Article Text

Abstract
Background: This study examined the effects of inhaled furosemide on the ventilatory and perceptual response to high-intensity constant-load cycle exercise in chronic obstructive pulmonary disease (COPD).
Methods: In a randomised, double-blind, placebo-controlled, crossover study, 20 patients with COPD (mean (SD) forced expiratory volume in 1 s 45 (15)% predicted) received either nebulised furosemide 40 mg or placebo on two separate days. Thirty minutes after each treatment, patients performed pulmonary function tests and a symptom-limited cycle exercise test at 75% of their maximum incremental work rate. Changes in spirometry, plethysmographic lung volumes, dynamic operating lung volumes, ventilation, breathing pattern, cardiovascular function, dyspnoea intensity and exercise endurance time were compared between treatments.
Results: Compared with placebo, treatment with furosemide resulted in a mean (SD) decrease in dyspnoea intensity at the highest equivalent exercise time (ie, isotime for each patient) of 0.9 (1.0) Borg units (p<0.01) and an increase in exercise endurance time of 1.65 (0.63) min (p<0.05). These improvements were associated with increases in dynamic inspiratory capacity, tidal volume and mean tidal expiratory flow rates at isotime (p<0.01). The eight patients whose exercise endurance time improved by >1 min had greater changes in operating lung volumes (p<0.05), submaximal oxygen pulse (p<0.05) and oxygen uptake (p = 0.05) than those in whom exercise endurance time did not improve.
Conclusion: Alleviation of exertional dyspnoea after single-dose furosemide inhalation in COPD is multifactorial but improvements in dynamic ventilatory mechanics are contributory in some individuals.
Statistics from Altmetric.com
Perceived respiratory difficulty (dyspnoea) and activity limitation are the dominant symptoms of chronic obstructive pulmonary disease (COPD) and contribute importantly to perceived poor health-related quality of life in this population.1 Traditionally, efforts to alleviate dyspnoea have largely focused on improving dynamic ventilatory mechanics, reducing ventilatory demand, or both of these in combination.2–8 However, recent studies have indicated that it may be possible to reduce the perception of exertional dyspnoea and improve exercise tolerance by altering the activity of vagal pulmonary afferents. In this regard, several published studies have found that inhalation of nebulised furosemide, a powerful loop diuretic known to modulate the activity of sensory afferents in the lungs and airways of laboratory animals,9 ,10 alleviates the sensation of dyspnoea provoked by different respiratory stimuli applied experimentally in healthy humans.11–13 Ong et al14 showed that inhaled furosemide reduced dyspnoea intensity at a standardised time during constant work rate cycle exercise but not during incremental exercise in patients with COPD. A more recent study by Laveneziana et al15 also found no effect on respiratory sensation during incremental exercise with simulated expiratory flow limitation in healthy humans. While the study by Ong et al suggested that altered vagal afferent activity in response to topical furosemide directly and independently influenced the intensity and quality of dyspnoea in COPD, these authors did not conclusively rule out the possible simultaneous effects of inhaled furosemide on ventilatory demand and/or dynamic ventilatory mechanics. In particular, it remains unclear whether inhalation of furosemide, by altering vagal pulmonary afferent activity and reducing cholinergic tone of airway smooth muscle, can improve dynamic airway function (ie, reduce dynamic hyperinflation) and in this manner contribute to exertional dyspnoea relief. It is also possible that inhaled furosemide may affect the cardiovascular response to exercise by either reducing dynamic pulmonary hyperinflation or by direct diuretic effects.
The purpose of this study was therefore to determine if the reduction in exertional dyspnoea ratings following inhalation of furosemide was associated with improvements in ventilatory mechanics, ventilatory demand and/or cardiovascular function or was independent of these mechanisms. Our hypothesis was that improvement in exertional dyspnoea and exercise endurance in response to treatment with inhaled furosemide will be associated with a bronchodilator action of this medication. In a randomised, double-blind, placebo-controlled crossover study, we therefore compared the effects of inhaled furosemide and placebo on dyspnoea intensity, airway function, ventilation, breathing pattern, dynamic operating lung volumes, pulmonary gas exchange, cardiovascular function and exercise endurance during high-intensity constant-load exercise in COPD.
METHODS
Subjects
Subjects included clinically stable patients with COPD who were >40 years of age with a cigarette smoking history of ⩾20 pack-years, forced expiratory volume in 1 s (FEV1) ⩽70% predicted, FEV1/forced vital capacity (FVC) <70% and a modified baseline dyspnoea index focal score of ⩽6.16 Patients were excluded if they had significant diseases other than COPD that could contribute to dyspnoea and exercise limitation; a history of asthma, atopy, nasal polyps; exercise-induced arterial blood oxygen desaturation to <80% on room air; or were allergic to sulfa drugs.
