smoking status was verified using exhaled carbon monoxide levels. Lung function tests, nicotine dependency and motivation to quit smoking were assessed. Quit rates and relapse rates were determined at 1-year follow-up for all subjects.
Results: At 1 year the quit rates among smokers were 11.9% in the CT group and 11.8% in the control group (p = 0.95). Relapse rates for former smokers were 10.0% and 10.5% in the CT and control groups, respectively (p = 0.81). Significant predictors (p<0.05) for smoking cessation were: high motivation to quit, low dependency, low ratio of forced expiratory volume in 1 s to forced vital capacity, low pack years, higher age, longer period of abstinence and CT findings necessitating 3-month repeat CT scans.
Conclusions: Overall, quit rates were similar in the CT and control group at 1-year follow-up, with a net quit rate of 6.0%. Quit rates were higher and relapse rate lower among subjects with initial CT findings that necessitated a repeat scan 3 months later.
Statistics from Altmetric.com
Cigarette smoking is the leading cause of lung cancer, accounting for over 90% of all lung cancers.1 2 Most patients with lung cancer are diagnosed at an advanced stage as the onset of symptoms is often late. Lung cancer screening programmes with low-dose CT scanning are currently being evaluated in the hope of detecting lung cancer at an earlier stage and thereby improving survival.3–8
In this context, it has been claimed that screening for lung cancer with CT would provide participants with a “license to smoke” and facilitate continued smoking, or even increase the amount smoked. Any potential benefits of screening in the form of improved survival from lung cancer may therefore be at risk. On the other hand, a few studies (without control groups) have indicated that screening may provide a “teachable moment” and promote smoking cessation.9 A 14% quit rate was reported in lung cancer screening programmes at 1-year follow-up,10 11 which is higher than the quit rate of approximately 1–4% in the general population,12 although these figures may not be directly comparable. To date, no randomised controlled trials have investigated the effect of lung cancer screening programmes on participants’ smoking habits.
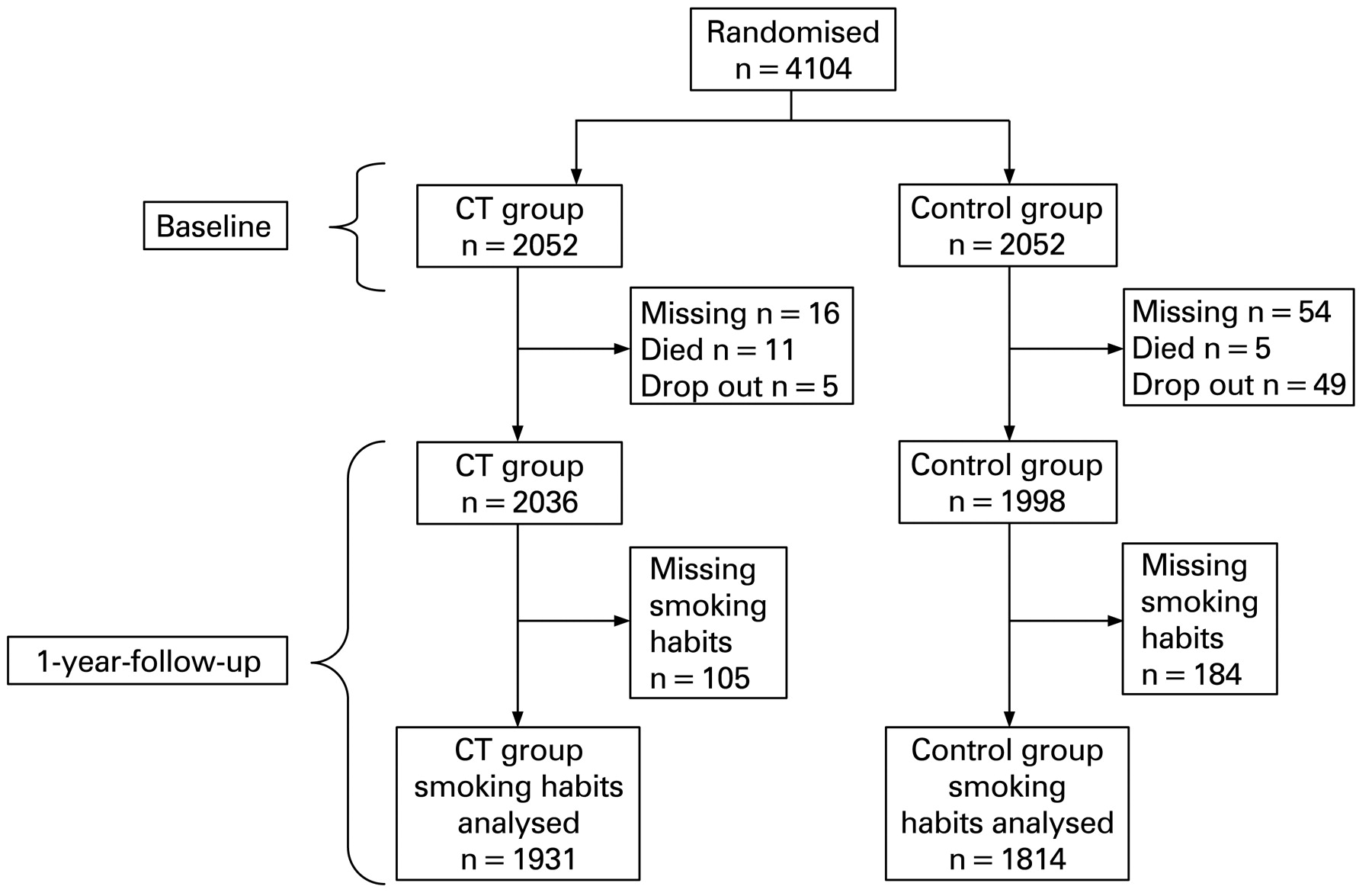
The purpose of this study was to investigate whether participation in the Danish Lung Cancer Screening Trial (DLCST) influenced smoking habits. The DLCST is a 5-year randomised trial that enrolled 4104 participants who were equally randomised to either annual screening with CT of the chest or no intervention (fig 1). The DLCST therefore provides a unique opportunity to study the influence of CT screening on smoking habits. This paper presents the results at 1-year follow-up.

{kind=link}
Flow chart of participants in the Danish Lung Cancer Screening Trial.
METHODS
Study population
Individuals volunteered for the DLCST by responding to advertisements in local and regional free newspapers. Participants were men and women aged 50–70 years with no lung cancer-related symptoms. Between 1 November 2004 and 31 March 2006, a total of 4104 participants (mean age 58 years; 45% women) were enrolled after receiving both oral and written information about the trial and signing informed consent papers. The trial is being performed in one institution in Denmark: Gentofte University Hospital, Copenhagen. Participants were randomised by a computer program (random permuted blocks of 10 participants) to either annual screening by low-dose CT of the chest (CT group) or no intervention (control group). The ongoing study is scheduled to last 5 years: an initial (prevalence) screening followed by four annual (incidence) screenings.
