Article Text

Abstract
Introduction: Malignant mesothelioma is a fatal neoplasm, which is rapidly increasing in incidence throughout Western Europe. To date there have been no studies reporting on the natural history and interventional practices on a comprehensive unselected population, as opposed to reports from referral institutions or compensation claimants. We present a population based study capturing data on all patients with mesothelioma presenting within a defined geographical area over a 4 year period in the UK.
Method: Data of all cases occurring in Leeds with a population of 750 000 were collected retrospectively from 2002 to 2003 and prospectively from 2004 to 2005. All patients’ hospital records and the Trust histology database were reviewed, as well as coroner’s reports on all patients with a post mortem diagnosis of mesothelioma.
Results: Over the 4 year study period, there were a total of 146 cases in Leeds; 77% were male. Median age was 74 years (range 36–93). Median survival from diagnosis was 8.9 months. 92% and 8% had histological or cytological confirmation, respectively. 85% had documented evidence of definite or probable exposure to asbestos. 110/146 (75%) had symptomatic pleural effusions at presentation. Twice the number of patients (42 vs 17) were managed with surgical rather than bedside pleurodesis and these had a lower recurrence rate (14% vs 47%; p = 0.02). 122 patients had video assisted thoracoscopic surgery/cutting CT biopsies or chest drains. 73/122 (60%) had prophylactic radiotherapy to these sites. There were seven cases (5%) of tract invasion by tumour and six of these had received prophylactic radiotherapy. Median time to seeding was 174 days. 92/146 (63%) had a performance status of 2 or better at diagnosis but only 54/146 were considered fit for chemotherapy. Of these, 28 (52%) declined chemotherapy; the overall uptake of chemotherapy or entry into a trial was 18%. No patient had radical surgery.
Conclusion: This comprehensive population based audit has shown that the median age at presentation of malignant mesothelioma is increasing and baseline performance status and survival is worse than in selected series. 37% of patients were considered suitable for palliative chemotherapy but less than 20% accepted this offer. Thorascopic pleurodesis appears to be associated with fewer recurrences. The role of prophylactic radiotherapy to chest drain and biopsy sites needs reappraisal.
Statistics from Altmetric.com
Malignant mesothelioma is a fatal neoplasm with very few patients surviving more than 2 years from onset.1 Mortality in the UK is projected to peak at 2450 deaths per year by 2015.2 Previous studies from the UK have reported a median survival of 14 months3 and median age at diagnosis of 64 years.4 There are no data in the literature on the overall natural history and management within a complete and unselected population from a defined geographical area.
Recent studies show that chemotherapy for malignant mesothelioma may be starting to have a clinical impact.5 A phase III study of cisplatin with pemetrexed demonstrated improved survival and response rates compared with those receiving single agent cisplatin alone.6 However, survival benefit was modest, and in their recent systematic review, Ellis et al acknowledged that advantages in survival benefit, improved symptom control and quality of life with chemotherapy over and above active supportive care (active symptom control) have yet to be established.7 MSO1, a British Thoracic Society (BTS)/Medical Research Council (MRC) sponsored trial comparing two chemotherapy regimens with active symptom control, is complete and publication of their results is imminent. Current BTS recommendations state that entry into chemotherapy trials for mesothelioma should be encouraged.8
We present a population based audit capturing very nearly 100% of patients with mesothelioma presenting in a defined geographical area over a 4 year period. The audit recorded: age and performance status at presentation, survival from diagnosis, management of pleural effusion and uptake into chemotherapy trials.
METHODS
The study included all new cases of malignant mesothelioma within the boundaries of the five Leeds primary care trusts between 1 January 2002 and 31 December 2005. This well defined geographical area encompasses the 750 000 population of Leeds, a conurbation in West Yorkshire, UK. All patients included in the audit were seen at the Leeds Teaching Hospitals NHS Trust as part of their diagnostic and/or management process.
