Article Text

Statistics from Altmetric.com
In patients receiving treatment for pulmonary tuberculosis (TB), change in sputum culture from positive to negative is the principal outcome measure of a therapeutic response in both clinical practice1 2 and drug trials.3 Patients will often stop producing sputum early in the course of treatment.4 We have tested the assumption that “no sputum” means that the patient is “culture negative”, as this has never been confirmed experimentally.
We prospectively followed 16 patients with newly diagnosed pulmonary TB. Sputum samples were collected at diagnosis, during weeks 1 and 2, at months 1, 2 and 4, and on completing treatment. Those patients who were not producing sputum spontaneously had specimens collected by induction. This was performed in a purpose-built negative pressure isolation chamber (Elwyn E Roberts Isolators, Shropshire, UK) where patients inhaled 3% hypertonic saline via an ultrasonic nebuliser for 20 min. Samples were homogenised with Sputasol (Oxoid, Basingstoke, UK). A dilution series was plated on 7H11 Middlebrook agar made selective with antibiotic tablets (Mycobacteria Selectatabs (Kirchner), MS24 series (Mast Diagnostics, UK)) and the viable colony count was calculated.5
The patients were divided into three groups:
Group 1: four patients who produced sputum spontaneously throughout treatment (3 men; median age 47.5 years (range 35–72); 3 Caucasian, 1 Asian; 1 HIV-positive; all sensitive to first-line TB treatment).
Group 2: four patients who never produced sputum and had induced sputum (IS) samples collected throughout (3 men; median age 38.5 years (range 23–51); 2 Black African, 1 Caucasian, 1 Jamaican; 1 HIV-positive; 3 sensitive to first-line TB treatment).
Group 3: eight patients who initially produced spontaneous sputum but underwent IS when this ceased (7 men; median age 31 years (range 17–47); 5 Black African, 2 Caucasian, 1 Asian; 1 HIV-positive; 6 sensitive to first-line TB treatment).
Patients with fully susceptible TB (n = 13) were treated with standard 6-month chemotherapy with a four-drug initial regimen. Three patients with isoniazid-resistant TB received appropriate continuation therapy.
