Article Text

Statistics from Altmetric.com
INTRODUCTION
All children experience head colds and many consult their doctor because of associated coughing.1 Cough with colds remedies are among the most commonly used medications in children in Western societies, despite evidence suggesting ineffectiveness of medication to treat cough as a symptom. The aetiology of coughing in children will cover a wide spectrum of respiratory disorders, and finding and treating the underlying cause is important.
Community-based surveys show that parental-reported cough as an isolated symptom has a high prevalence.2 3 Reported cough without colds has a prevalence of 28% in boys and 30% in girls.4
The recognised underdiagnosis of asthma led to the importance of cough as a symptom being stressed. However, there is increasing evidence that children are inappropriately treated for asthma based on cough as the sole symptom.5 6
Coughing in children can be distressing and has a major impact on a child’s sleep, school performance and ability to play. It may similarly disturb other family members’ sleep and be disruptive for school teachers. Considerable parental anxiety is generated in families with a child with problem coughing.7 8
The reported severity of a child’s cough may relate to how it affects parents and teachers. Recent evidence has highlighted that parental reporting of the frequency and severity of a child’s cough is unreliable compared with objective measures, and this is especially true for nocturnal cough. Indeed, it has been suggested that cough as reported in surveys and as a clinical trial outcome should either not be used or be interpreted with caution.9–12 This limits the certainty that can be placed on most of the published literature that has not used objective cough measurements.
The need and purpose of BTS recommendations on the management of cough
These guidelines are needed because childhood coughing is a common problem that generates much anxiety, has numerous different causes and is often wrongly diagnosed and inappropriately treated. Differences between childhood and adult cough suggest the need for separate guidelines. The “big three” causes of adult chronic cough (cough variant asthma, postnasal drip and gastro-oesophageal reflux) are not necessarily valid for children.13
The aim is to produce guidelines that are relevant to the clinical management of cough in children up to 12 years of age without known lung disease in primary and secondary care. Both adult and childhood conditions and treatments will need to be considered when dealing with teenagers. No attempt has been made to provide a comprehensive list of all causes of coughing.
These guidelines cover acute, chronic and recurrent coughing. We have used the approach that an attempt should be made to arrive at a specific diagnosis for cause of cough (specific cough). We have covered the commonly encountered situation of a child who does not appear to have a specific pointer to a cause or to have significant underlying serious disease but has problem cough (non-specific isolated cough).
Methodology for generation of the guidelines
There is currently a lack of evidence on which to make evidence-based statements for the diagnosis, investigation and treatments included in this guideline. Most of the features of a cough and investigations have not been formally evaluated for their predictive value in the diagnosis of a specific condition. In the Cochrane Library database, three recent systematic reviews of treatment of prolonged non-specific cough in children (inhaled anticholinergics, theophyllines and cromones) found no eligible randomised controlled trials (RCTs) and, in a further review (treatment of gastro-oesophageal reflux), three paediatric studies were found but none could be included in the meta-analysis.14–17
In order to make opinion and consensus-based statements based on the known literature that would be useful the following methodology was used.
Step 1
MDS performed a database literature search (Medline, Embase, Cochrane Library and Google Scholar) initially using the terms “cough” AND “child”. Exclusions included non-English language papers and papers on pertussis vaccine development. Also excluded were papers on specific diseases including asthma, cystic fibrosis and pneumonia for which management guidelines have already been published. Abstracts of papers were then reviewed and relevant papers obtained. The relevant studies to the UK population were largely performed in Europe, North America, Australia, New Zealand and South Africa.
Specific searches of the databases were subsequently made adding the terms “gastroesophageal reflux”, “cough variant asthma”, “isolated” OR “non-specific cough” AND “randomised controlled trial” OR “placebo”.
Step 2
MDS produced a framework document.
Step 3
The framework document was sent to the other team members (AB, SMcK, ME, RP) who modified the document and added their opinions until consensus was obtained.
Step 4
General practitioners (VMcG, TC and NW [GP trainee]) and paediatricians (NK, DO’D [trainee] and JH [trainee]) provided further comments on improving the usefulness of the guidelines.
Terms used in this guideline
Cough
For the purposes of this document, the following definition is used: “Cough is a forced expulsive manoeuvre, usually against a closed glottis and which is associated with a characteristic sound”.
Acute cough
A recent onset of cough lasting <3 weeks.
Chronic cough
A cough lasting >8 weeks.
The main reason to classify cough on this time basis is that 3–4 weeks allows most simple infective causes of cough to have resolved and identifies those children with chronic cough that might require further investigations.
Prolonged acute cough
Clearly there is a “grey” area between acute and chronic cough, sometimes called “subacute cough”.18 An example of such a situation would be a child with pertussis or postviral cough whose cough may be slowly resolving over a 3–8-week period. If a cough is resolving, an additional period of time may be required to elapse before performing further investigations. Most acute coughs associated with upper respiratory infections should be abating in the second and third week. However, if the cough is not waning by the third week and is becoming more severe in frequency and intensity (“relentlessly progressive”), earlier investigations may be warranted (see table 2).
Recurrent cough
A recurrent cough without a cold is taken as repeated (⩾2/year) cough episodes, apart from those associated with head colds, that each last more than 7–14 days.19 20 If the periods of resolution are short, frequently recurrent cough will be difficult to distinguish from persistent chronic cough.
Postviral cough
Postviral cough is a cough originally starting with an upper respiratory tract infection but lasting >3 weeks.
Specific cough
A specific cough is one in which there is a clearly identifiable cause.
Non-specific isolated cough
The term “non-specific isolated cough” has been used to describe children who typically have a persistent dry cough, no other respiratory symptoms (isolated cough), are otherwise well with no signs of chronic lung disease and have a normal chest radiograph.
