Article Text

Statistics from Altmetric.com
Merkel cell carcinoma (MCC) and small cell lung cancer (SCLC) share quite distinct similarities such as almost undistinguishable histological presentation (fig 1a,b) and highly aggressive biological behaviour with high rates of metastasis and poor survival rates.1 2 While tobacco smoking and genetic susceptibility have been identified as risk factors for SCLC,3 4 sun exposure and immunosuppression are the main risk factors for MCC.1 In January 2008, a new virus, called Merkel cell polyomavirus (MCPyV), was desribed by Feng et al as a likely causative agent of MCC, proving monoclonal MCPyV–genome integration in 8 of 10 MCCs.5 Since then these findings have been reproduced by several groups.6 7

{kind=link}
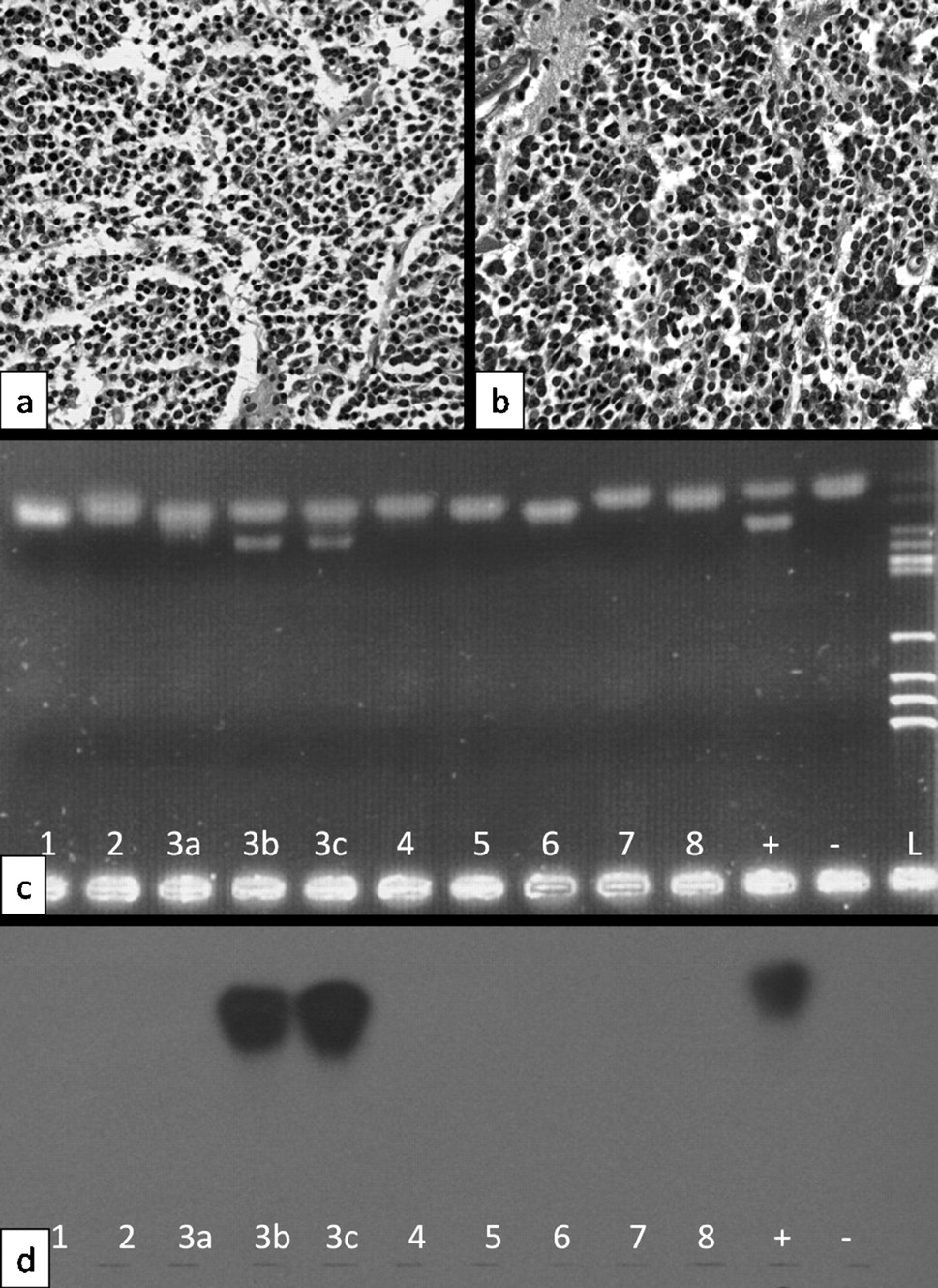
Histological features of (a) Merkel cell carcinoma (MCC; H&E staining, ×400) and (b) small cell lung cancer (SCLC; H&E staining, ×400). Both tumours are composed of highly mitotic, small basophilic tumour cells. (c) Electropherogram of a 1.5% agarose gel for MCV138 in eight patients with SCLC (three samples from patient 3) including a positive (+), and negative control (–) and an HaeIII size ladder (L). (d) Corresponding Southern blot. Samples 3b and 3c display specific PCR products, confirmed by Southern blot analysis.
