Article Text

Statistics from Altmetric.com
P69 CAN CHANGES IN SPIROMETRY OVER TIME BE INTERPRETED USING CROSS-SECTIONAL REFERENCE DATA?
1S. Stanojevic, 1T. J. Cole, 1A. Wade, 1C. Bastardo, 2A. Prasad, 3P. H. Quanjer, 1J. Stocks. 1UCL Institute of Child Health, London, UK, 2Great Ormond Street Hospital, London, UK, 3Sophia Children’s Hospital, Rotterdam, The Netherlands
Background: Serial spirometry measurement can facilitate the identification of individuals with rapid lung function decline. In clinical practice, however, repeated measurements are commonly interpreted using cross-sectional reference data, despite well recognised limitations (Van Pelt et al. AJRCCM 1994).
Aim: To assess adjustments for the correlated nature of repeated measurements in order to interpret changes over time using cross-sectional reference data.
Methods: Normal lung growth can be viewed as roughly a constant Z-score (adjusted for height, age and sex) over time, with the uncertainty around the change normally distributed around a mean change of 0 Z-scores. The standard deviation of the change depends on the correlation (r) between the two measurements (Cole, Human growth in context, 1998). The adjusted Z-score for change (Zc) adjusts the observed Z-score change for the baseline Z-score and the interval between measurements. Spirometry data from 938 healthy, white subjects (aged 5–18 years) measured twice over time intervals 0.1 and 5 years, were collated to estimate the occasion-to-occasion correlation coefficient (r) for FEV1 Z-score (Stanojevic et al. AJRCCM 2008). Measurements less than one year apart had an r value of 0.90, such that normal within-subject variability in health after one year is 0 ± 0.88 Z-scores. Changes in spirometry were also assessed after a one-year interval in 98 children with cystic fibrosis (aged 4–12 years) to determine the clinical implications of using the Zc.
Results: Based on a cross-sectional cut-off of <−1.64 Z-scores, 32/98 patients had an abnormal result at baseline, of whom 21 remained abnormal after one year. Of those with normal results at baseline, 10 had abnormal results at follow-up. Using Zc, 31 subjects declined significantly in lung function (<−1.64 Zc), of whom 22 were normal and nine were abnormal at baseline. Most importantly, 14 subjects classified as “normal” on both test occasions using the cross-sectional cut-off had significant lung function decline using Zc. Zc also identified 23 subjects with improving lung function.
Conclusion: Adjusted Z-scores for change take into account previous results and facilitate interpretation of lung function over time and appear to be more sensitive at detecting lung function deterioration than cross-sectional Z-scores.
Funding: This study was funded by Asthma UK.
P70 OXYGEN UPTAKE RESPONSES IN CHILDREN WITH CHRONIC CHEST DISEASES FOLLOWING SIMULATED SPORTING ACTIVITY
1P. J. Oades, 2D. Stevens, 2C. A. Williams, 2N. Armstrong. 1Royal Devon and Exeter Foundation NHS Trust, Exeter, UK, 2CHERC, University of Exeter, Exeter, UK
Introduction: Oxygen uptake (VO2) during moderate steady-state exercise (SSE) has been used to assess recovery following more strenuous exercise. Understanding how children with chronic chest diseases (CCD) recover from exercise may provide insight into physiological disturbance in disease. This study aimed to investigate the SSE VO2 responses over 24 h following a period of repetitive short burst physical activity that simulated typical sport in children with CCD and healthy controls.
Methods: Twenty-seven children with stable CCD (19 cystic fibrosis (CF) and eight non-CF bronchiectasis; age 12.7 ± 3.1 years; FEV1 82 ± 23% PR) and 25 controls (age 13.4 ± 3.3 years, FEV1 102 ± 12% PR) performed simulated sporting activity (SSA) by exercising on a cycle ergometer repeatedly for 2-minute periods at moderate-to-heavy intensity (∼50% DGET-VO2peak) with 1 minute of rest between bursts. Participants attempted to complete up to 10 exercise bouts and then performed three identical moderate intensity SSE tests (∼80% GET) at 3 minutes (test 1), 1 h (test 2) and 24 h (test 3) post SSA. During each test VO2 was measured continuously by on-line respiratory gas analysis.
Results: Aerobic capacity was significantly lower in the CCD group than in the controls. Repeated measures analysis of variance and subsequent Tukey tests revealed, in the children with CCD, a significant increase in VO2 between test 1 and test 2 (0.78 ± 0.26 to 0.83 ± 0.28 l/minute, p<0.01), followed by a significant decrease between test 2 and test 3 (0.83 ± 0.28 to 0.79 ± 0.28 l/minute, p<0.01). Test 3 VO2 remained elevated above test 1 VO2 but not significantly (0.79 ± 0.28 to 0.78 ± 0.26 l/minute). The controls showed a sequential and significant decrease in VO2 between tests 1 and 2 (1.15 ± 0.38 to 1.07 ± 0.32 l/minute, p<0.01) and tests 2 and 3 (1.07 ± 0.32 to 1.03 ± 0.32 l/minute, p<0.05).