Study participants are current or ex-smokers with a history of at least 20 pack-years. Ex-smokers had to have quit smoking after the age of 50 years and less than 10 years ago. All participants were able to climb two flights of stairs without pausing. Pulmonary function tests (PFTs) are performed annually and, at baseline, forced expiratory volume in 1 s (FEV1) was at least 30% of predicted normal. Applicants with body weight above 130 kg or previous treatment for lung cancer, breast cancer, malignant melanoma or hypernephroma were excluded from the study. Individuals with a history of any other cancer within the previous 5 years, or tuberculosis within 2 years, or any other serious illness that would shorten life expectancy to less than 10 years were also excluded.
Counselling
Each annual visit is scheduled to last approximately 30 min for both the CT group and the control group. The participants receive minimal smoking cessation counselling (<5 min). An abnormal PFT is used to motivate participants to stop smoking and participants with normal PFT are also advised to quit smoking. The nurses who provide smoking cessation counselling are certified smoking cessation nurses with at least 3 years’ experience of counselling.
Assessments
At inclusion, information regarding age, gender, educational background and occupational status was collected for each participant, together with information on former and current smoking habits (self-reported), carbon monoxide (CO) level in exhaled air (also at 1-year follow-up), smoking status (also at 1-year follow-up), cigarettes smoked per day on average since smoking started, pack years, age smoking started, nicotine dependence score13–16 (baseline smokers only) and motivation to quit smoking (baseline smokers only).
In the present study, which presents results from the initial (prevalence) visit and the first annual follow-up, the first question in the Fagerström Questionnaire Q1 (“How soon after you wake up do you smoke your first cigarette?”) was used to evaluate smokers’ nicotine dependency. This question has four ratings: 0 (⩾61 min), 1 (31–60 min), 2 (6–30 min) and 3 (within 5 min). In addition, motivation to quit smoking was investigated using the question(“How strong is your motivation to quit smoking?”) with scores from 1 (no motivation) to 5 (high motivation).17 18
Participants in both groups had annual spirometric tests according to recommendations of the European Respiratory Society (ERS). A computerised system (Spirotrac IV; Vitalograph, Buckingham, UK) was used and results were expressed in absolute values and as percentage of predicted values, calculated according to European reference equations.19 The CO level in exhaled air was determined in both groups to validate smoking status and to determine smoking intensity. A CO level >10 parts per million (ppm) has been defined as compatible with current smoking.20–22 Expired CO can also be used as a marker of the intensity of smoking and as a substitute marker for the change in quantity smoked from baseline to 1-year follow-up (ΔCO).