Because SCLC and MCC share obvious similarities in histological presentation, Wetzels et al recently published the first report looking for MCPyV prevalence in SCLC.8 They investigated a small cohort of 10 patients with SCLC, finding no prevalence for MCPyV. We performed a molecular pathology study in a relatively large cohort of 31 patients (36 samples) analysing the presence of MCPyV DNA by PCR and chemiluminescence Southern blot hybridization of PCR products. These data are the first to test the findings of Wetzels and colleagues.
Based on the DNA sequences published by Feng et al, we designed two sets of primers in order to test the formalin-fixed and paraffin-embedded (FFPE) tissues for the presence of specific MCPyV DNA. After DNA extraction from FFPE tissues, PCR amplification using these primer combinations resulted in a 138 bp product (MCV138 forward: 5′-GGTTAGAGATGCTGGAAATGACC-3′; reverse: 5′-CAAATAAGCAGCAGTACCAGGC-3′) and a 191 bp product (MCV191 forward, 5′-CCACTTTATTATCTTAGCCCAT-3′; and reverse, 5′-TCCTTTTGGCTAGAACAGTGTC-3′) targeting the large and small T-antigen region of MCPyV (isolate MCC-Mpt-LS2). Results were confirmed by chemilumeniscence Southern blotting with specific probes for MCV138 and MCV191, omitting primer sequences and carrying a 5′ digoxigenin label (DIG-MCV138 forward, 5′-GTAAGAAGTTTAAGAAGCACCTAG-3′; and DIG-MCV191 forward, 5′-GATCTCGCCTCAAACCTCACAAG-3′). DNA quality was confirmed by β-globin PCR using the GH20 (5′-GAAGAGCCAAGGACAGGTAC-3′) and PCO4 (5′-CAACTTCATCCACGTTCACC-3′) primer set.
Of the 36 SCLC specimens, 35 revealed a β-globin PCR product. These 35 specimens were from 30 patients (13 women and 17 men, clinically not differentiated in limited and extensive disease; 2 patients with three samples each and 1 patient with two samples). Their mean (SD) age was 67.9 (8.6) years. MCPyV sequences were detected in 2 of 30 patients (7.5%), specifically in three of 35 samples (two of these three samples are from 1 patient, both positive for MCV138 (fig 1c,d) and the remaining sample was positive for MCV191). The PCR-negative controls, containing all other PCR components and water instead of DNA, were constantly negative in all experiments.
Based on the data presented here, it is unlikely that MCPyV plays a significant pathogenetic role in SCLC; nevertheless a supplemental role as cofactor in the pathogenesis of SCLC cannot be ruled out completely. Rather we assume that a MCPyV prevalence of 7.5% represents the MCPyV prevalence in the general population. We found almost identical numbers for the MCPyV prevalence in non-MCC tumours of sun-exposed skin.7 More data will be needed to prove this assumption. Nevertheless, the morphological similarities of both tumours are striking and will keep the intriguing idea of a possibly (polyoma-) virus-associated pathogenesis in mind.
Footnotes
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.