Study design
After giving written informed consent, patients completed (1) an initial screening visit to determine eligibility for the study; (2) a second visit designed to familiarise patients with all tests that would be performed during subsequent treatment visits; and (3) two treatment visits randomised to order, conducted 2–10 days apart. Visit 1 included a thorough medical history, clinical assessment, chronic dyspnoea evaluation, complete pulmonary function testing and a symptom-limited incremental cycle exercise test. Visit 2 included pulmonary function tests and a constant-load cycle exercise test. After randomisation of treatments (visits 3 and 4), baseline pulmonary function tests were performed before patients inhaled a 4 ml solution containing either furosemide 40 mg (10 mg/ml) or placebo (0.9% saline), administered by means of a jet nebuliser (Parimaster compressor with Pari LC Jet+ nebuliser; PARI Respiratory Equipment, Richmond, VA, USA) with subjects breathing spontaneously for 15 min using a facemask. Approximately 30 min after inhalation of either furosemide or placebo, subjects performed pulmonary function tests followed by a symptom-limited constant-load cycle exercise test at 75% of their maximal incremental work rate. Before each visit, subjects were asked to withdraw from short-acting β2 agonists (4 h), short-acting anticholinergics (6 h), long-acting β2 agonists (12 h), long-acting anticholinergics (24 h), short-acting theophyllines (24 h) and long-acting theophyllines (48 h). Subjects avoided caffeine and heavy meals for at least 4 h before testing and avoided alcohol and major physical exertion entirely on visit days. All visits were conducted at the same time of day for each subject.
Pulmonary function testing
Pulmonary function tests, including routine spirometry and constant-volume body plethysmography, were conducted in accordance with recommended techniques17 ,18 by use of automated equipment (Vmax 229d with Autobox 6200 DL; SensorMedics, Yorba Linda, CA, USA). Measurements were expressed as percentages of predicted normal values;19–21 predicted normal inspiratory capacity (IC) was calculated as predicted total lung capacity (TLC) minus predicted functional residual capacity (FRC).
Cardiopulmonary exercise testing
Symptom-limited exercise tests were conducted on an electronically braked cycle ergometer (Ergoline 800S; SensorMedics) by use of a cardiopulmonary exercise testing system (Vmax229d; SensorMedics) as previously described.5–7 Incremental exercise testing was performed at visit 1 and consisted of a steady-state resting period of at least 3 min followed by 1 min of unloaded pedalling with subsequent increases in work rate in stepwise increments of 10 W each minute, starting at 10 W. Maximal work rate (Wmax) was defined as the highest work rate that the subject was able to maintain for at least 30 s. Constant-load exercise tests consisted of a steady-state resting period, a 1 min period of unloaded pedalling, then an immediate stepwise increase in work rate to 75% Wmax (rounded up to the nearest 5 W) which was maintained until the point of symptom limitation; endurance time was defined as the duration of loaded pedalling.
Measurements were collected at rest and during exercise while subjects breathed through a mouthpiece and a low resistance flow transducer with nasal passages occluded by a noseclip. Measurements included the following: cardiopulmonary and breathing pattern parameters (minute ventilation (VE), oxygen uptake (V̇o2), carbon dioxide production (V̇co2), end-tidal carbon dioxide partial pressure (Petco2), tidal volume (Vt), breathing frequency (fR), inspiratory (Ti) and expiratory time (Te), inspiratory duty cycle (Ti/Ttot), mean inspiratory (Vt/Ti) and expiratory flow (Vt/Te)) were collected on a breath-by-breath basis and compared with predicted normal values;22 oxygen saturation (Spo2) was measured by pulse oximetry; heart rate was measured by 12-lead ECG; blood pressure was measured by auscultation of the right brachial artery using a sphygmomanometer with an arm cuff; intensity of dyspnoea (breathing discomfort) and leg discomfort was assessed using the 10-point Borg scale23 at rest, during the last 30 s of every 1 min interval during exercise and at end of exercise; operating lung volumes (end inspiratory and end expiratory lung volumes (EILV, EELV)) were derived from IC manoeuvres7 ,24 performed at rest, within the last 30 s period of each 2 min interval during exercise and at end of exercise; and the reason(s) for stopping exercise were recorded.
All breath-by-breath measurements were averaged in 30 s intervals throughout each test stage (ie, rest, exercise and recovery). Cardiorespiratory measurements collected over the first 30 s period of every second minute during exercise were linked with symptom ratings and IC measurements collected in the latter 30 s of the respective minute (to avoid contamination of averaged breath-by-breath data surrounding IC manoeuvres). Three main time points were used for evaluation of exercise parameters: pre-exercise rest, isotime and peak exercise. Pre-exercise rest was defined as the steady state period after at least 3 min of breathing on the mouthpiece while seated at rest before the start of exercise; cardiorespiratory parameters were averaged over the last 30 s of this period and IC measurements for this period were collected during breathing on the same circuit immediately after completion of the quiet breathing period. Isotime was defined as the highest equivalent exercise time achieved during each of the constant-load tests performed by a given subject, rounded down to the nearest whole minute. Peak exercise was defined as the last 30 s of loaded pedalling; cardiorespiratory parameters were averaged over this time period and IC measurements and Borg ratings of dyspnoea and leg discomfort were collected immediately after the end of this period.
