Article Text

Abstract
Background: Many studies have found that the risk of childhood asthma varies by month of birth, but few have examined ambient aeroallergens as an explanatory factor. A study was undertaken to examine whether birth during seasons of elevated ambient fungal spore or pollen concentrations is associated with risk of early wheezing or blood levels of Th1 and Th2 type cells at 24 months of age.
Methods: 514 children were enrolled before birth and followed to 24 months of age. Early wheezing was determined from medical records, and Th1 and Th2 type cells were measured in peripheral blood using flow cytometry. Ambient aeroallergen concentrations were measured throughout the study period and discrete seasons of high spore and pollen concentrations were defined.
Results: A seasonal pattern was observed, with birth in autumn to winter (the spore season) associated with increased odds of early wheezing (adjusted odds ratio 3.1; 95% confidence interval 1.3 to 7.4). Increasing mean daily concentrations of basidiospores and ascospores in the first 3 months of life were associated with increased odds of wheeze, as were increasing mean daily concentrations of total and specific pollen types. Levels of Th1 cells at age 24 months were positively associated with mean spore concentrations and negatively associated with mean pollen concentrations in the first 3 months of life.
Conclusions: Children with higher exposure to spores and pollen in the first 3 months of life are at increased risk of early wheezing. This association is independent of other seasonal factors including ambient levels of particulate matter of aerodynamic diameter ⩽2.5 μm and lower respiratory infections.
Statistics from Altmetric.com
Numerous studies have found the month of birth to be associated with the risk of allergic sensitisation1–4 or asthma5–12 later in life, an observation suggesting that exposure to seasonal allergens in the perinatal period may contribute to the development of atopic disease. However, previous studies have shown little consistency as to which months are associated with the highest asthma risks, and whether these months are associated with higher ambient concentrations of specific aeroallergens such as fungi or pollen. In addition, month of birth may represent exposures other than aeroallergens—including respiratory syncytial virus (RSV),5 air pollution and residential dampness—all of which have been associated with development of early childhood wheeze and asthma.13
Aeroallergen exposure is clearly associated with asthma exacerbations,14 15 but the role of such exposures in disease induction is less clear. The initial priming of T cells to respond to allergens is thought to occur during late gestation and the neonatal period, and early-life exposure to ambient allergens may reinforce T cell switching to favour a predominance of Th2 cells.16 Kihlström et al17 18 found that children born in the 3 months before a season of extremely high birch pollen were at increased risk of asthma at age 5, but children born after this season (whose mothers were exposed during pregnancy) were not. A cohort study of children at risk for atopic disease found that higher concentrations of Penicillium spp and total fungal spores in living room air of infants 2–4 months of age were associated with an increased risk of wheeze and persistent cough at age 12 months.19 20 Another longitudinal study reported that higher spore concentrations in living room air collected when infants were 2–3 months old were associated with increased risks of lower respiratory infection at 1 year of age21 and of allergic rhinitis at age 5.22 Recent work also implicates early-life exposure to airborne particulate matter (PM) with development of asthma and allergen sensitivity in young children in the Netherlands.23
In the present analysis we examine whether the association between month of birth and early wheezing at age 2 could be explained by high ambient spore or pollen exposure in the first 3 months of life. Additionally, we measured levels of Th1 and Th2 type cells in peripheral blood at age 24 months to determine whether cytokine profiles were associated with early-life exposure to aeroallergens.
METHODS
Participants and recruitment
Subjects were children in the Center for the Health Assessment of Mothers and Children of Salinas (CHAMACOS), a birth cohort study that is investigating the effects of environmental exposures on the health of low-income, predominantly Mexican, immigrant families in an agricultural region of California. Pregnant women were recruited between October 1999 and October 2000 through collaborating prenatal clinics. Women were eligible to participate if they were less than 20 weeks’ gestation, 18 years of age or older, spoke English or Spanish, qualified for low-income government health insurance (Medicaid) and planned to deliver at the county hospital. Of 1130 eligible women, 601 agreed to participate and 536 newborn infants were enrolled in the study. The present analysis was limited to 514 children with complete medical record data through 24 months of age. Blood samples for measurement of Th1 and Th2 cytokines were available for 236 of these children at the 24-month visit (median age 23.9 months; interquartile range (IQR) 0.9 months; range 21.7–29.0 months).
