Article Text

Abstract
Rosai-Dorfman disease is a rare disorder which seems to involve not only the lymph nodes but most other organs of the body. The case history is presented of a woman who was thought to have atypical carcinoma of the lung but in whom a diagnosis of Rosai-Dorfman disease was eventually made following a range of investigations including CT scans, positron emission tomography (PET) and histological analysis of open lung biopsy specimens. She remains well with no further progression of the disease without treatment. Rosai-Dorfman disease can mimic lung carcinoma and shows increased activity on PET scanning, so histological confirmation should be sought in all cases.
Statistics from Altmetric.com
A 43-year-old non-smoking Afro-Caribbean woman was referred from the radiology department to the lung cancer clinic with an incidental finding of right hilar opacity on the chest radiograph. She had recently been seen in the emergency department for ongoing pleuritic-type chest pain when the radiograph was taken. She had been well with no major medical problems and was not taking any regular medication. She had not lost any weight and felt well in herself and denied any night sweats.
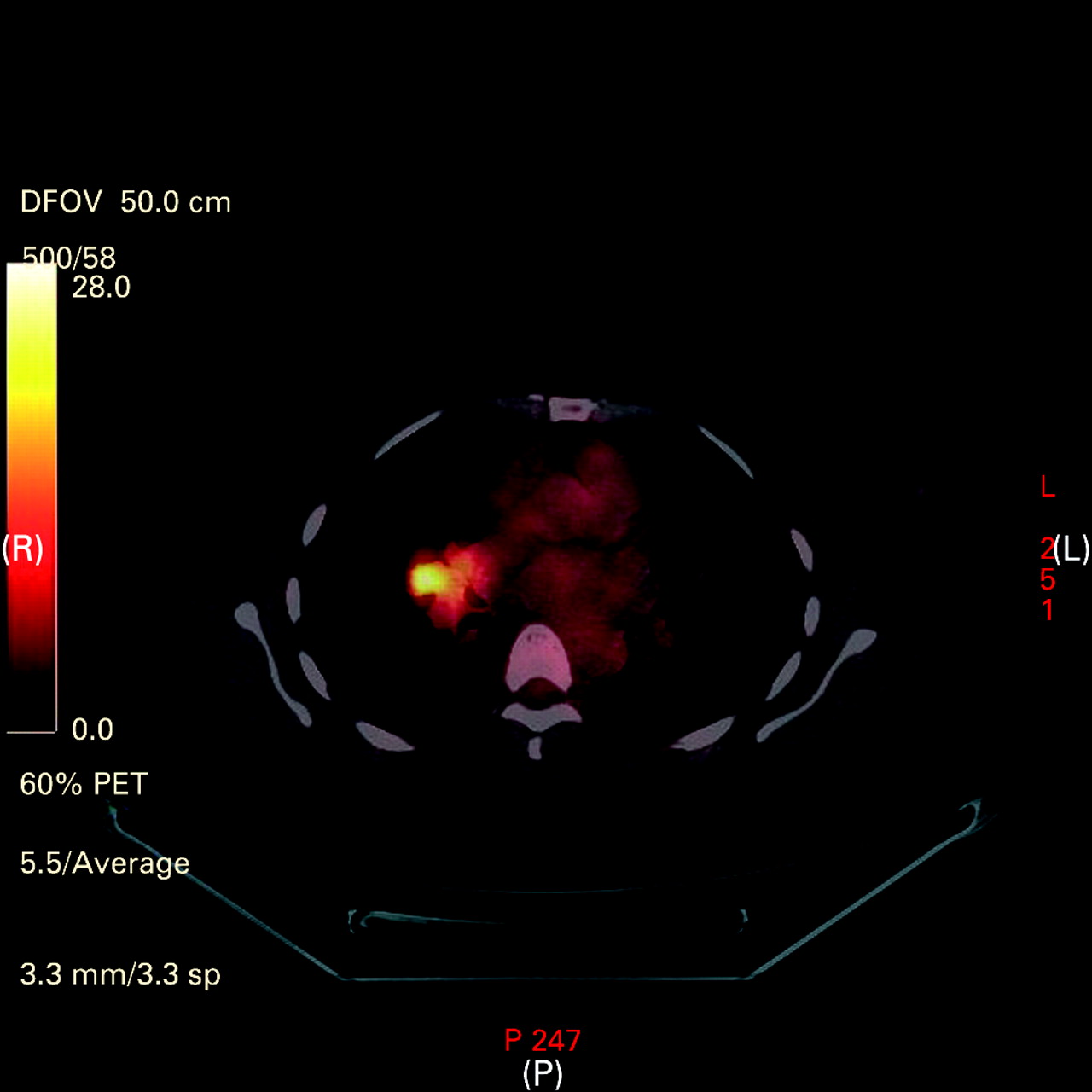
Her physical examination was normal and there was no palpable lymphadenopathy. The investigations, including renal function, liver function tests, serum calcium, C-reactive protein, full blood count and erythrocyte sedimentation rate, were all within normal limits. CT scans of the thorax and upper abdomen were performed which showed an ill-defined 30×34 mm soft tissue mass in the right hilum associated with irregularity of the middle lobe bronchus which medially was in contact with the pericardium. There was also fullness of the left retrocrural area secondary to a pathological lymph node of 12 mm. It was therefore felt to be primary carcinoma of the lung staged as T3N3M0. Flexible bronchoscopy only showed some external compression of the middle lobe bronchus. Histological examination of the right middle lobe biopsy and cytological testing of the bronchial washings failed to show any malignant cells. An 18F-fluorodeoxyglucose positron emission tomography (PET) scan also confirmed a 3.5 cm metabolically active mass in the right hilum (fig 1) and a metabolically active small adjacent lymph node. Surprisingly, another focus of high uptake was seen in the right buttock, making all these findings suggestive of metastatic lung carcinoma, but somewhat atypical.