Statistical analysis
The sample size of 20 subjects provides the power (80%) to detect a significant difference in dyspnoea intensity measured at a standardised time during exercise based on a relevant difference in Borg dyspnoea ratings of ±1 Borg unit, a standard deviation based on values established in our laboratory for a similar group of 105 patients with COPD,24 α = 0.05 and a two-tailed test of significance. Treatment responses were compared by paired t tests with appropriate Bonferroni adjustments for multiple comparisons. Reasons for stopping exercise were analysed using the Fisher exact test. Pearson correlations were used to establish associations between standardised (isotime) measurements of exertional dyspnoea intensity and relevant independent variables; forward stepwise multiple regression analysis was carried out with significant variables and relevant covariates. A p<0.05 significance level was used for all analyses. Results are reported as mean (SD) unless otherwise specified.
A post hoc subgroup analysis was conducted after examination of the data showed that eight subjects had a clear furosemide-induced improvement in exercise endurance time by >1 min (responders) compared with the remaining subjects who had no improvement in exercise endurance time (non-responders). Within- and between-group comparisons were made using a two-way repeated measures analysis of variance.
RESULTS
Twenty subjects with moderate to severe COPD and significant chronic activity-related dyspnoea completed the study (table 1); an additional subject with severe disease was withdrawn from the study due to worsening of COPD symptoms. CT scans of the chest were available for all subjects allowing examination of the presence of emphysema; 10 subjects had moderate to severe emphysema, 9 of these with an upper lobe predominance; the remaining 10 subjects only had minimal airspace dilatation.
Treatment order was balanced such that nine (45%) were randomised to receive treatment with furosemide first. There were no pre-dose differences in spirometric parameters or plethysmographic lung volumes between placebo and furosemide treatment visits, other than a significantly (p = 0.033) higher peak expiratory flow rate (PEFR) on the furosemide treatment day (table 2). However, this difference in PEFR was maintained after furosemide and resulted in no significant treatment response compared with placebo.
Post-treatment changes in resting pulmonary function are shown in table 2. There were no significant pre- to post-dose differences in response to treatment with placebo. After furosemide, measurements of forced spirometry did not change; TLC did not change; slow vital capacity (SVC) and inspiratory capacity (IC) increased; and FRC and residual volume (RV) decreased. Despite these within-treatment differences, the only significant treatment response after furosemide compared with placebo was in the pre- to post-dose change in SVC (mean difference 0.13 l, 95% confidence interval (CI) 0.05 to 0.21, p = 0.002); the treatment response in RV (mean difference −0.14 l, 95% CI −0.30 to 0.01, p = 0.060) reflected that of SVC since TLC did not change. The increase in SVC (decrease in RV) after furosemide may be explained in part by the prolongation of total expiratory time by an average of 1.7 s (p = 0.08) during the vital capacity manoeuvre (r = 0.52, p = 0.014).
Treatment responses to constant-load cycle exercise
Exercise endurance time increased by a mean (SD) of 1.65 (2.9) min (16 (21)%) after treatment with furosemide compared with placebo (p = 0.017, paired t test; p = 0.004, Wilcoxon signed rank test); endurance time increased by >1 min in eight subjects (mean (SD) increase of 4.4 (2.2) min), changed by less than ±1 min in 11 subjects (mean (SD) change of 0.2 (1.3) min) and decreased by 4 min (13%) in 1 subject who had a very long endurance time of 30 min after placebo. The distribution of reasons for stopping exercise was different after furosemide than after placebo (p = 0.029): fewer subjects stopped primarily because of dyspnoea (25% vs 35%) and more subjects stopped because of leg discomfort (50% vs 40%) or a combination of breathing and leg discomfort (25% vs 10%).
Dyspnoea intensity during exercise is shown in fig 1. After treatment with furosemide compared with placebo, dyspnoea intensity decreased by 0.9 (1.0) Borg units (p = 0.006) at isotime (10.2 (8.7) min) during exercise (table 3); in 15 subjects dyspnoea intensity decreased by at least 1 Borg unit, in four subjects the dyspnoea rating did not change and in 1 subject the dyspnoea intensity increased by 2 Borg units. Borg ratings of perceived breathing and leg discomfort were not significantly different at the end of exercise (table 3).
