Article Text

Statistics from Altmetric.com
S104 THE NATIONAL LUNG CANCER AUDIT: PROGRESS IN THE FIRST 3 YEARS—DATA COMPLETENESS
1PA Beckett, 2R Stanley, 1MD Peake. 1Clinical Effectiveness and Evaluation Unit, Royal College of Physicians, London, UK, 2The Information Centre for Health and Social Care, Leeds, UK
Introduction: The National Lung Cancer Audit is an audit of lung cancer run jointly by the Royal College of Physicians and The Information Centre for Health and Social Care. Its development was driven by the realisation that lung cancer outcomes vary widely across the UK and are poor compared with other western countries. The aim of the audit is to record outcomes in lung cancer on a large scale and through case-mix adjustment, start to explain the wide variations noted. Although Wales and Scotland have recently been submitting data to the audit, this abstract presents results for England only from the first 3 years of the audit, focusing on the quality of the data.
Results: Support for the audit has grown steadily. Currently, all cancer networks in England and Wales submit data to the audit and only two trusts have never contributed. In 2005, there were 10 920 evaluable cases submitted, rising to 16 922 in 2006 and 20 639 in 2007. As seen in the table, the quality of the data has also improved.
Conclusions: The aims of collecting data on the majority of incident cases of lung cancer and mesothelioma in the UK have been achieved. Participation is now very high and data completeness has started to improve. This will allow case-mix adjustment of outcomes by trust and network to be published in the forthcoming annual report. It is hoped that this will explain previously observed geographical variations in lung cancer outcomes.
S105 CHANGES IN LUNG CANCER INCIDENCE IN SOUTH ASIANS IN LEICESTER 1990–2005
1M Day, 1J Poole, 1D Meechan, 2LK Smith, 3CM Free, 3JA Bennett, 3MD Peake. 1Trent Cancer Registry, Sheffield, UK, 2University of Leicester, Leicester, UK, 3Glenfield Hospital, Leicester, UK
Introduction: In a previous study we demonstrated that lung cancer incidence in the Leicester south Asian population was approximately 60% lower then the rest of the population for men and 70% lower for women. However, our data suggested that the incidence was rising in this population between 1990 and 1999.1 We expanded the original data to determine if the reported increased trend of lung cancer incidence in south Asians has continued to rise.
Methods: Leicester patients diagnosed with lung cancer between 1990 and 2005 were identified from Trent Cancer Registry data. Ethnicity was assigned using nam-pechan software, deprivation by Townsend score (2001). Ward level population estimates by 5-year age band, sex and ethnicity were obtained from the 2001 census. Using Poisson regression, variations in incidence by ethnicity, deprivation and period of diagnosis were then assessed, calculating the interaction between period of diagnosis and ethnicity to compare trends over time.
Results: In south Asian men, the risk of lung cancer has increased by nearly 70% for patients diagnosed between 2000 and 2005 compared with those diagnosed between 1990 and 1994 (incidence ratio (IR) 1.67, 95% CI 1.0 to 2.8) with a small fall seen in non-south Asian men (IR 0.84, 95% CI 0.8 to 0.9). The increases for south Asian men are seen across all deprivation groups, with the greatest increase in the least deprived group. There was a non-significant increase in the risk of lung cancer in south-Asian women, although numbers were small (IR 1.46, 95% CI 0.61 to 3.78), and a significant rise in lung cancer incidence in non-south Asian women (IR 1.27, 95% CI 1.1 to 1.5) (see fig).
Conclusions: Lung cancer in UK resident south Asians is increasing and may represent changing smoking habits. South Asians presenting with “red flag” respiratory symptoms and/or abnormal chest x rays should be assessed urgently and lung cancer should be considered as a possible diagnosis.

References
S106 SOCIAL DEPRIVATION AND LUNG CANCER CHARACTERISTICS: THE INSIDE STORY
J Greenwood, A Ponnuswamy, E Othman, VS Sreeguru Lakshman, I Whittle, MJ Ledson, MJ Walshaw. Liverpool Heart And Chest Hospital, Liverpool, UK
Introduction: There is a well-recognised association between deprivation and ill health and less affluent individuals are at greater risk of developing lung cancer. Using tools based on postcode to estimate deprivation, we looked at factors that might contribute to its development within the catchment of our large lung cancer unit (>400 cases per year), serving a city population of varying economic status.
Patients and Methods: We looked at smoking history, spirometry, WHO performance status, cancer stage, tumour cell type and treatment; and correlated these with the deprivation indices IMD and Health IMD provided by the local public health department in all 3441 patients (1811 men) diagnosed with lung cancer from January 2000 to April 2008.