Figure 1 illustrates the types of cough intensity over time.21

SUMMARY OF GUIDELINES FOR COUGH IN CHILDREN
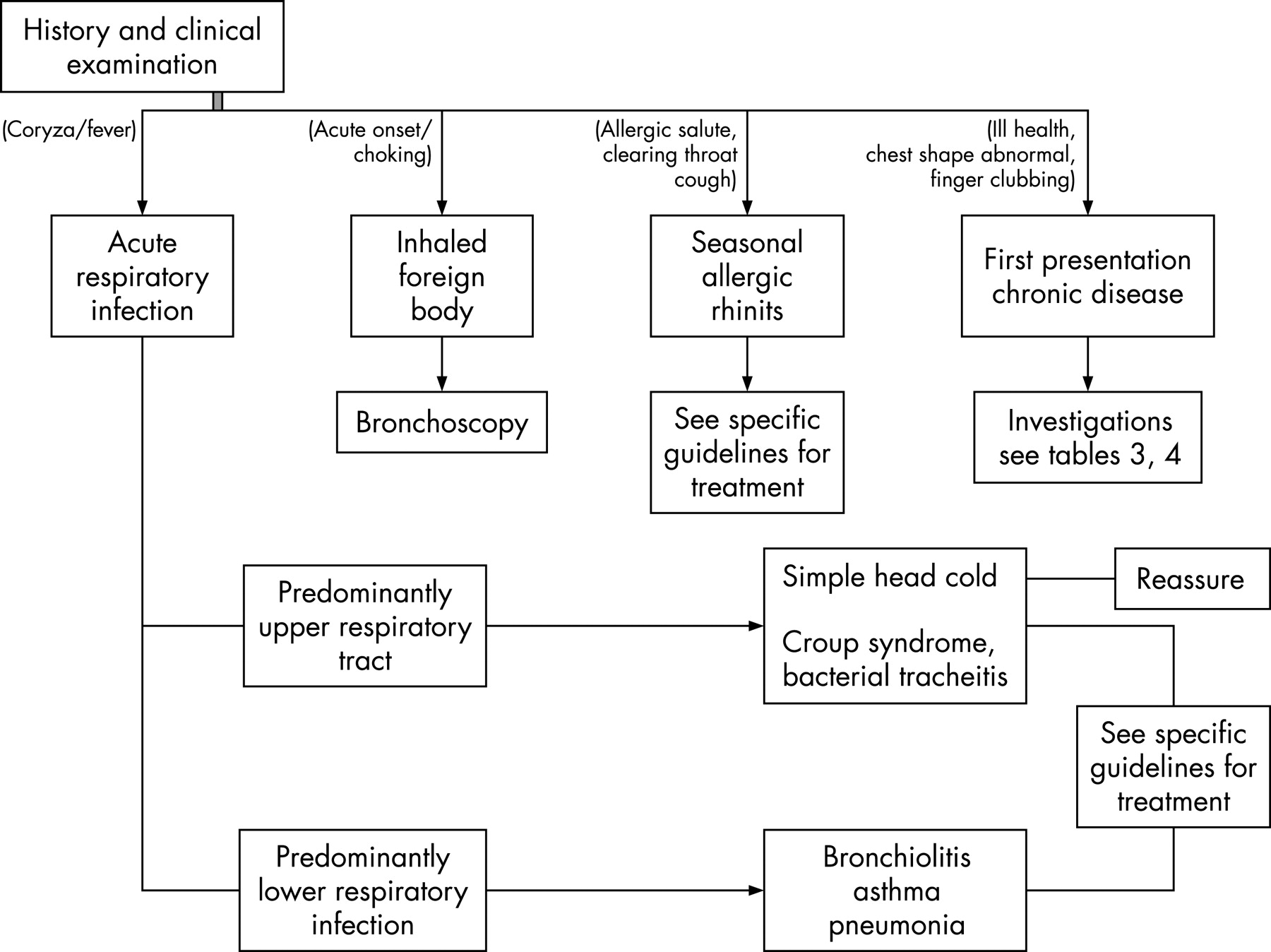
Acute cough (fig 2)

Diagnosis
The majority of children with acute cough have a viral respiratory tract infection.
An attempt should be made to arrive at a specific clinical diagnosis (see table 1).
The absence of fever, tachypnoea and chest signs appear to be most useful for ruling out future complications in children with cough in primary care.
Investigations
Most children with cough due to a simple upper respiratory tract infection will not need any investigations.
Children in whom an inhaled foreign body is a likely cause of cough should undergo urgent bronchoscopy.
A chest radiograph should be considered in the presence of lower respiratory tract signs, relentlessly progressive cough, haemoptysis or features of an undiagnosed chronic respiratory disorder (see table 2).
Treatments
Over-the-counter medications are as effective as placebo for acute cough with head colds in children.
Bronchodilators are not effective for acute cough in non-asthmatic children.
Antibiotics are generally not effective or recommended for treating acute coughs caused by simple “head colds”.
Macrolide antibiotics should be given early (first 1–2 weeks) to children with pertussis.
Antihistamines and intranasal steroids are beneficial for children with an allergic cough in the pollen season.
Education
There may be benefits from educating the community and medical profession about the natural history of cough with head cold. For the majority of children the cough will have resolved by 14 days; however, for an important minority the cough will take 3–4 weeks to resolve. Giving this information to parents may reduce the need for subsequent doctor consultations, providing the cough is subsiding and provided that warnings are given about when to reconsult (eg, ongoing fever, tachypnoea).