Data collection
Paediatric medical records were collected from all facilities where the child had received care between birth and 24 months of age. A single registered nurse abstracted relevant information onto standardised forms. A child was considered to have early wheezing if medical records indicated a clinician’s diagnosis of asthma at any time between birth and 24 months of age. Because many of these children may not continue to have asthma at later ages,24 we considered this diagnosis to represent “early wheezing” rather than asthma.
Standardised interviews were administered to the mothers during pregnancy, after delivery and when the children were aged approximately 6 months (median 6.4 months; IQR 1.0 month) and 12 months (median 12.4 months; IQR 1.5 months). Interviews assessed demographic data and child exposures (eg, duration of breastfeeding, second-hand smoke, frequency of colds and presence of pets in the home), and were conducted in English or Spanish by bilingual bicultural interviewers. Home inspections were conducted by trained inspectors when the children were 6 and 12 months of age to assess environmental exposures (eg, wall moisture measurements, visible fungal growth, evidence of cockroach or rodent infestation and presence of a gas stove).
Blood was analysed for Th1- and Th2-associated cytokines if the sample was received at the study laboratory within 48 h of collection. Methods for Th1 and Th2 analysis have been described previously.25 Briefly, 500 μl of whole blood were activated for 4 h with phorbol 12-myristate 13-acetate (PMA) and ionomycin (Sigma-Aldrich, St Louis, Missouri, USA) to stimulate cytokine production. Fluorescent stain was then applied with antigen-specific antibodies for CD4+ T lymphocytes (PerCP, Becton Dickinson, Franklin Lakes, New Jersey, USA), interferon (IFN)-γ (IFN-γ/FITC, Becton Dickinson) and interleukin (IL)4 (IL-4/PE, Becton Dickinson). With flow cytometry, the CD4+ population was identified and gated; these cells were then examined for expression of IFNγ and IL4. Cells that stained positive for IFNγ were classified as Th1 cells and those that stained positive for IL4 were classified as Th2 cells. Th1 and Th2 percentages were defined as the proportion of CD4+ cells identified as IFNγ or IL4 positive, respectively.
Measurement of ambient spore and pollen air concentrations
The study area (Salinas Valley, California) is a valley approximately 90 km long and 15 km wide, with a Mediterranean climate characterised by mild rainy winters and dry summers. Spore and pollen concentrations were measured between October 1999 and July 2003, a period that encompassed the in utero period and first 24 months of life for all study children. The time frame of interest was exposure during the first 3 months of life.
Airborne spores and pollen were collected with a Hirst-type sampler26 (Seven-Day Recording Volumetric Spore Trap; Burkard Manufacturing Co, Rickmansworth, UK) located in the city of Salinas and placed 10 m above the ground to avoid over-representation of local vegetation. An American Academy of Allergy, Asthma, and Immunology-certified analyst read three slides per week throughout the study period.
Twenty-seven spore and 48 pollen groups were identified. Seven fungal groups were observed on more than half of all sampling days and accounted for 82% of the annual spore concentrations: Cladosporium spp (44%), basidiomycetes (25%), ascomycetes (6%), Aspergillus or Penicillium spp (4%), Botrytis spp (1%), smuts or myxomycetes (1%) and Alternaria spp (0.5%). Ten plant groups were observed on more than 10% of all sampling days and accounted for 75% of the annual pollen concentrations: cypress (32%), oak (11%), pine (7%), grass (6%), nettle/pellitory (4%), mulberry (4%), alder (4%), elm (3%), sage/wormwood (2%) and plantain (2%).
For each child the mean daily spore and pollen concentrations during the first 3 months of life were calculated for the four identified spore and seven identified pollen types that accounted for more than 3% of the total. The four spore and seven pollen groups also were summed to create variables for total spore and pollen concentrations in the first 3 months of life.
