Article Text

Statistics from Altmetric.com
TB epidemiology
THE OUTCOME OF A COHORT OF TUBERCULIN POSITIVE, PREDOMINANTLY SOUTH ASIAN, NEW ENTRANTS AGED 16–34 TO THE UK: BLACKBURN 1989–2001
I. W. Choudry1, L. P. Ormerod2,3. 1Central Lancs PCT; 2Royal Blackburn Hospital; 3University of Central Lancs, UK
Background: The incidence of TB in new entrants aged 16–34 with positive tuberculin tests but normal chest x ray/examination after initial entry is uncertain and has been estimated for the NICE economic appraisal of new entrant screening.
Methods: New entrants aged 16–34 years predominantly from South Asia with tuberculin tests inappropriately positive for BCG history from 1989–2001 were studied and matched to the local notification database to July 2006.
Results: 479 entrants with normal chest x rays were identified. Median age was 24.0 years, 19% had prior BCG. The observation time was 4668.5 years. 49 developed clinical TB up to July 2006. The median detection of TB was 47 months, 75% by 79 months and none after 156 months. The incidence density of cases was 1050/100 000 person years (95% CI 756 to 1344), an annual risk of 1.05% (10.5% at 10 years; 15.8% at 15 years). 5% of individuals mainly students had moved out of the area. Of the remainder 29% were definitely shown still to be locally GP registered. Efforts are continuing to assess the remaining 312 individuals.
Conclusion: These patient-derived data show a minimum risk of TB disease of 10.5% at 10 years. The true rate could be even higher because (a) some persons may have moved/not been notified locally and (b) gamma-interferon test would now remove false positives. The NICE Guidelines section 12.2.8 (p 168) states “The health economic model shows cost-effectiveness when risk over 15 years after entry in the UK exceeds 12%”. These data show that this cohort of South Asian entrants have TB levels of a minimum of 10.5% suggesting it would be cost effective to screen such entrants (currently excluded) for latent TB infection.
THE EPIDEMIOLOGY AND TREATMENT OF ENVIRONMENTAL MYCOBACTERIA IN THE PORTSMOUTH AREA
J. Graves, S. Scrivener. Queen Alexandra Hospital, Portsmouth, UK
Introduction: The occurrence of environmental mycobacteria in patients’ microbiological samples processed at The Queen Alexandra Hospital in Portsmouth was investigated. The numbers and types of organisms identified were noted, and whether these patients were investigated and treated in accordance with the 2000 BTS guidelines. Further information on tolerance and success rates of treatment was also gathered where applicable.
Methods: The microbiology department generated a list of all the patients who had grown an atypical mycobacterium, from any site, between 1/5/2004 and 31/5/2006. All of these patients’ case notes were reviewed by a clinician. Information was collected on organism type, site of infection, number of positive samples, patients immune status, presence of chronic lung disease, chest radiograph appearances, symptoms, whether the patient was treated, with which drugs, duration of treatment, success rate (conversion to culture negative) and tolerance of treatment.
Results: 79 patients were identified, with a total of 11 different organisms. 57% were male and 43% were female. Out of the environmental mycobacterium that can more commonly cause disease, MAI (31%) was the commonest organism identified. This was followed by M. Xenopi (18%), M. Chelonae (13%), M. Malmoense (7%) and M. Kansasii (2%). Bronchiectasis was the commonest concomitant lung disease identified (32%). 22% of the patients had some form of immunocompromise. Only 30% of the patients growing an environmental mycobacterium were treated. 55% of those treated had MAI, 25% had M. Xenopi, 10% had M. Chelonae and 5% each had M. Kansasii and M. Malmoense. The ‘rapid-grower’ M. Chelonae patients were all Cystic Fibrosis Paediatric patients. Advice was taken from King’s College Paediatric TB Team regarding treatment. Neither patient became culture negative and treatment was abandoned. Out of the ‘slow-growers’ (MAI, Xenopi, Kansasii and Malmoense) antibiotics consistent with the guidelines were prescribed 94% of the time and the intended duration of treatment was consistent with the guidelines in 83% of patients. However, the intended duration of treatment was only met in 50% of cases and only 33% were culture negative at the end of treatment. 33% of patients did not tolerate the treatment. Reasons given included diarrhoea with lethargy, peripheral neuropathy, renal and liver toxicity and decreased visual acuity. Of the 70% of patients not treated, the commonest reason cited was that the organism was felt to be a contaminant (60%). Other reasons included death and concomitant treatment for mycobacterium tuberculosis.
Discussion: Environmental mycobacteria are widely distributed in nature and are often found without evidence of disease. There is much debate as to which patients require treatment, with which drugs and for how long. The current guidelines are complex and do not include evidence from recent trials and hence clinicians have been uncertain or reluctant to follow them. Our survey found that MAI was the commonest organism identified. Although the antibiotics and intended duration of treatment stated at the start were usually consistent with the guidelines, we found that only 50% of cases complied with this, with about 1/3 becoming culture negative at the end of treatment. It should be noted that 1/3 of our patient remained on their treatment at the time of the survey, which may therefore underestimate this cure rate. Up to date guidelines are needed for management of these patients, and management by physicians with experience and expertise in this field is essential in order to provide the best service for these complex patients who frequently have significant other co-morbidities.
INCREASING ANTI-TUBERCULOSIS DRUG RESISTANCE IN THE UK
M. E. Kruijshaar3, J. M. Watson3, F. Drobniewski4, C. Anderson3, J. G. Magee2, E. G. Smith1, I. Abubakar3. 1Health Protection Agency, Centre for Infections, London, UK; 2Health Protection Agency, Mycobacterium Reference Unit, London, UK; 3Health Protection Agency, Regional Centre for Mycobacteriology, Newcastle, UK
Background: The incidence of tuberculosis is increasing in England, Wales and Northern Ireland. This study examines the recent trends in, and factors associated with, anti-tuberculosis drug resistance in these three countries.
Methods: Information on drug susceptibility for Mycobacterium tuberculosis complex isolates was obtained from UK reference laboratories. Isolates were matched to tuberculosis cases reported to the enhanced tuberculosis surveillance system, which contains clinical and demographic information. Trends in drug resistance and associated factors were analysed using logistic regression. Strain typing information for cases with multi-drug resistant tuberculosis (MDR-TB) were obtained from the reference laboratories.
Results: The proportion of culture-confirmed cases with MDR-TB remained stable between 1998 and 2005 at around 1%. Resistance to isoniazid increased from 5% to 7% in the first five years of this period. Rifampicin, ethambutol and pyrazinamide resistance remained stable at around 1.2%, 0.4% and 0.6% respectively. The increase in isoniazid resistance outside London was a result of changes in place of birth and ethnicity of cases. In London, the rise was related to an outbreak. For cases with MDR-TB susceptibility to second line drugs was available for cases reported in 2002 (84% of cases), 2003 (86%), 2004 (95%) and 2005 (100%). One case was identified as extensively drug resistant (XDR). This case was reported in 2003. Strain typing information was available for 42% of MDR-TB cases reported in 2004–5. The proportion clustered was 20%.
Conclusions: The level of MDR-TB has remained stable despite increases in isoniazid resistance. Strain typing data suggest that some transmission of MDR-TB may be occurring, but the data are limited and most cases for which data were available were unclustered. The increase in isoniazid resistance reflects changes in the characteristics of cases and inadequate control of transmission in London. The observed increases highlight the need for early case detection, rapid drug susceptibility testing and improving treatment completion. Universal strain typing will facilitate the investigation of these trends.
A COMPARISON OF TUBERCULOSIS CASE RATES IN THE HOME-BORN WHITE POPULATIONS OF THE UK AND USA: AN INCREASING DISPARITY
S. Durairaj, N. Schluger, M. Asim, N. Sinnott, P. D. O. Davies. Cardio-thoracic Centre, Liverpool, UK
Introduction: In 2005 we presented data regarding the increasing TB rates in England compared with a decreasing trend in USA. (Duraira, Davies PDO. Increasing tuberculosis in England and Wales compared with a decreasing trend in the USA: a matter of migration. Thorax 2005;60:ii20.) We have now carried out a further analysis to compare case rates in the home-born White populations of the UK and USA.
Methods: Data were compared using government based websites www.cdc.gov for USA statistics and www.hpa.org.uk for the UK.
Results: We compared the rate of TB in the home-born White populations of the UK and USA over the most recent 12-year period for which data are available. The data show that in 1993, the rates/100 000 for the US born White population was 3.6, compared with 4.78 for the equivalent population in UK. By 2001 the rate in the White home-born US population was 1.5 compared with the equivalent UK figure of 3.6. The latest available data are for 2005. In this year the rate in US White home-born population had declined further to 1.3 compared with the UK figure which had remained static at 3.6 (see fig). The difference in the rates in similar population groups are therefore nearly three times higher in UK compared with the USA. As seen in the figure the US rates continue to decline in the home born White population compared with rates in UK.

Conclusion: There is a widening disparity between rates of TB in the White home-born US population compared with the equivalent UK population. Rates in the UK group seem to have stopped declining. The reasons for the disparity is not yet clear. It is possible that the more aggressive policy of giving preventive therapy to individuals with latent tuberculosis in the US may be making some contribution. One possible explanation could be that there may be unidentified transmission from immigrants to the White population within the UK where TB among some ethnic minority groups is rising, whereas rates among all groups in the US continue to fall (Duraira et al, 2005).
ACCURATE DATA COLLECTION: IMPACT ON TREATMENT OUTCOMES AT A RURAL TB PROJECT IN ZIMBABWE
R. M. Smith1, K. M. Scott2, R. D. Barker1, F. J. C. Millard1, M. Glenshaw3, E. Manomano3. 1Department of Respiratory Medicine, King’s College Hospital; 2King’s College, London School of Medicine at Guy’s, King’s and St Thomas’s Hospitals, London, UK; 3Murambinda Mission Hospital, Buhera, Zimbabwe
Introduction: Our first attempts to determine treatment outcomes for the rural TB project in Buhera district, Zimbabwe showed poor case detection; during 2004 the TB detection rate was 422/100 000/year (64% of WHO estimate). However, treatment outcomes for those registered appeared suspiciously good considering the high HIV prevalence (see table). We wished to improve the accuracy of data collection to determine “true” outcomes.
Methods: Two data managers have been employed. They have made concerted efforts to establish accurate treatment outcomes by regularly visiting the district’s primary healthcare clinics and supporting the home-based care team with defaulter follow-up.
Results: Treatment outcomes reported for 2005 were worse than for 2004; only 44% achieved treatment success in 2005 and 46% defaulted. We believe this apparent deterioration in outcomes is a reflection of increasingly accurate data recording. Patients had been recorded as treatment complete when their outcomes were unknown. Revised results following intensive activities to gain true outcomes for those treated in 2005, and data from 2006 will be presented.
Conclusions: TB notifications in the district remain below WHO estimates. The data are likely to be more accurate than previously reported. It is essential that true outcomes are recorded in order that the problems can be defined and appropriate strategies for improving TB control implemented. These “truer” TB treatment outcomes are far from meeting the Stop TB Partnership Targets. Treatment success rates are low, and very few patients achieve “cure”. Follow-up of defaulters is difficult in such rural settings but essential in order to avoid emergence of drug-resistant TB. Systems previously in place for follow-up of defaulters have largely disintegrated owing to the political and economic situation. Further research is necessary. However, a picture is emerging of poor access to chronically under-resourced healthcare services leading to poor case detection and case holding. Local and national initiatives are needed, including improved access to diagnosis by decentralisation of sputum collection, support of the national laboratory in provision of culture and DST, collaboration with the HIV service and continued strengthening of patient follow-up at the community level. We in the UK can help by providing financial and technical support for these interventions.
INCREASING TREND OF NON-TUBERCULOUS MYCOBACTERIA IN ENGLAND, WALES AND NORTHERN IRELAND 1995–2006: REAL OR ARTEFACT?
R. M. Smith1, K. M. Scott2, R. D. Barker1, F. J. C. Millard1, M. Glenshaw3, E. Manomano3. 1Department of Respiratory Medicine, King’s College Hospital; 2King’s College, London School of Medicine at Guy’s, King’s and St Thomas’s Hospitals, London, UK; 3Murambinda Mission Hospital, Buhera, Zimbabwe
Introduction: Since the late 1980s, the number of cases of tuberculosis has increased in England, Wales and Northern Ireland. In light of this, reports of infections with non-tuberculous mycobacteria were investigated to see whether such infections showed similar trends.
Methods: Hospital laboratories in England, Wales and Northern Ireland voluntarily report mycobacterial infections to the Health Protection Agency Centre for Infections. Details routinely reported include age and sex of the patient, species and specimen type. All records of non-tuberculous mycobacterial infection between 1995 and 2006 were extracted and analysed.
Results: The number of reported infections rose from 460 in 1995 to 1609 in 2006, an increase of 350%. Nine out of fourteen species reported increased in numbers over the period studied. The six most commonly reported species in 2006 were M avium-intracellulare, M gordonae, M kansasii, M malmoense, M chelonae and M xenopi. These species account for 82% of all infections. Most infections were in males (60%) and in older age groups (51% were over 60) and 73% were isolated from pulmonary specimens.
Conclusions: The total number of non-tuberculous mycobacterial infections reported has increased considerably since 1995. This may be due to changes in diagnostic and reporting practices and the rise in HIV infection and other causes of immunosuppression in the population. An investigation into possible contributions to this increase will be presented.
Asthma: clinical aspects
THE EFFECT OF MECHANICAL HEAT RECOVERY VENTILATION ON THE CONTROL OF ASTHMA: A RANDOMISED CONTROLLED TRIAL
G. R. Wright1, S. G. Howieson2, C. Mcsharry1, A. D. Mcmahon1, R. Chaudhuri1, J. Thompson1, I. Fraser1, L. Mcalpine3, S. Wood1, N. C. Thomson1. 1University of Glasgow; 2University of Strathclyde; 3Monklands General Hospital, Loncashire, UK
Background: Sensitivity to the house dust mite allergen Dermatophagoides pteronyssinus 1(Der p1) is commonly associated with asthma in the UK. The warm, humid environment of modern homes favours the house dust mite population, but the effect of improved domestic ventilation on the control of asthma is uncertain.
Methods: We conducted a randomised double-blind placebo-controlled trial of the installation of mechanical heat recovery ventilation in the homes of 120 adults with asthma who were sensitive to Der p1. Activation of the unit was concealed from the subjects; half were activated at randomisation, the others were inactive for the 12 months of the study. All subjects had conventional allergen avoidance at baseline. The primary outcome measure was morning peak expiratory flow at 12 months. Secondary outcome measures included evening peak expiratory flow rate, asthma control questionnaire score, St George’s Respiratory Questionnaire score, courses of oral corticosteroids, hospitalisation, rhinitis visual analogue scores, relative humidity, Der p1 levels, and specific IgE to house dust mite.
Results: At 12 months, the change in mean morning peak expiratory flow, as compared with baseline, did not differ between the mechanical ventilation group and the control group (mean difference 13.59 l/min, 95% CL −2.66 to 29.85, p = 0.100). However, evening mean peak expiratory flow was significantly improved in the mechanical ventilation group (mean difference 24.56 l/min, 95% Cl 8.97 to 40.15, p = 0.002) and there were fewer hospitalisations for asthma. (0 vs 4, p = 0.029). Values for other clinical outcome measures did not differ between the two groups at 12 months. Nasal symptoms significantly improved in the MHRV group compared to the control group at 6 months (nasal discharge mean difference −1.36, 95% Cl −2.30 to −0.42, p = 0.005), but not at 12 months (mean difference −0.46, Cl −1.47 to 0.55, p = 0.371). Indoor relative humidity was reduced more effectively in the bedrooms of mechanically ventilated homes in winter months. Der p1 analysis is awaited.
Conclusion: Installation of mechanical ventilation in the homes of adults with chronic asthma and sensitivity to house dust mite results in an improvement in some indices of asthma control.
EXAMINING THE RELATION BETWEEN ASTHMA AND RHINITIS RESPONSE FOLLOWING OMALIZUMAB THERAPY
L. P. Boulet1, R. Niven2. 1Institut de Cardiologie et de Pneumologie de l’Universite Laval, Qubec, Canada; 1North West Lung Centre, Manchester, UK
Background: Omalizumab, an anti-IgE antibody, has proven efficacy as add-on therapy in the treatment of severe persistent allergic (IgE-mediated) asthma, reducing exacerbations, emergency visits, and improving quality of life. Additionally, improvements in rhinitis control have been seen in patients with persistent allergic rhinitis. We investigated the relationship between efficacy of omalizumab on lung and nasal outcomes in patients with co-existing allergic (IgE-mediated) asthma and rhinitis.
Methods: This post hoc analysis of the SOLAR study examined whether a response to omalizumab in terms of asthma control predicted a higher likelihood of a large rhinitis response. Patients were classified as asthma responders if they were judged by the physician to have achieved complete or marked improvement in asthma control according to a five-level evaluation (complete control; marked improvement in control; discernable but limited control; no appreciable change; worsening in control), based on multiple aspects of response including patient interviews, review of medical notes, spirometry and diaries of symptoms, rescue medication use and peak expiratory flow. Patients were classified as having a large rhinitis response if they achieved a ⩾1.5-point improvement in Rhinitis Quality of Life Questionnaire (RQLQ) overall score. The RQLQ self-administered questionnaire contains 28 items covering eight domains (overall, activity limitation, sleep impairment, non-nasal or non-ocular symptoms, practical problems, nasal symptoms, eye symptoms, emotional function), and assesses the previous seven days.
Results: Data were available for 207 omalizumab patients (123 (59.4%) asthma responders, 84 (40.6%) asthma non-responders) and 192 placebo patients. Overall, 90% of patients had severe persistent asthma according to GINA 2002 classification. The likelihood of a large rhinitis response (⩾1.5-point improvement in RQLQ) was significantly greater in omalizumab-treated asthma responders than in the placebo group (64.2% vs 35.4%, p<0.001). In patients who did not respond to omalizumab in terms their asthma, the percentage of patients who responded in terms of their rhinitis (32.1%) was similar to placebo. The odds ratio for a large rhinitis response in omalizumab-treated asthma responders vs asthma non-responders was 3.79 (95% CI 2.11 to 6.82).
Conclusions: Response to omalizumab therapy in terms of improvement in asthma control is associated with a significantly increased probability of improvement in quality of life associated with rhinitis symptoms. Omalizumab-treated asthma responders are 3.8 times more likely to experience a large (⩾1.5 point) improvement in rhinitis related quality of life scores than omalizumab-treated asthma non-responders.
EFFECT OF INHALED CORTICOSTEROIDS ON SMALL AIRWAY DYSFUNCTION IN MILD TO MODERATE PERSISTENT ASTHMATICS
D. Menzies, S. Ismail, P. Hopkinson, A. Nair, B. Lipworth. University of Dundee, Dundee, UK
Background: Small airway dysfunction in asthma is poorly characterised. We have investigated the effect of inhaled corticosteroids (ICS) on small airway inflammation and calibre in adult asthmatics.