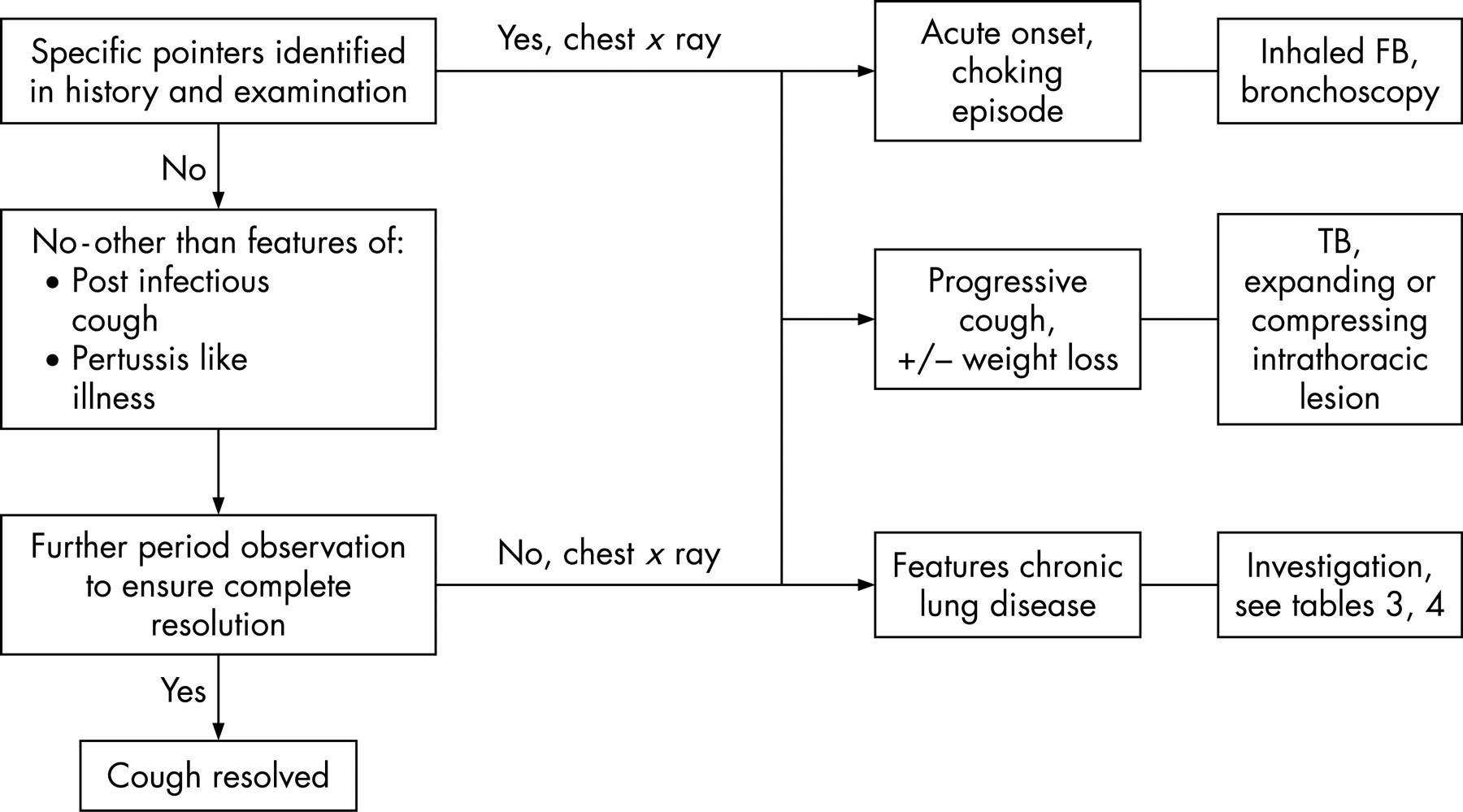
Prolonged acute cough (fig 3)

There is a “grey” area between acute and chronic cough (cough lasting >8 weeks), sometimes called “subacute cough”. Much coughing in children lasting >3 weeks is related to transient viral or pertussis-like infections. A period of observation (3–8 weeks) may therefore be needed to determine if further investigations will be required. If the cough is abating and the child is otherwise well, no further tests may be required; however, it will be important to follow-up the child in 6–8 weeks’ time to ensure that the cough has resolved. If the cough is progressive or if a retained inhaled foreign body is likely, earlier investigations are required. Most acute coughs associated with upper respiratory infections should be abating in the second week, whereas a relentlessly progressive cough becomes increasingly severe (frequency and severity) beyond 2–3 weeks. In this situation, diagnoses that should be considered include pertussis, retained inhaled foreign body, expanding mediastinal neoplasm, lobar collapse secondary to mucus plug and tuberculosis (often with accompanying weight loss). A chest radiograph will usually be needed.
Recurrent cough
A recurrent cough without a cold is taken as repeated (⩾2/year) cough episodes—apart from those associated with head colds—that each last more than 7–14 days. If the periods of resolution are short, frequently recurrent cough will be difficult to distinguish from persistent chronic cough.
Chronic cough (fig 4)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The management of chronic coughing relates to first making an accurate underlying diagnosis and then applying specific treatment for that condition (see tables 4 and 5).
Most chronic coughs in childhood are not due to the same conditions as occur in adults. The use of adult-based cough algorithms is unsuitable for application in children.
The initial assessment should be used to identify pointers suggestive of specific disorders (see tables 3–5).
A detailed history should be taken and all children with cough should have a full clinical examination.
A chest radiograph is indicated for most children.
Spirometry with or without tests of bronchodilator responsiveness (BDR) or bronchial hyperreactivity (BHR) should be attempted in children old enough to perform the manoeuvres.
An attempt should be made to observe the cough and to obtain a sample of sputum.
A “wet” moist productive cough is an alert that there is chronic overproduction of mucus and great care should be taken before such children are labelled as “asthmatic”. Protracted bacterial bronchitis or a more serious condition such as cystic fibrosis should be considered.
Allergy testing (skin prick or RAST specific testing) may be helpful in determining if a child is atopic and, in the correct background, that would make problem coughing more likely to be due to asthma.
In otherwise well children with non-specific isolated dry coughing with no specific disease pointers, empirical trials of anti-asthma, anti-allergic rhinitis or anti-gastro-oesophageal reflux therapy are unlikely to be beneficial and are generally not recommended.
However, as it can be difficult to rule out asthma as a cause of coughing in young children, a trial of anti-asthma therapy (typically inhaled corticosteroids) may be used. In such a trial the treatment should be effectively delivered in adequate doses with clearcut outcomes recorded.
A definite period of time should be set (eg, 8–12 weeks), after which the trial of anti-asthma medication should be stopped. If the child has responded to anti-asthma therapy and the treatment has subsequently been stopped, cough variant asthma is suggested by an early relapse that again responds to treatment. If there is no response, the treatment should be stopped as asthma is unlikely and the cough is unresponsive to asthma medication. This is important so that children with simple recurrent viral bronchitis or postviral cough do not end up on long-term high doses of inhaled corticosteroid.