Results: Only 6.4% were non-smokers, and 42% were still smoking at diagnosis. As regards performance status, 28% were WHO 0, 22% 1, 26.6% 2, 3.2% 3 and 3.7% 4. Although 30% had clinical diagnoses, 23% were adenocarcinoma, 22% squamous, 10.5% small cell and 14.5% miscellaneous. Stage at presentation was 1a 3%, 1b 5.2%, 2a 0.6%, 3a 4%, 3b 6.7% and 4 15.6%. Although 11% were resected and 30% underwent radical oncological treatment, the remainder were offered palliation only. As regards deprivation, IMD and Health IMD scores ranged from 8.45 and 0.8 to 87.4 and 3.6 (least deprived to most deprived, respectively). Univariate analysis revealed that the most deprived had a worse performance status and spirometry (paired data available for 1504 patients), were more likely to be smokers and had a more advanced stage of cancer (paired data available for 643 patients) and were more likely to be clinical diagnoses, but when histology was obtained there was a preponderance of small cell and squamous subtypes.
Conclusion: In this large cohort of lung cancer patients, those who were socially and economically deprived presented later in the course of their disease and were less fit than more affluent patients. Such factors militate against effective treatment for this patient group and illustrate the urgent need for strategies to improve the economic and social wellbeing of population groups who are at risk of lung cancer.
S107 PLEURAL FLUID MESOTHELIN LEVELS: DIAGNOSTIC ACCURACY, REPRODUCIBILITY AND RELIABILITY AFTER PLEURODESIS
1HE Davies, 2RS Sadler, 1CE Manners, 1RJO Davies, 2BL Ferry, 1YCG Lee. 1Oxford Centre for Respiratory Medicine, Churchill Hospital, Oxford, UK, 2Department of Immunology, Churchill Hospital, Oxford, UK
Serum measurement of soluble mesothelin, a new biomarker for mesothelioma, is FDA approved for clinical use. Mesothelin is released from pleural mesotheliomas; thus the measurement of pleural fluid mesothelin has potential advantages over serum quantification.
Aims: To determine the utility of pleural fluid mesothelin level by assessing its diagnostic value in unselected patients with undiagnosed pleural effusions, short-term reproducibility and longitudinal change with time and variation after pleurodesis.
Methods: Mesothelin concentrations were determined in 408 pleural fluid and 64 serum samples by ELISA (CIS Bio, France). Pleural fluid was prospectively collected from patients (n = 167) presenting with an undiagnosed pleural effusion. Serial pleural fluid samples were obtained from patients (n = 34) who had an indwelling pleural catheter or repeated thoracentesis. Pleural fluid and blood mesothelin levels were measured in 32 patients before and after talc pleurodesis.
Results: Pleural fluid mesothelin concentrations were significantly higher (p<0.001) in mesothelioma patients (n = 24) than those with metastatic carcinomas (n = 67) and benign effusions (n = 75): median (interquartile range) 40.3 (18.3–68.1) versus 6.1 (1.5–13.2) versus 3.7 (0–12.4) nmol/l, respectively. At the optimal cutoff (20 nmol/l), pleural fluid mesothelin has an excellent diagnostic sensitivity (71%) and specificity (90%) for mesothelioma. Pleural fluid mesothelin measurement provided additional value over cytological analysis. In pleural fluids with “suspicious” (but not definite malignant) cytology (n = 11), pleural fluid mesothelin levels greater than 20 nmol/l were 100% specific in diagnosing mesothelioma. In cytology-negative effusions (n = 94), pleural fluid mesothelin offered negative and positive predictive values of 94% and 75%, respectively, for mesothelioma. Intra-individual reproducibility was excellent. In serial pleural fluid samples obtained within 7 days, mean (SD) variation of mesothelin was −0.11 (8.42) and 0.76 (6.02) nmol/l in mesothelioma and non-mesothelioma patients, respectively. Pleural fluid mesothelin levels increased significantly with time (r = 0.60, p<0.001) in mesothelioma patients. Talc pleurodesis did not significantly alter mesothelin levels in pleural fluid or serum (median change −5.78 and 0.0 nmol/l, respectively).
Conclusion: Pleural fluid mesothelin provides additional diagnostic value for mesothelioma over cytological examination. Mesothelin measurements are highly reproducible in the short term (<7 days), are not affected by pleurodesis and increase over time in mesothelioma patients reflecting disease progression.
S108 A PHASE I TOXICITY, DOSE FINDING AND PRELIMINARY EFFICACY ASSESSMENT OF LIPOTEICHOIC ACID-T FOR PLEURODESIS IN MALIGNANT PLEURAL EFFUSION
1NM Rahman, 1HE Davies, 2M Salzberg, 1EL Hedley, 3P Truogg, 4R Midgley, 5D Kerr, 6C Clelland, 1RJO Davies. 1Oxford Centre for Respiratory Medicine, Oxford, UK, 2Pharma Brains Ltd, Basel, Switzerland, 3Lunamed, Switzerland, 4Cancer Research UK, Oxford, UK, 5Department of Clinical Pharmacology, Oxford University, Oxford, UK, 6Department of Clinical Pathology, Oxford Radcliffe Hospitals, Oxford, UK
Background: Lipoteichoic acid T (LTA-T) is a pro-inflammatory Gram-positive bacterial cell wall motif that acts through the Toll-like receptor pathway. LTA-T may be a trigger for the pleural inflammation seen after pleural infection, resulting in a fibrosed pleural cavity. We hypothesised that intrapleural LTA-T administration could control malignant pleural effusion (MPE) by inducing pleurodesis.