Measurement of particulate matter (PM) concentrations
Particulate matter (PM) data were obtained from the Monterey Unified Air Pollution Control District (MBAPCD) which operated an air pollution monitoring station within 0.5 km of the study’s aeroallergen station. For 24 h every sixth day, the MBAPCD station measured PM with aerodynamic diameters ⩽10 μm (PM10) and ⩽2.5 μm (PM2.5) with high-volume Sierra-Andersen gravimetric samplers (Thermo Scientific, Waltham, Massachusetts, USA). For each child we calculated the mean 24 h PM2.5 and PM10 concentration during the first 3 months of life.
Seasonal patterns of exposure
To determine seasonal patterns of ambient exposures, we plotted daily concentrations of spores and pollen over the study period. A Lowess smooth27 was fitted to each scatterplot and high-concentration days were defined as those in which the fitted values were ⩾40% of the maximum fitted value. High concentration days were clustered in time, resulting in three distinct periods each year: (1) high spore/low pollen concentration, termed the “spore season”, (2) high pollen/low spore concentration, termed the “pollen season”, and (3) periods with low concentrations of both. These seasons are shown in fig 1, with the period of participants’ births (16 February 2000 through 18 June 2001) shown in black along the x axis. The children were categorised according to season of birth, with low spore/low pollen as the reference category. There was very little overlap between the spore and pollen seasons; however, four children born between 16 February 16 and 1 March 2000 overlapped the end of the spore season and the beginning of the pollen season. These children were classified as pollen season births because their primary early-life exposure would be pollen. (Changing these children to spore season births did not change the results markedly.)
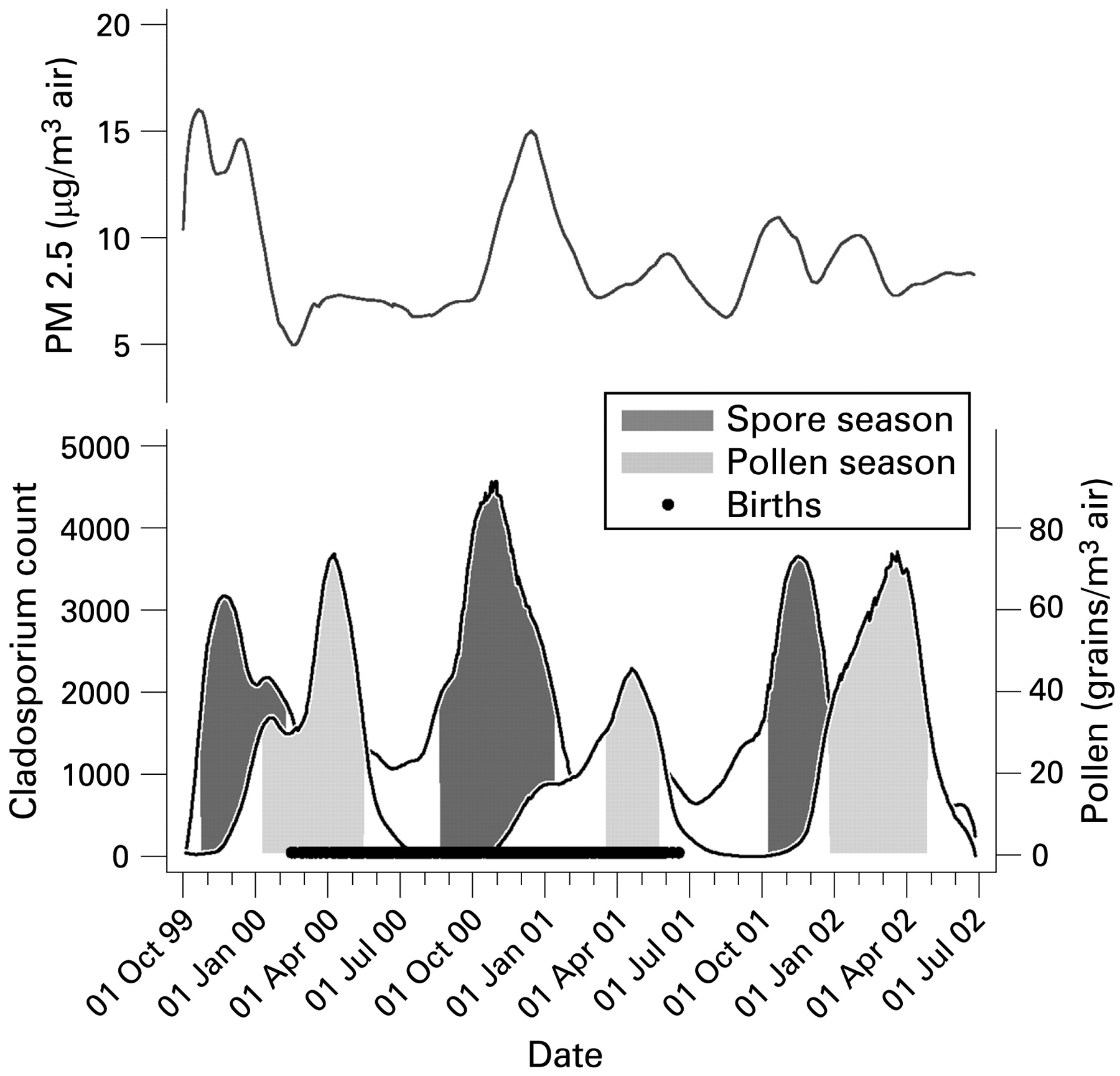
Lowess smoothing of daily spore and pollen concentration and mean particulate matter with aerodynamic diameter ⩽2.5 μm (PM2.5) levels. Salinas Valley, California, 1999–2002.