Psychotherapy regimes may be helpful in treating psychogenic coughing.
An attempt should be made to remove children with chronic cough from exposure to aeroirritants such as environmental tobacco smoke.
Non-specific isolated dry coughing in an otherwise well child should be differentiated from those with more serious conditions. “Red flag” alert symptoms/signs include:
neonatal onset
cough with feeding
sudden onset cough
chronic moist cough with phlegm production
associated night sweats/weight loss
continuous unremitting or worsening cough
signs of chronic lung disease.
ACUTE COUGH IN CHILDREN
1. Introduction
Recommendation 1.1
The majority of children with acute cough have a respiratory tract infection and an attempt should be made to arrive at a specific clinical diagnosis (table 1).22
Acute cough is usually caused by viral upper respiratory tract infection, probably with associated bronchitis in children but may arise from lower respiratory tract infections, hay fever, an inhaled foreign body or be the first presentation of a chronic disorder. Symptomatic upper respiratory tract infection with cough in school children typically occurs 7–10 times per year.23 24
Prospective studies of acute cough in young children in general practice have suggested that about 50% recover by 10 days and 90% by 25 days, so 10% still have problems in the third to fourth weeks. This was supported by a recent systematic review of the natural history of acute cough in which it was estimated that about one-quarter will still be unwell with cough at 2 weeks.25 26
2. Investigations
Recommendation 2.1
Most children with cough due to a simple upper respiratory tract infection will not need any investigations.
The absence of fever, tachypnoea and chest signs appear to be most useful for ruling out future complications in children with cough in primary care.
In a prospective cohort study of 222 children aged 0–4 years in primary care with acute cough, the presence of fever, tachypnoea and chest signs were associated with an increased risk of subsequently developing a complication (any new symptom or sign suggestive of deterioration). Reconsultations occurred in 10% of cases which were mostly due to persisting symptoms; reported serious complications were rare with two hospital admissions for bronchiolitis and one for pneumonia.27 28
Recommendation 2.2
Children in whom an inhaled foreign body is a likely cause of cough should have an urgent rigid bronchoscopy.
Recommendation 2.3
A chest radiograph should be considered in the presence of lower respiratory tract signs, a cough that is relentlessly progressive beyond 2–3 weeks, haemo-ptysis or features of an undiagnosed chronic respiratory disorder (table 2).
While the cough associated with acute head cold may take 2–4 weeks to fully resolve, the cough severity and frequency is usually abating after the second week. Occasionally a child is seen with an acute onset cough which is relentlessly progressing in frequency and severity beyond 2–3 weeks. In this situation, diagnoses that should be considered include retained inhaled foreign body, expanding mediastinal neoplasm, lobar collapse secondary to mucus plug and tuberculosis (often with accompanying weight loss). Table 2 summarises some of the indications for performing a chest radiograph in a child with acute cough.
3. Treatments: cough with simple head colds
While parents report benefit from various over-the-counter preparations for treating children’s cough, there is little evidence of a specific pharmacological effect.
Recommendation 3.1
Over-the-counter medications are as effective as placebo for acute cough with head colds in children.
A systematic review of six RCTs and a further recent RCT found that over-the-counter antitussives, antihistamines and antihistamine-decongestant combinations were as effective as placebo with the potential for causing side effects.29 30
Recommendation 3.2
Bronchodilators are not effective for acute cough in non-asthmatic children.
RCTs of salbutamol versus placebo showed no beneficial effect for acute cough in non-asthmatic children.31 32
Recommendation 3.3
Antibiotics are generally not effective or recommended for treating acute coughs caused by simple “head colds”.
While there is evidence that an early antibiotic prescription for children with coughing with “head colds” increases parental satisfaction, a systematic review of the evidence shows that antibiotics are not beneficial and may be associated with side effects. This included children with acute bronchitis and green-coloured sputum in the absence of signs of possible pneumonia.33–35
Recommendation 3.4
There may be benefits from educating the community and medical profession about the natural history of cough with head cold.
For the majority of children the cough will have resolved by 14 days but, for an important minority, the cough will take 3–4 weeks to resolve. Giving this information to parents may reduce the need for subsequent doctor consultations providing the cough is subsiding27 28 36 and provided that warnings are given about when to reconsult (eg, ongoing fever, tachypnoea).
Recommendation 3.5
Parents should be warned that information obtained from the internet on cough may be unreliable.
According to one study of the 19 website pages identified in the year 2000, 10 contained more incorrect than correct information and only 1 appeared to be mostly correct.37
4. Treatments: cough with specific diagnosis
Recommendation 4.1
Evidence-based guidelines exist for treatment of the following common specific causes of acute cough and should be referred to: community-acquired pneumonia,38–40 croup,41 bronchiolitis,42–44 asthma.45
Recommendation 4.2
Macrolide antibiotics should be given early to children with pertussis.
If pertussis has been diagnosed, macrolide antibiotics—if given very early (in the first 1–2 weeks) in the course of the disease—can slightly alter the clinical course but their main role is to reduce the period of infectivity.46 However, the early stages of pertussis can be difficult to distinguish from a simple head cold, making this recommendation hard to carry out in practice other than in the situation when coughing starts after a known exposure. Azithromycin and clarithromycin are equally effective but have fewer side effects than erythromycin.47–49
Anecdotal evidence suggests that using salbutamol or steroids might reduce severity of the cough spasm in pertussis, but this has not been confirmed in RCTs.50 51 A recent Cochrane review concluded that there was insufficient evidence (poor study quality) to draw conclusions about the efficacy of steroids, salbutamol or antihistamines in the symptomatic relief of coughing in pertussis. There were no statistically significant differences in coughs per 24 h or duration of hospitalisation between these interventions and placebo.52
Recommendation 4.3
Antihistamines and intranasal steroids are beneficial for children with an allergic cough in the pollen season.