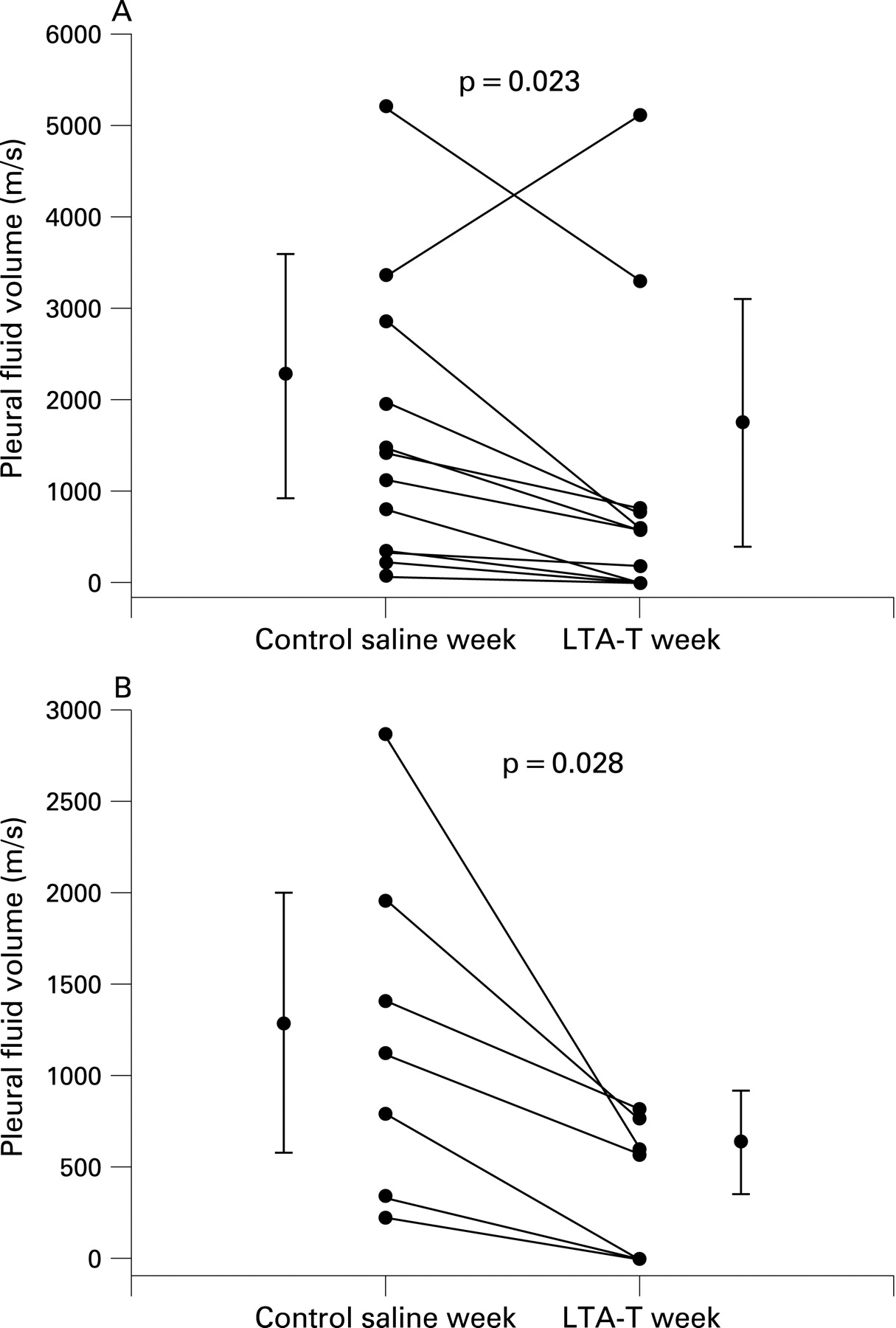
Method: This study was a dose escalation and toxicity study performed in 13 patients with MPE requiring drainage. An indwelling pleural catheter was placed and a “control” (intrapleural saline) was administered; pleural fluid production then was recorded for 7 days (week 1). An escalating single dose of intrapleural LTA-T was administered on day 7; fluid production was recorded over the next week (week 2), and long-term fluid control assessed. The primary outcome measure was toxicity and safety profile.
Results: Dose was limited by toxicity at 3000 μg single dose (systemic inflammatory reaction requiring hospital admission). Therapeutic dose was 750–1500 μg with only mild and inconsistent side effects at this dose. Pleural fluid production decreased significantly after intrapleural LTA-T compared with saline alone (fig), and this was due to a reduction in those receiving 750 μg or more LTA-T (saline control week 1244 ml, SD 933, LTA-T week 394 ml, SD 375, diff 850 ml, SD 699, 95% CI 204 to 1497, p = 0.018, fig). 86% of patients treated with LTA-T achieved pleural fluid control for at least one month.
Conclusion: A single dose of intrapleural LTA-T has a mild and favourable toxicity profile when compared with standard pleurodesis agents and may induce effective pleurodesis in MPE. Further larger scale studies are now required using this agent.

{kind=link}
{kind=link}