Methods: After withdrawal of usual treatment and a steroid free run-in, mild to moderate persistent asthmatics underwent four weeks of prospective treatment with 800 μg per day of inhaled beclometasone. Healthy volunteers acted as a control group. Airway inflammation was quantified using tidal (FENO) and alveolar (CALV) nitric oxide, and bronchial flux (JNO). Impulse oscillometry was used to determine total, central and peripheral airway resistance.
Results: Compared with healthy volunteers (n = 27), asthmatics (n = 21) after withdrawal of usual ICS treatment had significantly different values for FENO (median 10.7 ppb; IQR 17.9 to 17.7 vs 33.8 ppb; 16.8 to 52.5, p<0.001); JNO (0.48 nl/s; 0.37 to 0.89 vs 1.71 nl/s; 0.67 to 2.55, p<0.001); CALV (1.27 ppb; −1.00 to 2.07 vs 2.14 ppb; 1.49 to 3.95, p = 0.009); total resistance (0.49 kPa/sl; 0.36 to 0.64 vs 0.36 kPa/sl; 0.30 to 0.41, p = 0.002); and peripheral resistance (0.09 kPa/sl; 0.02 to 0.16 vs 0.01 kPa/sl; −0.01 to 0.03, p<0.001); but not central resistance (0.38 kPa/sl; 0.35 to 0.47 vs 0.36 kPa/sl; 0.29 to 0.39, p = 0.099). ICS attenuated FENO (p<0.001), JNO (p<0.001) and CALV (p = 0.012), such that values were no longer significantly different from HV (p = 0.59, 0.79 and 0.66 respectively). There were no commensurate changes in peripheral airway resistance or spirometry indices.
Conclusion: Treatment with ICS suppresses peripheral inflammation in mild to moderate asthmatics, but has no effect on airway calibre.

THE LONGITUDINAL CORRELATION BETWEEN FRACTIONAL EXHALED NITRIC OXIDE AND SPUTUM EOSINOPHIL COUNTS IN REFRACTORY ASTHMA
P. Haldar, S. Birring, M. Berry, C. Brightling, P. Bradding, A. Wardlaw, I. Pavord, R. Green. Institute for Lung Health, Leicester, UK
Introduction: Fractional exhaled nitric oxide (FeNO) concentrations correlate significantly with sputum eosinophil counts in cross-sectional studies of asthma and have been proposed as a simple clinical tool for monitoring eosinophilic airway inflammation. However, little is known of the longitudinal correlation between these parameters. We investigated this relation in 88 patients with refractory asthma who are current non-smokers regularly attending the Glenfield Hospital Difficult Asthma Clinic.
Methods: All patients had 3 or more paired measurements of FeNO at 50 ml/s and induced sputum eosinophil counts over time. Longitudinal correlation coefficients (Lc) were calculated from within subject analysis of covariance of log transformed FeNO and % sputum eosinophil counts.
Results: 504 paired measurements were obtained (median 5/subject (range 3–12)). Baseline correlation between the parameters was weak but significant (r = 0.39, p<0.001). The overall within subject longitudinal correlation was weaker (Lc = 0.28, p<0.001). After stratifying the cohort according to concordance between FeNO and sputum eosinophils at baseline, subjects that exhibited concordance had superior longitudinal correlation (concordant group Lc = 0.34 vs discordant group Lc = 0.19). Within the discordant group, subjects expressing sputum eosinophilia without elevation of FeNO showed the poorest longitudinal correlation between the variables (Lc = 0.08, p = 0.48). We also explored the longitudinal correlation in measurements performed when subjects had concomitant symptoms (Juniper asthma control score >1.57). No significant longitudinal correlation was seen between the parameters during expression of symptoms (Lc = 0.05 calculated from 240 measurements in 68 patients, p = 0.471). This dissociation was mainly due to persistent elevation of FeNO in the absence of sputum eosinophilia (seen with 47.7% of measurements). Compared with the entire cohort, the subgroup of patients expressing this pattern (n = 16) were predominantly female (87% vs 44%, p = 0.002), younger (mean age 39 vs 49.8 yrs, p = 0.002) with minimal eosinophilic inflammation (GM Eos 0.67% vs 4,5%, p = 0.001).
Conclusion: Although a significant longitudinal correlation exists between FeNO and sputum eosinophil counts this is of weaker magnitude than cross-sectional measurements. In a subgroup of patients with uncontrolled asthma symptoms there is no longitudinal correlation between FeNO and sputum eosinophils. The clinical applicability of FeNO guided therapy for refractory asthma may therefore be limited.
A QUALITATIVE ANALYSIS OF HRCT SCANS IN DIFFICULT ASTHMA
S. Gupta1, S. Siddiqui1, P. Haldar1, M. Berry1, R. Green1 J. Entwisle2, I. Pavord1, A. Wardlaw1, C. Brightling1. 1Institute for Lung Health, Glenfield Hospital; 2Glenfield Hospital, University Hospitals of Leicester, UK
Aim: Bronchial wall thickening (BWT) and bronchiectasis (BE) are familiar radiological features in asthma. We sought to identify the prevalence of these airway geometry changes in a large difficult asthma cohort and to explore the association between BWT, BE and clinical characteristics.
Materials and Methods: Patients attending our “Difficult Asthma Clinic” are extensively characterised in terms of history, lung function, health status and airway inflammation. Out of 463 patients attending our clinic between February 2000 and November 2006, 185 had HRCT scans and were included in the study. Thoracic radiologists determined the presence of BWT or BE. Patients were categorised into those with neither BWT or BE (BWT-/BE-), BE only (BWT-/BE+), BWT only (BWT+/BE-) or both (BWT+/BE+).
Results: The difficult asthma cohort (n = 185) had a mean (SEM) age 49.75 (1.0) years, male: female ratio 73:112, disease duration 26.2 (1.4) years and smoking history of 6.77 (1.0) pack years. Other clinical characteristics for the whole cohort were: FEV1/FVC ratio 69.69 (1.1), FEV1 % predicted 72.38 (2.0), bronchodilator response (BDR) 8.59 (1.0)%, BDP equivalent 2289 (237.5), sputum neutrophils 61.76 (2.1) %, sputum eosinophils (geometric mean 2.06 (95% CI 1.6–2.7)%. Four distinct groups were formed based on presence or absence of bronchiectasis and bronchial wall thickening. Clinical characteristics of each group were as shown in the table.
Conclusion: Bronchiectasis independent of bronchial wall thickening is associated with airflow limitation, longer disease duration and higher age in difficult asthma. Further quantitative and longitudinal studies are required to assess airway calibre in this disease cohort.
THE RELATIONSHIP BETWEEN GASTRO-OESOPHAGEAL REFLUX AND VOCAL CORD DYSFUNCTION IN A CLINICAL SETTING
N. J. Pargeter, A. H. Mansur. Severe Asthma Unit, Birmingham HeartlandsHospital, UK
Introduction: Vocal cord dysfunction (VCD) represents paradoxical inspiratory vocal cord adduction and is commonly misdiagnosed as asthma. Various case reports have implicated gastro-oesophageal reflux disease (GORD) in triggering VCD. However, the exact prevalence of GORD in VCD has not been previously reported, which is the subject of this study.
Method: Eighty patients (66 females, 14 males, mean age 47.7, age range 16–79) consecutively referred to a VCD clinic were studied using a pre-designed protocol that included in-depth interviews and flow volume loops. Diagnosis of VCD was made via nasendoscopy. The cohort comprised three groups: confirmed VCD (by nasendoscopy); suspected VCD (not seen on nasendoscopy but suggestive from flow volume loops and/or classical symptoms); excluded VCD. Diagnosis of GORD was made by barium swallow and/or 24-h pH monitoring. GORD positive patients (60/80, 75%) received at least eight weeks of twice-daily, high-dose proton pump inhibitor (PPI) therapy. Due to poor GORD symptom control 6/60 (10%) went on to have anti-reflux fundoplication surgery, in line with their physicians’ recommendations. Patients were asked for feedback on their throat symptoms pre and post GORD treatment.
Results: VCD diagnosis was confirmed in 34 patients (42.5%), of which, 28 (82%) had physician diagnosed asthma and 27 (79%) had GORD. In the GORD positive group, nasendoscopy showed refluxive change in the larynx in 20/27 patients (74%). 22/27 patients (81.5%) attributed reflux as a trigger of VCD. However, only 6/27 (22.2%) reported improvement in VCD symptoms following anti-reflux treatment. Thirty one patients conformed to suggestive VCD diagnosis. In this group, 28 (90%) had physician diagnosed asthma. 25/31 patients (81%) had GORD and 18/25 (72%) had laryngeal refluxive change on nasendoscopy. 22/25 (88%) reported reflux as a common trigger of VCD, but only 9/25 (36%) reported improvement in symptoms following anti-reflux treatment. VCD was excluded in 15 patients whose symptoms were attributed to throat irritation 9/15 (60%) and globus pharyngeus 6/15 (40%). In this group, 9 patients (60%) also suffered from asthma and 8/15 (53%) had GORD. Laryngeal refluxive change was observed in 2/8 (25%) cases. 3/8 patients (37.5%) reported symptom improvement following anti-reflux treatment.
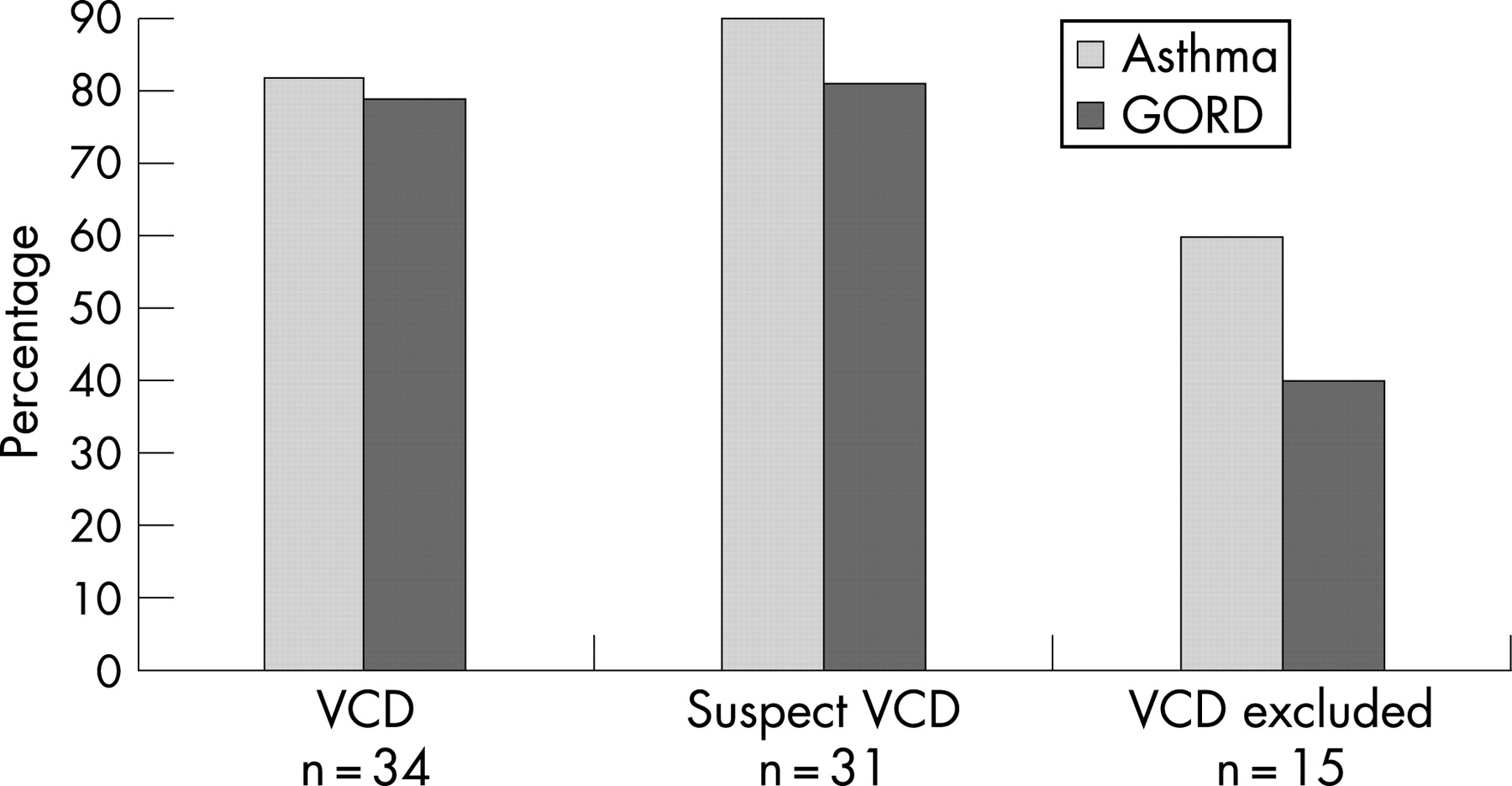
Conclusion: GORD is common in patients with confirmed and suspected cases of VCD and is reported as a trigger for VCD in the majority of patients in this group. However, anti-reflux treatment seems to be effective in a minority of GORD confirmed cases, which would implicate other factors in VCD aetiology.
Clinical trials in NIV
NON-INVASIVE VENTILATION IN PATIENTS WITH ACUTE CARDIOGENIC PULMONARY OEDEMA: THE 3CPO TRIAL (A MULTICENTRE RANDOMISED CONTROLLED TRIAL)
A. Gray1, M. W. Elliott4, S. Goodacre3, D. E. Newby2, F. Sampson3, J. Nicholl3, M. Masson1. 1Royal Infirmary of Edinburgh; 2University of Edinburgh; 3University of Sheffield; 4St James’s University Hospital, Leeds, UK
Introduction: This open prospective randomised trial of the early management of acute cardiogenic pulmonary oedema (ACPO), aimed to determine (a) the clinical effectiveness of non-invasive ventilation (CPAP or NIPPV) and standard therapy against standard therapy alone, and (b) the comparative effectiveness of CPAP and NIPPV.
Setting: Emergency Departments of 26 centres between July 2003 and April 2007. Entry criteria: Clinical/radiological characteristics of ACPO, respiratory rate>20/min, arterial hydrogen ion >45 nmol/l (pH<7.35). Intervention: standard therapy, non-invasive positive pressure ventilation (NIPPV; inspiratory pressure 8–20 CmH2O, expiratory pressure 4–10 cmH2O) or (CPAP; 5–15 cmH2O). All patients received standard medical treatment at discretion of treating physician. Oxygen was titrated to a maximum of 60%.
Outcomes: Primary: 7-day mortality for standard therapy versus non-invasive ventilation. Secondary: 30-day mortality, combined 7-day mortality and intubation rate. Ancillary: Improvement in physiology, symptoms, myocardial infarction and intubation rates. Power calculation: Sample size 1,200 to detect 6% mortality difference with 80% power. Intention-to-treat analysis.
Results: 1069 patients (mean age 78 years; 43% male) were recruited and randomised to standard therapy (n = 367), CPAP (n = 346; 10 (4) cmH2O) or NIPPV (356; 14 (5)/7 (2) cmH2O). At entry patients were tachycardic (heart rate 113 (22)/min), acidotic (pH 7.25 (0.11)), tachypnoeic (respiratory rate 32 (7)/min) and hypoxic (oxygen saturation 90 (8)%). Compared to standard therapy, non-invasive ventilation was associated with greater improvements in tachycardia (102 (23) vs 96 (22)/min, p<0.001), acidosis (pH 7.33 (0.11) vs 7.36 (0.11), p = 0.002) and tachypnoea (26 (6) vs 25 (6), p = 0.023) at one hour. The 7-day and 30-day mortality was similar for standard therapy and non-invasive ventilation (9.8% versus 9.5% (p = 0.869) and 16.6% versus 15.6% (p = 0.685) respectively). Combined end-point 7-day death or intubation rate was similar for both forms of non-invasive ventilation (11.7% vs 11.1%, CPAP vs NIPPV; p = 0.806).
Conclusions: In patients with ACPO, non-invasive ventilation induces a faster improvement in respiratory distress and metabolic disturbance, but has no effect on short-term mortality. CPAP and NIPPV appear to be equally efficacious.
Funding: This project was funded by the NIHR Health Technology Assessment Programme (project number 01/43/01). The views and opinions expressed are those of the authors and do not necessarily reflect those of the Department of Health.
SHORT- AND LONG-TERM MORTALITY FOLLOWING NON-INVASIVE VENTILATORY SUPPORT FOR ACUTE TYPE II RESPIRATORY FAILURE
J. C. Bright, R. Karadi, P. M. Turkington, B. R. O’Driscoll. Salford Royal NHS Foundation Trust, UK
Background: Non-invasive ventilation (NIV) is now widely available in the UK for the support of type II respiratory failure. Ventilatory support for COPD and OHVS (obesity hypoventilation) is accepted but its use in acute pulmonary oedema (APO) and pneumonia remains controversial. Despite this “real world” usage of NIV is increasing.
Aims: To determine the outcome for patients who presented to the acute medical on-call service with Acute Type II Respiratory Failure requiring NIV.
Methods: Retrospective analysis of admissions to Salford Royal Hospital’s Medical High Dependency March 2001–August 2006 with Type II respiratory failure who required non-invasive bi-level ventilation (BiPAP). Only acute presentations were reviewed. All information was obtained from electronic patient hospital records (i SOFT).
Results: 67% of admitting physicians were non-respiratory trainees. 297 patients (140 male, 157 female) with 331 admissions (282 new and 49 repeat) were studied. Admission diagnosis: acute pulmonary oedema (APO) 31, COPD 199 (COPD alone 143), COPD+OHVS 22, OHVS 21, pneumonia 18, others 40.
Conclusions: Despite the use of ventilatory support, Type II respiratory failure is still associated with a poor short- and long-term prognosis. The high early mortality may reflect poor patient selection by the admitting physician. If the findings are reproducible consideration of formal training in ventilatory support for all general physicians participating in the acute on call is warranted. The worst prognosis was observed in the APO and pneumonia cohorts. OHVS cohort had the best outcome.
PREDICTORS OF A SUCCESSFUL OUTCOME IN NON-INVASIVE VENTILATION FOR ACUTE HYPERCAPNIC RESPIRATORY FAILURE: A PROSPECTIVE OBSERVATIONAL STUDY
B. Chakrabarti1, R. M. Angus2, S. Agarwal2, S. Lane3, P. M. A. Calverley1. 1Clinical Sciences Centre, University Hospital Aintree; 2Aintree Chest Centre, University Hospital Aintree; 3Department of Medical Statistics, University of Liverpool, UK
Introduction: Non-invasive ventilation (NIV) reduces both the need for intubation and mortality in acute hypercapnic respiratory failure (AHRF). We have prospectively identified variables associated with an increased likelihood of NIV failure in AHRF to determine whether hyperglycaemia has an independent effect on outcome.