Conclusions: SSE VO2 responses following SSA differ between children with CCD and controls. Children with CCD demonstrate persistent elevation of VO2 during constant intensity exercise for 24 h following SSA.
P71 EARLY RECOVERY OF OXYGEN UPTAKE FOLLOWING EXERCISE TESTING IN CHILDREN WITH CHRONIC CHEST DISEASES
1D. Stevens, 2P. J. Oades, 1N. Armstrong, 1C. A. Williams. 1CHERC, University of Exeter, Exeter, UK, 2Royal Devon and Exeter Foundation NHS Trust, Exeter, UK
Introduction: The value of exercise performance as a measure of wellbeing in patients with chronic chest diseases (CCD) is becoming increasingly recognised. Many studies to date have concentrated on peak aerobic capacity (VO2peak) as a measure of fitness. Our aim was to investigate changes in oxygen uptake (VO2) during early recovery following exercise and relate them to VO2peak and markers of disease severity.
Methods: 19 patients with cystic fibrosis (CF) (aged 13.1 ± 2.9 years; 10 female) and eight children with other stable CCD (aged 11.1 ± 2.2 years; seven female) underwent maximal cardiopulmonary exercise testing on a cycle ergometer. VO2 was measured before, while exercising to VO2peak and during recovery. Early VO2 recovery was quantified by the time in seconds to reach 50% of the VO2peak value. Early VO2 recovery was correlated against lung function (FEV1 % predicted) and VO2peak (ml/minute/kg). Disease severity was graded in the CF group by the Shwachman score (SS).
Results: In the CF group the SS was significantly correlated with early VO2 recovery (r = −0.63; p = 0.004) and FEV1 (r = 0.72; p = 0.001). FEV1 was significantly lower in the CCD group compared with the CF group (68 ± 21 vs 87 ± 21% predicted, respectively; p = 0.044), yet no significant differences were found between the CF and CCD groups for VO2peak (34.7 ± 8.0 vs 35.9 ± 8.4 ml/kg/minute, respectively; p = 0.715) and early VO2 recovery (58 ± 16 vs 56 ± 16 s, respectively; p = 0.755).
Conclusion: In young CF patients, early VO2 recovery following maximal exercise and FEV1 are significantly related to disease severity. FEV1, however, does not fully reflect exercise performance and recovery in young patients with CF and other CCD. Measures of recovery following exercise may enhance our objective assessment of functional impairment in those with cardiopulmonary disease and deserves further research.
P72 DOES ETHNICITY INFLUENCE LUNG FUNCTION IN PRESCHOOL CHILDREN?
1C. M. Bastardo, 2S. Sonnappa, 2P. Aurora, 1J. Stocks. 1Department of Respiratory Medicine, UCL Institute of Child Health, London, UK, 2Departments of Respiratory Medicine, UCL Institute of Child Health and Great Ormond Street Hospital for Children, London, UK
Introduction: Guidelines for assessing lung function (LF) in preschool children have been published recently1 but little is known about the influence of ethnic background on LF in this age group.
Methods: LF was assessed using multiple breath washout (lung clearance index (LCI) and functional residual capacity (FRC)), whole body plethysmography (specific airways resistance; sRaw) and spirometry (FVC, FEV1 and FEF75–25) in healthy white and south Asian preschool children between 4 and 6 years, recruited from the local community. Spirometric parameters were expressed as Z-scores adjusted for height, age and sex.2 Statistical analysis was by t test and multiple linear regression (MLR).
Results: 37 white children (median age 5.78 years, range 4.39–6.99, 51% female) and 31 south Asian (median age 5.45 years, range 4.09–6.89, 48% female) were recruited. MLR showed significant differences between white and south Asian children for FVC and FEV1 but not for other LF measurements. However, after adjusting for age, sex and height, significant differences between the two ethnic groups were seen for all spirometry outcomes but other LF measurements continued to remain similar, although height was a significant predictor for most outcomes. (see table). Differences were also apparent when expressing spirometric outcomes as Z-scores, with FVC and FEV1 being 0.7 (95% CI 0.09 to 1.23) and 0.7 (95% CI 0.15 to 1.19) lower in the Asian than white children, whereas FEF75–25 Z-scores were similar (0.39; 95% CI −0.40 to 1.01).
Conclusions: Spirometry measurements are lower in south Asian than white healthy preschool children but other LF measures appear to be similar. These ethnic differences should be taken into account to prevent errors in interpretation of LF measurements.