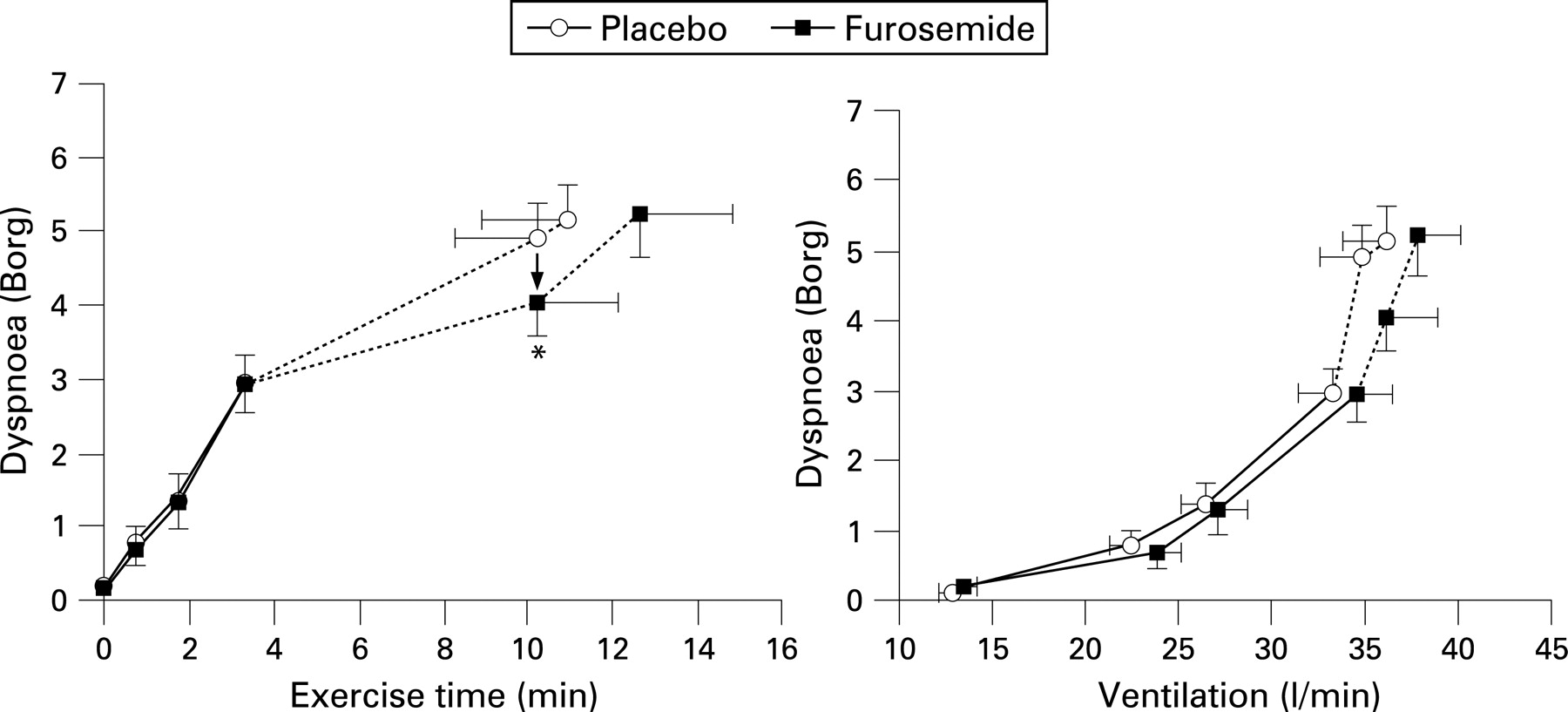
There were no statistically significant treatment differences in pre-exercise resting measurements of breathing pattern, pulmonary gas exchange or cardiovascular function. Measurements at the symptom-limited end point of exercise (peak) are shown in table 3; there were small but significant increases in peak V̇o2 (p = 0.012), V̇co2 (p = 0.013), VE (p = 0.009) and Vt/Te (p = 0.029) after furosemide compared with placebo. Measurements at the highest equivalent isotime during exercise are shown in table 3; there were small increases in Vt (p = 0.038), IC (p = 0.028) and Vt/Te (p = 0.032) after treatment with furosemide compared with placebo.
Mean cardiorespiratory responses to exercise after treatment with furosemide and placebo are shown in an online data supplement. Breathing pattern was relatively deeper and slower with a small but consistent prolongation of Ti and no significant change in Vt/Ti. Dynamic IC increased by approximately 0.12 l at rest and throughout exercise after treatment with furosemide compared with placebo; however, exercise-induced changes in dynamic IC from rest were not significantly different across treatments (table 3). Furosemide had no significant effect on dynamic IRV throughout exercise.