We retrospectively analysed all cases from 2002 to 2003, and all cases from 2004 to 2005 were studied prospectively. Cases were identified by diagnosis from the Leeds Cancer Centre database for the retrospective portion of the audit, and from 2004 onwards were identified prospectively at regional multidisciplinary team (MDT) meetings. The audit population was then validated using the Cancer Centre database and MDT records, as well as the Trust histology database and regional coroner’s records. The audit population was also compared with data held by the Northern and Yorkshire Cancer Registry and Information Service (NYCRIS) (table 1).
All patients included in the audit sample were discussed by the Leeds Cancer Centre MDT and were accepted as having a diagnosis of malignant mesothelioma. In nearly all cases the diagnosis of malignant mesothelioma was made following clinical and radiological review with contrast thoracic CT and supported by thoracoscopic appearances together with histological specimens of biopsy material and immunocytochemistry of cytological specimens when present.9–11
Identified patients’ records were reviewed for the audit by physicians from the Department of Respiratory Medicine, Leeds Teaching Hospitals NHS Trust. The following data were recorded from the case notes.
World Health Organisation/Eastern Cooperative Oncology Group (WHO/ECOG) performance status at presentation. Where not formally documented, the performance status was ascertained from the other clinical details recorded.
History of asbestos exposure, classified as definite, probable or uncertain. Probable exposure was used to describe patients in high risk occupations who did not report definite exposure.
Incidence of symptomatic pleural effusions at presentation, and any complications of management.
Prophylactic radiotherapy and incidence of tract invasion by tumour.
Recruitment into chemotherapy trials.
Survival from date of diagnosis, for this audit defined as the date of the histological/cytological sample. Patients diagnosed after death were excluded from the survival analysis.
Statistical analysis
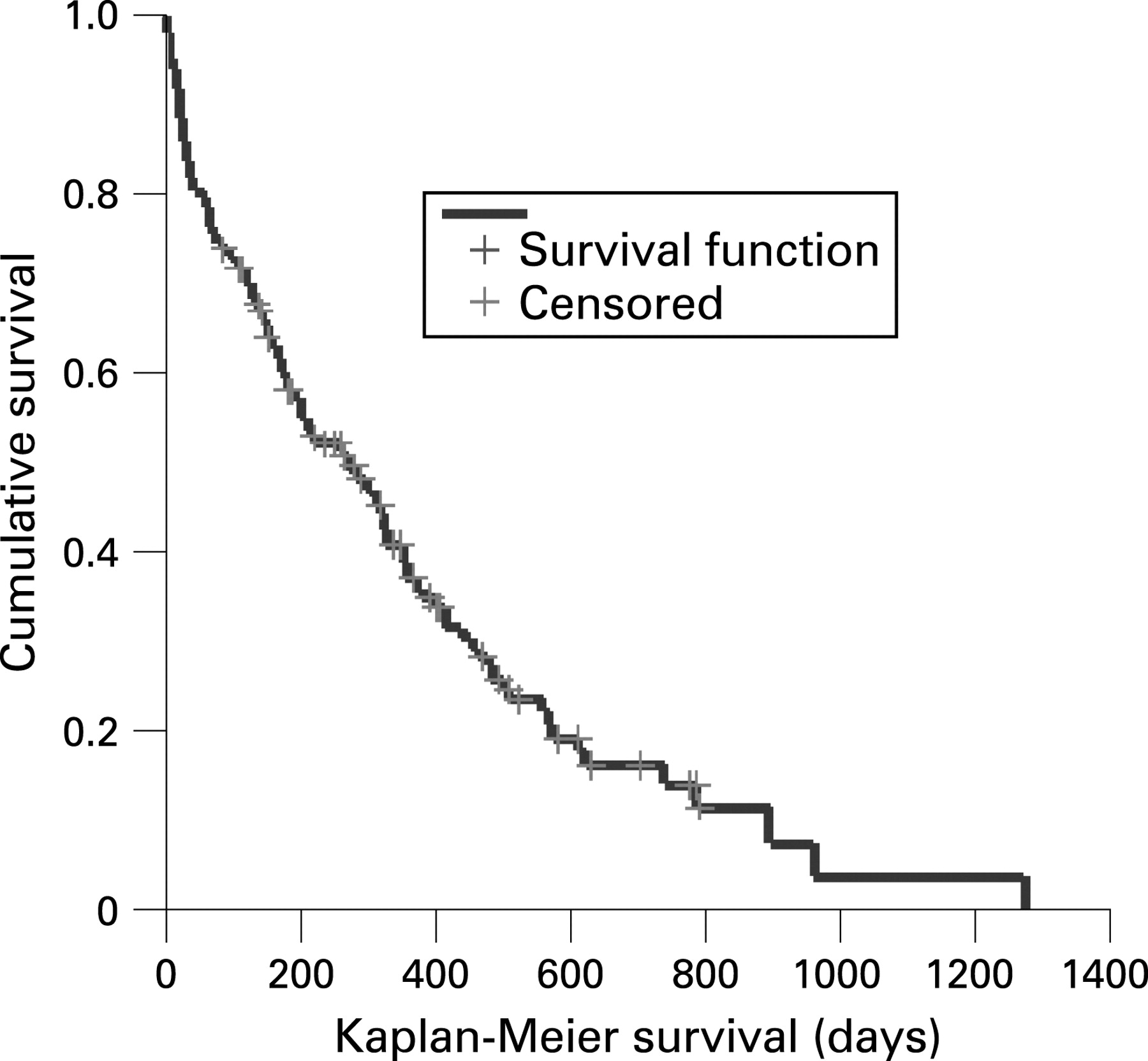
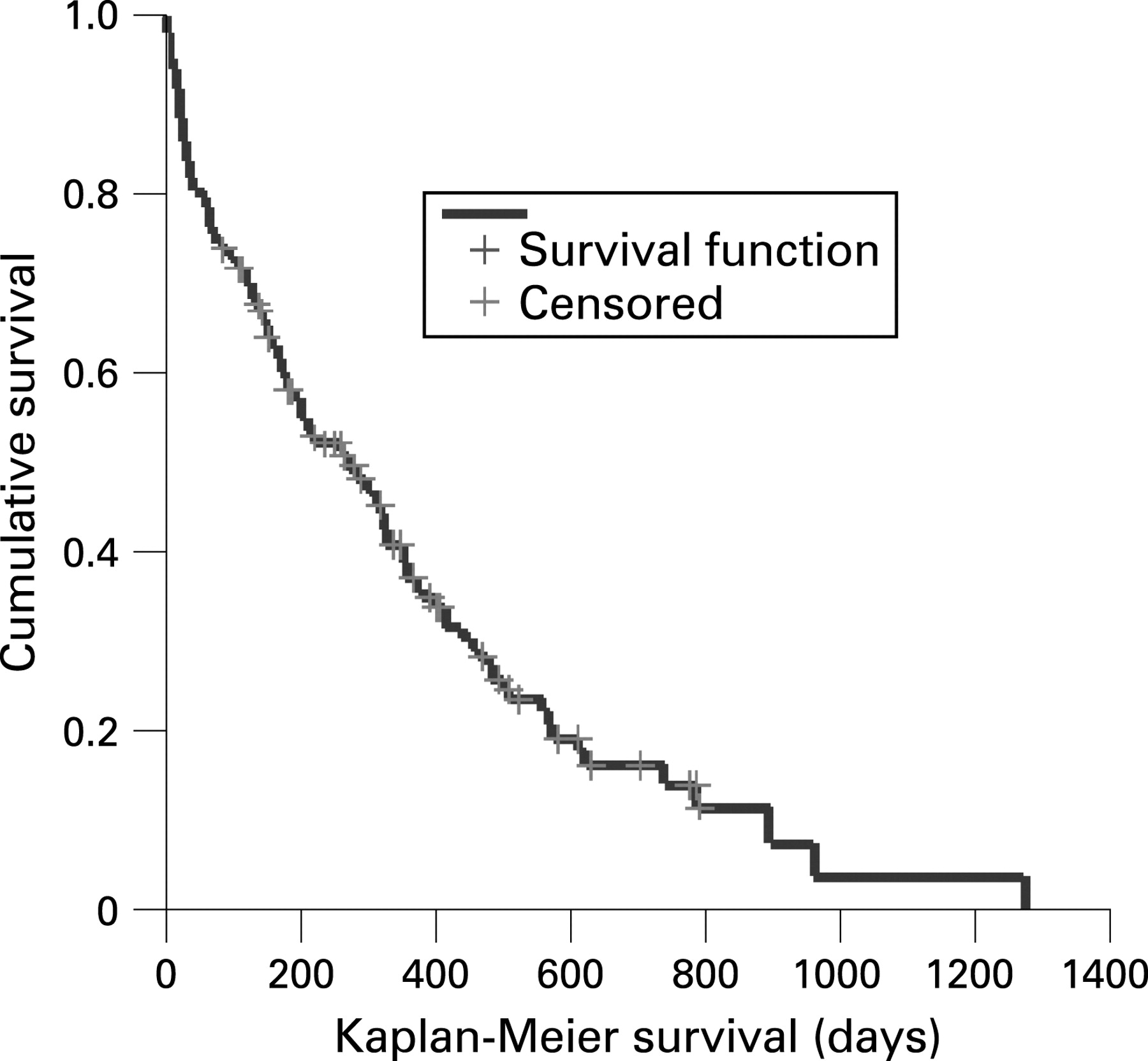
All tests were performed using SPSS V.11.0 (SPSS Inc, Chicago, Illinois, USA). Results are presented as absolute frequencies. Survival curves were calculated using the Kaplan–Meier method and compared using the log rank test. Using this method, patients who are alive at the time of analysis are censored, meaning their survival to the date of analysis is represented in the survival curve, but their presence does not affect the cumulative survival ratio. The χ2 and Fisher’s exact tests were used to compare categorical data. Significance was assumed at the standard 5% level.
RESULTS
Population demographics