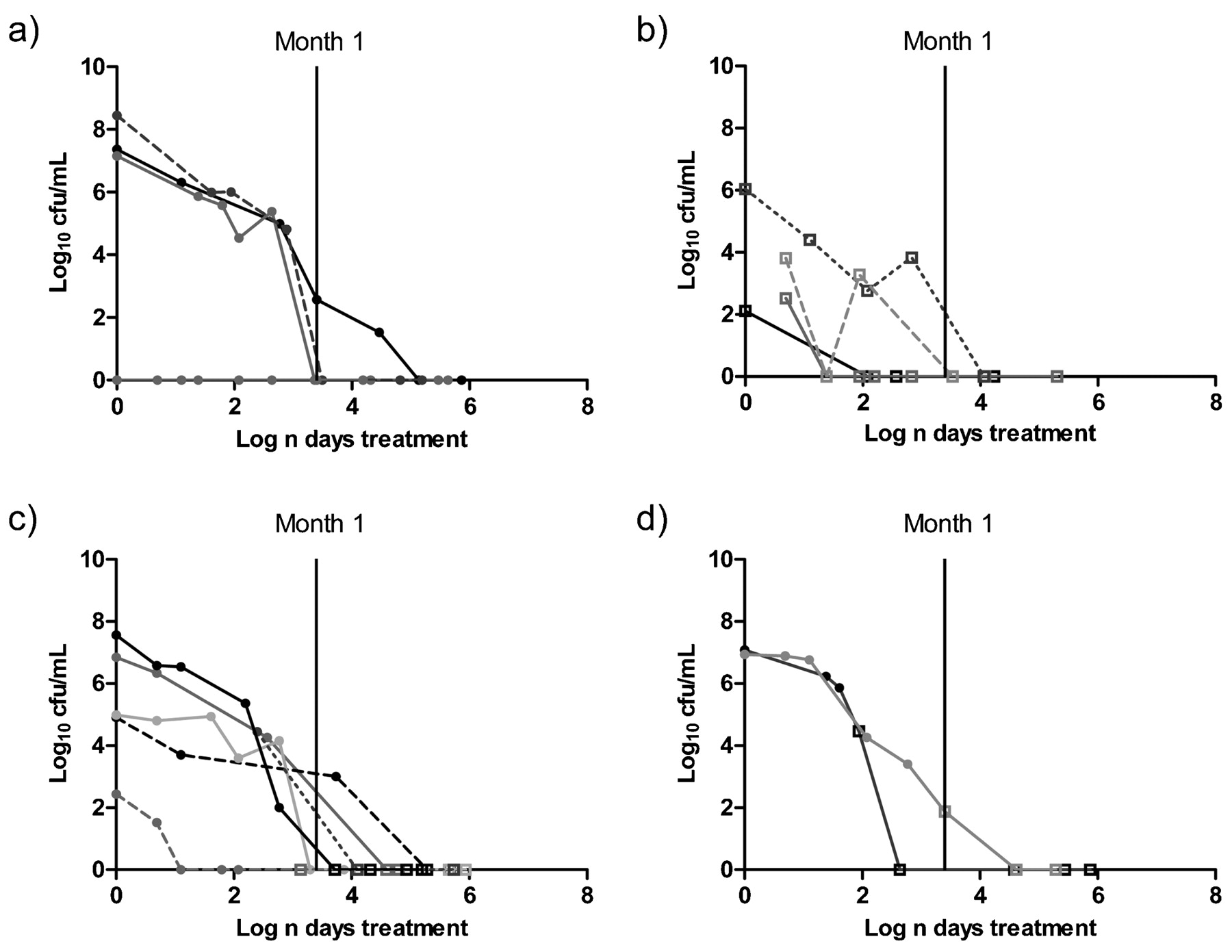
The sputum bacterial load of patients in group 1 became steadily negative during treatment, although they continued expectorating sputum throughout (fig 1a). Patients in group 2 (fig 1b) had a lower initial bacterial load, which also declined to zero on treatment. In group 3, four patients stopped spontaneously producing sputum within 1 month of starting treatment. Six of eight patients had IS samples that were repeatedly culture negative (fig 1c). Only two patients had IS samples that were culture positive; in both cases this was from a single specimen obtained within 1 month of starting treatment (fig 1d). All subsequent IS samples were then culture negative.

{kind=link}
Fall in bacterial load (log10 cfu/ml) with treatment for (a) patients in group 1 (all samples collected spontaneously; n = 4); (b) patients in group 2 (all samples collected by induction; n = 4); (c) patients in group 3 in whom all induced samples collected after spontaneous sputum stopped were culture negative (n = 6); (d) patients in group 3 in whom two samples collected within the first month of treatment (3.4 log n) were culture positive, after which all samples were culture negative (n = 2). Closed circles, spontaneous samples; open squares, induced samples.
Our data suggest that patients on appropriate treatment who stop producing sputum spontaneously are, or will shortly become, culture negative. Performing sputum induction in patients who have stopped producing sputum spontaneously rarely produces a positive result, implying that it should only be performed in patients whose clinical course is uncertain. Cessation of sputum production, especially after 1 month of treatment, appears to be a useful surrogate for culture negativity.
Footnotes
Competing interests SHG has acted as a consultant for Tibotec, has lectured at meetings sponsored by Bayer and has received funding from Tibotec and Bayer for clinical trials. FMRP was part funded by a research fellowship from Tibotec and EDCTP; neither had any involvement in the study.
Ethics approval This study was approved by the Whittington Hospital research ethics committee.
Provenance and Peer review Not commissioned; externally peer reviewed.