An RCT has shown that antihistamines are beneficial for reducing cough frequency and intensity during the pollen season.53 Intranasal steroids may have an efficacy advantage over antihistamines.54
CHRONIC COUGH IN CHILDREN
1. Introduction
Most coughing in children is related to transient infections. A period of observation (3–8 weeks) may therefore be needed to determine if further investigations will be required. Indeed, in one study about 50% of children with apparent persistent nocturnal cough improved in the 2 weeks after presentation, irrespective of how long the cough had been going on before the time of assessment.55 If the cough is abating no further tests may be required, whereas if the cough is progressive or if a retained inhaled foreign body is likely, earlier investigations are required.
A recurrent cough without a cold is taken as repeated (⩾2/year) cough episodes apart from those associated with head colds that each last more than 7–14 days. If the periods of resolution are short, recurrent cough will be difficult to distinguish from persistent chronic cough. In addition, many children with asthma syndromes or more serious underlying illnesses such as cystic fibrosis have recurrent cough with flare-ups during disease exacerbations. Therefore, in these guidelines, children with prolonged acute cough, chronic cough and recurrent cough are not specifically separated. Clinical experience suggests that most children with chronic cough have recurrent viral bronchitis (recurrent cough) or postviral syndromes (subacute cough) and are otherwise healthy. In a 2-year prospective cohort study, rhinovirus (32%), pertussis (17%) and respiratory syncytial virus (11%) were the most frequent respiratory pathogens detected from children with prolonged coughing episodes, but other infections have been associated with prolonged cough including Mycoplasma, Chlamydia and adenovirus.56 57
Classifications
Generally, cough in children can be placed in one of three overlapping categories58 by a good history and thorough physical examination.
These three categories are:
1. Normal child
Recent objective audio recording studies suggest that normal children (currently free from upper respiratory tract infections) have, on average, 11 coughs each day with some experiencing more than 30 episodes per day.59 60 Cough frequency and severity increase during upper respiratory tract infections and some children experience recurrent upper respiratory tract infections (eg, 8–10 episodes, predominantly in the winter) with each new infection being associated with coughing that may last more than 7 days (eg, recurrent viral bronchitis). It is therefore difficult and requires experience to be sure when a child is normal.61 62
2. Specific cough
After a detailed clinical assessment, pointers often suggest a specific diagnosis and requirement from additional investigations (tables 3 and 4).
3. Non-specific isolated cough
Clinical experience and epidemiological studies indicate that a significant number of children are otherwise well with no underlying serious illness and appear to have a “non-specific isolated persistent cough”. This term has been used when an isolated dry cough persists with no other chest signs or symptoms in an otherwise completely well child in whom appropriate investigation has revealed no abnormality.58 63 “Non-specific isolated persistent cough” should not be thought of as a diagnosis in itself, but rather as a label. As these children truly have increased cough frequency and severity,64 there is probably a specific but as yet unidentified cause. Although the precise diagnosis is not available, it is possible that they have mild forms of the specific diagnoses listed in table 3 or very occasionally a more serious underlying condition (table 4).
Recent evidence suggests that only a small proportion of children with non-specific isolated persistent cough have asthma. They have different risk factors from classical asthma and only a small number subsequently develop asthma with wheezing. Bronchial hyperreactivity (BHR) is associated with the symptom of wheeze but not isolated dry or nocturnal cough, and is not predictive of the response to asthma treatment or the subsequent development of asthma.65–68 In addition, studies of airway inflammation that include induced sputum and bronchoalveolar lavage fluid suggest that only a small number of children with unexplained isolated cough have evidence of eosinophilic airways inflammation.69–71 Some of these children have heightened cough receptor sensitivity.72 The role of gastro-oesophageal reflux as a cause of isolated cough in otherwise well children is unclear. Gastro-oesophageal reflux is a frequent finding in infancy, with or without vomiting, and is only sometimes associated with cough symptoms.
2. Evaluation
When evaluating a child with a chronic cough, the key aims are to decide if:
a diagnosis can easily be made clinically or whether it is necessary to perform further investigations to make a diagnosis or rule out certain more serious conditions;
there are any effective treatments available or whether reassurance and support are all that is needed.
Pointers in the history
There is limited published evidence but much experience on which to make statements on how the characteristics of a cough relate to the underlying cause (table 5).
Traditionally, cough is characterised by its time of onset (neonatal, infancy and childhood), nature (dry or productive), its quality (brassy, croupy, honking, paroxysmal or staccato), the timing (persistent, intermittent, nocturnal and on awaking), triggering factors (cold air, exercise, feeding, seasonal, starts with a head cold), alleviating factors (bronchodilators, antibiotics) and presence of associated symptoms (eg, wheezing, shortness of breath).
Recommendation 2.1
A detailed history should be taken and should address the following questions:
How and when did the cough start?
What is the nature and quality of the cough?
Is the cough an isolated symptom?
What triggers the cough?
Is there a family history of respiratory symptoms, disorders and atopy?
What medications is the child on, what treatments has the child had for the cough and what effect have they had on the cough frequency and severity?
Does the cough disappear when asleep (suggests psychogenic or habit cough)?
Does the child smoke cigarettes or exposed to environmental smoke?
Recommendation 2.2
Cough starting in the neonatal period requires further investigation. All neonates and infants with an unexplained persistent cough should be observed feeding by an experienced nurse.
Chronic cough starting in the neonatal period usually indicates significant disease, especially if it starts in the first few days or weeks of life. Possible diagnoses include:
Aspiration: tracheo-oesophageal fistula or laryngeal cleft. A moist cough following feeding, irritability and arching after feeds or choking on feeds require further investigations.
Congenital malformation: compression of airway or tracheobronchomalacia.
Cystic fibrosis.
Primary cilial dyskinesia, especially if there is chronic persistent rhinitis from birth.
Lung infection in utero or in perinatal period (eg, cytomegalovirus, respiratory syncytial virus, Chlamydia).
Recommendation 2.3
Determine if the cough is wet and productive or dry.