1. Beydon, et al. Am J Respir Crit Care Med 2007;175:1304–45.
2. Stanojevic, et al. Am J Respir Crit Care Med 2008;177:253–60.
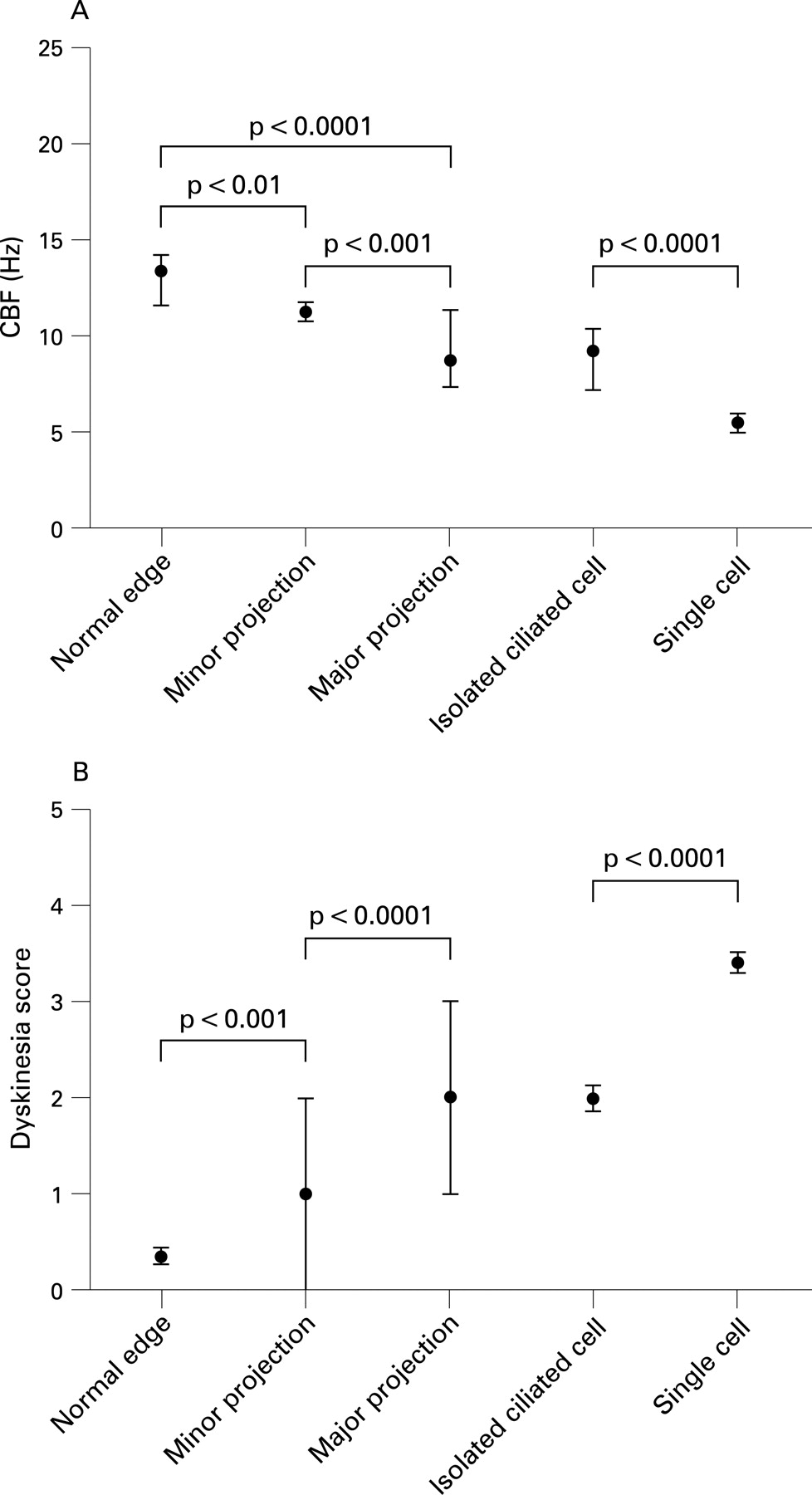
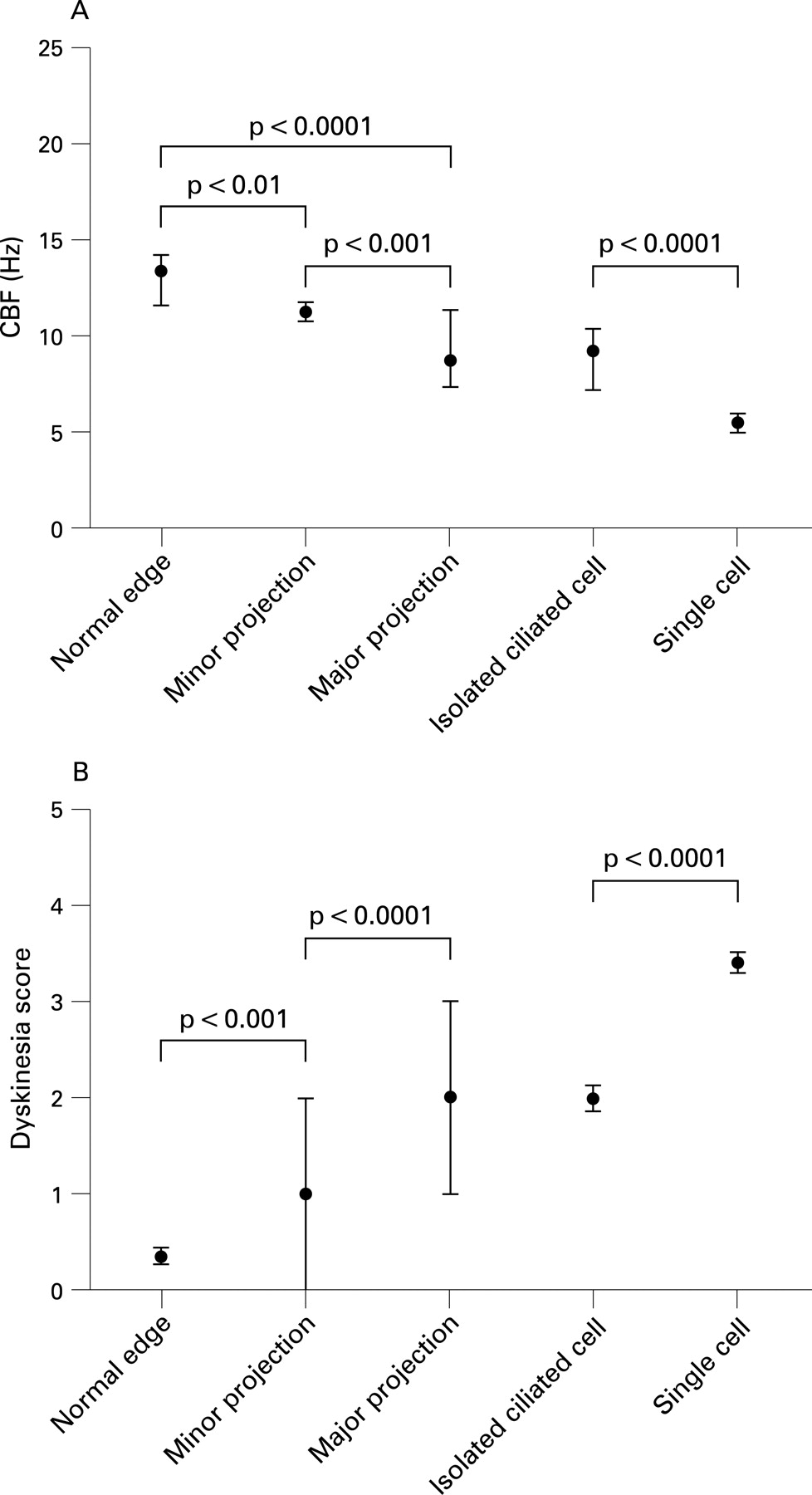
P73 DISRUPTION OF CILIATED EPITHELIAL EDGES RESULTS IN A SLOWER CILIARY BEAT FREQUENCY AND INCREASED CILIARY DYSKINESIA
B. Thomas, A. Rutman, C. O’Callaghan. University of Leicester, Leicester, UK
Introduction and Objectives: Ciliary function studies for the diagnosis of primary ciliary dyskinesia (PCD) are performed on nasal brush biopsy samples. Whereas in many cases intact uniform ciliated edges are observed, disrupted edges are also seen.
Aim: To determine if cilia on disrupted edges beat with a normal beat pattern and frequency similar to that of cilia on undisrupted edges.
Methods: Nasal brush biopsy samples from 42 children in whom the diagnosis of PCD was excluded were assessed. Samples were categorised into five groups: a normal ciliated edge (>50 μm in length); a ciliated edge (>50 μm in length) with minor cellular projection; a ciliated edge (>50 μm in length) with major cellular projection; an isolated ciliated cell on an epithelial strip >50 μm in length and single unattached ciliated cells. Ciliary beat frequency (CBF) and beat pattern of 50 samples from each group were determined using a high speed digital video microscopy system. The percentage of dyskinetically beating cilia in each sample was assessed and expressed as a dyskinesia score (0, normal beat pattern throughout the sample; 1, dyskinetic beat pattern in ⩽25% of the cilia; 2, dyskinetic beat pattern in ⩽50% of the cilia; 3, dyskinetic beat pattern in ⩽75% of the cilia and 4, dyskinetic beat pattern in all cilia).