We also examined seasonal patterns of PM air pollution using Lowess plots. Figure 1 shows that the periods of raised PM2.5 tended to coincide with those of high spore concentrations. No seasonal patterns were observed for PM10, but this is not surprising since the components of PM10 (PM2.5 and PM10–2.5) have different temporal peaks which would tend to reduce PM10 seasonality.
Data analysis
Logistic regression was used to examine the association between early wheezing and mean ambient spore and pollen concentrations in the first 3 months of life. Spore and pollen concentrations were negatively correlated, and no child (including the four children born in the overlap of the spore and pollen seasons) simultaneously experienced high spore and pollen levels in the first 3 months of life; total spore and pollen exposures were therefore not included in the same model. Separate models were also created for individual spore and pollen types. Because of the wide difference in ranges of spore and pollen concentrations, odds ratios were standardised to an increase in units equal to the interquartile range (IQR) for each exposure.
Associations between Th1 and Th2 profiles at age 24 months and mean spore and pollen concentrations were examined by linear regression. Th1, Th2 and the ratio of Th1:Th2 were log-transformed and three influential (outlier or leverage) points were excluded. Th1 and Th2 were analysed both as absolute levels and as the percentage of total CD4+ cells; as the results were similar by both approaches, we present only the latter.
To explore the possibility of confounding, we examined other early-life exposures (table 1) that we hypothesised might be associated with early wheezing. Variables of particular interest were physician-diagnosed respiratory infections; visible mould, dampness or evidence of cockroaches or rodents in the home; and PM2.5 exposure, all of which may display seasonal patterns. Variables associated with both the exposure (season of birth) and outcomes (wheezing or Th1/Th2) were included as covariates in the multiple regression models. Covariates were kept in the model if they had a p value <0.1 or if their exclusion changed the coefficient for the main effect by 10% or more. Because exposure to PM2.5 and spores were highly correlated (r = 0.6), we regressed spore concentration on PM2.5 and used the residuals from this regression in the models that contained spore variables.