Subgroup analysis
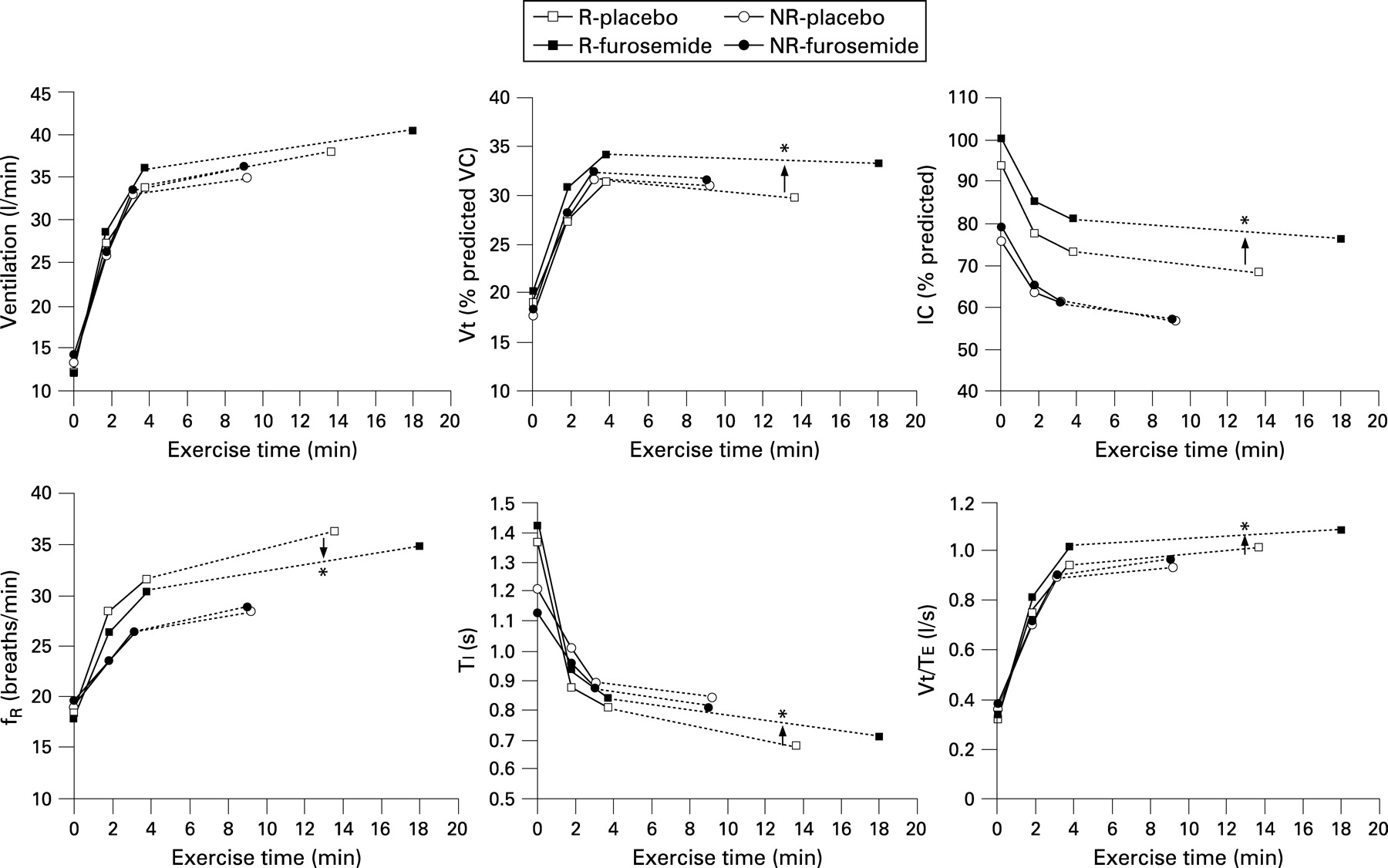
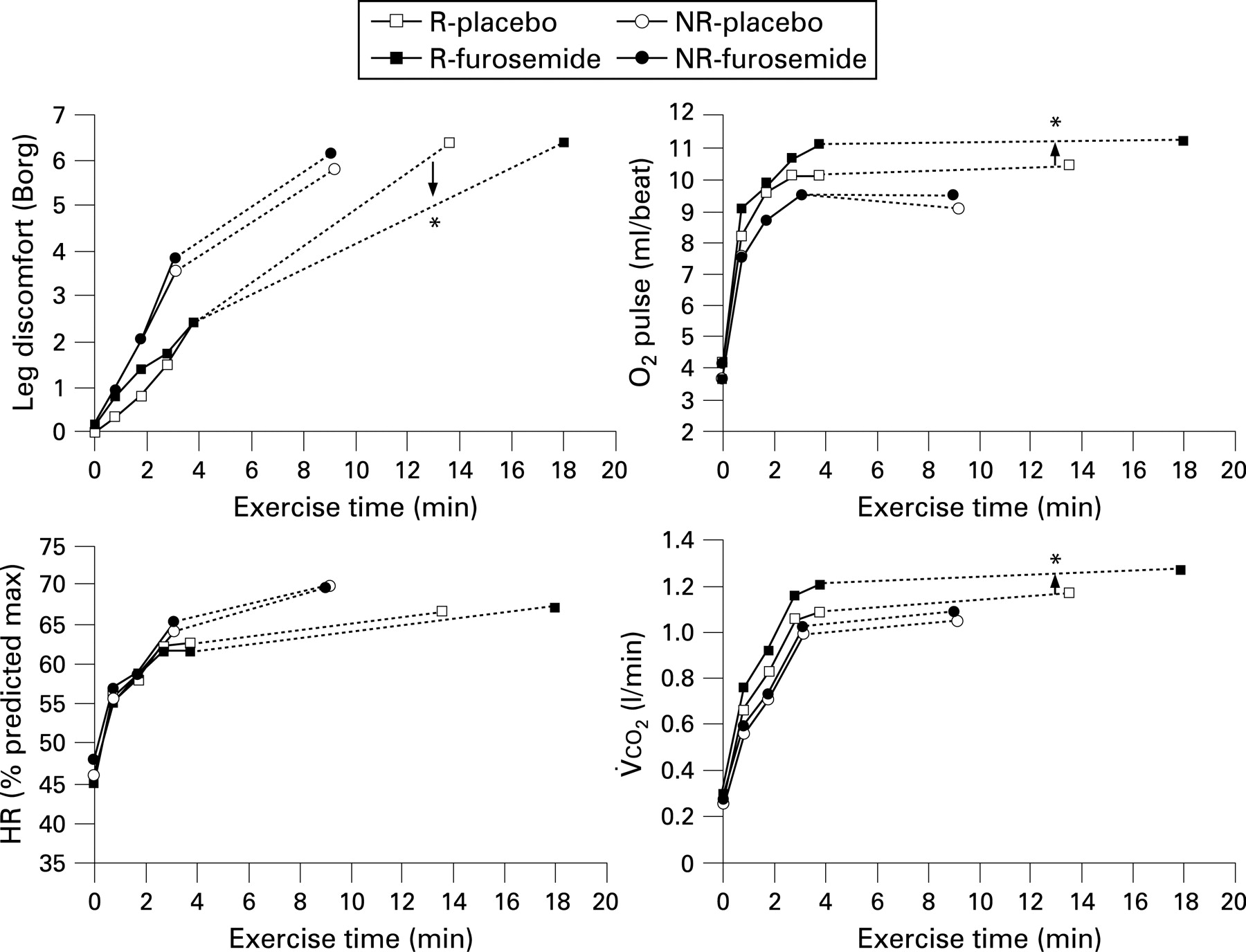
Baseline pulmonary function showed that responders (subjects with a furosemide-induced improvement in exercise endurance time >1 min) had significantly less severe expiratory airflow limitation and hyperinflation than non-responders (subjects who did not improve exercise endurance time). Mean improvements in exercise endurance and dynamic ventilatory mechanics that were seen in the group as a whole were driven by the changes seen in the responder subgroup (fig 2). Additional cardiovascular responses to inhaled furosemide were uncovered by the subgroup analysis; although heart rate and blood pressure responses to exercise did not change, oxygen pulse increased significantly (p<0.05) at isotime during exercise and at peak exercise (fig 3). There were seven patients in the non-responder subgroup in whom exercise endurance did not improve but in whom dyspnoea intensity was reduced at isotime during exercise by 1 Borg unit. In these patients there were no changes in cardiovascular measurements or intensity of leg discomfort, and changes in dynamic respiratory mechanics were intermediate to those of the responders but non-significant (ie, isotime IC increased by a mean of 0.11 l). Additional information on the subgroup analysis is presented in an online data supplement.

{kind=link}
{kind=link}
{kind=link}
Correlates of improvement
Intra-subject reductions in dyspnoea at the highest equivalent isotime correlated with concurrent changes in Ti (r = −0.78, p<0.0005), Vt percentage predicted VC (r = −0.61, p = 0.004) and IC percentage predicted (r = −0.46, p = 0.040). Covariates of this improvement included baseline PEFR (r = −0.66, p = 0.002), sRaw (r = 0.64, p = 0.002), IC (r = −0.49, p = 0.029), FEV1 (r = −0.49, p = 0.030) and FEV1/FVC (r = −0.45, p = 0.049), all expressed as percentage predicted. Using stepwise multiple regression analysis, 80% of the variance in the change in dyspnoea intensity at isotime was explained by the combination of isotime changes in Ti, Vt/Te and Vt (r2 = 0.796). Increased exercise endurance time correlated significantly with the decreased dyspnoea intensity at isotime (r = −0.45, p = 0.047).