It is worth determining if the cough is productive (wet/moist with sputum production versus dry). Reporting of this feature compares well with the amount of phlegm seen at bronchoscopy.73 A cough that sounds wet or productive implies either an increase in airway secretions or abnormalities in its clearance mechanisms. It may be difficult to be sure if a young child has a productive cough as most young children—and especially those <5 years of age—do not expectorate sputum but tend to swallow it. They often vomit and the sputum colour can be seen in the vomitus.
Dry non-productive cough may be suggestive of allergens in an allergic child, viral infections, tuberculosis or inhaled irritants.
Children with isolated dry cough who appear otherwise healthy and have a normal chest radiograph could have one of the conditions listed in table 3. Children with stable asthma cough more frequently than controls and an increase in coughing heralds the onset of an exacerbation in children with asthma whose parents report cough to be a significant feature in their exacerbations.74 Many of the conditions listed in table 4 can be difficult to distinguish from asthma.
Children with persistent productive (moist or wet) cough which may or may not be associated with ill health and recurrent pneumonia or pulmonary infiltrates on the chest radiograph should be investigated to determine if they have bronchiectasis or any of the specific suppurative lung conditions that eventually lead to bronchiectasis (table 4).
Cough productive of casts is unusual and suggests the rare plastic bronchitis.75
Recommendation 2.4
Determine whether the cough occurs in paroxysmal spasms and is associated with an inspiratory “whoop”.
Paroxysmal spasmodic cough with or without an inspiratory “whoop” is the major feature of the pertussis syndromes with Bordetella pertussis being the most likely organism.56 57 76–78 Post-tussive vomiting often occurs.
Pertussis may be underdiagnosed in children and adolescents. In a community-based survey, parents reported cough lasting longer than 2 weeks in the past 12 months in 22% of children aged 5–14 years of age, 18% of whom met the case definition for pertussis.77 In a second study, 37% of school-aged children with cough lasting >2 weeks had serological evidence of recent B pertussis infection. Pertussis should be considered in any child coughing for >2 weeks (especially if associated with whooping or vomiting), even if the child has been previously immunised.78
A staccato-like cough in infancy has been described in Chlamydia infections.79
Recommendation 2.5
Determine if the cough is brassy, croupy or bizarre and honking.
A brassy, barking or croupy cough is suggestive of tracheal or glottic irritation and children appeared distressed with the cough.80–86 A “seal-like” barking or brassy cough which is particularly severe with concomitant viral upper respiratory infection occurs in children with tracheal compressive lesions or in those with tracheomalacia, including the so-called “TOF cough” following repair of a tracheo-oesophageal fistula.
A disruptive bizarre honking cough in a child who exhibits “la belle indifference” suggests a psychogenic cough.87–92 Although the literature generally lumps together the bizarre honking psychogenic cough with habit coughs, clinical experience would suggest that habit coughs occur as a dry non-irritative repetitive coughing, often persisting long after a head cold has already resolved. Psychogenic and habit coughs generally increase when parents or teachers are present. Traditionally, these coughs are described as not being present at night. However, a recent case report using a cough monitor suggests that some do have increased cough at night.90
The condition of “psychogenic cough” is not well defined but the diagnosis implies that there is no underlying organic cause for the coughing. The underlying cause may relate to the secondary gain produced by the coughing (eg, absence from school). There is little information on how accurate clinical characteristics (table 5) are at identifying children with a non-organic cause of coughing.
Suggestive features of non-organic coughing include:
bizarre honking disruptive coughing;
cough that obviously increases with attention and decreases with involvement and concentration in some activity or sleep;
child exhibits “la belle indifference” to the disruptive coughing.
Recommendation 2.6
Children with true haemoptysis require further investigation including a chest radiograph.
It is important to ensure that a child truly has haemoptysis. Apparent haemoptysis may be related to nose bleeds, cheek biting, haematemesis or factitious illness.
Causes of haemoptysis include:
pneumonia/lung abscess
chronic lung disease with bronchiectasis (eg, cystic fibrosis)
retained inhaled foreign body
tuberculosis
pulmonary haemosiderosis
tumour
pulmonary arteriovenous malformation
pulmonary hypertension
Recommendation 2.7
Determine if the cough is an isolated symptom.
Children with coughing associated with wheezing or breathlessness should have the following conditions considered:
asthma
retained inhaled foreign body
recurrent pulmonary aspiration
airways compression or tracheobronchomalacia
bronchiolitis obliterans or interstitial lung disease
neonatal chronic lung disease
cardiac disease with either congestive heart failure or large left-to-right shunts.
Other atopic disorders such as eczema or allergic rhinitis make a diagnosis of asthma more likely.
It is important to remember that parents may report associated shortness of breath with the bout of coughing and that this is different from true breathlessness when a child is not actually coughing.
Recommendation 2.8
Determine what triggers the cough.
Children with asthma may cough with exercise (especially in cold air), excitement and at night. Children with psychogenic cough typically have increased cough when given attention by others and the cough disappears when the child is asleep. Swallowing or postprandial cough suggests the possibility of recurrent pulmonary aspiration.
Recommendation 2.9
Determine if there is a family history of respiratory disorders.
A strong family history of asthma and other atopic disorders puts a child into the background that makes an asthma diagnosis more likely.
A history of tuberculosis or an elderly relative with a cough is important for the diagnosis of tuberculosis.
Recommendation 2.10
Determine what medication the child is on.
Children treated with angiotensin-converting enzyme inhibitors may develop persistent cough.93 94 It is important to record what treatments have been used for the cough and what effect these have had.
3. Pointers in the clinical examination
Recommendation 3.1
All children with cough should have a full clinical systematic examination including an assessment of the child’s general health, height and weight centile, nutritional status and ENT examination.
Digital clubbing will be missed unless specifically sought, and asymmetric auscultatory signs also point to the need for further investigation.
A normal clinical examination does not exclude significant pathology. It is worth asking the child to cough or “huff” as part of the examination as this may help identify children with a loose wet cough.
