Article Text

Statistics from Altmetric.com
A 6 month old infant presented with a history of cough and noisy breathing since 5 weeks of age. He had been evaluated many times in a local emergency department for episodes of cough, wheeze and retractions. His parents reported that his symptoms seemed to be worse when he was supine and did not respond well to steroids or bronchodilators. He had been feeding and growing normally.
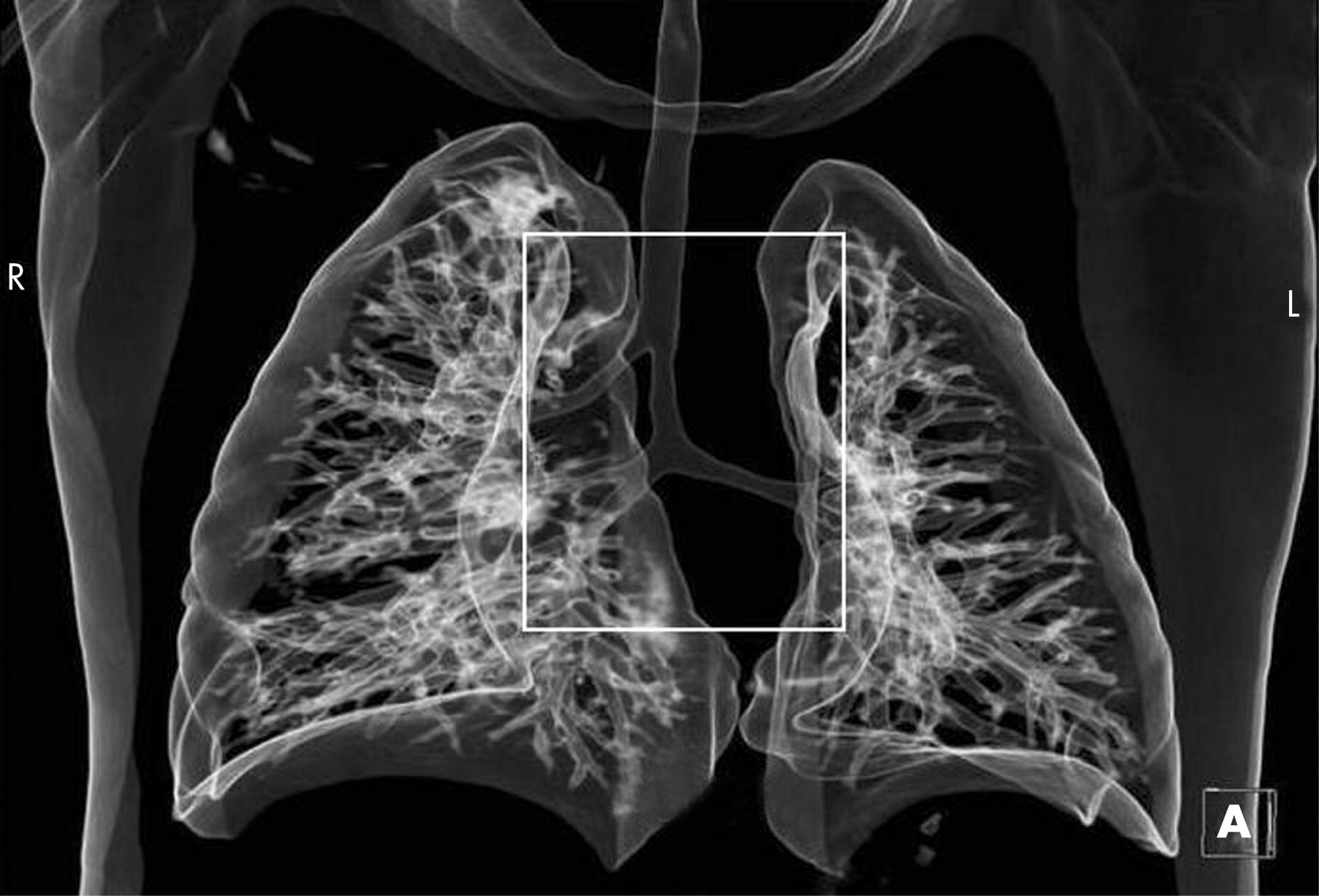
On examination he was slightly tachypnoeic with mild subcostal retractions and coarse upper airway sounds. He was admitted for observation and underwent CT scanning of the chest and neck with intravenous contrast followed by three-dimensional reconstruction and virtual bronchoscopy. This revealed a right sided tracheal bronchus arising 1.2 cm above the carina, comparable in size to the right mainstem bronchus (figs 1 and 2).


{kind=link}
{kind=link}
Scanning was performed on a 64-slice multidetector CT scanner (Siemens Sensation 64) using low dose paediatric protocols for minimum patient dose. Specific scan parameters included CARE Dose software (Siemens) with kV 120 and mAs 60. Slice thickness was 0.75 mm from 0.6 mm detectors and scan reconstruction was at 0.5 mm intervals. The effective radiation dose to a patient of this size can be as high as 4.6 mSv using these parameters. The risks and costs of such a study must be weighed against those of bronchoscopy under sedation, the usual means of making the diagnosis.
An incidence of up to 2% has been reported for tracheal bronchus.1 The term “pig bronchus” or “bronchus suis” is used when the entire right upper lobe bronchus stems from the trachea. Congenital tracheobronchial abnormalities may be asymptomatic and discovered as incidental findings or may present with stridor, recurrent pneumonia or atelectasis.2 Expectant management is preferred and surgical resection is typically reserved for patients with severe or persistent symptoms.
The patient was discharged from hospital with medical treatment for gastro-oesophageal reflux. His symptoms resolved over the course of 2 months.
Learning points
The differential diagnosis for noisy breathing in infants should include congenital tracheobronchial anomalies, especially when symptoms fail to respond to conventional treatment.
The ability to diagnose and characterise these abnormalities non-invasively has been enhanced by use of multidetector CT scanning and 3D airway reconstructions.
Observation of such patients with mild symptoms is an appropriate management option as their symptoms will often improve or resolve with time.
Acknowledgments
The authors thank Dr Mahadevappa Mahesh for his assistance with radiation dose calculation.
Footnotes
Competing interests: None.