Positron emission tomographic scan showing a right hilar mass with increased 18F-fluorodeoxyglucose uptake.
An ultrasound-guided biopsy of the right buttock mass was performed and histological analysis showed a core of adipose tissue and sheets of histiocytes with abundant pale eosinophilic cytoplasm with scattered lymphocytes and plasma cells. This was felt to be some sort of benign histiocytic proliferation independent of her thoracic and abdominal pathology. The diagnosis therefore remained unclear.
After multidisciplinary team discussion, thoracotomy was performed to obtain an open lung biopsy specimen. A mass originating from and encasing the right middle lobe bronchus was seen. It was also encircling the middle lobe bronchus and invading into the pericardium. Histological examination of a frozen section of the mass revealed benign-looking histiocytes which were similar to those in the earlier biopsy specimen from the buttock. Since pneumonectomy would have been required, and given the benign nature of the frozen section, biopsies were taken, the station 10 node was removed and the thorax closed.
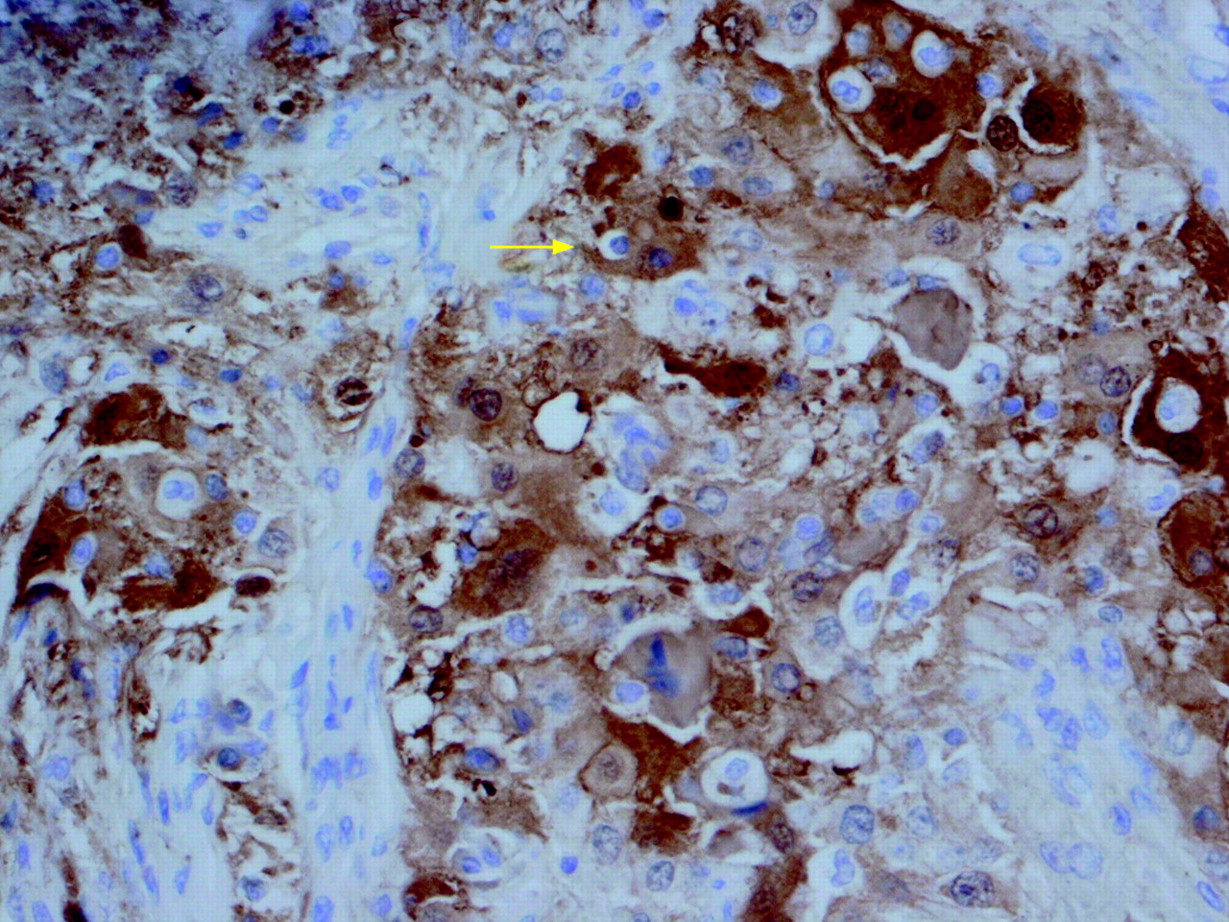
Histological analysis showed stroma expanded by a mixed population of cells including histiocytes, lymphocytes and plasma cells. No granuloma formation was seen. There was a suggestion of emperipolesis. Immunohistochemistry and special staining was performed including Ziehl-Nielsen, Wade-Fite and PAS stains showing no acid-fast bacilli or fungi. CD23 and LCA stains highlighted the histiocytes. The cells were also strongly and diffusely reactive with S100 protein with cytoplasmic and nuclear positivity (fig 2). CD68 and kappa and lambda immunohistochemistry was also tested. All these tests confirmed a diagnosis of Rosai-Dorfman disease.
{kind=link}
{kind=link}
Immunohistochemical stain for S100 protein showing emperipolesis at the top right hand corner. Magnification ×400.
