Article Text

Statistics from Altmetric.com
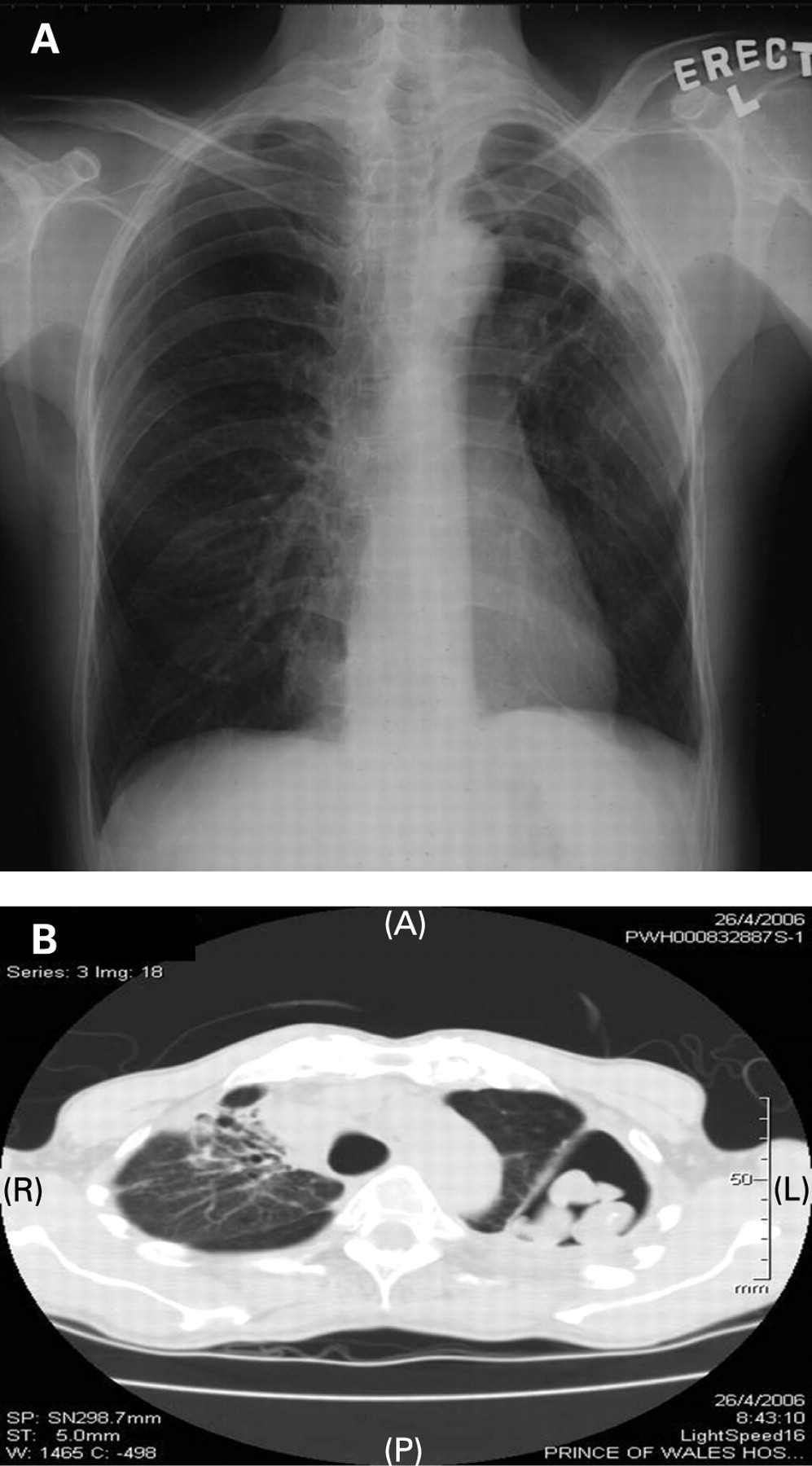
A 47-year-old man with a negative Mantoux test received infliximab 800 mg fortnightly in August 2005 for treatment of ankylosing spondylitis. He developed haemoptysis after receiving the third dose in September 2005 and therefore infliximab was stopped. CT thorax in April 2006 showed evidence of mycetoma at the left upper lobe (fig 1A, B). In view of persistent haemoptysis and radiological deterioration, voriconazole 200 mg daily was started and left upper lobe lobectomy was performed. Histopathology showed caseous granulomatous inflammation, destroyed bronchial wall with inflammatory cell infiltration and fungal mycelium was seen. Culture of the resected tissue grew Scedosporium apiospermum (fig 2A, B). Haemoptysis subsided after surgery.


{kind=link}
{kind=link}
Learning points:
Scedosporium infection may present in a wide range of pulmonary manifestations from simple colonisation to mycetoma formation and invasive disease, simulating aspergillosis.1
Antitumour necrosis factor agents should be used with caution as these may lead to opportunistic infections as a result of suppression of T cell mediated immunity.2 To the best of our knowledge, this is the first case report of pulmonary scedosporium infection as a complication of infliximab therapy for ankylosing spondylitis.
Footnotes
Competing interests: None.
Ethics approval: Ethics approval was obtained.
Patient consent: Obtained.
Linked Articles
- Airwaves