Results: See table and fig. A significantly lower CBF and a significantly higher dyskinesia score were observed in all sample types compared with that of a normal ciliated edge.
Conclusions: If ciliary beat frequency is measured and beat pattern assessed from cilia that are not part of an intact undisrupted strip of ciliated epithelium, the results should be viewed with caution.
P74 HIGH-RESOLUTION COMPUTED TOMOGRAPHY IN CHILDREN WITH CONFIRMED POST-INFECTIOUS OBLITERATIVE BRONCHIOLITIS
1M. Brodlie, 2M. Muller, 2N. Byrne, 2L. Mitchell, 2D. A. Spencer. 1Newcastle University, Newcastle upon Tyne, UK, 2Freeman Hospital, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK
Introduction: Postinfectious obliterative bronchiolitis (OB) is an irreversible small airway disease associated with persistent wheeze, cough and dyspnoea occurring after a discrete infection in infancy associated with characteristic high-resolution computed tomography (HRCT) changes and having excluded all other relevant conditions. The clinical course of OB in children is not well described.
Objective: To describe the features and progression of HRCT findings in a cohort of children with OB.
Methods: Children with OB were identified from a unitary database. A consultant radiologist reviewed all HRCT scans independently and scored each lobe (0, none; 1, mild; 2, moderate; 3, severe) for mosaicism (inspiration), mosaicism (expiration), bronchiectasis (peripheral or central), bronchial wall thickening and tree-in-bud sign.
Results: A total of 13 children was identified, 12 post-adenovirus and one post-Mycoplasma pneumoniae. 21 scans were reviewed. Serial scans were performed in eight children. When present bronchiectasis and the tree-in-bud sign occurred in the same lobes affected by OB. Peripheral bronchiectasis was identified in 17 (81%) scans, in contrast to classic radiological teaching that bronchiectasis is usually central in OB. When considering individual lobes in serial scans (median of 37 months apart), bronchiectasis improved in five, deteriorated in three and was unchanged in 25; bronchial wall thickening improved in two, deteriorated in six and was unchanged in 34. Expiratory scans revealed more severe OB in 43% of lobes compared with inspiratory views and in 12% this provided the only evidence of OB. When considered alone, OB was present in 71% of inspiratory scans, 62% of expiratory and 73% of dual inspiratory and expiratory scans combined.
Conclusions: Bronchiectasis is common in OB and is usually peripheral in nature. Bronchiectasis and the tree-in-bud sign occur in the same lobes as mosaicism. To optimise the detection of OB inspiratory and expiratory scans should both be performed if possible. In a moderate number of children bronchiectasis improved over time and this justifies the practice of performing repeat scans. Clearly, this should be balanced against the risks of increased radiation exposure however.
P75 MONITORING FOR TREATMENT COMPLICATIONS IN CHILDREN WITH SEVERE CHRONIC ASTHMA
S. J. Moss, M. C. McKean, C. O’Brien, D. A. Spencer. Newcastle upon Tyne Hospitals NHS Trust, Newcastle upon Tyne, UK
Introduction and Methods: Potential adverse effects of long-term systemic and high dose inhaled corticosteroids in chronic asthma are well documented. Other potentially toxic agents such as methotrexate are increasingly used in paediatric practice. We suspected that screening for treatment-related adverse effects was not being performed in a consistent manner and therefore undertook a retrospective case note review of patients in our tertiary paediatric respiratory clinics to obtain baseline data for future audit. All patients had confirmed chronic severe asthma requiring treatment at step 5 or above of the BTS asthma guidelines.
Results: 31 patients (median age 12.5 years (2–17), 23 male) were maintained on a median daily dose of 5 mg prednisolone and had received a median of three booster courses in the past year. Nine patients were receiving omalizumab, three subcutaneous methotrexate and four continuous subcutaneous terbutaline. 29% of patients were <9th centile for height, and 27% were >98th centile for weight. 22% of patients who had dual x ray absorptiometry scans had a lumbar spine density Z score of ⩾−2. No patients were found to be hyperglycaemic. Raised blood pressure was documented intermittently in 20% of patients, but no persistent hypertension was detected. Significant cutaneous infection occurred in one patient rendered lymphopenic by methotrexate therapy. 10 patients underwent assessment of adrenal function and this was abnormal in three. The presence of Cushingoid features, myopathy, cataracts and depression were not well documented.
Conclusions: Performance and documentation of monitoring for potential treatment-related adverse effects was not conducted in a consistent manner in our patient group. A more robust method of monitoring to include a formal annual review of therapy is required.