DISCUSSION
The main findings of this study are as follows: (1) single-dose inhalation of nebulised furosemide was associated with reductions in the intensity of exertional dyspnoea with attendant improvement in exercise endurance time; (2) inhaled furosemide was associated with minor but consistent changes in slow vital capacity at rest, together with small mean changes in IC and breathing pattern during high-intensity constant-load exercise; (3) improvements in exertional dyspnoea (and exercise endurance) occurred in the absence of significant changes in ventilatory demand and pulmonary gas exchange during exercise and correlated with improved volume and timing components of breathing; and (4) subgroup analysis showed that individuals in whom exercise endurance improved the most after furosemide inhalation had greater improvements in airway and cardiovascular function during exercise.
The patients in this study had moderate to severe COPD with severe ventilatory constraints during exercise and clinically significant chronic activity-related dyspnoea. Consistent with the results of a previous study in COPD by Ong et al,14 we found that single-dose inhalation of nebulised furosemide was associated with a significant decrease in ratings of dyspnoea intensity at a standardised time during exercise by an average of 0.9 Borg units (p<0.01); dyspnoea intensity was reduced by at least 1 Borg unit in 15 of 20 patients at isotime after treatment with inhaled furosemide compared with placebo. This is the first study, however, to demonstrate significant improvement in exercise endurance time (by an average of 1.65 min (16%); p<0.02) after treatment with inhaled furosemide compared with placebo in this population. Improved endurance time correlated with reduced dyspnoea intensity ratings at isotime during exercise. Differences in our results with those of Ong et al probably reflect differences in study protocols. For example, incremental and constant-load cycle exercise tests were conducted on separate days in our study to avoid the potentially confounding effects of peripheral locomotor muscle fatigue on measures of exercise endurance.25 ,26
We considered the following potential mechanisms of dyspnoea relief during exercise after treatment with inhaled furosemide: (1) reduced intrinsic mechanical loading of the inspiratory muscles secondary to improved airway function and reduced dynamic hyperinflation; (2) reduced ventilatory demand; (3) furosemide-induced alterations in vagal pulmonary afferent activity, independent of changes in dynamic ventilatory mechanics and/or cardiovascular function; and (4) any combination of the above.
An earlier study in COPD observed a very small but statistically significant bronchodilator effect after inhalation of furosemide as evidenced by a change of 0.05 l (∼5%) in FEV1.14 This is unlikely to be due to a direct effect of furosemide on airway smooth muscle as it has been shown to have no effect on airway contractility in vitro.27 ,28 However, there is evidence that inhaled furosemide, by increasing slowly adapting receptor (SAR) activity9 and decreasing rapidly adapting receptor (RAR) activity,9 ,10 may cause reflex bronchodilation secondary to reduced parasympathetic outflow and thus cholinergic tone of airway smooth muscle.29–32 We observed no significant change in resting tests of airway function or plethysmographic lung volumes after treatment with inhaled furosemide compared with placebo. This finding is similar to previous studies in healthy subjects12 and in subjects with asthma.33 Interestingly, furosemide inhalation was associated with a significant increase in SVC by an average of 0.13 l. This may be explained, at least in part, by consistent increases in expiratory time during the VC manoeuvre (by an average of 1.7 s). Inspection of maximal flow-volume loops and expiratory volume-time plots before and after treatment showed that these were essentially superimposed for each subject. We postulate that this increased ability to tolerate a more prolonged expiration during spirometry may be associated with altered vagal mechanoreceptor input from the airways, as previously described.9 ,10 ,13 ,29 ,31 ,34 At isotime during exercise, dynamic IC was increased significantly by an average of 0.12 l after furosemide inhalation with no difference in dynamic IRV. Rest-to-peak exercise changes in IC, which reflect the rate of dynamic lung hyperinflation during exercise, were similar across treatments. These small mean changes in exercise IC were approximately 50% of the change previously seen with various inhaled bronchodilators.4 ,5 ,7 Small but significant increases in mean expiratory flow (with an unchanged Te) in the setting of a reduced EELV were measured after furosemide, suggesting some attenuation of expiratory flow limitation as an explanation of the increased IC.
Nishino et al13 previously found that VE was significantly reduced in healthy subjects during mechanical loading of the respiratory system at rest after inhaled furosemide compared with placebo, suggesting that furosemide may reduce central ventilatory drive and that this may explain, at least in part, the observed dyspnoea relief. We could find no evidence of reduced ventilatory demand at rest or during exercise when patients were randomised to treatment with inhaled furosemide. In fact, ventilation tended to increase after furosemide (p = 0.066), mainly due to an increase in Vt, and did so in the absence of a concomitant increase in dyspnoea ratings. Furthermore, there were no differences in the pulmonary gas exchange responses to exercise that would account for the observed dyspnoea relief. The increase in Vt at a standardised time during exercise following inhaled furosemide could be accommodated in these hyperinflated patients as a result of the simultaneous recruitment of IC (without further reducing dynamic IRV). Interestingly, we found that 80% of the variance in post-furosemide improvements in dyspnoea ratings (at isotime) was explained by concomitant increases in Ti, Vt/Te and Vt. We speculate that these changes in the volume and timing components of breathing could represent the effects of inhaled furosemide on dynamic ventilatory mechanics (increased Vt/Te and reduced EELV).