Methodology: All patients receiving NIV within 24 h of admission for respiratory acidosis complicating AHRF (pH<7.35; PaCO2 >6 kPa) at University Hospital Aintree between June 2006 and June 2007 were studied. On admission, blood samples including random blood glucose (RBG) were taken before NIV began.
Results: 100 consecutive episodes in 88 patients fulfilled the entry criteria; COPD exacerbations ± pneumonia accounting for 86%. NIV failure occurred in 16%. On univariate analysis, NIV failure was associated with increasing age (76 vs 68 years; p = 0.013), elevated RBG (8.99 mmol/l vs 6.86 mmol/l; p = 0.002), baseline RR (33 vs 26; p = 0.001), APACHE 2 score (18.75 vs 14.39; p = 0.001) and mean 1- and 4-h pH (7.25 vs 7.29; p = 0.028; 7.32 vs 7.27; p = 0.017); a possible relation existed with baseline pH (7.26 vs 7.21; p = 0.097), female gender (p = 0.051) and lower GCS (p = 0.08). NIV failure occurred in 31% (15/48) when RBG was ⩾7 mmol/l compared to 2% (1/50) where RBG ⩽6.9 mmol/l (p = 0.003). NIV failure was not associated with pneumonia, lung function, delay in NIV administration and a previous diagnosis of diabetes mellitus (p>0.1). On multivariate analysis, baseline RR (p = 0.019), RBG ⩾7 mmol/l (p = 0.028), female gender (p = 0.010), 1-h pH (p = 0.049) and 4-h pH (p = 0.007) emerged significant correctly classifying 99% of successes and 75% of failures. An ROC curve was constructed between RR and NIV outcome (area under curve 0.775; p = 0.001). The success rate of NIV reached 98% (43/44) in the subgroup with combination of baseline RR ⩽30/min and RBG <7 mmol/l contrasting to just 42% (8/19) in the sub-group with baseline RR >30/min and RBG ⩾7 mmol/l.
Conclusions: Glycaemia on admission is independently associated with failure of NIV in acute AHRF. Success of NIV in AHRF is more likely in patients with a baseline respiratory rate ⩽30/minute and a random glucose <7 mmol/l.
NON-INVASIVE VENTILATION IN MOTOR NEURON DISEASE: AN AUDIT OF CURRENT PRACTICE
B. Green, K. Adeniji, J. Wilkinson. Southampton General Hospital, UK
Background: The use of non-invasive ventilation (NIV) for symptom palliation in motor neuron disease (MND) is now well recognised, however uptake and access to NIV services shows significant regional variation. An MND NIV service was established in Southampton in 2004 for patients with respiratory symptoms or declining lung function. The possible benefits of NIV use in MND are discussed at initial assessment. Patients are offered a trial of NIV on the basis of orthopnea or symptoms of hypercapnia.
Objective: To evaluate referral outcome and degree of respiratory compromise at the time of referral by retrospective notes audit.
Results: Fifty two referrals were identified over a three-year period. 22 (42.3%) received a trial of NIV. 16 (72.7%) tolerated NIV trial. 10 died before the trial, 2 were inappropriate for, and 5 declined an NIV trial. 13 received active follow-up. 15 (28.8%) accepted long-term NIV. 28 died over the audit period. Median survival from time of diagnosis for patients who accepted home NIV was 26 months compared to 13 months for patients who failed to tolerate NIV (p = 0.03). There was no significant correlation between time to referral, BMI, bicarbonate, PaCO2, forced vital capacity (FVC)% predicted, bulbar score, orthopnea or hypercapnic symptoms, and overall outcome of the referral. Patients tolerating NIV had higher mean arterial bicarbonate (28.1 vs 25.1 mmol/l, p = 0.04) and higher PaCO2 (5.85 vs 5.12 kPa, p = 0.05) than patients that failed NIV trials. Patients who failed an NIV trial had a mean FVC% predicted of 51% compared to 36% in patients who accepted NIV (p = 0.014). No significant correlation between toleration of NIV and bulbar dysfunction score was seen (p = 0.265).
Conclusions: When an NIV service is available to MND patients its use is widely applicable and well tolerated. We observed a significant survival advantage in patients who accept home NIV although the aim of the treatment is symptom palliation. Although severity of bulbar dysfunction has previously been cited as a limitation to the use of NIV our findings do not support this. NIV was better tolerated in patients with worse respiratory function as measured by lower FVC% predicted, higher bicarbonate and higher PaCO2.
LONG-TERM OUTCOME OF VENTILATORY SUPPORT IN PATIENTS WITH RESPIRATORY FAILURE DUE TO DUCHENNE MUSCULAR DYSTROPHY
M. Ali, I. E. Smith, T. Quinnell, J. M. Shneerson. 1Papworth Hospital NHS Trust, Cambridge, UK
Introduction: Duchenne muscular dystrophy (DMD) is an X-linked recessive disease characterised by progressive muscle weakness. Respiratory muscle weakness is inevitable and often leads to hypercapnic respiratory failure. Non-invasive ventilation (NIV) has been shown to improve quality of life and survival of patients with DMD who develop respiratory failure. One previous study from the UK has reported a five-year survival of 85% for hypercapnic DMD patients who were treated with NIV.
Aim: To evaluate the characteristics and long-term outcomes of patients with DMD referred to a specialist service.
Method: Patients were identified from the database. Thirty two case notes (between March 1985 and March 2007) were available for a retrospective review. Patients with Becker muscular dystrophy were excluded.
Results: All were males (mean age of 20 yrs at the time of referral). All were unable to walk. Eighteen (56%) had scoliosis. Median FEV1/FVC at the time of referral was 0.5 l/0.6 l (n = 14). Mean peak inspiratory and expiratory pressures were 35 and 32 cm H2O (n = 7 and 10 respectively). Eighteen (56%) had abnormalities detected on ECG or echocardiogram. Twenty two (69%) were given NIV over the period of study (including 19 who were given NIV at their first assessment)—13 had daytime hypercapnia, 3 had already been trialled on NIV, 2 had only nocturnal hypoventilation and 4 were weaned to long-term NIV after prolonged invasive ventilation. One failed to be weaned and required long-term tracheostomy ventilation. Median survival following NIV was 7 years (95% CI 1 to 12). Following NIV, one survived for 12 years and another was still alive 22 years later. Mean age at death for NIV users was 27 years. Among 22 NIV users, 10 reported pressure sores from the mask or nasal symptoms but all continued to use NIV.

Conclusion: This study reports the survival of DMD patients following NIV over a longer period than previously reported from the UK. Following NIV, median survival was 7 years whereas 2 patients were still alive at 10 years. Following prolonged invasive ventilation, 4 out of 5 were weaned successfully to long-term NIV.
PROSPECTIVE STUDY OF INITIATION OF HOME MECHANICAL VENTILATION TO INVESTIGATE THE CHANGES IN PATIENT DEMOGRAPHICS OVER A TWO-YEAR PERIOD
M. Jheeta, A. J. Williams, N. Grey, A. C. Davidson, N. Hart. Lane FoxRespiratory Unit St Thomas’ Hospital, London, UK
Background: Home mechanical ventilation (HMV) is an established treatment for patients with chronic hypercapnic respiratory failure due to a variety of conditions. Although the evidence for the treatment of obstructive airways disease (OAD) is limited (Meecham-Jones et al, 1995), there is evidence that HMV is useful for the management of chronic respiratory failure complicating neuromuscular disease (NMD) and chest wall disease (CWD) (Leger et al, 1994; Simonds and Elliot, 1995). More recently with the increasing numbers of obese patients presenting with chronic hypercapnic respiratory failure, HMV has been shown to be an effective therapy (Masa et al, 2001; Prez de Llano et al, 2005). Although the Eurovent survey (Lloyd-Owen et al, 2005) highlighted the differences in the demographics of HMV users across Europe, there was no particular focus on the patients with obstructive sleep apnoea and obesity hypoventilation syndrome (OSA/OHS). The aim of the current study was to assess the changes in HMV-user demographics in a regional centre over a two-year period.
Method: The data were collected from the electronic discharge summary database. In addition to basic patient details, information was collected about the admission episode including admission urgency, length of stay, diagnostic group, specific diagnosis, ventilator used and settings and interface. The groups were NMD, OAD, CWD, OSA/OHS, and other. We compared the data between May 2005 to May 2006 and May 2006 to May 2007.
Results: See table. Although there was no change in age, sex or admission urgency over the two-year period, there was a 14% increase in the number of patients initiated on HMV. Furthermore, there was a 23% decrease in the number of patients with NMD initiated on HMV. This was reflected by a fall in all of the specific neuromuscular disease groups. However, there was an increase of over 90% in the patients initiated on HMV with OSA/OHS. All other diagnostic groups remained relatively unchanged.
Conclusion: In addition to an overall increase in initiation of HMV over a two-year period, we have observed a change in the type of patients that are commenced on HMV. There has been a decrease in the NMD group, which was more than matched by an increase in the OSA/OHS group. This increase in activity and change in HMV-user demographics is likely to have significant implications on the structure of the service which will need to be modified in terms of nursing, medical and technical provision in order to adequately manage these differing patient groups.
Acknowledgement: MJ is a medical student at Guy’s, King’s & St Thomas’ School of Medicine who undertook this project as part of an extended Special Study Module.
Lung cancer: basic mechanisms
FOURIER TRANSFORM INFRARED SPECTROSCOPY MEASURING METABOLIC MARKERS IN SPUTUM IN PATIENTS WITH AND WITHOUT LUNG CANCER
R. Ghosal1, K. E. Lewis2, P. Kloer1, R. Mehta3, D. Parry3, C. Llewellyn-Jones1, S. L. Prior2, L. A. J. Mur4, P. D. Lewis2. 1Respiratory Unit, Carmarthenshire NHS Trust; 2School of Medicine, ILS, University of Swansea; 3Bro Morganwwg NHS Trust, Brigend; 4Institute of Biological Sciences, University of Wales,Aberystwyth, UK
Introduction: There are 1.3 million worldwide and over 37 000 new cases of lung cancer diagnosed in the UK each year. The incidence of lung cancer is higher in Wales than the UK average. MEDLUNG is a long-term study measuring different combinations of metabolic biomarkers for early detection of lung cancer. Biofluids, including sputum and serum, and biopsy tissue are being collected prospectively from people undergoing bronchoscopy for suspected lung cancer. A key objective of this project is to evaluate Fourier transform infrared (FTIR) spectroscopy for metabolic markers in sputum. FTIR is an established, cost effective technique that enables rapid, high-throughput analysis of different sample types. FTIR has great potential as a metabolic fingerprinting technique and has been applied in a wide variety of clinical settings. We have carried out a preliminary study to evaluate: (1) suitability of sputum as a biofluid for easy/cost effective processing for FTIR (2) ability of FTIR to distinguish between primary lung cancer and non-cancer cases from sputum.
Method: Patients: Five (biopsy proven) non-small cell lung cancer (cases) and 26 non-cancer controls (mixture of stable COPD patients, “healthy” smoking and non-smoking members of staff). Procedure: sputa was collected prior to bronchoscopy (cases) or in clinic (controls) and were frozen within 2–3 h. Sputum cells were isolated by centrifugation and freeze dried. Bronchial cell presence in sputum was confirmed by microscopy. Freeze dried cell extracts were processed in triplicate for FTIR. FTIR spectra data processing and multivariate analysis were performed using Matlab software.
Results: All sputum samples contained bronchial cells and lung cancer patients did not have more bronchial component. This suggests the difference in metabolites is due to different expression rather than cases just producing more sputum (cells).
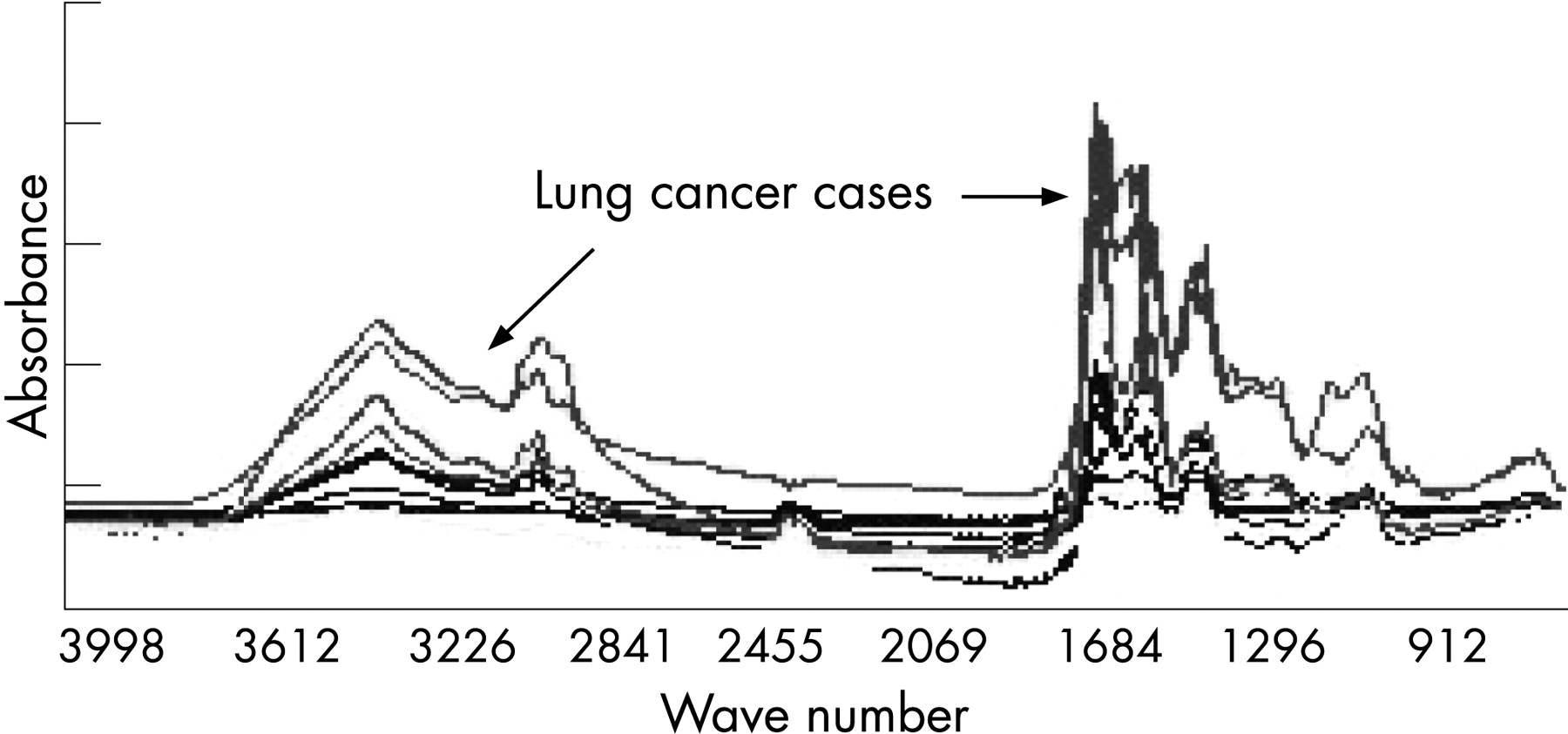

Conclusion: This pilot suggests that (1) sputum is suitable as a biofluid for easy/cost effective processing for FTIR and (2) FTIR can potentially distinguish between cancer and non-cancer cases in sputum. Greater recruitment and longer term (10-year) follow-up is now assessing combinations of biomarkers in not only diagnosing lung cancer, but detecting pre-cancerous lesions and monitoring response to treatment.
DEGRANULATION OF STROMAL MAST CELLS OF THE TRYPTASE-ONLY PHENOTYPE IS ASSOCIATED WITH IMPROVED PROGNOSIS IN NON-SMALL CELL LUNG CANCER
C. M. Ohri, A. Shikotra, T. Welsh, D. Waller, P. Bradding. Institute for Lung Health, Glenfield Hospital, Leicester, UK
Introduction: It is unclear whether mast cells play a role in preventing cancer formation. We have previously identified a survival advantage for patients with non-small cell lung cancer (NSCLC) who have mast cell infiltration of tumour islets compared to patients who do not.
Methods: The aim of this study was to identify the phenotype of mast cells (either MCTC, expressing both chymase and tryptase, or MCT, expressing tryptase only) and their state of degranulation in the tumour stroma and islets in NSCLC, using immunohistochemical analysis. The degree of each mast cell degranulation was evaluated using a degranulation index (DI) as follows: 0 = no degranulation, 1 = less than one third degranulation, 2 = one to two thirds degranulation, 3 = more than two thirds degranulation. We compared 20 patients with above median survival (mean survival = 1452 days) versus 20 patients with below median survival (mean survival = 256 days), (p<0.0001).
Results: The mean densities of MCTC and MCT in tumour islets were higher in patients with a survival above the median (1.2 (0.48) and 2.58 (0.40) cells/mm2 respectively) compared to those below the median (0.05 (0.02) and 0.19 (0.08) cells/mm2 respectively) (p = 0.003 for both MCTC and MCT). In patients with above median survival, the MCT phenotype in the stroma were degranulated to a greater degree than in those with below median survival (mean DI = 2.29 (0.073) versus 1.89 (0.112) respectively) (p = 0.007), as seen in figure 1. In figure 2, a ROC curve demonstrates five-year survival with regards to MCT DI in the stroma (area under curve = 0.798, 95% CI 0.661 to 0.934).
Conclusions: Both MCT and MCTC mast cells infiltrate the tumour islets in patients with NSCLC and good prognosis. While increasing islet infiltration by mast cells also predicts good prognosis, this is accompanied by a higher degree of MCT degranulation in the NSCLC stroma. Taken together, degranulating mast cells in the tumour stroma, when accompanied by mast cells infiltrating the tumour islets, contribute to an immune response which protects against tumour dissemination.


PROTEOMIC ANALYSIS OF RESECTABLE NON-SMALL CELL LUNG CANCER: IMPACT OF SMOKING, HISTOLOGICAL TYPE AND STAGE OF DISEASE
S. Rathinam1, S. Nyangoma2, D. Ward2, A. Alzetani1, J. Starczynski1, A. Martin2, P. Johnson2, N. D. James2, P. B. Rajesh1. 1Birmingham Heartlands Hospital, Foundation Trust; 2Cancer Research UK Institute for Cancer Studies, University of Birmingham, UK
Background: Surface Enhanced Laser Desorption Ionisation Time of flight Mass Spectrometry (SELDI-TOF-MS) is a mass spectrometry method used to generate “proteomic profiles” of body fluids such as serum. We have used this technique to produce serum proteomic profiles of non small cell lung cancer (NSCLC).
Aim: To determine the impact of smoking, histopathology of the tumour and staging on the proteomic profiles in NSCLC.