RESULTS
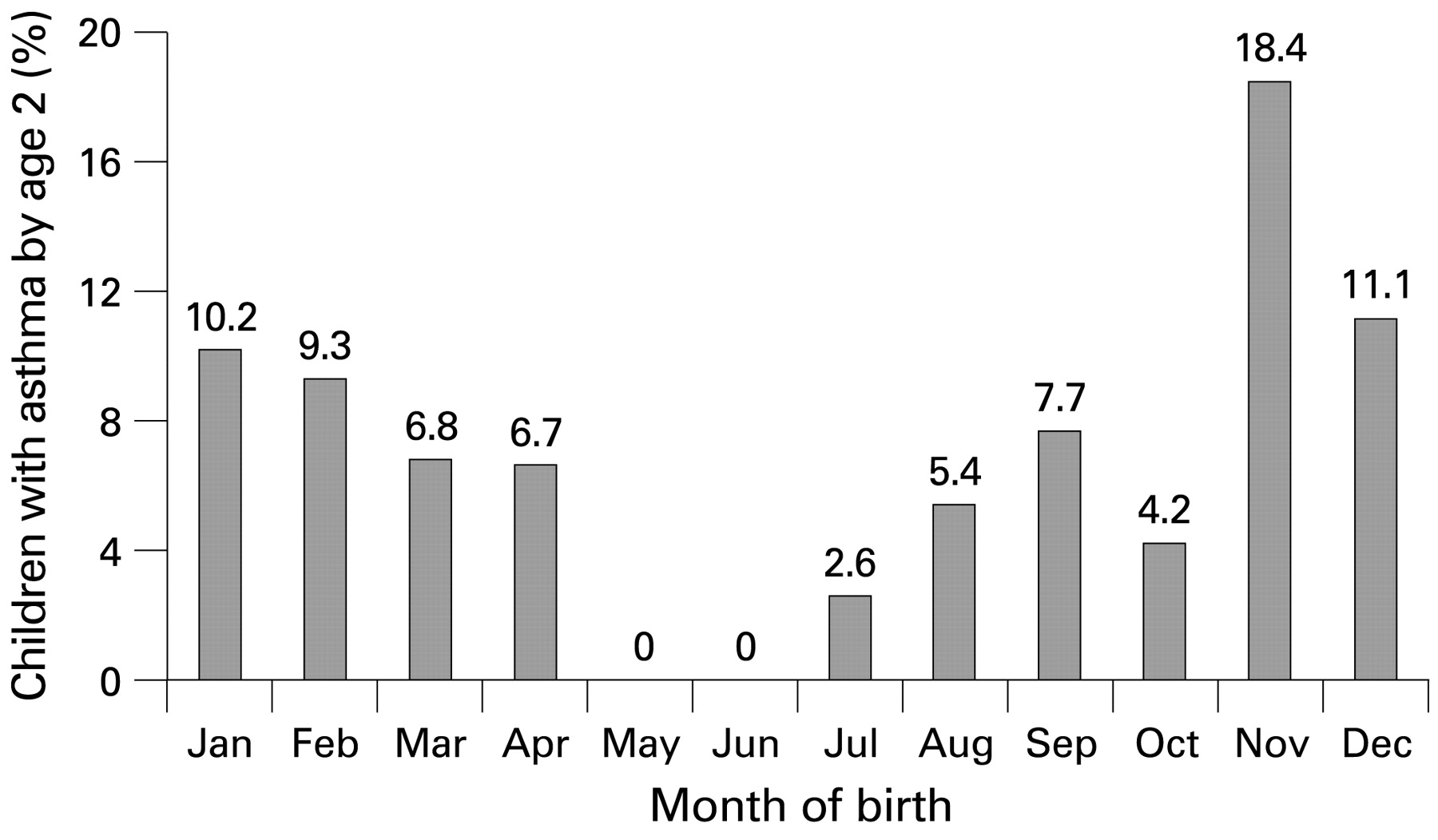
Table 1 shows the characteristics of the study population. Children were predominantly low income and of Mexican descent. Thirty-five children (6.8%) had a diagnosis of early wheezing by 24 months of age; a clear pattern was observed with month of birth (fig 2). The unadjusted odds ratio (OR) for early wheezing for children born during the spore season relative to children born outside the spore and pollen seasons was 2.8 (95% CI 1.2 to 6.5) (table 1), an association that persisted after controlling for confounders (aOR 3.1, 95% CI 1.3 to 7.4)(not shown). Poverty status, tobacco smoke exposure and lower respiratory tract infection in the first year of life also were associated with increased odds of early wheezing, and higher PM2.5 exposure, pets, gas stove or rodents in the home were of borderline statistical significance. Wall moisture measured at the age of 6 months was associated with reduced odds of early wheezing.