ENT examination should include the external auditory meatus, looking for wax or a foreign body which may cause chronic cough possibly through stimulation of the auricular branch of the vagal nerve.95
Rarely, mannerisms associated with unusual stereotypic coughs would suggest Tourette’s syndrome.96 However, the diagnosis of Tourette’s syndrome cannot be made on a single tic, including isolated cough.
Cough can be a manifestation of congestive heart failure with pulmonary oedema which will occur most commonly in infancy.
4. Investigations
Recommendation 4.1
A chest radiograph is indicated for most children with chronic cough.
A chest radiograph will give a good overview of the state of the lungs and may give indications for further investigations. A chest radiograph may not be indicated if a mild specific disorder is definitively diagnosed (asthma/allergic rhinitis or if a pertussis-like illness is clearly resolving). However, a normal chest radiograph does not always exclude significant pathology such as bronchiectasis and further imaging may be needed.
Recommendation 4.2
Spirometry with or without tests of bronchodilator responsiveness (BDR) or bronchial hyperreactivity (BHR) should be attempted in children old enough to perform the manoeuvres.
Spirometry also gives a good overview of the state of lung volumes and airways calibre. Unfortunately the presence of BHR in children with isolated cough is not predictive of the response to asthma treatment or the subsequent development of asthma.68 97 98
Recommendation 4.3
An attempt should be made to observe the cough and to obtain a sample of sputum.
This will be difficult in young children and may require help of an experienced physiotherapist. The sample can be sent for microbiological assessment (culture and sensitivity, virology including using PCR) and for differential cytology.
Recommendation 4.4
Allergy testing (skin prick or RAST specific testing) may be helpful in determining if a child is atopic and in the correct background that would make problem coughing more likely to be due to asthma.
The presence or absence of pointers suggesting specific and serious lung disease will determine the requirements for more detailed investigations (tables 3–5).
In an otherwise healthy child with chronic dry or recurrent cough, the investigations may be initially limited to those for conditions in table 3 but careful follow-up is required to ensure no signs of more serious disease develop. A child presenting with chronic productive cough and signs of chronic respiratory disease will require assessment for the conditions listed in table 4.
5. Treatment of chronic cough
Recommendation 5.1
The use of adult-based cough algorithms are unsuit-able for application in children.
Marchant et al99 found that asthma, gastro-oesophageal reflux or upper respiratory disorders were the cause of cough in fewer than 10% of patients at a tertiary referral unit. The “big three” causes of adult chronic cough (cough variant asthma, postnasal drip and gastro-oesophageal reflux) are not necessarily valid for children.13
Recommendation 5.2
An attempt should be made to remove children with chronic cough from exposure to aeroirritants such as environmental tobacco smoke.
Children cough more if they are passive smokers and this is usually secondary to parental smoking. There is considerable evidence that exposure to environmental irritants such as cigarette smoke and home pollutants (such as nitrogen dioxide and PM10 particles) is associated with increased coughing.
Although there is little information to show that removal from these aeroirritants is helpful, it seems sensible to try and remove the child from such exposures.100–103 The adolescent who develops a recurrent or persistent cough should be suspected of cigarette smoking.
6. Treatments: cough with a specific diagnosis
Recommendation 6.1
The management of chronic coughing relates to first making an accurate underlying diagnosis and then applying specific treatment for that condition.
Evidence-based guidelines and review articles exist for treatments of the following specific disorders associated with cough and should be referred to: asthma; cystic fibrosis; immune deficiencies; primary ciliary dyskinesia; tuberculosis.
Recommendation 6.2
Children with protracted bacterial bronchitis should first have other underlying conditions excluded and sputum cultured before this diagnosis is made. A trial treatment of physiotherapy and a prolonged course (eg, 4–6 weeks) of appropriate antibiotics may be tried.
There have been considerable concerns about using the term “chronic bronchitis” in children with worries that asthma and more serious underlying conditions may be missed. Juvenile chronic bronchitis with persistent endobronchial infection (recently labelled persistent bacterial bronchitis) has been described for many decades.104–112 Children have chronic or recurrent cough with sputum production. This term should only be used after underlying causes have been excluded (table 4). Despite these concerns, there appears to be a group of children who have persistent productive cough in whom other underlying diagnoses have been excluded and for whom anti-asthma therapy has failed. For these children, a trial of intensive physiotherapy and a prolonged course of an appropriate antibiotic may be useful. A recent Cochrane review of antibiotics for prolonged moist cough in children found two suitable but not high quality studies that suggest beneficial effects from using antibiotics in this situation, but cautioned that antibiotics also have their own side effects.113–115 In a recent study using an adult-based algorithm approach to the child with chronic cough (majority with wet cough), the most common final diagnosis was “protracted bacterial bronchitis” and this condition may therefore be more common than previously thought.99 Further research is needed to determine how frequent this condition is and whether it is a precursor to bronchiectasis or chronic obstructive pulmonary disease in adulthood.
7. Treatments: non-specific isolated cough in an otherwise well child
The evidence base for treating children with non-specific persistent isolated cough (which includes postviral cough and recurrent viral bronchitis) is sparse and no treatments seem particularly effective. Parental reassurance is required and usually the cough eventually subsides with the passage of time. If the impact of the cough is mild and there are no diagnostic pointers in an otherwise well child, a period of observation with no diagnostic tests or treatments should be considered.
Recommendation 7.1
Whenever specific work-up is not pursued as part of the management plan, this should be time limited (eg, 6–8 weeks) and a comprehensive review performed to ensure that the cough is resolved and no specific pointers have developed.
Recommendation 7.2
In otherwise well children with non-specific isolated coughing with no specific disease pointers, empirical trials of anti-asthma, anti-allergic rhinitis or anti-gastro-oesophageal reflux therapy are unlikely to be beneficial and are generally not recommended.
Asthma therapy
Anti-asthma therapy has not been shown to be effective for children with non-specific persistent isolated cough (either not effective or insufficient evidence).