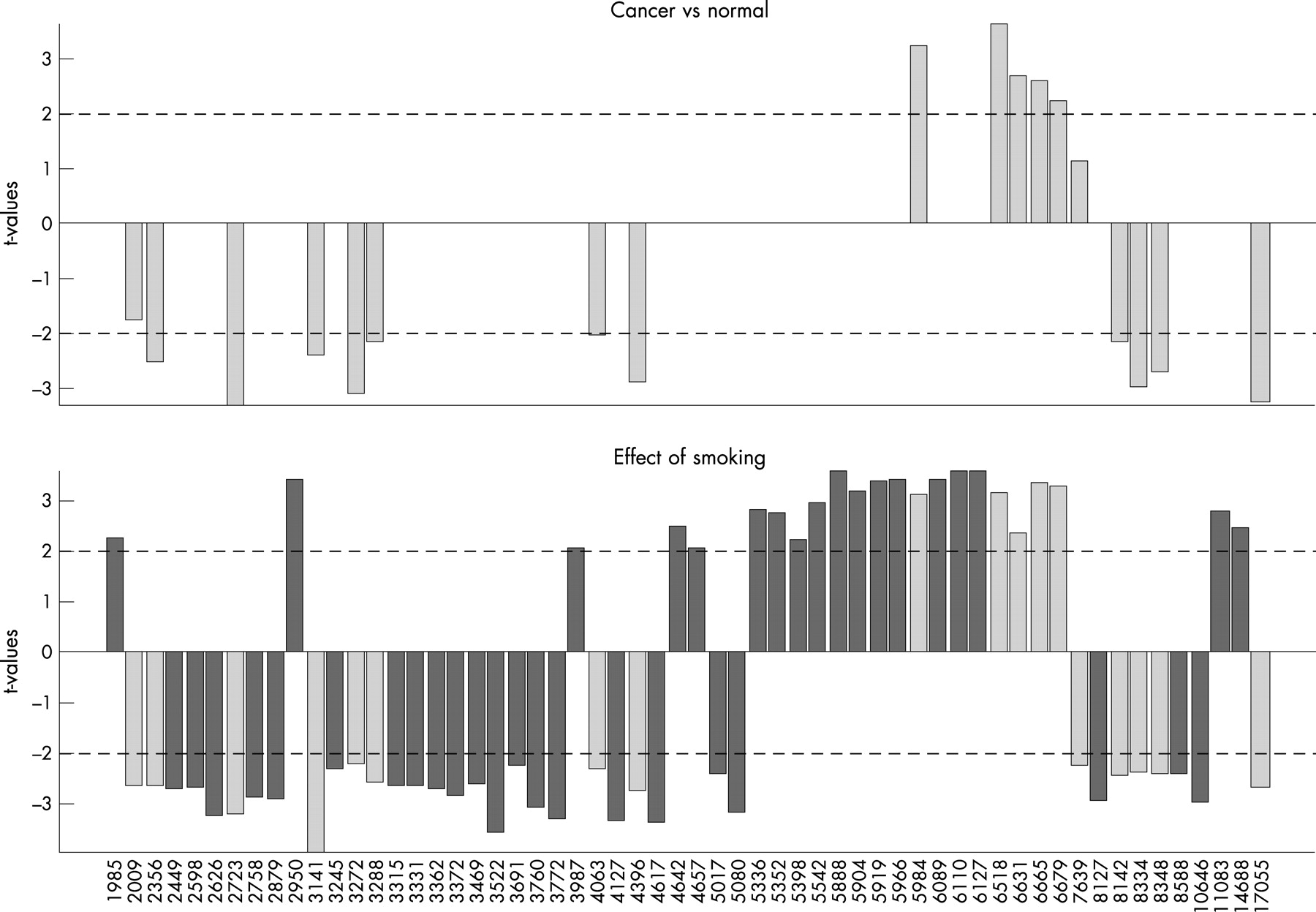
Methods: This analysis was performed as a part of the carcinoma of the lung biomarker (CLuB) Study, a prospective observational study with LREC, R&D Approval and NCRN support. The target group were patients undergoing surgery for lung cancer and the controls were from matched non-cancer subjects. Serum samples were analysed using SELDI-TOF-MS. Peak intensities were extracted from the proteomic profiles and a multiple linear regression model was used to evaluate how smoking, cancer type and stage affects the proteome. The p values from t tests of the significance based on the corresponding parameter estimates were used to identify their associated effects on peak intensities. These changes were further evaluated using two-sample t test.
Results: Between January 2005 -September 2006, 70 patients (66% male, median age 65.5 (SD10.0)) and 75 control subjects (70% male, median age 62.9 (SD 12.5)) were recruited. 131 peaks were detected in the SELDI analysis, of which 40 showed significant differences between cancer patients and controls (p<0.01).The smoking status is in table 1. The histology and stage distribution is shown in tables 2 and 3. There was a correlation between the stage of NSCLC and the intensity of certain peaks in the serum proteomic profiles. The differences between adeno and squamous carcinoma were modest. Smoking also had a clearly detectable influence on the profiles. Some peaks were found to be influenced by cancer alone, some by smoking alone and some by both cancer and smoking.
Conclusions: There was a correlation between the stage of the disease and the intensity of certain peaks in the serum proteomic profiles of patients with NSCLC however the differences between adeno and squamous carcinoma were modest. Smoking also had a clearly detectable influence on the profiles.
QUALITY OF RNA EXTRACTED FROM BIOPSIES OF NON-SMALL CELL LUNG CANCER COLLECTED USING DIFFERENT TECHNIQUES
M. H. Lawson1, D. Rassl2, J. Brenton1, J. Hadfield1, M. Goddard2, N. Screaton2, G. Murphy3, R. C. Rintoul2. 1CRUK Cambridge Research Institute; 2Papworth Hospital NHS Foundation Trust; 3University of Cambridge, UK
Introduction: Analysis of RNA using high throughput methods offers a powerful tool for research. However the gene expression profiles generated by such methods are influenced by the quality of the starting RNA which can be influenced by the collection procedure, storage and method used for extraction as well as the type of tissue. At Papworth prospective banking of lung cancer biopsy specimens for use in future research projects has recently begun. This project aims to compare the quality and yield of RNA extracted using a standard method, from non-small cell lung cancer (NSCLC) biopsy specimens collected by different techniques.
Methods: NSCLC biopsy specimens were collected by fibre-optic bronchoscopy (FOB), endobronchial ultrasound guided biopsy (EBUS) or CT-guided needle biopsy. The specimens were snap frozen in liquid nitrogen and stored at −80°C until analysis. RNA was extracted using an RNeasy Mini kit (Qiagen) according to the manufacturer’s instructions. Yield and quality were assessed using a Nanodrop spectrophotometer and by capillary electrophoresis using an Agilent Bioanalyzer.
Results: Yield and quality of extracted RNA was dependent on both the type of biopsy analysed and the quality of each biopsy. Needle biopsy provided the smallest samples and the least RNA. FOB provided the highest yield of RNA and the best quality RNA. The EBUS samples were the largest but did not yield more RNA than FOB samples.
Discussion: It is accepted that the quality of RNA analysed can significantly influence the results of gene expression analysis. Therefore ensuring uniform RNA quality is important in any investigation of comparative gene expression. We have demonstrated that different methods of biopsy collection for lung cancer specimens can result in differences in the quality of RNA when using a standardised extraction protocol. The tissue disruption and homogenisation step of the extraction may need to be optimised for each biopsy type to improve RNA quality. However much of the RNA degradation may be a result of unavoidable tissue crushing during collection activating RNases. The implication is that the most robust design would ensure uniform RNA quality by matching biopsy types for comparison.
THE ASSOCIATION OF LUNG CANCER AND SINGLE NUCLEOTIDE POLYMORPHISMS IN CODON 178 AND THE FIRST INTRON OF THE DNA REPAIR GENE O6-ALKYLGUANINE-DNA ALKYLTRANSFERASE
P. A. J. Crosbie1, G. Mcgown2, M. Thorncroft2, P. N. S. O’Donnell1, S. Lewis3,K. Harrison3, R. Agius3, M. Santibanez-Koref4, G. Margison2, A. Povey3, P. V. Barber1. 1Wythenshawe Hospital; 2Carcinogenesis Group, Paterson Institute for Cancer Research; 3Centre for Occupational and Environmental Health, University of Manchester; 4Institute of Human Genetics, University of Newcastle, UK
Introduction: Chronic exposure to tobacco smoke is associated with over 90% of lung cancer cases in the UK. Interindividual differences in the ability to repair DNA damage, caused by carcinogens in tobacco smoke, may be a factor in determining the risk of developing lung cancer. One important component of the bodies defence against a subgroup of carcinogens, known as alkylating agents, is the DNA repair protein O6-alkylguanine-DNA alkyltransferase (MGMT). Previous work has shown that two single nucleotide polymorphisms (SNP) are significantly associated with MGMT DNA repair activity: within intron 1 (rs12268840) and in codon K178R (rs2308327). The association with lung cancer risk and these SNPs were investigated using three hospital case control studies.
Methods: Genotyping was undertaken on 617 subjects of whom 255 had lung cancer. All subjects were recruited from the Bronchoscopy Unit, Wythenshawe Hospital over a ten year period. All subjects were aged 40 or older; cases were defined as having an incident diagnosis of lung cancer and controls were cancer free. The majority of the population had a smoking history (89%) and were male (62%). Cases (n = 255) were older (n = 362) (68.9 (10.2) vs 64.4 (10.7) years, p<0.001) and had smoked significantly more than controls (52.4 (32.7) vs 46.6 (33.3) pack-years).
Results: The presence of the 178R allele was associated with a reduced risk of lung cancer in two of the three studies (p<0.05). In a meta-analysis, the odds ratio (95% CI) associated with the 178R allele relative to the 178K allele was 0.64 (0.45 to 0.92; p = 0.01) and 0.51 (0.24 to 1.11; p = 0.09) in fixed effects and random effects models respectively. A pooled analysis, which was adjusted for age, gender, smoking exposure (pack-years) and case-control series, revealed a reduced odds ratio (OR, 95% CI) for codon 178R heterozygotes (0.67, 0.45 to 1.01) and homozygotes (0.10, 0.01 to 0.94): the trend for a decreased risk with the number of R alleles was significant (p = 0.008). This trend was especially significant in subjects with above median smoking exposure (trend test p = 0.003) but not in those with below median exposure (p = 0.73). There was no evidence of an association between the intronic polymorphism and lung cancer risk.
Conclusions: These results provide evidence of a protective effect of the codon 178R allele with respect to lung cancer risk, especially in heavy smokers. This effect may be due to the polymorphism affecting the function of the MGMT protein and/or levels in MGMT activity.
Improving outcomes in smokingcessation
IMPORTANT FACTORS IN SMOKING CESSATION IN OLDER PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE VERSUS CRITICAL LIMB ISCHAEMIA
P. Gleeson1, A. Johnson2. 1Kent & Canterbury Hospital; 2Guy’s & St Thomas’ NHS Foundation Trust, London, UK
Introduction: Smoking cessation is a most important part of management for patients with COPD and peripheral vascular disease (PVD). Little is known about the effectiveness of various smoking cessation interventions in older patients (60 years and above) with these conditions and whether there is any correlation between smoking cessation and diagnosis.
Aim: To assess the effectiveness of smoking cessation interventions in older patients with COPD or critical limb ischaemia; to ascertain if the diagnosis was a factor in giving up smoking and if not, to understand the reasons behind starting and stopping nicotine use.
Patients and Methods: Forty patients admitted to hospital with either an acute exacerbation of COPD (n = 20) or critical leg ischaemia (n = 20) manifested as ischaemic rest pain, ulceration or gangrene with/without amputation were recruited from SE London (St Thomas’ Hospital (STH)) and Kent (Kent & Canterbury Hospital, K&CH). Only those of 60 years of age or older who had stopped smoking before admission were included in the study. Patients were asked a series of 25 questions focussing on demographics, smoking history, reasons for starting smoking and age at starting, reasons for stopping, when and how, and knowledge and attendance (if any) at a smoking cessation clinic. Patients were also asked if they regretted smoking. The questionnaire was a mixture of specific closed questions and broad open questions allowing participants to express their views.
Results: 80% of vascular and 75% of respiratory patients were male and the median age was 70 years. 67.5% had been manual labourers but 27.5% had been in either office or professional employment. 16/40 patients had smoked 16–20 cigarettes per day, one had smoked <5 and four >30 per day. All patients had started smoking before the age of 20 years, two when under 10. All patients gave similar reasons for starting—peer pressure, part of the job, cheap cigarettes, advertising, the War. Most patients had stopped smoking in the last few weeks to 10 years but two had stopped 30 years before. 13/40 patients had stopped within the previous six months. Both vascular and respiratory patients reported stopping because of episodes of shortness of breath and in addition, half of the vascular patients stopped because of fear of immobility due to amputation. Hospitalisation was a potent trigger to quit (the sheer size of STH making it difficult to smoke) while patients at K&CH were afraid they would not be treated if they continued to smoke. Of those who had stopped years before, respiratory symptoms of breathlessness and coughing in public were important in 44% of COPD and 18% of vascular patients. Financial hardship was important for some patients in Kent while family support helped patients in both areas to stop. 60% of all patients had tried to quit more than once. Only 9/40 had tried nicotine patches, three regarding them as key to success. Only three had used other products without success. Most patients had not used anything to help them give up and relied on willpower. Only three had attended a smoking cessation clinic and two found it helpful. 75% of patients were not aware of any smoking cessation clinic in their area. 52.5% of patients regretted smoking but the remainder had no regrets.
Conclusions: Shortness of breath frightened people most and was a strong motivating force to quit, but the threat of amputation along with other medical conditions were also important. Most patients in this age group had not made use of aids to stop smoking and the majority were not aware of smoking cessation clinics. Most relied on willpower to stop. Smoking cessation interventions need to be offered to older smokers both in the primary care setting and also in hospital. Older patients perceive the urgency of stopping smoking and can therefore be highly motivated and receptive to smoking cessation advice and interventions. A period of hospitalisation should be used to encourage and inform elderly patients.
SMOKING CESSATION ADVICE FOR HOSPITAL IN-PATIENTS: ROOM FOR IMPROVEMENT
E. L. Roddy, K. Mortimer, K. Allen, R. Thomas, M. J. Ward, G. M. Cox. Kingsmill Hospital, Nottinghamshire, UK
Introduction: The widely publicised Thorax smoking cessation guidelines state that “all health professionals should give brief advice on smoking cessation” to all patients who smoke, and hospital admission is an ideal opportunity for health professionals, including doctors, to advise patients to give up smoking and provide practical support in the form of nicotine replacement therapy and referral to specialist services.
Methods: We conducted a snapshot survey of all medical, surgical and obstetric/gynaecology inpatients at our medium-sized district general hospital located in a deprived ex-mining area of the East Midlands. The authors visited all medical, surgical and obstetric/gynaecology wards and undertook a short questionnaire with those patients who were willing and able to participate. We asked about smoking status, whether smokers had been advised to quit on this admission and if so by whom, whether they had been offered nicotine replacement therapy and where they obtained their cigarettes. All responses were anonymous.
Results: Many of those questioned were ex-smokers, particularly on cardiac and respiratory wards, although we did not collect specific data on this. Some smokers had been offered NRT which was not then prescribed, and many smokers who had not been advised to quit commented that they felt they should have been, particularly in surgery. Most patients who had been advised to quit had been advised by doctors, and some by specialist nurses.
Conclusion: These “real-life” results show that despite guidelines, and the wide availability of nicotine replacement therapy, many smokers especially in non-medical specialties are still not being given adequate help and support to quit during inpatient attendances. They also show that smuggled cigarettes remain widely available, which may be related to the deprived area that the hospital is situated in. More work needs to be done to educate health professionals from all specialties to advise and assist patients to quit smoking in hospital.
A QUESTIONNAIRE SURVEY ON SMOKING POLICY AND SMOKING CESSATION TOOLS IN UK SECONDARY SCHOOLS
J. T. Samuel1, K. E. Lewis1, L. G. Mcalpine2. 1Basildon University Hospital, Essex, UK; 2Monklands Hospital, Airdrie, UK
Introduction: 70–80% of smokers start when they are of school age. Smoking cessation (SC) is part of health education in schools but its delivery and implementation is variable. On behalf of the British Thoracic Society (BTS) Tobacco Committee (TC), we surveyed schools across the UK regarding their policies on smoking and what services/teaching they employ.
Methods: A cross-sectional survey of secondary schools local to members of the TC between October and December 2006. Following initial telephone contact, anonymous self-addressed questionanaires were posted to the lead for Professional, Social and Health Education in each school.
Results: Sixty questionnaires were sent out and 49 replies were received (response rate of 82%). All responders said they had a complete smoking ban for students in the school premises. 88% had a policy for staff smokers. 61% reported policy breach by students and 16% by staff. 82% reported time specifically dedicated to SC in the curriculum. 37% reported that staff were not comfortable with their level of knowledge of tobacco smoking and SC and only 41% had access to any training in SC education. Although 47% said their available education tools were of a high standard, only 27% reported they had the appropriate skills to motivate and assist pupils who smoke to quit. 92% of schools felt that the BTS could help them educate on the effects of smoking on health and deliver SC advice.
Conclusion: Individual school policies on smoking do exist but are frequently breached, mainly by pupils but also by staff. A significant proportion of responding schools did not feel comfortable with their levels of knowledge and skills with less than half saying they had access to appropriate training. Three in four responders felt they did not have the skills to assist pupils who smoke to quit. Help from the BTS was welcome by most schools. Utilising the expertise of members of the newly formed British Association of Stop Smoking Practitioners (BASSP) in secondary schools perhaps concentrating on staff education and confidence building is being considered.
EARLY EXPERIENCE WITH VARENICLINE IN A HOSPITAL-BASED SMOKING CESSATION CLINIC
J. Ryder, R. Angus, L. Davies. Aintree Chest Centre, Liverpool, UK
Background: University Hospital Aintree is a large, teaching hospital in Liverpool. The local adult smoking prevalence is 34%, rising to almost 60% in one of our catchment PCTs. The local SMR for lung cancer is more than 200, and we see 1500 admissions annually with COPD exacerbations.
Methods: In 2001, a hospital-based smoking cessation clinic was established. Specialists see in-patients, out-patients and staff, and the intervention consists of initial assessment, pharmacological support and intensive counselling. In January 2007, varenicline was added to the hospital formulary. According to our protocol, smokers were initially offered NRT to aid their quit attempt. If they had used NRT in the past, or the quit attempt failed, varenicline or bupropion was offered.
Results: From January to June 2007, 463 new referrals (72% female) were seen. 74 (16%) were prescribed varenicline. Mean (SD) age 55 (10.6) years, 59 (80%) female. Fourteen smokers were staff members, 60 were patients with an underlying respiratory diagnosis. Only one patient was thought suitable for varenicline by the specialist but was refused on medical grounds. Varenicline was prescribed for mean (SD) 8.3 (5.8) weeks. 37 (50%) reported side effects (see table). There was no difference in side-effects between women and men. Twelve (16%) discontinued the medication due to nausea and/or vomiting within the first 4 weeks. A further five patients discontinued through choice. 52/74 (72%) had sustained quit attempts at 4 weeks compared with 98/160 (61%; χ2 NS) smokers using NRT in the same period.