{kind=link}
{kind=link}
Physician-diagnosed early wheezing according to month of birth. Salinas Valley, California, 1999–2001.
In adjusted analyses there was only a weak association between total spore concentration in the first 3 months of life and early wheezing (table 2). However, basidiospore and ascospore exposure were each associated with increased odds of wheezing (aOR per IQR of exposure 2.1 and 2.8, respectively). Higher total pollen concentration in the first 3 months was associated with increased odds of early wheezing (aOR 2.0; 95% CI 1.1 to 3.9). Increasing concentrations of cypress, oak, pine, alder and mulberry pollen in the first 3 months of life were also associated with greater odds of early wheezing, of which the associations for cypress, pine and alder were statistically significant.
The median level of Th1-type cells in this population was 3.4% of total CD4+ lymphocytes (IQR 3.07; range 0.03–21.6). The median level of Th2-type cells was 0.9% of total CD4+ cells (IQR 0.8; range 0.4–4.1). We have previously shown that early wheezing was associated with higher Th2 levels in this population.28
The associations between Th1, Th2 and Th1:Th2 ratio and ambient spore and pollen concentrations in the first months of life are shown in table 3, with β coefficients representing the percent change in Th1, Th2 or Th:Th2 associated with a unit increase in spore or pollen concentration equal to the IQR. The Th1:Th2 ratio was positively associated with the number of colds and negatively associated with early PM2.5 exposure and having a gas stove in the home (not shown). Thus, analyses controlled for these variables. The ambient spore concentration in the first 3 months of life was positively associated with Th1 levels and Th1:Th2 ratio. Early-life pollen concentration was negatively associated with Th1 levels at age 2 years.
DISCUSSION
Children born during periods of high ambient spore concentration (16 February 2000 to 1 March 2000 or 21 August 2000 to 10 January 2001) were found to be at greatest risk of early wheezing by the age of 24 months. Although a high concentration of total ambient spores in early life was not associated with wheezing, high concentration of basidiospores and ascospores in the first 3 months was. Total pollen concentration in the first 3 months of life was also associated with increased odds of wheezing, with individual associations seen with cypress, pine and alder pollen. These associations were independent of lower respiratory illnesses and PM2.5 exposure in the first 3 months of life, both of which were also associated independently with increased odds of wheezing. Control for other seasonal factors such as dampness, cockroaches and rodents in the home did not alter these findings.
Our finding of increased odds of wheezing with elevated ambient concentrations of certain fungi is somewhat consistent with Gent et al,20 who found higher indoor concentrations of Penicillium spp and total fungi at 2–4 months of age to be associated with a greater risk of wheezing at age 1 year. Indoor fungi measurements were not included in this analysis, but ambient and indoor concentrations have been shown to be correlated and the relationship is seasonally dependent.29 Indoor concentrations of Penicillium/Aspergillus (which cannot be distinguished and are reported as one group) are often elevated in damp homes,30 which may explain why our ambient measures were not associated with early wheezing.
To our knowledge, this is the first study to examine early-life exposure to multiple outdoor fungal groups. Basidiospores are often the most abundant outdoor allergen-bearing particle and, along with ascospores, are released during rainfall or as humidity increases,31 a finding that is consistent with the crude association of early wheezing and being born in the spore season (table 1) which coincides with the rainy season in the study area. Gregory and Hirst first suggested basidiospores as possible allergen sources,32 but far less is known about the allergenicity of ascospores.30 Cladosporium spp, although present in very high concentrations in this region during the spore season, were not associated with wheezing.