All CT scans were performed on a MDCT scanner (16 rows Philips Mx 8000 idt; Philips Medical Systems, Eindhoven, The Netherlands). Scans were performed using a low-dose technique.23 24 The CT scanning results were used to divide participants into two groups, one with clinically significant CT findings (positive group) and one without (negative group). Participants in the positive group were informed that their CT result required further diagnostic follow-up, usually a repeat scan 3 months later. Participants with no significant findings were informed about the scan result and were scheduled for their next annual CT scan.
Definitions and statistics
Ex-smokers were defined as participants who had been abstinent from smoking for at least 4 weeks prior to the baseline screening visit. At the 1-year follow-up, participants were divided into four groups depending on smoking status: continuous smokers (baseline smoker who continued smoking through 1-year follow-up); recent quitters (baseline smoker who had quit smoking at least 4 weeks before the 1-year follow-up); continuous ex-smokers (baseline ex-smoker who did not smoke throughout 1-year follow-up); re-starters (baseline ex-smoker who started smoking during 1-year follow-up).
Both univariate and multiple logistic regression analyses were performed to evaluate predictors for smoking. Only participants with complete data (3542/3745, 95%) were included in the multiple logistic analyses for predictors. Baseline characteristics (gender, age, pack-years and PFT) of the CT and control groups were compared using the Student t test and smoking status was compared using the χ2 test. Both the CT and control group were analysed in one multiple logistic model with the randomisation as a covariate among others as a predictor for smoking. Analyses were performed using SAS statistical software Version 15.0 and a p value <0.05 was considered statistically significant.
RESULTS
At entry there were no significant differences between the CT and control groups in age, gender, PFT, pack-years or smoking status (table 1).
Smoking cessation in baseline smokers
Throughout the 1-year follow-up period an equal number of smokers stopped smoking in the two groups: 174 (11.9%) in the CT arm and 165 (11.8%) in the control arm (p = 0.95). Missing values regarding smoking habits at 1-year follow-up were 5.3% in the CT group and 11.6% in control group (p<0.01). Inclusion of all non-attendees in the analysis, and assuming that they were all still smokers, resulted in a quit rate of 11.3% (174/1545) in the CT group and 10.4% (165/1579) in the control group (p = 0.47).
Baseline predictors for smoking abstinence at the 1-year follow-up in the CT group (univariate model) were lower FEV1/FVC ratio, lower number of cigarettes smoked on average per day since smoking started, lower number of pack-years, lower Fagerström Questionnaire Q1 score and higher motivation to quit. Similar findings were seen in the control group (table 2).
Predictors for continuous smoking were analysed in a multiple logistic regression model. The covariates examined are listed in table 3, which shows predictors for continuous smoking. Higher pack years, higher FEV1/FVC ratio, higher dependency (Fagerström Q1), lower motivation and lower age were significant predictors for continuing smoking. Randomisation to either CT or control group and gender was not a predictor for continuous smoking (table 3).
Re-starters among baseline ex-smokers
During the 1-year of follow-up a similar number of ex-smokers began smoking again (re-starters) in the CT group (n = 47, 10.0%) and the control group (n = 44, 10.5%) (p = 0.85). Information about smoking habits at 1-year follow-up was missing for 7.5% of the CT group and 11.4% of the control group (p = 0.04). Inclusion of all non-attendees in the analysis, and assuming that they all started smoking again, resulted in a restart rate of 16.7% (85/507) in the CT group versus 20.7% (98/473) in the control group (p = 0.11).
In the CT group, abstinence at 1-year follow-up in ex-smokers was associated with a longer period of abstinence before study entry and a lower number of pack-years (univariate model). Similar findings were observed in the control group (table 4). This was tested using multivariate logistic regression (table 5). Shorter duration of smoking abstinence at entry and lower age significantly predicted smoking re-start at 1-year follow-up.
CO measurements
In both the CT and the control groups, five ex-smokers had an expired CO value above 10 ppm at 1-year follow-up (excluded from analysis). The average change in ΔCO (individual level) was −1.33 ppm in the CT group and −1.77 ppm in the control group (p = 0.21). These figures are based on all participants regardless of smoking status.
Influence of CT findings on smoking habits
A total of 173 participants (129 current and 44 ex-smokers) received a positive CT result at baseline and were rescanned 3 months later (positive group). For baseline smokers the quit rate was 17.7% in the positive CT group compared with 11.4% in the group with no significant CT findings (p = 0.04). In baseline ex-smokers, the smoking relapse rate was 4.7% in the positive CT group and 10.6% in the group with no significant CT finding (p<0.01).