The total number of confirmed cases in this series over a 4 year study period was 146 for a population of 750 000. The calculated incidence was 4.9 per 100 000 population per year. A further four cases had a diagnosis based on clinical evidence and CT appearances; two are still alive and two have died. These patients were excluded from our population as they had no histological/cytological confirmation of mesothelioma and the diagnosis was therefore uncertain. There was no obvious increase or decrease in incidence over the study period (table 1). Median age at the time of diagnosis was 74 years (range 36–93).
Diagnosis
The diagnosis of malignant pleural mesothelioma was confirmed with a histological specimen in 91.8% (134/146) of the sample before or after death. Cytological evidence supported the clinical diagnosis in 8.2%.
In our series, subtypes of mesothelioma were recorded in 36% of the sample. There were 34 epithelioid, 10 sarcomatoid (of which five were desmoplastic) and nine biphasic cases identified.
WHO/ECOG performance status at diagnosis
Performance status at diagnosis was as follows: 0 (11%), 1 (32.9%), 2 (19.1%), 3 (25.3%) and 4 (7.6%). Performance status was not recorded in six (4.1%) patients. Mean performance status at presentation was 1.8. Patients with a performance status worse than 2 were not eligible to receive chemotherapy.
Asbestos exposure
Asbestos histories were recorded in 86% (126/146) of cases overall. Definite asbestos exposure was reported in 57% (72/126), 28% (35/126) reported probable exposure and 15% (19/126) could not recall any previous exposure.