Two RCTs have compared inhaled corticosteroids (beclomethasone, fluticasone) with placebo for treating children with isolated non-specific cough. A small beneficial effect was observed only for the study using very high dose fluticasone but the author advises caution regarding the potential for side effects.55 98
There is currently insufficient evidence (no RCTs) to support the use of inhaled anticholinergics14 in the treatment of persistent non-specific cough in children.
There is currently insufficient evidence (no RCTs) to support the use of theophyllines in the treatment of persistent non-specific cough in children.15
There is currently insufficient evidence (no RCTs) to support the use of inhaled cromones16 in the treatment of persistent non-specific cough in children.
One RCT was unable to show a therapeutic advantage of ketotifen over placebo for treating infants and young children <3 years with chronic cough (or wheeze).116
There is currently insufficient evidence (no RCTs) to support the use of leucotriene receptor antagonists in the treatment of persistent non-specific cough in children.117
It can be difficult to determine whether a child with non-specific isolated coughing has underlying cough predominant asthma and therefore might respond well to anti-asthma treatment. Many practitioners therefore now recommend a “trial of anti-asthma therapy” for young children with isolated coughing (conditions listed in table 1) as a test for asthma. This practice is less than ideal but results from an imprecise definition of asthma and lack of suitable available tests to confirm a diagnosis of asthma in young children.
Recommendation 7.3
If a trial of anti-asthma therapy is used to diagnose problem coughing as being caused by asthma, the treatment should be effectively delivered in adequate doses and clearcut outcomes recorded.
A definite period of time should be set (eg, 8–12 weeks) after which the trial of anti-asthma medication should be stopped.
Before embarking on a “therapeutic trial” of asthma medication, it is worth first attempting to document bronchial hyperresponsiveness (eg, peak flow variability during a period of home monitoring, forced expiratory volume in 1 s response to acute administration of bronchodilator, or an acute bronchoconstriction to a simple exercise test).
When using a “trial of medication” to make a diagnosis of cough variant asthma, it is important that the treatment is effectively delivered in adequate doses and that clear outcomes are recorded by parents. The response to short-acting bronchodilators should be recorded to determine if they provide short-term relief of coughing. In order to clearly confirm or exclude a diagnosis of asthma, inhaled corticosteroids are likely to be required (eg, beclometasone dipropionate or budesonide 400 μg per day for the defined period of 8–12 weeks). Alternatively, for those with chronic cough (regular daily or nocturnal), a therapeutic trial of oral steroid (eg, prednisolone 1–2 mg/kg for 3–5 days) is an effective tool to resolve symptoms quickly and point to a diagnosis of asthma.118
If a child has frequently recurrent cough lasting more than 2 weeks with “head colds” but completely recovering in between that might be due to asthma, a longer period of treatment (eg, 8–12 weeks) would be required to determine whether the cough frequency and severity of the episodes has been reduced.
If the child has responded to anti-asthma therapy and the treatment has subsequently been stopped, cough variant asthma is suggested by an early relapse that again responds to treatment. If there is no response the treatment should be stopped as asthma is unlikely and the cough is unresponsive to asthma medication. This is important so that children with simple recurrent viral bronchitis or postviral cough do not end up on long-term high doses of inhaled corticosteroid.
Postnasal drip and rhinosinusitis therapy
It has been suggested that allergic rhinitis and sinusitis are associated with cough that results from postnasal drip and irritation of the larynx, although the evidence behind this is lacking.119 120 The typical adult symptoms of sensation of secretions dripping down the posterior pharynx from the back of the nose and frequent “throat clearing” type of cough may be difficult to elucidate from a child. Children with chronic allergic rhinitis may have a transverse nasal crease due to the “allergic salute” from frequent nose rubbing. When a true harsh self-propagating cough is present, it is unlikely that treatment of nasal secretions will be beneficial as it is likely that the same pathological process occurs in both the nose and the laryngotracheobronchial tree. In adults a major diagnostic criterion is response to treatment. Sinusitis has been described in association with allergic rhinitis and asthma in children.121–123
Recommendation 7.4
In children with a throat clearing type of cough and signs of allergic rhinitis, allergen avoidance and a trial of therapy is indicated.
Allergen avoidance, oral antihistamines and intranasal cortico-steroids are the cornerstones of management.124
Recommendation 7.5
Empirical gastro-oesophageal reflux therapy is not indicated for non-specific cough in children.
Although non-controlled studies have found improvement of cough with treatment for gastro-oesophageal reflux, a recent Cochrane review showed that there was a lack of data on which to base recommendations for the empirical treatment of gastro-oesophageal reflux in children with cough.125–127
Recommendation 7.6
In arriving at a diagnosis of psychogenic or habit cough, the physician should first be sure that organic causes are unlikely and that the suggestive features are present.
Suggestive features of non-organic coughing include:
bizarre honking disruptive coughing;
cough that obviously increases with attention and decreases with involvement and concentration in some activity or sleep;
child exhibits “la belle indifference” to the disruptive coughing.
Habit or “tic”-like coughs are generally less disruptive.
Recommendation 7.7
Acknowledgments
The following people read these guidelines during their formation and provided detailed feedback with helpful suggestions for improvements to make these guidelines more generalisable: Dr Vincent McGovern, Children’s Respiratory Clinic, Royal Belfast Hospital for Sick Children, Belfast; Dr Robert Carroll, Grove Medical Practice, Skegoneill Health Centre, Belfast; Dr Naoimh White, Department of General Practice, Dunluce Health Centre, Belfast; Dr Neil Kennedy, Department of Child Health, Queen’s University Belfast; Dr Dara O’Donoghue, Royal Belfast Hospital Sick Children, Belfast; Dr Jenny Hughes, Royal Belfast Hospital Sick Children, Belfast.
REFERENCES
Supplementary materials
These guidelines have been superceded
Please find the up to date BTS Guidelines here:
Guidelines for respiratory management of children with neuromuscular weakness >>
Managing passengers with stable respiratory disease planning air travel: British ThoracicSociety recommendations >>
Guidelines for the management of community acquired pneumonia in children >>
British Thoracic Society guideline for advanced diagnostic and therapeutic flexible bronchoscopy in adults >>
Footnotes
Competing interests: None.