Other studies also support our finding of an association between early wheezing and pollen exposure in the first months of life. Kihlström et al17 18 observed increased risk of sensitisation and allergic asthma among Swedish children exposed to unusually high levels of birch pollen in the first months of life. Although birch pollen was not detected in this region, a strong association was observed with alder pollen and early wheezing. Alder and birch are closely related, and the major allergens from members of the birch family have been shown to crossreact.33
Despite the observed associations of early wheezing and a number of antigenic spores and pollen, our Th phenotype data do not offer any insight into the likelihood that the associations are related to atopic sensitisation. The extent to which early exposure to antigens is important with respect to subsequent risks is not well established and is undoubtedly related to a complex interplay of genetic predisposition, other environmental exposures and the intensity and duration of exposure to specific allergens.34 Given the developmental processes that govern Th maturation in children35 and the fact that most of these children with early wheezing will not develop asthma later in childhood,24 36 it is not surprising that no clear association between a Th phenotype and antigen exposure was observed in this study.
We have assumed that the first 3 months of life represent the critical time period for exposure to ambient allergens, based on previous studies.34 The sequential aeroallergen seasons dictate that children with high spore exposure between birth and 3 months of age are likely to have high pollen exposure between 3 and 6 months of age. Thus, it is possible that the increased odds of wheezing associated with basidiospores and ascospores may actually represent an effect of exposure to pollen at slightly later ages. However, the seasonal pattern also offers the advantage of clearly differentiating children with high spore and pollen exposure because children born during the spore season have low early pollen exposure and vice versa. Thus, no children had a high exposure to both spores and pollen in the first 3 months of life.
An additional possibility is that other factors with seasonal patterns, such as PM2.5 or RSV, are confounding the association of pollen and spores with wheezing. PM2.5 was associated with early wheezing in this population. However, analyses of pollen and spores controlled for this variable. We were not able to control for RSV in this analysis. Wu et al5 recently showed that infants in Tennessee who were approximately 4 months of age at the peak of the RSV season were at highest risk of developing asthma by age 5, and that the seasonal birth pattern for asthma directly mirrored the pattern for RSV bronchiolitis. Wu et al found the highest risk of asthma among children born in the autumn, while our study found the highest risk among children born in the autumn and winter. The authors attributed this increase in risk to RSV exposure rather than ambient allergen exposure, which was not measured. We do not have information on the seasonal pattern of RSV infection in this population. However, if the RSV peak in our study region occurs between December and February, as it did in the Tennessee study, RSV could be another possible explanatory factor for the observed birth season pattern of asthma risk.
Few studies have examined the roles of spore, pollen and PM exposures in the early postnatal period in the development of childhood asthma or chronic wheezing. One strength of this study is that it linked date of birth to specific periods of elevated ambient allergens. We used outdoor measurements of a large number of fungal and plant groups reduced to epidemiologically relevant categories33 and time-resolved to participant data. The number of children with early wheezing in this study was small (n = 35), leading to imprecise estimation of the odds ratios. However, despite the small number of cases, we found several risk factors to be significantly associated with early wheezing. Unfortunately, atopy status as measured by skin prick testing was not available for these children, so we were unable to differentiate atopic from non-atopic wheezing. This is relevant since a large number of non-atopic children with wheezing will lose their symptoms in later childhood.36
In conclusion, we found that birth during periods of high spore or pollen concentrations was associated with wheezing at the age of 2 years in this largely Mexican immigrant population. Our Th lymphocyte data do not provide evidence that the association of early aeroallergen exposure with wheezing is related necessarily to allergic sensitisation in this group. Despite our lack of more specific data on atopic sensitisation to aeroallergens, these latter findings are consistent with the expectation that most of our subjects will lose their wheeze in later childhood, as has been observed in populations of largely European origin.36
Acknowledgments
The authors thank Z Dyer, N Kwaan, the CHAMACOS staff and students, and the CHAMACOS participants and their families, without whom this study would not have been possible.
REFERENCES
Footnotes
Funding: Funding for this study was received from the National Institute of Environmental Health Sciences (NIEHS) and the US Environmental Protection Agency.
Competing interests: None.
Ethics approval: Study procedures were approved by the University of California, Berkeley Committee for the Protection of Human Subjects.