Survival
Survival was measured from the date of diagnosis, which for this audit was defined as the date of the histological/cytological sample. Three of 146 patients were diagnosed after death and were excluded from the survival analysis. Median survival from the time of the clinical diagnosis was 267 days (95% confidence interval (CI) 178 to 356), or approximately 8.9 months (fig 1). Median survival for the histological subtypes were 325 days (95% CI 240 to 410, n = 34) for epithelioid, 175 days (95% CI 0 to 445, n = 10) for sarcomatoid and 161 days (95% CI 93 to 229, n = 9) for biphasic. Median survival for the remaining 97 cases without an identified histological subtype was 211 days (95% CI 119 to 302).
{kind=link}
Management of pleural effusion
In our series, 110/146 (75%) patients had symptomatic pleural effusion at presentation. This is similar to the 78% of patients with pleural effusions identified at presentation by Clayson in the north of England in her recent community based study.12 Ninety-nine of 110 (90%) of those patients with a symptomatic pleural effusion received active treatment: 42% (42/99) received surgical pleurodesis; 17% (17/99) pleurodesis via a chest drain at the bedside with talc slurry (9/17), bleomycin (6/17) or tetracycline (2/17) as the pleurodesing agent; 26% (26/99) had a drain only; 13% had long term indwelling catheters.13 Not all patients received drainage or pleurodesis. Cited reasons included problems with blocked and dislodged drains, patient refusal or futility in a dying patient. Ten per cent (11/110) of those with symptomatic pleural effusion received no intervention or simple aspiration only.
Of the 99 patients who received active management of their pleural fluid, the total recurrence rate (as defined by an increase in breathlessness with radiological evidence of fluid re-accumulation) was 23%. Patients with a surgical rather than bedside pleurodesis had a lower recurrence rate (14% vs 47%; p = 0.02, Fisher’s exact test). Recurrence after bedside pleurodesis was 8/17 (47%) and after chest drain only 9/26 (35%), and this was not statistically significant.
Prophylactic radiotherapy to prevent tract invasion with tumour
A total of 122 patients had video assisted thoracoscopic surgery (VATS), cutting CT biopsy or chest drain. Overall, 60% (73/122) of these patients had prophylactic radiotherapy to their intervention sites. Patients referred for prophylactic radiotherapy received three separate daily fractions of 7 Gy. There were seven cases (5%) overall of tract invasion by tumour and 6/7 of these cases had received prophylactic radiotherapy, three of those within 6 weeks of the procedure. The median waiting time from intervention to radiotherapy was 52 days. Thus in the patients who received no radiotherapy, the incidence of metastasis was 2% (1/49) compared with 8% (6/73) in those who had (p = 0.243, Fisher’s exact test). The median time from intervention to appearance of a metastasis at the tract site was 174 days (range 76–360).
Chemotherapy
The majority of patients who received chemotherapy were entered into the MSO1, the BTS/MRC randomised control trial comparing mitomycin, vinblastine and cisplatin together or vinorelbine alone with active symptom control (ASC) (n = 13, three of these randomised to ASC). Earlier during the study period, seven patients were recruited into a commercially sponsored study comparing pemetrexed vs pemetrexed/cisplatin vs pemetrexed/carboplatin.
Ninety-two of 146 (63%) patients had a performance status at presentation of 2 or better thereby not precluding them from chemotherapy trials on this basis. However, 22/92 (24%) had such severe comorbidity that it was decided by their oncologist that they were unfit for chemotherapy. A further 16/92 (17%) were unable to consent or died. Thus only 54/146, or 37% of the total, were suitable for and were offered chemotherapy. Of these, 28/54 (52%) declined this option and eventually only 26/146 (18% of the total) were randomised into chemotherapy trials. In patients who were fit enough and received chemotherapy, median survival was 479 days (95% CI 421 to 537 days).