Conclusion: Varenicline is acceptable to and well tolerated by smokers attending a hospital based smoking cessation clinic. The drug is suitable for most hospital patients. As this is a report of clinical practice, rather than a randomised controlled trial, many of the reported side effects could be due to nicotine withdrawal. However, in keeping with previous studies of “healthy smokers”, nausea was a common problem. In our clinic, approximately 1:6 stopped the drug due to nausea and/or vomiting. It remains to be seen how well sustained these quit attempts will be at 6 and 12 months, but our early experience is certainly encouraging.
ACHIEVING A SMOKE-FREE SITE IN A DISTRICT GENERAL HOSPITAL: A SURVEY OF PERCEPTIONS OF HEALTHCARE WORKERS
M. D. Shipley, R. Allcock. Gateshead Health NHS Trust, UK
Background: In December 2006 all UK NHS trusts introduced smoke-free regulations prohibiting smoking on all NHS sites. These rules are to be implemented by all NHS trust staff. We have investigated barriers to the implementation and enforcement of these regulations.
Methods: Study participants were 85 medical and nursing staff working in acute medicine at the Queen Elizabeth Hospital, Gateshead. They completed a questionnaire reporting their behaviour when exposed to smokers on NHS hospital sites.
Results: Over 50% of medical and nursing staff reported that they would not challenge patients, staff or visitors smoking on NHS trust sites. Employees appeared more likely to challenge patients than visitors, and were more likely to challenge visitors than other staff. Fear of aggression was the most commonly reported reason for not challenging smokers.

Conclusions: This study has highlighted perceived barriers to the implementation of a smoke free NHS in a district general hospital medical unit. Most medical and nursing staff do not enforce NHS policy. Most medical and nursing staff would not challenge patients, staff, and visitors to stop smoking on a hospital site. There are perceived barriers to the implementation of NHS smoke free regulation by medical and nursing staff working in medical units at District General Hospitals in the North East of England. Many staff report non-compliance with NHS and local policies for enforcement of smoke free hospitals. There is scope to improve this through training in NHS policy and how to avoid aggression.
ATTITUDES OF CURRENT AND EX-SMOKERS TO THE BANNING OF SMOKING IN PUBLIC AND ENCLOSED SPACES IN ENGLAND
H. Burhan, J. Ryder, K. Dowd, S. Haworth, B. Brockway, L. Davies. Aintree Chest Centre, University Hospital Aintree, Liverpool, UK
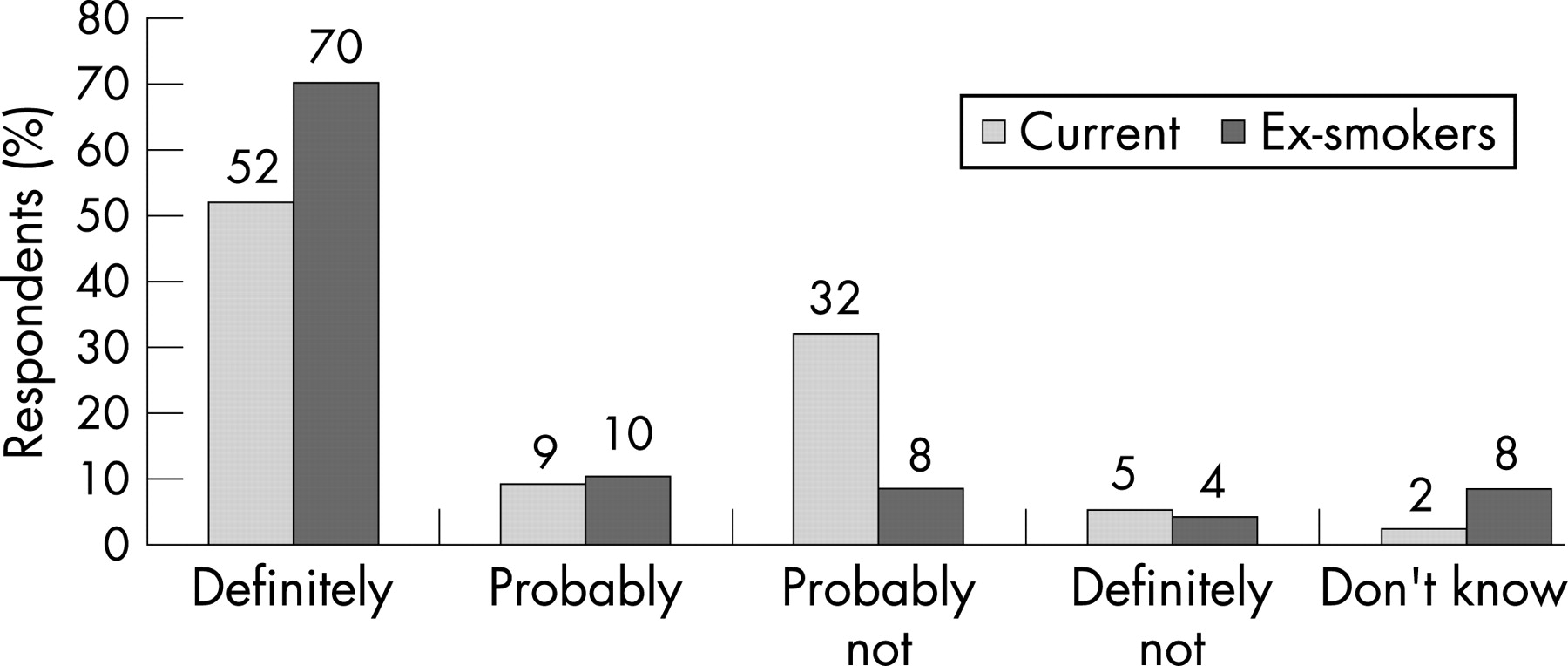
Introduction: Patients attending Smoking Cessation Clinics often attend with partners or supporters who themselves may be current or ex-smokers. Are there differences between these two groups in attitudes towards the ban on smoking in enclosed public spaces and workplaces in England? We assessed awareness of the ban in the six weeks prior to its implementation in 71 Smoking Cessation Clinic attenders to see whether current smokers, and accompanying ex-smokers differed in their perceptions of the value of the ban.
Results: See table. All respondents were aware of the smoking ban prior to the legislation being enacted. The most frequently cited reasons for quitting in ex-smokers were ill health or hospital admission (55.5%), cost (18.6%), and family pressure (11.1%). Most current smokers (61.4%) had made 2–5 attempts to quit previously; 20.4% of ex-smokers claimed to have quit at their first attempt. There was a statistically significant difference between current and ex smokers’ responses (p<0.05); student t test. No significant differences were observed between smokers and ex-smokers in response to the question “Do you think the ban on smoking in enclosed and public spaces would help you quit?” (p = 0.44). Ex-smokers were significantly more likely to be bothered by a smoky atmosphere in a pub, club or bar than smokers (20 (74.1%) vs 17 (38.6%), p = 0.004); this difference was less significant when asked regarding smoky restaurants or cafes (23 (52.3%) vs 21 (77.8%), p = 0.06). Current smokers were significantly more likely to disagree with the comment “the smoking ban will make me more likely to eat out” (p = 0.01).

Conclusions: All those surveyed were aware of the imminent smoking ban. Both smokers and ex-smokers felt that the ban would be helpful in giving up smoking. Despite this there were statistically significant differences in opinion as to whether the ban was a good idea. Current smokers were less bothered by smoky environments than ex-smokers, and did not feel the ban would encourage them to eat out more frequently.
Pulmonary circulation: assessmentand treatment
BOSENTAN FOR INOPERABLE CHRONIC THROMBOEMBOLIC PULMONARY HYPERTENSION: A RANDOMISED, PLACEBO-CONTROLLED TRIAL—BENEFIT
J. Pepke-Zaba1, E. Mayer5, G. Simmoneau7, L. J. Rubin6, I. Lang4,M. M. Hoeper3, H. A. Ghofrani2. 1Papworth Hospital, Cambridge, UK; 2University Hospital, Giessen, Germany; 3University of Hanover Medical School; 4Medical University of Vienna, Austria; 5Johannes Gutenberg University Medical School, Mainz, Germany; 6University of California, USA; 7Antoine Beclere Hospital, Clamart, France
Background: Chronic thromboembolic pulmonary hypertension (CTEPH) is a life-threatening condition, characterized by obstruction of the pulmonary vascular bed causing increased pulmonary vascular resistance (PVR) and progressive pulmonary hypertension (PH). The treatment of choice is pulmonary endarterectomy (PEA), and is potentially curative. However, up to 50% of patients referred for surgery are not eligible. Additionally, 10–15% of patients experience post-operative persistent or recurrent PH. Since arteriopathy in CTEPH shares pathology with pulmonary vascular changes in pulmonary arterial hypertension (PAH), the efficacy and safety of the dual endothelin receptor antagonist, bosentan, has been evaluated in patients with inoperable CTEPH or with persistent or recurrent postoperative H.
Methods: BENEFiT is the first multicentre, prospective, double-blind, placebo-controlled study of medical treatment for inoperable CTEPH or PH after PEA. Patients were randomised to receive bosentan or placebo for 16 weeks (62.5 mg twice daily increasing to 125 mg twice daily after 4 weeks). Independent co-primary endpoints: percentage change from baseline in PVR at rest at week 16 OR change from baseline to week 16 in 6MWD. Other endpoints included: change from baseline to week 16 in WHO functional class (FC), haemodynamics, time to clinical worsening, SVO2, change from baseline in NT-pro-BNP and Borg dyspnea index.
Results: 157 patients were randomised to bosentan or placebo. The PVR analysis set excluded 20 patients (9 placebo, 11 bosentan) and the 6MWD analysis 17 patients (7 placebo, 10 bosentan) because they were considered “operable” post-randomisation or due to a missing baseline or post-baseline assessment. Co-primary endpoints: change in PVR from baseline to week 16 was +30 dyn×sec/cm5 in the placebo group compared to −146 dyn×sec/cm5 in the bosentan group, a significant treatment effect of 24.1% (95% CI −31.5 to −16.0; p<0.0001) (fig). No treatment effect was observed on 6MWD at 16 weeks, which increased in the placebo group by 0.8 m compared to 2.9 m in the bosentan group. Other endpoints are shown in table 1. Safety results were consistent with the established safety profile for bosentan from other trials.
Conclusions: These results suggest that bosentan improves haemodynamics in patients with inoperable CTEPH or with persistent or recurrent PH after PEA.
PULMONARY ARTERY OCCLUSION PRESSURE ANALYSIS IN CHRONIC THROMBOEMBOLIC AND IDIOPATHIC PULMONARY HYPERTENSION
M. Toshner1, J. Suntharalingam2, E. Soon1, K. K. Sheares1, P. White1, R. Hughes2, P. Fesler3, R. Naeije4, J. Pepke-Zaba1. 1Papworth Hospital, Cambridge, UK; 2Royal United Hospital, Bath, UK; 3Montpelier University Hospital, France; 4Erasme University Hospital, Brussels, Belgium
Introduction: Pulmonary artery occlusion pressure (PAOP) waveform analysis is emerging as a useful tool for partitioning pulmonary vascular resistance. Previous work in chronic thrombo-embolic pulmonary hypertension (CTEPH) has suggested that it can identify patients at high risk of operative mortality and residual distal disease. The selection of patients suitable for pulmonary endarterectomy (PEA) is critical given that small vessel disease and arteriopathy account for over one third of operative deaths. To determine if PAOP analysis could discern between predominantly proximal and distal disease we examined patients with operable proximal CTEPH, inoperable distal CTEPH, and idiopathic pulmonary arterial hypertension (IPAH) including connective tissue associated PAH where the vascular obstruction is distal in nature.
Methods: All subjects were diagnosed using standard Venice classification criteria and assessed by the surgical team. PAOP were performed at right heart catheter and analysis of waveforms were undertaken blinded using a computer model as previously described and expressed as an upstream % (Rup). Statistical analysis between groups was by ANOVA.
Results: Of 35 patients recruited 14 were proximal operable CTEPH, 7 distal inoperable CTEPH and 13 IPAH/CTD. Mean Rup was significantly higher in operable, mean 86% (SD 7.6), versus inoperable disease mean 69.9% SD (8.7) p = 0.001. Postoperatively two patients died. These two patients were the lowest flow directed Rups in the operative group. IPAH mean Rup 77% (SD 8.6) was also significantly lower than proximal isease p = 0.008.

Conclusions: PAOP analysis continues to show potential for discriminating between surgically operable predominantly proximal and inoperable distally distributed disease and we confirm the observation that a low Rup is a risk factor for mortality post PEA. In IPAH as hypothesised the Rup was lower than proximal disease but not with sufficient sensitivity to distinguish between the two groups.
A RANDOMISED CONTROLLED TRIAL TO INVESTIGATE THE EFFECTS OF A PHYSIOTHERAPIST-LED REHABILITATION PROGRAMME ON EXERCISE CAPACITY AND QUALITY OF LIFE MEASURES IN PATIENTS WITH PULMONARY HYPERTENSION
A. Wilkinson1, C. A. Elliot2, S. Mawson1, I. Armstrong2, C. Billings2, D. G. Kiely2. 1Department of Physiotherapy, Royal Hallamshire Hospital; 2Sheffield Pulmonary Vascular Disease Unit, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Pulmonary rehabilitation has been demonstrated to be an effective intervention in a number of cardiopulmonary diseases. In pulmonary hypertension a recent study has demonstrated an improvement in exercise capacity following a period of intensive in-patient rehabilitation.
Methods: In a randomised-controlled trial we examined the effects of an out-patient based physiotherapist led rehabilitation programme. 40 patients with pulmonary hypertension were recruited. All patients had been stable for at least six weeks. Patients were excluded if on continuous oxygen, in NYHA Class IV, or with severe mobility or balance problems. Patients were randomised into two groups; control group receiving standard best practice and a rehabilitation group receiving best practice plus a physiotherapist-led rehabilitation programme. Patients were seen by the physiotherapist in a single one to one class and given a prescribed set of exercises tailored to the individual needs of the patient. The patient was followed up with telephone support during the 3-month period and the patient was encouraged to continue with their regular exercise regime. Blind assessment was undertaken pre intervention and following 3 months. Outcome measures included distance walked on incremental shuttle (ISWT) and endurance shuttle (ESWT) and SF-36 and CAMPHOR quality of life questionnaires. Data are presented as mean (standard deviation). Analyses were made using the t test and p<0.05 (two-tailed) was considered significant.
Results: After 3 months there was a statistically significant increase in the ISWT distance in the rehabilitation group compared to baseline 278 (151 versus 255 (141) m, p = 0.028, and a trend towards an improvement in the ESWT 493 (473 m compared to 382 (465) m, p = 0.07. There was no significant difference in the Control group: for the ISWT 261 (132 compared to 262 (142) m at baseline and the ESWT 411 (409 compared to 471 (431) m at baseline. There were no statistically significant differences in quality of life measures.
Conclusions: This pilot study suggests that a physiotherapy-led rehabilitation programme for patients with pulmonary hypertension can be safely performed in the home setting and has the potential to improve exercise capacity through education and controlled exercise and a multicentre trial is planned.
Acknowledgement: This study was supported by a grant from the PHA-UK.
NON-INVASIVE ASSESSMENT OF PULMONARY BLOOD FLOW USING AN INERT GAS REBREATHING DEVICE IN PATIENTS WITH PULMONARY HYPERTENSION
L. E. R. Mclure, A. Brown, A. Peacock, M. K. Johnson. Scottish Pulmonary Vascular Unit, Glasgow, UK
Objective: Cardiac output (CO) is an important prognostic marker in pulmonary hypertension (PHT). A non-invasive measure of CO would be valuable in monitoring disease progression. Inert gas rebreathing using acetylene is a well established method for the non-invasive measurement of pulmonary blood flow (PBF) and has been validated in patients with PHT. Recently a new rebreathing technique (Innocor, Innovision, Denmark) using nitrous oxide analysed by a rapid photoacoustic method has been developed. The device is small, portable and convenient for use during exercise. This technique has been validated for patients with left heart failure. The aim of this study was to investigate the accuracy of this new inert gas rebreathing technique in patients under investigation for PHT.
Methods: Twenty three patients (14 female, 9 male) under assessment at the Scottish Pulmonary Vascular Unit had CO measured by three methods: inert gas rebreathing (Innocor) giving PBF, cardiac magnetic resonance (CMR) imaging giving pulmonary artery flow and thermodilution (TD) during right heart catheterisation (RHC) giving right-sided cardiac output. All the subjects had a provisional diagnosis of PHT by echocardiography. CMR imaging (using cine imaging with steady state free precession and phase contrast velocity encoding sequences) and RHC were performed within 48 h of Innocor measurements. PHT was confirmed in 16 patients (8 idiopathic, 5 chronic thromboembolic, 3 connective tissue disease associated). PBF and CO were expressed as volumes by dividing by heart rate, giving estimates of stroke volume (SV). Agreement between techniques was assessed using Bland-Altman analyis and correlation.
Results: All three methods showed good correlation for stroke volume estimates (Innocor vs CMR, r = 0.91; Innocor vs TD, r = 0.89, CMR vs TD, r = 0.95). Bland-Altman analysis showed that the best agreement was obtained between CMR and TD SV with bias (limits of agreement) of −3.2 ml (−19.4 to +12.9 ml). However, the inert gas rebreathing technique also provided values of reasonable accuracy. Innocor vs MRI SV gave bias (limits of agreement) of −2.5 ml (−23.5 to +18.5 ml) (see fig 1) whereas Innocor vs TD SV gave bias (limits of agreement) of −7.4 ml (−30.9 to +16.2 ml).
Conclusion: Inert gas rebreathing using the Innocor device provides an accurate, non-invasive means of assessment of pulmonary blood flow in patients with suspected PHT.

ISCHAEMIC STROKES AND PULMONARY ARTERIOVENOUS MALFORMATIONS (PAVMS): PAVM EMBOLISATION REDUCES STROKE RISK
C. L. Shovlin1, J. E. Jackson2, E. Kulinskaya1. 1Imperial College and Hammersmith Hospital; 2Hammersmith Hospital, London, UK
Background: Pulmonary arteriovenous malformations (PAVMs) provide a right-to-left (R-L) shunt between the pulmonary arterial and venous circulations. Paradoxical embolic strokes affect high proportions of PAVM patients. Embolisation can be used to treat PAVMs if the condition is recognised, however, until now, no direct evidence for reduction of stroke incidence has been presented.