{kind=link}
{kind=link}
P76 OUTCOME OF CONFIRMED CONGENITAL CYSTIC ADENOMATOID MALFORMATION OF THE LUNG IN THE NORTHERN REGION OF ENGLAND: 22 YEARS EXPERIENCE, 1985–2006
J. Mangalore Devdas, B. Ray, P. Hammond, M. Ward-Platt, M. C. McKean. Royal Victoria Infirmary, Newcastle upon Tyne, UK
Objectives: To establish the natural history of confirmed congenital cystic adenomatoid malformation (CCAM) cases in the northern region of England over a 22-year period from 1985 to 2006 inclusive.
Methods: This population-based study identified cases for subsequent review using the prospectively collected regional NorCAS (Northern Congenital Anomaly Survey), fetal medicine databases and hospital admission records.
Results: Thirty-seven cases of CCAM were confirmed by computed tomography scan (or with histopathological/postmortem confirmation). Twenty-six (70%) had been accurately identified by antenatal ultrasound scans. Twenty-nine (78%) were live births. Six cases died postnatally (16% of total cases; 20% of live births), all were premature (mean gestation 29 weeks). Ten subjects (27% of total; 35% of live births) required surgical excision. Thirteen (35% of total; 45% of live births) have been managed conservatively, are alive and well with mean age at last follow-up of 2.3 years. Mean maternal age, gestation and birth weight were 27 years, 36 weeks and 2900 g, respectively. The apparent prevalence of confirmed CCAM in the north of England is one in 25 000 live births. CCAM is more common in females (62%), the left lower lobe (39%) and right lower lobe (32%). Sixty per cent developed symptoms, 44% in the first year of life. The commonest symptoms were recurrent respiratory tract infection (30%). Two cases developed pneumothorax and one lung abscess. In subjects who had surgical intervention (80% in the first year of life) half were symptomatic in the neonatal period. Two patients had major postoperative complications; one with bleeding into the pleural cavity requiring re-exploration and another with bronchopleural fistula requiring chest drain insertion. One patient developed pectus excavatum following surgery. No fatalities resulted from surgery. Resected specimens allowed histopathological Stocker classification: 50% type 2, 30% type 1.
Conclusions: Few population-based studies on the prevalence of CCAM are available in the literature. The apparent prevalence of CCAM in the northern region of England is one in 25 000 live births. Thirty-five per cent of live births required surgery, most being symptomatic in early life. Prematurity contributed significantly to mortality in CCAM. Good surgical outcomes were observed. This study provides valuable information for counselling parents.
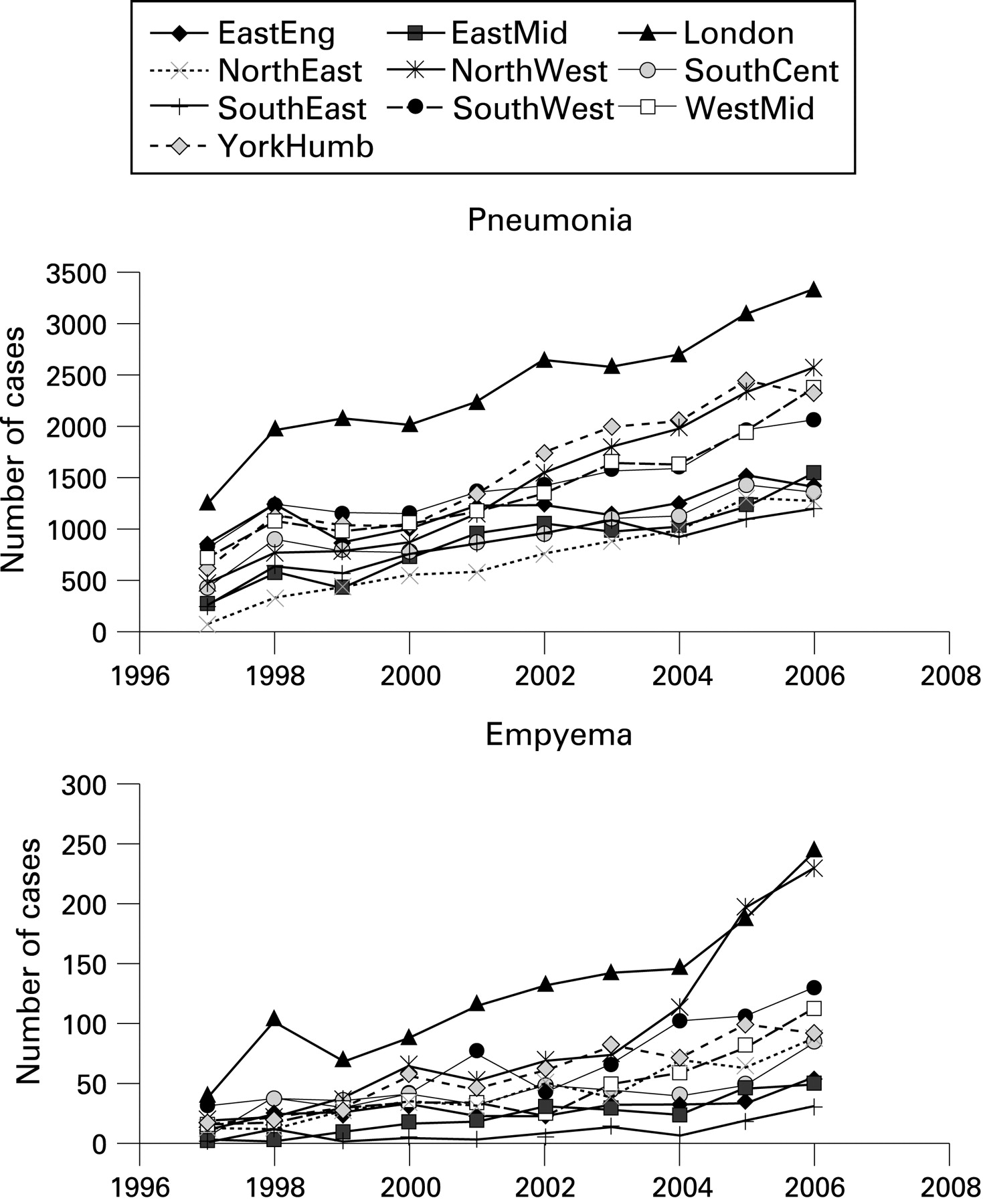
P77 MODELLING OF INCREASING PAEDIATRIC EMPYEMA AND PNEUMONIA ADMISSIONS IN ENGLAND 1996–2006 USING HOSPITAL EPISODE STATISTICS