DISCUSSION
The present study showed no difference in quit rates between the CT and control groups (11.9% vs 11.8%) in this lung cancer screening trial. There was no tendency to increase smoking rate or smoking intensity as assessed by changes in exhaled CO. There was no significant difference in the smoking relapse rate between the CT and control groups (10.0% vs 10.5%). This finding was validated in the multiple logistic regression model in which randomisation was not found to be a significant predictor. The absolute number of quitters minus re-starters (339 − 91) was 248 (ie, an overall quit rate of 6.0% (248/4104)). Smoking status was CO validated, which is the preferred approach in follow-up studies of smoking habits. Like other studies, our figures are markedly higher than the quit rate for smokers in the general population, which is about 4% in the Danish population.12 This has generally led to the misconception that CT scanning alone is responsible for increasing quit rates. However, in our study we found the same quit rate in the control group (11.8%), suggesting that participation in a screening trial per se induces smoking cessation. Another Danish study reported an 8% quit rate in heavy smokers after they received minimal smoking cessation counselling, similar to that provided in the present study.17 That result is similar to the quit rate found in our study. The higher number of quitters seen in lung screening trials can be explained by the fact that participants who volunteer for clinical trials are more motivated to stop smoking than the general population. This selection bias is also known to be related to social class. Although there was no difference in social class between our CT and control groups, more women of higher social class participated in the DLCST compared with the general population (data not shown).
Our study may be biased as current smokers may tend to miss follow-up visits more frequently than non-smokers because they do not wish to be confronted with their smoking. However, as smoking cessation is not the primary focus of the DLCST (the focus is on early lung cancer detection), we do not suspect that the change in smoking habits is different among participants who attended follow-up and those lost to follow-up. To our knowledge, this is the first large-scale randomised controlled study in which smoking habits were monitored in a lung cancer screening trial. Our study showed that participation in a CT scanning trial per se does not seem to have any effect on the smoking habits of the participants, which was erroneously claimed in earlier non-controlled studies.9–11
However, in a subset of the participants in our study a positive CT finding was a strong predictor for smoking cessation and for preventing relapse to smoking. Similar results have also been found in other studies.11 A positive CT finding that necessitated a repeat CT scan 3 months later might have been a frightening experience for the subjects and might have motivated them to quit smoking in the hope of improving the results of their repeat scan.25 Follow-up studies will show how long this effect persists in the DLCST. Even though participants with positive CT findings had a significantly higher quit rate and lower relapse rate, this did not result in an overall change in smoking behaviour between the CT and control groups. However, this is not surprising considering the small number of positive CT findings.
In smokers, high motivation to quit and low Fagerström Questionnaire Q1 score were the main predictors for smoking cessation at the 1-year follow-up. In ex-smokers, longer duration of abstinence at entry was the main predictor for abstinence at the 1-year follow-up. In baseline smokers, FEV1/FVC and number of pack years also reached significance as predictors, but the odds ratio was very close to 1, indicating little clinical impact.
The results of this study suggest that smokers with low nicotine dependency and those with a high motivation to quit are able to stop smoking. More intensive counselling and pharmacological treatment for smoking cessation should be administered in future lung cancer screening trials in an attempt to increase the quit rate. In screening trials, more focus should be put on smoking cessation and motivating smokers to stop as early as possible. This is important because abstinence from smoking is still the most effective method of preventing lung cancer.26–29 Monitoring smoking habits and behaviour in lung screening trials should therefore be a high priority.
In conclusion, this study did not demonstrate any difference in smoking habits in participants in a lung cancer screening trial when compared with a control group after 1 year (ie, CT screening neither induced more smoking nor promoted cessation compared with a control group). The net quit rate after 1 year was 6.0%. A positive result from CT scans motivated quitting and prevented relapse. Higher motivation to quit, lower degree of nicotine dependency and a longer period of abstinence were significant predictors for abstinence from smoking at 1-year follow-up.
Acknowledgments
The authors are grateful for the comments and suggestions from the other members of the steering committee of the Danish Lung Cancer Screening Trial: John Brodersen, Niels Seersholm, Paul Clementsen, Jann Mortensen, Birgit Guldhammer Skov, Hanne Hansen and Karen Skjøldstrup Bach. Language revision was performed by medical writer Anne Hendrie, UK.
REFERENCES
Footnotes
See Editorial, p 371
Funding: The study was funded by a governmental grant.
Competing interests: PT serves on advisory boards for Pfizer, Sanofi Aventis and GSK and has been a speaker at events sponsored by the same companies regarding smoking cessation treatments. MD serves on advisory boards for Pfizer and GSK and has been a speaker at events sponsored by the same companies regarding smoking cessation treatments.
Ethics approval: The Danish Lung Cancer Screening Trial is approved by the ethical committee of Copenhagen.