Methods: A cohort study of 219 consecutive individuals with PAVMs was performed. Six markers of PAVM severity (respiratory symptoms; oxygen saturation; R-L shunt (by radionucleide scan); size of largest feeding artery to PAVMs; presence of small PAVMs; and PAVM multiplicity); 12 patient or HHT-associated variables, and seven neurovascular risk factors (smoking status; hypertension; atrial fibrillation; diabetes mellitus, hypercholesterolaemia; cardiac disease; and migraines) were measured and/or recorded prospectively. To assess constant and time-dependent potential predictive variables for stroke, and rate-reduction by PAVM embolisation, several contiguous time intervals between events (stroke, embolisation and/or last follow-up) were defined per patient. An extension of Cox proportional hazards regression model, Anderson-Gill, suitable for the analysis of recurrent events was fitted with embolisation as a time-dependent covariate using SPLUS 6.
Results: Thirty (13.7%) individuals experienced an ischaemic stroke at median age 50.5 (95% CI 41.5 to 59.5) years. Only 10 (33%) had a pre-existing diagnosis of PAVMs. All had underlying hereditary haemorrhagic telangiectasia but only 12 (40%) were aware of this at the time of their stroke. No strokes occurred following obliteration of all angiographically visible PAVMs. Strokes did occur in some patients in spite of previous embolisation: all had small untreatable PAVMs (feeding artery diameter ⩽2–3 mm) in addition to the PAVMs which had been embolised. Overall, in the strongest model of ischaemic stroke (Wald test p value 4.7×10−5) which analysed 250 pre and post embolisation intervals with 4 degrees of freedom, embolisation at a median age of 45 years significantly reduced the rate of ischaemic stroke (p = 0.028). The Anderson Gill models demonstrated no association of ischaemic stroke with PAVM severity markers or neurovascular risk factors.
Conclusions: Ischaemic strokes occur in undiagnosed patients with PAVMs. Stroke risk can be reduced by PAVM embolisation.
BRAIN-NATRIURETIC PEPTIDE CORRELATES TO ECHOCARDIOGRAPHIC INDICES OF RIGHT VENTRICULAR FUNCTION IN PATIENTS WITH FIBROTIC LUNG DISEASE
T. J. Corte, S. J. Wort, R. Engel, G. Giannakoulas, A. U. Wells. Royal Brompton Hospital, London, UK
Introduction: Pulmonary hypertension (PH) contributes to increased mortality and morbidity in patients with interstitial lung disease (ILD). Non-invasive tools for diagnosis and monitoring of PH in these patients are desirable. Elevated BNP levels are associated with higher mean pulmonary artery pressures (mPAP) on right heart catheter (RHC). Although accuracy of echocardiography in these patients has been questioned, it is more available than RHC. The relation between BNP levels and echocardiographic indices of PH is unknown in ILD patients.
Methods: All patients with ILD referred for BNP levels during 2005–7 were included. (n = 91, 51 male, mean age 64 (16) years). All patients had concurrent pulmonary function, 54 patients had six-minute walk testing (6MWT) and 16 had concurrent RHC. Echocardiography tapes were reviewed by an independent cardiologist blinded to patients’ other results. Relationships between BNP levels and echocardiographic measures PH were studied.
Results: Forty two patients had PH on echocardiography as defined by right ventricular systolic pressure (RVSP) >40 mmHg. Median tricuspid peak gradient (TRPG, n = 70) was 36 mmHg (14 to 129) n = 68, and mean pulmonary acceleration time (PAT, n = 90) 100 (29) ms. Median BNP level was 10 pmol/l (1.4 to 377). Diagnoses included idiopathic pulmonary fibrosis (n = 15), non-specific interstitial pneumonitis (n = 31), sarcoidosis (n = 10), chronic hypersensitivity pneumonitis (n = 10), organising pneumonia (n = 2), histiocytosis X (n = 2), and other ILD (n = 22). Patients had significant functional impairment, DLco 37.8 (16.1)%, 6MWT end SpO2 83 (9)%. BNP levels correlated with the following echocardiographic parameters: TRPG (r = 0.4, p<0.001), PAT (r = −0.33, p<0.01), right atrial pressure (r = 0.3, p<0.01), right atrial area (0.4, p<0.0001), and right ventricular inlet diameter (r = 0.4, p<0.001), but did not correlate with indices denoting left heart function. BNP also correlated with DLco (r = −0.38, p<0.001), DLco/VA (r = −0.33, p<0.01), WHO functional class (r = 0.33, p<0.01) and 6MW distance (r = −0.34, p = 0.01). In the subgroup of patients with RHC, BNP correlated with mPAP (r = 0.56, p = 0.03).
Approaching educational needs inprofessionals and patients
SUCCESSFUL IMPLEMENTATION OF A NEW ACUTE OXYGEN GUIDELINE USING A TARGET DRIVEN OXYGEN SATURATION SYSTEM (THE BASIS OF THE NEW BTS GUIDELINE) WITH OXYGEN CHAMPIONS AND DROP-IN TEACHING
L. Ward, M. Monaghan, D. Flowers, G. Price, A. Patel, G. Hands, A. G. Davison. Southend Hospital, UK
Introduction: The BTS will soon introduce a new guideline for acute oxygen therapy in adults. Oxygen will be prescribed by circling and signing for a target saturation on the drug card (94–98% aged below 70, 92–98% aged 70 and above, 88–92% for COPD). Nurses then administer oxygen using the appropriate delivery devices and flow rate to maintain the target saturation. Southend University Hospital was one of the two pilot sites for this scheme. An audit before the scheme showed that 10% of adult inpatients were given oxygen. 66% of these did not have their saturations checked before starting oxygen. Oxygen was prescribed in only 8% of patients. 93% had oxygen saturation monitored.
Methods and Results: Introducing a new policy involved training all doctors and nurses. There were lectures for all medical staff and ward managers. In addition groups of 8–12 nursing staff were instructed in a ward office using a novel 20 minute drop-in teaching sessions (within their shifts) conducted by two Respiratory CNS (oxygen champions) with sessions three times a day for 2 months. This involved a short PowerPoint presentation and verbal test at the end. A record was kept of all staff attending. After 2 months an average of 40% of the trained ward staff had attended. The new oxygen policy, a clinical oxygen guideline, and a PowerPoint training package for nurses were posted on the Southend University Hospital intranet. There were 3357 hits to these sites in the 5 months after introducing the policy. Six months after the introduction of the new policy a repeat audit showed that oxygen had been prescribed in 87% of those receiving it. Oxygen saturation was monitored in 98% of cases.
Conclusions: An acute oxygen policy based on a target saturation range can be successfully introduced using a high level implementation plan with formal lectures, drop-in nursing teaching and back-up information on the hospital intranet. The drop-in teaching methodology was crucial. Materials (PowerPoint lectures, teaching aids, example oxygen policy, etc) will be available with the new BTS acute oxygen guideline. Medical and nursing oxygen champions are being identified in each Trust and will help introduce the guideline.
TRAINING OF GENERAL PRACTICE NURSES: ARE WE PREPARED FOR THE NATIONAL SERVICE FRAMEWORK FOR COPD?
J. Upton1, H. Madoc Sutton1, A. Sheikh2, S. Walker1, M. Fletcher1. 1Education for Health, Warwick, UK; 2niversity of Edinburgh, Edinburgh, UK
Introduction: Following the new general practitioner contract (1990), it was recognised that practice nurses with specialist training had a key role to play in asthma management (Atkin and Lunt 1996). In 1993 49% of practice nurses ran asthma clinics without medical input, yet 22% of these did not have accredited training (Barnes and Partridge 1994). Here we describe current nurse-led general practice respiratory care, and investigate the level of training nurses have received to support it.
Methods: Questionnaires were sent to lead asthma and COPD nurses at 500 randomly selected UK general practices. Respondents reported their roles and specialist training, and the organisation of respiratory care. In the 1993 survey a “maximum role” was defined as a nurse running an asthma clinic without medical input. In this survey it was revised to mean that the nurse both diagnosed and gave follow-up care without medical input. Training was categorised as being accredited (a diploma or degree level module recognised by a university) or non-accredited.
Results: Response rates were high: 78% for asthma, and 74% for COPD nurses. The number of asthma nurses in a maximum role had increased from 49% in 1993 to 66% in 2006. Of these, 20% still did not have accredited training. In 2006 58% of COPD nurses held a maximum role. Of these nurses with a maximum role, 52% did not have accredited COPD training and 89% did not have accredited spirometry training.
Conclusion: The NSF will come in to force in 2008, yet the proportion of COPD nurses without accredited training is currently far higher than it was for asthma 13 years ago. We must not, in our hurry to deliver more primary based care for COPD, neglect the need for a skilled workforce to undertake the necessary roles. Primary care needs to prepare itself for the NSF now in order to ensure the provision of best possible patient care.
SELF-MANAGEMENT IN BRONCHIECTASIS. AN EXPLORATORY RANDOMISED CONTROLLED TRIAL OF A DISEASE SPECIFIC EXPERT PATIENT PROGRAMME COMPARED TO USUAL CARE IN PATIENTS WITH BRONCHIECTASIS
K. Lavery1, B. O’Neill2, S. Elborn1,3, J. Bradley1,2. 1Regional Respiratory Centre, Belfast Trust, Belfast City Hospital; 2Health and Rehabilitation Sciences Research Institute, University of Ulster; 3Department of Respiratory Medicine, Queen’s University Belfast, UK
Introduction: The NHS has endorsed the expert patient programme, which is a self-management programme designed to help patients manage their long-term condition. Previous research has highlighted from the patients’ perspective elements which could be included in a disease specific component of the expert patient programme for bronchiectasis.
Aim: To investigate the efficacy of a disease specific expert patient programme compared to usual care in patients with bronchiectasis.
Methods: Ethical approval was obtained. Sixty four patients with a diagnosis of bronchiectasis were randomised using concealed allocation to either the intervention (n = 32) or the control (n = 32) group. The intervention group attended a hospital-based programme once a week for eight weeks (two weeks’ disease specific education followed by six weeks expert patient programme) in addition to usual care. The control group received only usual care. The primary outcome measure was the Chronic Disease Self-efficacy Scale (CDSS). Other outcome measures included the Revised Illness Perception Questionnaire (IPQ-R) and the St. Georges Respiratory Questionnaire (SGRQ). Data collection was conducted at baseline and after 8 weeks by an independent blinded assessor.
Data Analysis: The Mann-Whitney test was used to assess between group differences in the change in each of the outcome measures. A p value <0.05 was considered statistically significant.
Results: There was a significant between group difference in change in 8 out of the 10 subscales (no significant difference in obtaining help and communication subscales) of the CDSS. There was no significant between group differences in change in six out of the seven subscales (significant difference in treatment control subscale) of the IPQ-R. The between group difference in change in the total score and three subscales of the SGRQ were small and not significant.
Discussion: This disease specific expert patient programme improved self-efficacy compared to usual care in patients with bronchiectasis. There was minimal effect on illness perception and no effect on quality of life, which is in agreement with other published studies. We will assess if these improvements in self-efficacy translate to improvements in other outcomes e.g. hospitalisation, antibiotic usage at a 6-month follow-up of this study.
A SURVEY OF SPECIALIST REGISTRAR KNOWLEDGE OF RADIATION DOSES FOR VARIOUS RESPIRATORY INVESTIGATIONS
G. T. Kyei1, E. F. Bowen2, C. F. J. Rayner1. 1St George’s NHS Trust; 2Hammersmith Hospitals NHS Trust, London, UK
Introduction: Radiological investigations are carried out in large numbers in the UK—it has been estimated that over eight million chest x rays and nearly 200 000 CT chests are carried out per annum. Doctors must balance the benefits of radiological investigations against risks from radiation exposure and provide patients with sufficient information to allow informed consent. We hypothesised that doctors are unaware of the radiation doses for various respiratory investigations.
Method: A questionnaire with a list of radiation exposures was given to 34 Respiratory Specialist Registrars (SpRs) during a teaching session. They were asked to write the dose of milliSieverts (mSv) next to each exposure. A database was used to analyse the results.
Results: 34/34 questionnaires were returned. The ranges of estimated radiation doses (true dose in brackets) were: Posterior-anterior chest x ray (PA-CXR) 0.2–5000 mSv (0.02 mSv); Frequent-flyer-100 h 10–20000 mSv (0.4 mSv); HRCT-chest-20 mm 10-500 000 mSv (0.48 mSv); Q 1–25000 mSv (0.8 mSv); HRCT-chest-10 mm 10–1 000 000 mSv (0.96 mSv); V/Q 2–50 000 mSv (1.2 mSv); CTPA 40–500 000 mSv (1.6 mSv); UK-yearly-dose 0.02–10 000 mSv (2.6 mSv); CT-chest 10–50 000 mSv (8 mSv). The results were also analysed to ascertain the estimated relative amounts of radiation from different exposures compared to radiation from a PA-CXR. The ranges of estimated relative dose (true relative dose in brackets) were: frequent-flyer-100 h ×0.3–×100 CXR (×20 CXR); HRCT-chest-20 mm ×3–×6000 CXR (×24 CXR); Q ×0.3–×250 CXR (×40 CXR); HRCT-chest-10 mm ×3–×8000 CXR (×48 CXR); V/Q ×1.5–×500 CXR (×60 CXR); CTPA ×2.5–×200 CXR (×80 CXR); UK-yearly-dose ×0.06–×1000 CXR (×130 CXR); CT-chest ×3–×5000 CXR (×400 CXR).


Discussion: This cohort of SpRs demonstrated a lack of knowledge regarding the radiation doses for different radiation exposures. They also failed to accurately identify the correct trend in relative doses for different exposures. Doctors need to be aware of the radiation doses of the investigations that they request, as well as the risks that such doses pose, in order to confidently request investigations in the patient’s best interests. The survey is small but we suspect that it highlights a gap in medical education. Further research is needed to see whether this knowledge gap exists within the wider population of UK doctors. If so, consideration should be given to improving medical education in this area.
WHAT DO PATIENTS WANT TO KNOW ABOUT COPD?
H. Bakere, J. Myers, D. Denn. Royal Cornwall Hospital, UK
Introduction: This study looked at patients participating in an eight-week community-hospital based pulmonary rehabilitation course to see what questions they had about their disease.
Method: During each 8-week pulmonary rehabilitation course, a group of 10–12 patients undertook a structured program of supervised exercise and education. During the sessions participants were encouraged to bring up concerns and issues. Questions were recorded on a flip chart for use at a question and answer session towards the end of the course. We collected the 135 questions asked by 16 groups (160 patients) in the period 2004–6.
Results: Questions fell into 5 areas. The largest numbers of questions concerned treatments (36%) followed by aetiology (29%), symptoms (21%), prognosis (4%), and miscellaneous. The 40 treatment-related questions concerned conventional, alternative and potential future treatments (fig). 33 questions were about aetiology. 40% of these were about smoking and 30% about the relation between COPD and asthma. 23 questions concerned the symptomatology of COPD. Roughly half of these questions concerned specific chest symptoms. The remainder related to more global symptoms such as muscle problems and tiredness.

Discussion: This study provides a snapshot of patients’ self-perceived educational needs during a period of pulmonary rehabilitation. A lot of questions related to treatment. Overall there was more interest in alternative therapy, future developments and possible surgery than commonly prescribed and established treatments. The number of questions asking about an aetiological link with asthma was surprising. Perhaps this suggests a folk belief that all wheezes are asthma. Questions about symptoms were equally split between chest and systemic symptoms. This suggests that COPD is a systemic disease not only from the scientific but also from the patient’s perspective. The relative lack of questions about prognosis might reflect patients shying away from an area that they think is depressing.
Conclusion: Looking at what relatively well-informed patients want to know about COPD can help us assess the effectiveness of our educational interventions, as well as giving us greater insights into this large patient group’s needs, concerns and priorities.
ASTHMA NURSE ADVISOR PROGRAMMES CAN IMPROVE CARE WITHIN A HEALTH COMMUNITY
N. I. O’Kelly, J. A. Smith, P. Gray. Lincolnshire Primary Care Trust, UK
Background: The Elite (East Lincolnshire Inspire Team) nurse advisor programme started in January 2005. The remit of the nurse advisor was to set up sustainable systems of care within practices, by using existing practice staff within a structured change management process. Practices were classified into levels of care based on assessments of their capability to provide asthma care to patients. This abstract reports on the outcomes at the end of the first year of activity (January 2005 to December 2005).
Methods: Thirteen practices were identified as having needs in developing asthma services. Baseline assessments of the systems for asthma care in the practice were performed. A Health Improvement Programme (HIP) was developed in conjunction with the nurse advisor and the respiratory clinicians within the practice. The practice programmes ranged in time from 1–2 sessions per week, over a 3–6 month period. The baseline assessments were repeated at completion of the HIP.
Results:
Better-trained clinicians
28 healthcare professionals received tailored education and training in airways disease.
Better structured care
At end of HIP all practices used standardised clinic templates and developed robust recall systems.
Reduced hospital admissions
Asthma admissions reduced in 6 practices, remained the same in 4 and increased in 3. Overall there was a 34% reduction in asthma admissions in all practices (19 admissions).
Increased achievement in GMS Quality Outcomes Framework (QOF) Data
There was wide variation in attainment of QOF points in asthma across the 13 practices. Despite this there was a noticeable increase in all practices in attainment of QOF points.
Conclusion: All practices involved in the ELITE programme improved in their capability to deliver asthma care. By targeting deficiencies in asthma care in GP practices and providing support in education and improving structures of care the standard of care delivered can be improved. Specifically this approach of delivering strategically focussed support to GP practices may reduce asthma admissions.
Asthma: defining the risks and therisky in children
AN IN-DEPTH STUDY TO DESCRIBE AND UNDERSTAND THE HEALTH EXPERIENCE OF TEENAGERS WITH UNCONTROLLED SEVERE ASTHMA: EXPERIENCES OF MEDICATION AND CONCORDANCE WITH THERAPY
K. Edgecombe1, S. Latter2, G. Roberts1. 1School of Medicine, 2School of Nursing, University of Southampton, UK
Introduction: Current asthma management guidelines aim to control asthma symptoms, prevent exacerbations and normalise lung function to enable people with asthma to lead normal lives. Despite our range of therapies for asthma, a sizable minority of teenagers still experience on-going asthma symptoms that limit their lifestyle and impair their quality of life. This gap between the available therapy and ongoing asthma symptoms is a particular problem in adolescence. Little is known about the health experiences of teenagers with uncontrolled severe asthma.
Aims and Objectives: To understand the experience of living with uncontrolled, severe asthma and to use this understanding to inform our clinical management and maximise the health experiences of these individuals.
Methods: Teenagers aged 11–18 years with uncontrolled severe asthma (ongoing symptoms despite the use of at least 800 μg/day inhaled corticosteroid) were recruited from Southampton University Hospital NHS Trust, St Mary’s Hospital, Portsmouth and St Mary’s Hospital, Newport. Semi-structured interviews were conducted with the teenagers. Teenagers, parents and their paediatricians also completed confidential questionnaires quantifying the severity of their asthma, quality of life and concordance with therapy. A transcription was made from the taped interview. This was analysed using a qualitative thematic approach.