1S. P. Rushton, 1D. Cliff, 1M. D. F. Shirley, 1M. Pearce, 2R. Gorton, 3J. Clark, 3D. A. Spencer. 1Newcastle University, Newcastle upon Tyne, UK, 2Health Protection Agency, North East, UK, 3Newcastle Upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK
Empyema thoracis is increasing in children in the developed world, although the reasons for this are unclear. We investigated trends in the number of cases for England over the period 1997–2006 in relation to pneumonia admissions.
Data on paediatric pneumonia and empyema were obtained from the hospital episode statistics database for the period 1997 to 2006. We used linear mixed effect (LME) models to investigate trends in individual strategic health authority areas (SHA) and relate these to changes in the background weather and baseline pneumonia cases using the SHA as a random effect.
The rise in cases of empyema in all SHA was exponential over this period (t = 7.943; p<0.000) although the pattern of increase was not homogenous. An LME with the mean temperature in each SHA for the month prior to the admission of cases was a significant predictor (t = −12.815, p<0.000) of the heterogeneous variation if we assumed an exponential model for the basic trend through time (correlation between predicted and observed cases 0.74, t = 3667, p<2.2 × 10−6). Rates of increase were high in the north and west, although the rate of increase in admissions in London was high relative to that of other southern health authorities. The incidence of pneumonia also increased in the same time period, but this did not explain the increasing trend in empyema cases (see fig).
It is possible that differences in environmental and health and social deprivation across the country are responsible for the differences in rates of both pneumonia and empyema observed across the UK, although the exponential nature of the increases suggests that other factors such as changes in the causative organisms themselves may be responsible. Enhanced paediatric pneumococcal empyema surveillance is now in place across the UK, but these data suggest that a similar system should also be implemented for all paediatric pneumonia.
P78 A METHODOLOGY FOR A NATIONAL DATABASE FOR CHILDHOOD ASTHMA
1S. W. Turner, 1R. Leece, 2C. Palmer, 1J. G. Ayres, 1T. Macfarlane, 2A. Mehta, 2G. Mehta, 3S. Cunningham, 4S. Mukhopadhyay. 1University of Aberdeen, Aberdeen, UK, 2University of Dundee, Dundee, UK, 3Royal Edinburgh Hospital for Sick Children, Edinburgh, UK, 4University of Brighton, Brighton, UK
Introduction: Childhood asthma is a common condition in which studies of large populations have demonstrated that causation is likely to involve genetic and environmental factors. Combinations of genetic and environmental factors may also be relevant to disease heterogeneity within the asthma population but this hypothesis remains untested; to do this would require a large study population. Here we present preliminary data that demonstrate the feasibility of establishing a national database to study gene–environment interactions in childhood asthma.