A subanalysis which compared responses in the group of patients in whom exercise endurance was improved while receiving furosemide (n = 8) with those who did not revealed that the former had significantly greater treatment effects on dynamic ventilatory mechanics and on oxygen transport as indicated by consistent improvements in the submaximal oxygen pulse, V̇o2 and V̇co2. Those who showed the largest improvements in exercise endurance and dynamic airway function during exercise had less severe COPD at baseline, but had similar flow and volume responses to furosemide at rest as the non-responders. To the extent that pulmonary vagal reflexes become more attenuated as the severity of COPD progresses, the relatively reduced bronchodilation effect in those with the worst disease may reflect this phenomenon.35 ,36
The improvements in submaximal metabolic parameters and oxygen pulse, together with significantly reduced perceived leg discomfort, point to possible improvements in cardiovascular performance. It is unclear whether this improvement relates to improved cardiopulmonary interactions as a result of mechanical unloading of the ventilatory muscles (as previously described with bronchodilator therapy)37 or to a direct “systemic” effect of furosemide on cardiac function. Moosavi et al12 showed that inhaled furosemide (40 mg) relieved the sensation of experimentally-induced dyspnoea (“air hunger”) for ∼1 h after its administration in healthy subjects at rest; however, clear evidence of a systemic diuretic effect was only apparent >1 h after treatment. Inhaled furosemide, whose salutary effects on exertional dyspnoea were evident within 1 h of dosing, had no demonstrable effect on heart rate or blood pressure responses at rest or during exercise in our study. It therefore seems unlikely that improvement in oxygen pulse (an imprecise surrogate for stroke volume) and V̇o2 at isotime during exercise was the result of a systemic diuretic effect. Nonetheless, this possibility could not be definitively ruled out in this study.
The question arises whether the relief of exertional dyspnoea observed in this study is due to a local effect of inhaled furosemide on vagal sensory afferent discharge independent of reflex anticholinergic bronchodilation, as has previously been postulated in both animal and human studies.9–14 The possibility of such direct vagal sensory influences would be supported by the finding of consistent improvements of dyspnoea at a standardised exercise stimulus with concomitant changes in breathing pattern (ie, Ti prolongation) in the absence of any change in dynamic ventilatory mechanics, metabolic or cardiovascular function.38–40 Such was not the case in the present study. However, our results do indicate that perceptual responses to inhaled furosemide were variable across patients and that those who benefited most were more likely to have the greatest bronchodilator effect during exercise. The seven subjects who experienced exertional dyspnoea relief in the absence of improvement in exercise endurance time tended to have inconsistent smaller improvements in dynamic IC but had no changes in cardiovascular responses or perceived leg discomfort during exercise. The relative importance of direct vagal effects on respiratory sensation (independent of any bronchodilator action) could not therefore be ascertained.
In conclusion, nebulised furosemide was associated with consistent and potentially clinically important improvements in dyspnoea intensity and exercise endurance in patients with advanced COPD. These acute improvements in exertional dyspnoea are multifactorial and could not be explained by alterations in ventilatory demand or pulmonary gas exchange. Improvements in airway function and dynamic ventilatory mechanics occurred in association with dyspnoea relief after inhaled furosemide. This is supported by the strong correlation between a reduction in dyspnoea and changes in the volume and timing components of breathing during exercise. The magnitude of the benefit of inhaled furosemide in this short-term study is similar to that reported following acute administration of a number of established treatments in advanced COPD.2–7 This study therefore supports the rationale for future assessment of inhaled furosemide as a therapeutic intervention for patients with COPD with incapacitating dyspnoea.
REFERENCES
Supplementary materials
web only appendix 63/7/606
Files in this Data Supplement:
Footnotes
Additional data are published online only at http://thorax.bmj.com/content/vol63/issue7
Presented in part at the ALA/ATS International Conference, San Diego, May 2006 (Amjadi K, Harris-McAllister VL, Webb KA, et al. Mechanisms of exertional dyspnea relief following nebulised furosemide in patients with COPD. Proc Am Thorac Soc 2006;3:A225.)
Funding: This study was funded in part by an Ontario Thoracic Society Block Term Grant. KA received a John Alexander Stewart Research Fellowship from the Department of Medicine, Queen’s University. DJ was supported by an Ontario Graduate Scholarship.
Competing interests: None.
Ethics approval: This study was approved by the local university/hospital research ethics committee.