Results: Twenty teenagers were recruited into the study. They were aged 11–18 years (median 14 years), had a median of 10 hospital admissions ever, 30% had had an intensive care admission, 25% were on maintenance prednisolone and their average percent predicted FEV1 (SD) was 89% (14). Four over-arching themes emerged from the data: school; close supportive relationships; healthcare professionals; medication and concordance. This abstract will focus on this last theme. Most teenagers self-administered their medication but most required reminders from their parents. Despite frequent education in clinic, some were did not understand why they were on each of their medication and when they should be used (non-intentional non-concordance) possibly because of frequent alterations. Additionally, many felt that only some of their medications worked but were concerned about adverse effects particularly those such as weight gain that affected their self image. When asked about intentional non-concordance, these factors were mentioned along with simply forgetting, not being bothered or conflict with other activities. In particular, most were not utilising their spacer when using a MDI. Explanations offered were that they could not be bothered or that it took too long to use the spacer device. The above table details how often teenagers reported that they failed to take their prophylactic medication. There was only fair agreement (kappa 0.36, p<0.01) between concordance reported by teenagers and parents; there was no agreement with their paediatricians’ report of their degree of concordance. Conversely, some teenagers were using more medication than prescribed, doubling doses if they were concerned about their asthma. Additionally half the participants lived with a pet that they were known to be sensitised to and 60% lived with a smoker.
Conclusions: Asthma affects every aspect of an adolescent’s life and this should be considered when developing a management plan. Concordance is a major issue but may be improved by understanding the patient’s view of their medications, tailoring devices to individual patients (particularly when prescribing a spacer device), minimising changes to therapy and utilising a written management plan. Although the study focuses on difficult asthma, some of the findings may be transferable to a wider patient group.
Acknowledgements: We would like to thank all the staff at the three sites who helped with the study and teenagers and their families.
WHAT ARE THE FACTORS THAT UNDERLIE PAEDIATRIC ASTHMA?
E. Neville-Smith, S. Price, K. Pike, R. Kurukulaaratchy, H. Arshad, G. Roberts.School of Medicine, University of Southampton, UK
Introduction: Asthma is a complex disease with variable clinical features and clinical course even within the paediatric age range. This may be explained by considering asthma to be a collection of phenotypes that all manifest variable airway obstruction. Classically the pathophysiology of asthma is said to involve airway inflammation, airway hyperreactivity and variable airway obstruction. Other factors may be involved in the pathophysiology of some of the specific asthma phenotypes. In this study we explored the factors underlying the variability expressed by children with asthma within the Isle of White 1989 birth cohort. In doing so we aimed to determine which factors were most important in explaining this variability.
Methods: A whole population birth cohort of 1456 infants was recruited on the Isle of Wight in 1989. Subjects have been reviewed at 1, 2, 4 and 10 years of age. All subjects with doctor-diagnosed asthma and symptoms in the past year were included in the analysis. The 10-year assessment included a detailed questionnaire about their symptoms, triggers and treatment, spirometry using ATS guidelines, skin prick testing to the common aeroallergens (house dust mite, mixed grass pollens, mixed tree pollens, cat, dog, negative and positive control; ALK-Abello, Horsholm, Denmark) and bronchial hyperresponsiveness (expressed as PC20 or inverse of the slope of the methacholine dose response curve). A factor analysis was undertaken using all the variables that were thought to be important in describing subjects’ asthma (firstly, birth weight, gestation, gender and, secondly, at age 10 years, BMI, both parents smoking, any smoke exposure, any pet exposure, furry pet at home, family history of atopy, current eczema, current rhinitis, current food allergy, socioeconomic group, positive skin prick test, percent predicted FEV1, PC20, inverse dose-response slope, log total IgE). Where there were two similar variables, that which maximally explained variance was chosen. The number of factors was chosen with reference to the screeplot. The model was rotated using varimax rotation to maximise the loadings on individual variables in each factor to determine whether there were distinct groupings of variables (Stata version 9).
Results: Data presented as count (%) or mean (standard deviations). Unless otherwise stated, data relates to age 10 years. Data were available for 178 subjects with current doctor-diagnosed asthma at age 10 years. They are described in the table. The final model had four factors and explained almost all the variance. Factor one reflected atopy (SPT, total IgE) and bronchial hyperreactivity (inverse slope)—elements which seem to be interlinked. Factor two reflected birth weight and gestation—possibly a reflection of small airways. Factor three reflected social class and smoking (any exposure)—which are known to be closely linked. Factor four reflected high BMI and female gender—which again are linked. There was minimal correlation between the four factors.
Conclusions: The factor analysis has highlighted four unique factors onto which different asthma related variables are loaded. This emphasises the there are multiple independent elements underlying asthma and that possibly not all are important for each individual child’s disease. This underlines the heterogeneity of childhood asthma. These data can now be utilised as a hypothesis generating exercise to explore whether this group of children with asthma can be divided into distinct asthma phenotypes based upon these elements.
Acknowledgements: We would like to acknowledge the contribution of all those involved in the recruitment and assessments of the cohort and the help of all the children and their families.
ARE YOUNG CHILDREN PRESENTING WITH COUGH IN THE ABSENCE OF WHEEZE AT INCREASED RISK FOR ASTHMA IN LATER CHILDHOOD?
S. W. Turner, L. C. Craig, P. J. Harbour, S. H. Forbes, G. Mcneill, G. Devereux, P. J. Helms, A. Seaton. University of Aberdeen, UK
Introduction: Young children often present to their general practitioner (GP) with respiratory symptoms and some are diagnosed with asthma, including those presenting with cough in the absence of wheeze. The present study tested the hypothesis that young children presenting to their GP with cough in the absence of wheeze were not at increased risk for asthma at five years of age.
Methods: 1924 pregnant women were recruited and their children followed up at 2 and 5 years of age. Attendance at the GP in the previous 12 months for cough and/or wheeze was determined from a questionnaire completed at 2 years of age. Children were categorised as “cough only” (C), “cough and wheeze” (CW), “wheeze only” (W) and “neither cough or wheeze” (N). At 5 years of age, a respiratory questionnaire was completed and a representative proportion had lung function determined.
Results: Questionnaire data were available in 1373 two year olds including 285 (21%) with C, 117 (9%) with CW and 43 (3%) with W. Data at 2 and 5 years of age were available in 1112 children. A history of doctor diagnosed asthma ever by 5 years of age was reported in 17% (39 children) with C, 48% (42 children) with CW, 47% (16 children) with W and 7% (55 children) with N, p<0.001 for trend. At 5 years of age, wheeze in the previous 12 months was reported in 13% (30 children) with C, 44% (38 children) with CW, 47% (13 children) with W and 7% (54 children) with N, p<0.001 for trend. The odds ratio for wheeze in the previous 12 months at 5 years of age in comparison to children with N were as follows: C 2.0 (95% CI 1.2 to 3.2); W 8.1 (95% CI 3.9 to 17.1); CW 10.4 (6.3 to 17.3). The mean (SD) FEV0.5 z scores were −0.12 (1.07) for C, −0.42 (0.96) for CW, −0.14 (1.02) for W and 0.05 (1.0) for N (ANOVA p = 0.014).
Conclusions: Isolated cough may be an early asthmatic symptom in young children however, cough in association with wheeze is a much better predictor of future asthma outcome than cough alone.
DIETARY INTAKE OF FRUIT AND CHILDHOOD ASTHMA
V. Garcia-Larsen, R. B. Newson, J. F. Potts, M. K. Tumilty, S. O. Shaheen.National Heart and Lung Institute, Imperial College, London, UK
Aim: To assess the relation between dietary intake of fruit and juices with asthma in London primary school children, and to replicate previous findings of a beneficial effect of apple intake.
Methods: We carried out a cross-sectional survey of children aged 5–10 in 35 schools in Greenwich, South London. 1436 children responded. A questionnaire answered by the parents was used to ascertain symptoms of asthma and of asthma severity in the last 12 months. We also asked about intakes of fruit and juices over the last 12 months: apples, pears, bananas, citrus fruit, fresh apple juice, apple juice from concentrate, miscellaneous apple juice, fresh orange juice, and orange juice from concentrate. Somers’ D (expressed as difference in proportions (DP)) was used to analyse the adjusted associations between outcomes and exposures after controlling for confounders. The Simes test was used to determine which p values could be regarded as significant after allowing for multiple statistical comparisons.
Results: In adjusted analyses, intake of apples (portions per day) was negatively associated with current asthma (DP −0.04, 95% CI −0.06 to −0.01; p = 0.01) and current wheeze (DP −0.04, 95% CI −0.07 to −0.01; p = 0.01) and with two measures of severity: wheezing attacks (DP −0.04, 95% CI −0.07 to −0.01; p = 0.005) and sleep disturbance due to wheezing (DP −0.03, 95% CI −0.06 to −0.01; p = 0.01). Banana intake (portions per day) was strongly negatively associated with all outcomes. After further adjustment for multiple comparisons, associations with banana intake remained statistically significant: current asthma (DP −0.04; 95% CI −0.07 to −0.02; p = 0.001), current wheeze (DP −0.04, 95% CI −0.07 to −0.02; p = 0.002), sleep disturbance (DP −0.04, 95% CI −0.06 to −0.01; p = 0.002) and asthma medication use (DP −0.05; 95% CI −0.08 to −0.02; p = 0.0002). Separate analyses were carried out excluding those children that avoided fruits because of allergies but this did not change the results.
Conclusion: The strong and consistent beneficial effect of banana intake on asthma symptoms deserves further attention in children. The finding on apples supports earlier reports.
RESULTS OF NURSE-LED HOME VISITS FOR CHILDREN WITH DIFFICULT ASTHMA
M. Bracken1, L. Fleming2, P. Hall1, N. van Stiphout2, C. Bossley1, N. Wilson1, E. Biggart1, A. Bush1. 1Paediatric Respiratory Royal Brompton Hospital; 2Imperial College, London, UK
Background: The management of children with severe asthma requires a systematic, inter-disciplinary approach. Our difficult asthma protocol involves a three-stage assessment. The nurse-led home visit is central to the stage 1 assessment. Only those with no remedial factors found at stage 1 progress to stages 2 (in-patient stay and bronchoscopy) and 3 (assessment of steroid responsiveness).
Aims: To establish the risk factors identified for children referred to the difficult asthma protocol; to determine what intervention strategies can be offered.
Methods: Patients were referred to the protocol within a tertiary paediatric respiratory centre. Following a nurse-led hospital visit a home visit was carried out (Stage 1). This addressed four key areas: psychological and social issues; adherence; smoking; and allergen exposure (pets and house dust mite, HDM).
Results: Forty six children (median age 12, range 5–17 years) were visited. A structured mood questionnaire was carried out during the hospital visit. 56% were subsequently referred to a child psychologist; however 74% of these referrals were made after additional information had been obtained at the time of the home visit. Inhaler techniques were assessed and GP prescription records checked. The availability of prescribed, in-date medications in the home was assessed. Poor adherence was thought to contribute to poor asthma control in 33% of patients. 14 parents admitted to smoking; there was evidence of smoking in the home in 7 cases. 24 children owned pets. 45% and 46% who owned a dog and cat respectively had a positive skin prick test (SPT). Only two households were found to be minimising pet exposure. Of 21 children who were SPT positive for HDM, 7 had no HDM avoidance, and 9 had partial measures. Ultimately, only 25% of those visited at home progressed to stage 2 of the protocol.
Conclusions: Nurse-led home visits can help identify potentially remedial factors for poorly controlled symptoms in children with difficult asthma. A home visit allows specific advice to be given and personalised plans of treatment recommended. It appears to be an effective strategy in the management of apparent therapy resistant asthma.
T-spot test in TB
THE ROLE OF T CELL BASED INTERFERON-γ RELEASE ASSAYS IN THE EVALUATION OF PATIENTS WITH SUSPECTED ACTIVE TUBERCULOSIS
T. S. C. Hinks1, D. P. S. Dosanjh1, J. A. Innes2, J. Deeks3, G. Pasvol4, S. Hackforth2, H. Varia4, X. Q. Liu1, K. Millington1, R. Gunatheesan1, V. Guyot-Revol1, A. Lalvani1. 1Tuberculosis Immunology Group, National Heart and Lung Institute, Imperial College London; 2Birmingham Heartlands Hospital; 3Department of Public Health and Epidemiology, University of Birmingham; 4Department of Infection and Tropical Medicine, Northwick Park Hospital,Harrow, UK
Introduction: Diagnostic evaluation of patients with suspected tuberculosis (TB) is challenging because existing tests lack speed and sensitivity and the role of new rapid blood tests for TB infection is unclear. As Mycobacterium tuberculosis infection is a prerequisite for TB disease, rapid determination of infection status with a test of high sensitivity could enable rapid exclusion of TB where this is clinically suspected.
Methods: We performed a prospective blinded study of 389 consecutive patients with suspected TB presenting to two urban hospitals in the UK. Patients underwent tuberculin skin testing (TST) and the enzyme-linked immunospot assay (ELISpot) incorporating early secretory antigenic target-6, culture filtrate protein-10 (standard assay) and a novel antigen Rv3879c (ELISpotPLUS).
Results: 194 patients had a final diagnosis of active tuberculosis, of which 154 were culture-confirmed. Sensitivity of ELISpotPLUS was 91% (95% CI 85 to 95) for culture-confirmed active TB and 89% (84 to 93) for culture-confirmed and highly-probable cases, significantly higher than the 79% (71 to 86; p = 0.005), and 79% (72 to 85; p = 0.01) sensitivity of TST in the two groups respectively. Corresponding negative likelihood ratios were 0.15 (0.10 to 0.24) and 0.25 (0.19 to 0.35) for ELISpotPLUS and TST respectively. ELISpotPLUS had 4% higher diagnostic sensitivity than standard ELISpot (p = 0.02). Combined sensitivity of ELISpotPLUS and TST in culture-confirmed and highly-probable cases was 99% (95 to 100), conferring a negative likelihood ratio of 0.02 (0 to 0.06) when both test results were negative.
Discussion: In routine hospital practice, ELISpotPLUS has higher diagnostic sensitivity than TST and combined use of these tests enables rapid and reliable exclusion of tuberculosis from the differential diagnosis.
RAPID IMMUNO-DIAGNOSIS OF ACTIVE EXTRAPULMONARY TUBERCULOSIS
R. A. M. Breen, A. Dunleavy, F. Perrin, T. D. Mchugh, S. Gillespie, I. Cropley, M. C. I. Lipman. The Royal Free and University College London Medical School, UK
Introduction: Laboratory tests are often unhelpful during the initial assessment of patients with possible extrapulmonary TB. However in many such cases, there is a strong local host response, suggesting that immune-based tests may be of some value as a rapid diagnostic method. To investigate this hypothesis, we prospectively recruited subjects who were being investigated for possible active pleural or peritoneal TB at our institution.
Method: The percentage of interferon-γ synthetic CD4+ lymphocytes present within either pleural fluid or ascites following overnight (16-h) stimulation with purified protein derivate of M tuberculosis (PPD) was assessed using flow-cytometry. A positive assay was defined as >1.5%. All assays were performed prior to diagnosis or commencement of anti-TB therapy and clinical decisions were made independently of immunological data.
Results: Twenty eight subjects with pleural effusion and 10 with ascites were recruited. Among the pleural cases 11 were diagnosed with TB (8 of 11 culture-confirmed). Of these 0 of 11 (0%) were AFB smear positive. Our PPD assay was positive in 11 of 11 (100%) of individuals diagnosed with TB and negative in 16 of 17 (94%) of individuals not diagnosed with TB. In those with ascites, 4 were diagnosed with TB of whom all were culture-confirmed but none were AFB smear positive. Of these, 4 of 4 (100%) diagnosed with TB had a positive PPD assay and 6 of 6 (0%) not diagnosed with TB had a negative assay. Combining the two groups our assay had a sensitivity of 100% and a specificity of 96% against final diagnosis of TB.
Conclusions: These data suggest that our rapid assay has utility in the diagnosis of pleural and peritoneal TB. Further work should be performed to assess its performance as well as that of commercial interferon-γ release assays in this diagnostically challenging group.
AN ECONOMIC EVALUATION OF THE USE OF INTERFERON γ RELEASE ASSAYS IN THE SCREENING OF CONTACTS AND NEW ENTRANTS FOR LATENT TB
M. Gray1, L. P. Ormerod1,2. 1Royal Blackburn Hospital; 2University of Central Lancs, UK
Background: The NICE 2006 Guidelines recommended the use of IGRA test to assess individuals with inappropriately positive tuberculin tests found through either contact or new entrant screening. Our local PCTs were persuaded to fund IGRA testing as being a cheaper option than unscreened treatment of latent TB infection (LTBI)
Results: In Blackburn from 1 August 2006 to 23 July 2007 all persons with an inappropriately positive Mantoux test were screened using Quantiferon-in-tube Gold (QFT) (Cellestis Ltd). 70 contacts (36 positive; 5 indeterminate; 20 negative) and 30 new entrants (17 positive; 4 indeterminate; 8 negative) were tested. Of the 9 indeterminate results, 7 were technical (in the first month of use, inexperienced lab reception staff refridgerated some samples).
Economic Costs: The cost of performing the QFT test was £35/test. From the NICE economic appraisal, system costs of LTBI treatment with 6H (isoniazid 6 months) was a median of £450 (range 250–800). It is assumed for the purposes of calculation that 3 months of rifampicin (R) and isoniazid (3RH) is equivalent. 100 QFT tests cost £3500. The saving in unnecessary treatment of LTBI for those with negative QFT was 28 × £450 = £12600 (range £7000–22400).
Conclusion: The use of QFT as an IGRA test as per NICE Guidelines was cost-effective with a net saving of £9100 (range £3500–£18,900). The “neutral” point for QFT use in this cohort was an 8% negative QFT rate (test cost £3500; LTBI saving £3600). Colleagues should be able to use these data that the use of IGRA testing is very likely to be more than cost-effective, to help persuade PCTs to fund such testing, where they are reluctant to do so.
TB CONTACT SCREENING IN IMMUNOCOMPROMISED HIV POSITIVE PATIENTS: IS THERE A RELATION BETWEEN T-SPOT TB REACTIVITY AND EXPOSURE TO THE INDEX CASE IN OUTPATIENT CONTACTS?
L. V. Baker1, J. Royal2, R. Enuechie2, C.Mazhude1. 1University Hospital Lewisham; 2Lambeth, Southwark and Lewisham Community TB team, London, UK
Introduction: Tuberculosis contact tracing in the immunocompromised in an outpatient setting is difficult. Evidence-based guidelines are lacking. The Interdepartmental Working Group on Tuberculosis: the control of tuberculosis in the United Kingdom (1998) guidelines recommend screening immunocompromised contacts known to have used the same rooms or areas as the index case on two or more occasions at the same time and immunocompetent contacts accumulating eight or more hours outpatient exposure. NICE guidelines recommend using gamma interferon assays in screening this population. Both the T-spot-TB assay (Oxford Immunotec) and Quantiferon gold (Cellestis) have been reported to identify reactivity proportionate to exposure in immunocompetent individuals, supporting the validity of standard screening approaches. This has not been reviewed in an immunocompromised, HIV positive population.