Methods: Children aged 2–16 years and with an asthma diagnosis from a respiratory paediatrician were recruited from 15 centres across Scotland. Children with other respiratory conditions were excluded. Asthma, quality of life and dietary questionnaires were completed and returned by post. Children attended an assessment when free of symptoms. The assessment was carried out by a research nurse and included spirometry, bronchodilator response, exhaled nitric oxide (ENO) and skin prick testing. Saliva was collected for cotinine assay and DNA extraction. A database was developed adhering to established protocols created for the UK Cystic Fibrosis database.
Results: At the time of writing, 96 children had been invited to participate, of whom questionnaires were returned in 48, mean age 10 years. Spirometry was measured in 28 children (mean FEV1 94% (SD 18)), bronchodilator response in 27 (mean change 6% (SD 9)), ENO in 26 (mean 35 parts per billion (SD 33)) and skin testing in 23 (21 skin prick positive). Saliva was obtained in 40 children.
Conclusions: We have established our methodology and demonstrated the feasibility of creating a national database to study childhood asthma. Recruitment continues and we aim to create one of the largest cohorts of asthmatic children for study of gene–environment interactions.
P79 DEVELOPMENT OF A CENTRALISED WEB-BASED DATABASE MANAGEMENT SYSTEM FOR RESPIRATORY RESEARCH PROJECTS
1S. Lum, 2R. White, 2T. Small, 1J. Stocks. 1Portex Respiratory Unit, UCL, Institute of Child Health, London, UK, 2J7IS Ltd, London, UK
Over the past decade, we have developed various relational databases to manage physiological and clinical data relating to lung development in health and disease. However, the retrieval of increasingly complex data has become problematical, exacerbated by software incompatibilities and changes in research directives.
Aim: To develop a data management system for research and clinical applications, that is user-friendly, has an open architecture to facilitate integration with a variety of applications, is customisable to unique projects and is web-based, providing a platform for multicentre studies.
Methods: A web-based database was developed using cutting edge technology (ColdFusion, MySQL and core software design and development techniques). Specifications were based on current and future requirements for storage and data-processing of cross-sectional and longitudinal data. Core questions relating to subject age (neonate/infant/child) and/or disease groups (eg, cystic fibrosis/asthma) formed the basis of the database structure to ensure consistency in data collection between research projects and to facilitate the development of new questionnaires.
Results: Archived demographic and clinical data from 1018 subjects (aged 3 weeks to 11 years) involving 850 variables were successfully transferred from existing databases to the new system, together with >6000 sets of lung function, cardiopulmonary exercise and skin-test data. Cross-sectional and longitudinal data can be extracted using the self-query function. New project questionnaires can be generated using the pool of core questions within the database.
Conclusions and Future Directions: The database represents cutting edge technology, which integrates our unique existing data and provided an invaluable tool to meet future requirements. The infrastructure of this self-managed, web-based database can be adapted for other clinical or research programmes. Additional features, including data management and data audit tools using traceability functions, plus the facility to transfer questionnaire data directly into the database using a “magic pen” (thereby reducing time and the potential for transcription errors) will soon be available.
Funding: Funding was provided by Smiths Medical, Asthma UK, CF Trust and the MRC.
P80 DEVELOPING A CAREGIVER QUALITY OF LIFE SCORE FOR WHEEZY PRESCHOOL CHILDREN
1Ms Olden, 1Dr Seddon, 2Prof Juniper. 1Royal Alexandra Children’s Hospital, Brighton, UK, 2McMaster University, Hamilton, Canada
Assessing asthma control in the preschool age group is problematical. Lung function is difficult to measure and may not be closely related to the quality of life (QOL). Validated QOL tools exist for caregivers of school-age asthmatic children. We aim to develop a QOL tool for wheezy preschool children and their families. As the first stage, we have explored QOL issues as perceived by caregivers and health professionals.
We interviewed 10 individual parents of children aged 1–5 years with recurrent wheezing, ran two parent focus groups involving a further nine parents and interviewed six health professionals. Parents were asked open-ended questions about how wheezing illness affected their child’s QOL and their own QOL. Professionals were asked what aspects of QOL were most likely to be affected by wheezing disease in preschool children and their carers.
Prominent themes that emerged were as follows. Parents on their child’s QOL: Missing fun activities, need to limit exercise, sleep disturbance. Parents on own QOL: Anxiety about child catching respiratory infections, worry about spotting deterioration, missing work/college, concern about not being listened to by professionals. Professionals on child’s QOL: Sleep disturbance, restriction of activity, upset about taking medications. Professionals on caregiver QOL: Stress of remembering to give medication, disturbed sleep, employment prospects.
Although there was considerable overlap, professionals focussed on the problems of medication impinging on QOL, whereas caregivers rarely mentioned this. Compared with items in the Juniper caregiver QOL questionnaire for school-age asthma, issues about acute attacks, as opposed to chronic symptoms, predominated.