The patient has not received any treatment to date and remains well with no further progression of her disease.
Discussion
Rosai-Dorfman disease, also known as sinus histiocytosis with massive lymphadenopathy, is a rare disease mostly reported in those of Afro-Caribbean descent during the first or second decade of life. The most common presentation is with bilateral massive painless cervical lymphadenopathy and fever; 25% of patients have extranodal disease. Viruses such as human herpes simplex have been associated without strong evidence,1 and the role of macrophage colony stimulating factor has also been considered as a possible trigger factor.2 It has been reported in association with HIV,3 lymphoma, amyloidosis4 and other lymphoproliferative disorders. Different extranodal sites including the skin, central nervous system, kidneys, orbit, skull, liver, pancreas and oral cavity have been reported to be involved. A case of bone marrow involvement has recently been described.5 Involvement of the larynx, lung and pleura has been reported in only a few cases,6 and the absence of massive lymphadenopathy is even more uncommon.7 Rosai-Dorfman disease shows increased uptake on the PET scan,8 which increases the suspicion of underlying malignancy as in our case.
There has been some reported benefit from the use of corticosteroids,9 but the use of chemotherapeutic agents has not proved to be beneficial. The prognosis is variable, with reported deaths10 and also a good outcome given the benign nature of the disease which tends to regress without any intervention. Our patient has remained well with no treatment and no symptomatic or radiological changes have been seen over a 2-year period.
In conclusion, Rosai-Dorfman disease is a rare disorder which seems to involve not only the lymph nodes but most other organs of the body. It can mimic lung carcinoma and even show increased activity on PET scanning, so histological confirmation should be sought in all cases given the benign nature of the disease which usually has a very good outcome.
Acknowledgments
The authors thank Dr P Naidoo, consultant histopathologist, Birmingham Heartlands Hospital NHS Trust, for all her help and support.
Footnotes
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.
Patient consent Obtained.