DISCUSSION
The data in this study we believe capture all cases of mesothelioma occurring in a defined geographical area for the 4 year period. All cases included in the audit were confirmed to be malignant mesothelioma on histological or cytological grounds before or after death. There is the possibility however that a few patients with a Leeds post code may have been referred to a hospital outside of Leeds. We know, however, from lung cancer studies in this area that the proportion of patients with a Leeds address referred to other hospitals outside of Leeds is less than 1%. The value for mesothelioma is therefore likely to be similar. Although registry data from NYCRIS for 2005 are not yet available, mesothelioma registrations for 2002–2004 are similar to patient numbers captured in our audit population (see table 1).
In this study, recording of asbestos exposure history in the clinical record reached 86% overall. Documentation of definite or probable asbestos exposure was 87 (85%) of 126 patients where asbestos histories were obtained and recorded. Howel et al, studying patients with malignant mesothelioma in West Yorkshire, obtained histories of likely or possible exposure in 95% of their sample from case notes or interviews with relatives of the deceased patient.14 15 It is likely therefore that the initial recording of an asbestos exposure history in medical notes may often be inaccurate. It is common, for example, for patients not to recollect exposure at the time of original consultation but at a later date.
At presentation, performance status was 1.8, median survival from the time of diagnosis 267 days (8.9 months) and median age at presentation 74 years. This compares unfavourably with the 272 case series by Yates et al in the south east of England where median survival from symptom onset was 14 months and a mean age at death of 65 years.3 In this earlier series, the authors thought they had captured almost all deaths from mesothelioma cases in the south east occurring in 1987 since this was the last year before the abolition of industrial death benefit and that in practice most cases were referred to the coroner irrespective of occupational history. This claim, however, is unsubstantiated. Age and performance status at presentation were significant poor prognostic indicators in scoring systems from the European Organisation for Research and Treatment of Cancer (EORTC).16 and the Cancer and Leukaemia Group B (CALGB) studies.17 These were validated in a 142 patient series by Edwards et al from the UK.4 Mean age at the time of diagnosis in the latter series was 64 years but selection bias may have occurred by including potentially younger patients referred through a tertiary cardiothoracic unit for radical surgical intervention. Entry into the 337 patient CALGB chemotherapy based series required a performance status of 0–1 and the worst survival (mean 1.4 months) occurred for patients with a performance status of 1/2 and white blood cell count ⩾15.6/μl. Based on these previous studies, our patients are disadvantaged by the fact they are a decade older and with worse performance status. We believe the poorer prognosis of this series is the result of capturing all patients in a defined geographical area. In addition, our data are consistent with the expectation that the mean age at presentation of mesothelioma is increasing because of a cohort effect of widespread asbestos exposure of men born between 1945 and 1950.18 Median survival for epitheliod, sarcomatoid or biphasic histological types was 325, 175 and 161 days, respectively. As in other series, sarcomatoid histology conferred a worse prognosis.4
The presence of pleural effusions associated with malignant pleural mesothelioma is common and problematic. It is commonly associated with chest pain,19 significantly worsens symptoms of breathlessness, reducing performance status and often requires inpatient hospital treatment, thus reducing quality of life further. The management of pleural effusion is not without risk. Complications can occur, such as tumour invasion of the tract,20 21 pneumothorax or introduction of infection into the chest cavity or a severe systemic inflammatory response to the pleurodesing agent.22 There is often the possibility that drainage of fluid will be ineffective because of lung encasement by the tumour, or that the effusion will quickly re-accumulate because of ineffective pleurodesis by surgical or medical means. The majority of patients received either a medical or surgical pleurodesis following drainage of a symptomatic effusion. In our population, more than twice as many were referred for a video assisted thorascopic pleurodesis. These patients had partial pleurectomies or talc poudrage.
Survival between the bedside and surgical pleurodesis groups was not significantly different but there were more recurrences in the talc slurry group. This may be because of rejection by the surgeons of those who on CT appearance were likely to have a trapped lung and those who were unfit. It is interesting that in the remainder of the patients following this selection a bedside pleurodesis conferred no statistical benefit than a chest drain only. A recent randomised trial of 501 patients showed no overall significant difference in 30 day outcomes between talc poudrage and talc slurry; however, subgroup analysis showed that patients with lung primaries had higher success rates through surgical pleurodesis.23 Further randomised trials are needed.
Patients are usually offered prophylactic radiotherapy locally to the chest wall following any interventional procedure to prevent the risk of seeding along the tract,7 the risk of such events being clinically important is unknown. The recommendation for treatment is largely based on a study by Boutin et al who, in a randomised controlled trial, compared 20 patients who received 21 Gy in three fractions within 10–15 days of their procedure with 20 controls. There were none versus eight metastases in the treatment versus control group, respectively. It was concluded that the incidence fell from 40% to zero as a result of treatment.24
Our experience of metastasis occurring along tracts has been different. Sixty per cent of our patients received prophylactic radiotherapy following VATS, cutting needle CT biopsies or chest drains. This rate, although poor, is above the combined rate from a series of patients collected from Northern England of 40% between 1998 and 2001.12 The absolute risk of a symptomatic recurrence in an unselected population is not known. In the 49 untreated patients, we had only one case of metastasis in the relevant area on the chest wall. The remaining six cases occurred in patients who had received prophylactic radiotherapy. Median time from procedure to treatment in these patients was 53 days. Only one of the six occurrences in the treated group received their radiotherapy within the 4 week maximum recommended by the BTS8; 50% (3/6) of those with chest wall metastasis received radiotherapy within 6 weeks of their procedure. While delay to treatment may be a reason for the ineffectiveness of prophylactic radiotherapy, it should be noted that there was only one occurrence in the untreated group. Recent support for the argument that radiotherapy is ineffectual at preventing tract invasion with tumour is given by the most recent randomised control trial by O’Rourke and colleagues.25
Complete data on the reasons for delays to prophylactic radiotherapy were not available; the most frequent examples from the available data include: delays to oncology referral, pressure on the radiotherapy service, morbidity surrounding the episode of intervention precluding rapid treatment and patients being unable to attend initial appointments. The median time to tract invasion was 174 days. Thirty-eight per cent (56/146) of our cohort had died at this point and this short survival time may explain in part why our incidence of tract invasion by tumour was low at 5%. In eight other series, the mean was 19% with extremes of 2% and 51%.20 24 26–32 We believe that the timing and benefit of prophylactic radiotherapy needs reappraisal.
Most trials of chemotherapy in mesothelioma stipulate a WHO/ECOG performance status of at least 2 or better. A significant proportion of patients with a performance status of 0–1 did not receive chemotherapy, and only two patients with a performance status of 2 were enrolled in clinical trials. This decision was made either at an MDT, which always included one of three oncologists with a declared interest in thoracic oncology, or following consultation with one of the oncologists after an MDT referral. Comorbidity was the main reason for patients being ineligible for chemotherapy. Of the patients who were offered chemotherapy (54/146, 37%), less than half accepted so only 26 of the original 146 (18%) in this cohort actually had it. Many patients were unwilling to undergo treatment side effects with uncertain benefit, especially perhaps because at the time of diagnosis they were asymptomatic. The results of the MSO1 trial may provide evidence to help patients make the decision as to whether or not they wish to receive chemotherapy or palliative care.
In summary, this population based audit has shown that the median age of diffuse pleural malignant mesothelioma at presentation is, as expected, increasing, median survival is not improving (and may be worsening) and a large proportion of patients have a poor performance status and comorbidities at presentation precluding palliative chemotherapy. In our series, surgical thorascopic pleurodesis appeared to be associated with fewer recurrences of effusions than those who received a bedside pleurodesis but this may reflect the patient selection. Further randomised control trials are needed. Finally, the timing and role of prophylactic chest wall radiotherapy to biopsy sites needs reappraisal.
REFERENCES
Footnotes
Competing interests: None.
Linked Articles
- Airwaves