Methods: We performed contact screening in an HIV outpatient clinic following exposure to infectious pulmonary tuberculosis. We defined immunocompromised as a CD4 count <350, present on two or more occasions during the exposure period. The index was symptomatic for 3–4 months. Contacts were identified within a 5-month exposure period. Contacts with a prior history of tuberculosis were excluded. T-spot-TB testing was performed 6 weeks after the last exposure. Indeterminate or borderline T-spot-TB results were repeated after a further 6 weeks.
Results: 114 contacts fulfilling the screening criteria were identified. 74 attended for screening, 72 underwent T-spot-TB testing. 16 countries of birth were documented, 64% with high endemic TB incidence. Prior tuberculin/T-spot-TB reactivity was not available. 81% had prior BCG vaccination. Attendances in common with the index ranged from 2–10 (median 4). 16 (22%) contacts were reactive on T-spot-TB testing, 1 of whom had active TB. Only 1 was indeterminate after repeat testing. There was no relation between frequency of attendance and the proportion of reactive cases, or to the elispot reactivity to the TB specific antigens, ESAT-6 or CFP10. Strain typing of the M tuberculosis isolates using MIRU typing revealed two different strain types—that is, unrelated to the index.
Conclusions: The T-spot-TB reactivity identified appears unrelated to outpatient exposure and is likely to represent background latent TB infection acquired following exposure in countries of birth with high endemic TB incidence.
T-SPOT-TB REACTIVITY FOLLOWING CHEMOPROPHYLAXIS FOR LATENT TUBERCULOSIS IN HIV POSITIVE PATIENTS
L. V. Baker, R. Enuechie, C. Mazhude. University Hospital Lewisham, London, UK
Introduction: Gamma interferon based assays for diagnosing tuberculosis (TB) infection are reported to measure effector T cell response to the TB specific antigens ESAT-6 and CFP-10. A reactive test reflects ongoing antigen exposure to the effector T cells, ie, current TB infection, rather than previous antigen exposure which is a memory T cell response. Logically, treatment for TB infection, whether active or latent disease, associated with antigen clearance would be expected to result in reversion to a non-reactive effector T cell response. Latent TB has a much lower bacterial and therefore antigen load, antigen clearance following treatment may be more likely.
Methods: We used the T-spot-TB assay in combination with Mantoux testing (10TU) in the assessment of immunocompromised HIV positive contacts (CD4 count <350) following exposure to infectious pulmonary TB. 17 patients were identified with latent TB, all of whom had reactive T-spot-TB tests. Chemoprophylaxis was offered using one of 2 regimens: patients on highly active antiretroviral treatment (HAART) received a 6 month course of isoniazid; those not on HAART were offered 3 months of rifampicin and isoniazid (Rifinah), or 6 months isoniazid. All patients were prescribed supplemental pyridoxine. Compliance was monitored by the TB nurses. Patients were offered a repeat T-spot-TB test post completion of TB chemoprophylaxis.
Results: 15 patients accepted chemoprophylaxis, 3 received Rifinah, 12 received isoniazid. One patient developed a rash on Rifinah but tolerated isoniazid monotherapy. Pretreatment CD4 counts ranged from 220–430, median 326. Corrected antigen-specific T-spot spot counts ranged from 0–152. 9 patients were reactive to both antigens, 3 to ESAT-6 only, 2 to CFP10 only. 2 patients had counts close to the cut off. To date 5 patients (33%) have had follow up T-spot-TB tests. 2 tests were non-reactive, 3 remained reactive (2 of which showed a rise in spot counts, 1 a fall). All patients were compliant. Tests were performed 2-3 months post completion of chemoprophylaxis, 2 patients had received Rifinah, 3 isoniazid.
Conclusion: T-spot-TB reactivity does not necessarily revert following TB chemoprophylaxis in HIV positive patients. This may lack of antigen clearance viable or non-viable organisms, or detection of a mixed memory not pure effector T cell response.
QUANTIFERON-TB OR QFT IN SARCOIDOSIS
A. K. Khan, N. Healy, J. Kieran, M. Cullina, V. Twormey, A. O’Regan. Galway University Hospital, Republic of Ireland
Background: Sarcoidosis is a granulomatous disease of unknown aetiology and variable prognosis. Active disease is associated with suppressed delayed type hypersensitivity-(DTH) to tuberculin skin testing-(TST). Therefore, a diagnosis of latent tuberculosis-(MTB) in the setting of active sarcoidosis is difficult. Immunosuppressive therapy significantly increases the risk of reactivating latent tuberculosis. The introduction of interferon assays such as QuantiFERON-G has provided an additional approach to diagnose latent MTB. No study has assessed the diagnostic yield of these assays in patients with sarcoidosis.
Methods: A study involving 24 patients with sarcoidosis were assessed for a history of MTB or previous exposure, prior BCG vaccination (confirmed with Scar), and prior tuberculin skin testing. 2TU Tuberculin PPD-RT23 SSI skin testing and QFT-G® analyses were performed. Four control subject were used: 2 TST positive (one with active TB, one with latent TB); 2 TST negative.
Results: Of the sarcoidosis cohort 13(53%) were on no treatment, 10(43%) were on prednisolone and one (4%) was on INFLIXIMAB and methotrexate. Twenty-one (87%) patients had prior BCG vaccination. None described recent close contact with MTB. Three (13%) had +ve TST and none had a +ve QFT-G®. All 3 patients had a previously documented negative TST. One patient, a nurse, was on immunosuppressant treatment (Infliximab) and had prior negative TST on at least two occasions. She neither had evidence of prior BCG nor of active tuberculosis. The other two positive TST were stage 1 disease and not on immunosuppressive therapy. Both control patients with positive TST had positive QFT-G® while those with negative TST were also negative on QTF-G®.
Conclusion: Interferon release assays for detecting latent tuberculosis added no clinically relevant information. These results suggest: (1) It is not cost effective to use QTF-G® in assessing patients with sarcoidosis; (2) Mechanistically, it is likely that the DTH immune suppression seen in sarcoidosis occurs at a cellular level rather due to migratory defect; (3) In view of the transient DTH immunosuppression and the risk of reactivating latent MTB in patients requiring corticosteroid or other treatment in sarcoidosis, our study demonstrates the need to perform yearly assessments for latent MTB on this population.
Basic mechanisms in interstitial lungdisease
OXIDATIVE STRESS INCREASES TRANSFORMING GROWTH FACTOR-BETA EXPRESSION AND DRIVES EPITHELIAL TO MESENCHYMAL TRANSITION IN HUMAN LUNG EPITHELIAL CELLS
M. R. Gorowiec, S. M. Parker, L. A. Borthwick, C. Ward, J. Lordan, G. C. Saretzki, P. A. Corris, J. A. Kirby, A. J. Fisher. Applied Immunobiology and Transplantation Research Group, Newcastle University, UK
Introduction: The response of lung epithelium to injury is considered crucial to the pathophysiology of chronic lung diseases including interstitial lung disease (ILD). Change in epithelial cell phenotype to that of a (myo)fibroblast via epithelial to mesenchymal transition (EMT) may contribute to lung remodelling and excessive connective tissue deposition seen in these diseases. As increased oxidative stress is commonly present in these diseases, we hypothesised that this injury source may drive EMT in the lung.
Methods: Lung epithelial cells (A549) were exposed to hydrogen peroxide H2O2 (concentration 50–400 μM) for 1 hour and left for 12 days. Generation of intracellular reactive oxygen species (ROS) was assessed by FACS analysis using DHR and MitoSOX staining. Change in cell morphology was monitored by phase contrast microscopy. Changes in expression of EMT markers were assessed by Western blotting and confocal microscopy. Zymography was used to assess presence of active matrix metalloproteinases (MMPs) in cell supernatants. Transforming growth factor-beta (TGF-β) mRNA level was determined using real-time PCR with GAPDH as endogenous control.
Results: Untreated A549 cells show a uniform epithelial morphology with high level expression of tight junction protein, E-Cadherin, with very low levels of the mesenchymal markers collagen type III and vimentin, and no expression of alpha-SMA. Exposure to H2O2 200 μM and 400 μM caused a marked change in cell morphology typical of EMT. At concentrations of 400 μM cells dramatically increased expression of collagen III (75 fold change), vimentin (5 fold change) and started to express α-SMA. Moreover collagen type III and fibronectin, as components of extracellular matrix in mesenchymal tissue, were secreted to extracellular space in response to H2O2 treatment. E-cadherin expression was almost completely abolished. Both 200 μM and 400 μM H2O2 increased 2 fold activity of MMP-9. Furthermore H2O2 exposure markedly upregulated TGF-β mRNA (2 fold change) after 2 hours post-treatment, which was maintained up to 72 hours suggesting that oxidative stress may stimulate EMT via TGF-β signalling.
Conclusion: Oxidative stress can induce EMT in lung epithelial cells. This may occur due to increased expression of TGF-β and provides a potential mechanism for fibrogenesis in the lung microenvironment.
BALF PROTEIN PERMEABILITY INDEX AND MATRIX METALLOPROTEINASES IN IDIOPATHIC PULMONARY FIBROSIS: A LINK BETWEEN ABERRANT VASCULAR PERMEABILITY AND PROGNOSIS?
S. Mckeown2, A. Richter1, D. Mcauley2, D. R. Thickett1. 1University of Birmingham, UK; 2Queen’s University, Belfast, UK
Aberrant alveolar-capillary permeability will deliver clotting cascade factors to the alveolar space and thus promote the low grade coagulopathy that may drive fibrogenesis. We hypothesised that matrix metalloproteinases (MMP) may determine the degree of increased alveolar-capillary permeability which may relate to severity or outcome in patients with idiopathic pulmonary fibrosis (IPF).
Methods: 22 patients with newly diagnosed IPF underwent bronchoscopy and bronchoalveolar lavage (BAL). MMP-1, -2, -3, -7, -8, -9, -12 and -13 protein in lavage fluid was measured by luminex-based multiplex array. Protein permeability index was calculated from the ratio of BAL fluid protein: plasma protein. Repeat bronchoscopy was performed in 8 patients after 4–6 months of treatment with combination therapy (Pred+ Aza ± NAC).
Results: MMP-2, 3, 7, 8, and 9 were elevated in patients with IPF compared to normal controls (all p<0.01). MMP levels did not reflect the degree of cellular inflammation. MMP-3 (r2 = 0.35, p = 0.004), MMP-7 (r2 = 0.32, p = 0.005), MMP-8 (r2 = 0.42, p = 0.001) and MMP-9 (r2 = 0.53, p = 0.000) correlated with BALF protein permeability index. There were modest negative relationships between lung function parameters and BALF MMP 3 (%FVC r2 = −0.2, p = 0.048) and MMP-7 (% TLco, r2 = −0.29, p = 0.008). Protein permeability index was significantly elevated in those patients who died during the follow-up phase (died median 0.015, versus survived 0.00434, p = 0.04). Similarly BALF levels of MMP-3, MMP-7, MMP-8 and MMP-9 were significantly elevated in those who died. Levels of MMPs remained elevated despite treatment in the patients who underwent repeat bronchoscopy.
Conclusions: Protein permeability index and BALF MMP levels are elevated and relate to outcome in patients with IPF. Current immunosuppressive treatment regimens are ineffective at abrogating these changes. These results suggest that targeting MMP and aberrant alveolar-capillary permeability is worthy of further study in patients with IPF.
LYSOPHOSPHATIDIC ACID INDUCES αVβ6 INTEGRIN MEDIATED TRANSFORMING GROWTH FACTOR-BETA ACTIVATION VIA GαQ IN EPITHELIAL CELLS
M. Xu1, J. Porte1, A. Knox1 D. Sheppard2, G. Jenkins1. 1The University of Nottingham, UK; 2Lung Biology Center, UCSF, California, USA
Introduction: Activation of latent transforming growth factor-beta (TGFβ) by the αvβ6 integrin is a critical step in the pathogenesis of acute lung injury and pulmonary fibrosis. Activation of the seven transmembrane domains G-coupled receptor, PAR1, can enhance αvβ6 integrin mediated-TGFβ activity via RhoA and Rho kinase. Lysophosphatidic acid (LPA) is a lipid mediator released locally during the early stages of wound repair, and is a ligand for the LPA class of G-coupled receptors.
Methods and results: This study investigates the mechanism of LPA induced αvβ6 integrin mediated TGFβ activation. We used a transformed mink lung reporter cell (TMLC) co-culture assay and PAI-1 real-time PCR to measure TGFβ activity. LPA stimulation of normal human bronchial epithelial cells (NHBE) lead to a dose and time dependent increase in TGFβ activity, which was blocked by an αvβ6 and pan TGFβ blocking antibodies. LPA stimulated TGFβ activity in NHBE was inhibited by RhoA inhibitor (C3 exoenzyme) and a Rho kinase inhibitor (H-1152) in a dose dependent manner. To determine the signal transduction pathway from LPA receptor to RhoA we used embryonic fibroblasts derived from Gα12/13-/- and Gαq-/-, or wild-type control mice engineered to express the αvβ6 integrin (MEFβ6). TGFβ activity was measured by co-culture assay and immunoblotting for Smad2 phosphorylation. Stimulation of wild-type MEFβ6 with 10 μM LPA lead to a time dependent increase in Smad2 phosphorylation that was inhibited by an αvβ6 antibody, but not the Gαi inhibitor, pertussis toxin. Gα12/13-/- MEFβ6s had low levels of basal TGFβ activity that could be increased following LPA stimulation, whereas Gαq-/- MEFβ6 had high levels of basal TGFβ activity that could not be further enhanced by LPA stimulation. To confirm the role of Gαq in LPA induced TGFβ activity in epithelial cells, we stimulated NHBE cells in the presence of the Gαq inhibitor GP antagonist-2A resulting in dose-dependent inhibition of TGFβ activity.
Conclusion: These data suggest that LPA induces αvβ6 integrin mediated TGFβ activation via RhoA and Gαq in epithelial cells, and this pathway may play an important role in the pathogenesis of acute lung injury and pulmonary fibrosis.
DIFFERENTIAL MODULATION OF LUNG FIBROBLAST AND ALVEOLAR EPITHELIAL CELL APOPTOSIS BY CYCLO-OXYGENASE (COX)-2 AND PROSTAGLANDIN E2 IS AN IMPORTANT MECHANISM IN THE PATHOGENESIS OF IDIOPATHIC PULMONARY FIBROSIS
T. M. Maher1, S. E. Bottoms1, P. F. Mercer1, C. J. Scotton1, A. Thorley3, A. U. Wells2, A. G. Nicholson2, G. J. Laurent1, T. D. Tetley3, R. C. Chambers1, R. J. Mcanulty1. 1Centre for Respiratory Research, University College London; 2Royal Brompton Hospital; 3National Heart & Lung Institute, Imperial College, London, UK
Introduction: Idiopathic pulmonary fibrosis (IPF) patients have reduced capacity to synthesise cyclo-oxygenase (COX)-2 and the anti-fibrotic mediator Prostaglandin E2 (PGE2). Outside the lung PGE2 protects epithelial cells from, but sensitises fibroblasts to, apoptosis. We hypothesise that reduced COX-2/PGE2 expression in IPF increases alveolar epithelial cell (AEC) apoptosis while rendering fibroblasts resistant to apoptosis.
Methods: Apoptosis in paraffin embedded IPF and normal lung was assessed by TUNEL and immunohistochemical staining for Active Caspase 3 (AC3), Fas Ligand (FasL), FADD and p53. Wild type and heterozygous COX-2 deficient mice received oropharyngeal bleomycin (2 mg/kg) or saline. Apoptosis at day 14 was assessed by TUNEL. Fibrotic primary type II AECs and fibroblasts were obtained from IPF patients undergoing lung transplant and control fibroblasts from patients undergoing lung resection. AECs and fibroblasts were serum starved and treated overnight with either the non-selective COX inhibitor, indomethacin (1 μg/ml), a COX-2 selective inhibitor (NS398, 5μg/ml) or PGE2 (32 ng/ml). Cells were then exposed to FasL (50 ng/ml) for 24 hours, harvested, stained with annexinV/propidium iodide and analysed by flow cytometry.
Results: Only occasional apoptotic cells were observed in normal human lung tissue. TUNEL and AC3 staining of IPF lung demonstrated frequent epithelial apoptosis, but an absence of fibroblast apoptosis. Expression of FasL, FADD and p53 was dramatically upregulated in IPF lung tissue. TUNEL staining showed increased AEC, but decreased fibroblast, apoptosis in COX-2 deficient mice compared to WTs. FasL caused apoptosis of normal fibroblasts (51.5% (mean) ±10.3% (SEM) increase compared to control). COX-2 inhibition with indomethacin and NS398 significantly reduced FasL apoptosis in normal fibroblasts by 35% (p = 0.01) and 23% (p = 0.03), respectively. Fibrotic fibroblasts were resistant to FasL induced apoptosis (8.7%±4.3% increase compared to control). PGE2 rendered fibrotic fibroblasts susceptible to apoptosis (42.3%±15.5%, increase compared to control (p = 0.04)). PGE2 reduced FasL induced apoptosis in primary fibrotic AECs by 18.2% (p = 0.02).
Conclusion: Reduced COX-2 and PGE2 expression has previously been demonstrated to play a role in the pathogenesis of IPF. These results suggest that increased AEC loss due to apoptosis and fibroblast persistence due to resistance to apoptosis are important mechanisms by which reduced COX-2/PGE2 expression leads to pulmonary fibrosis.
SERUM BIOMARKERS IN SYSTEMIC SCLEROSIS-ASSOCIATED PULMONARY FIBROSIS: KL-6 CORRELATES WITH DISEASE SEVERITY
R. K. Hoyles1, H. Sato1, S. R. Desai2, N. S. L. Goh1, F. A. Woodhead1, C. M. Black3, R. M. Du Bois1, C. P. Denton3, A. U. Wells1. 1Interstitial Lung Disease Unit, Royal Brompton Hospital; 2Department of Radiology, Kings CollegeHospital; 3Centre for Rheumatology, Royal Free and University College Medical School, London, UK
Background: A third of patients with systemic sclerosis (SSc) develop clinically significant pulmonary fibrosis (SSc-PF), with an associated 30% 10 year mortality. Alveolar epithelial injury has been implicated in the development of SSc-PF. The serum biomarker Krebs von Lungen factor 6 (KL-6), a mucin-like glycoprotein with increased expression on type II pneumocytes after injury, has been shown in unselected Japanese cohorts to associate with the presence of SSc-PF, and to inversely correlate with lung function. We have examined the associations between KL-6, disease severity, and systemic disease in a large retrospective UK SSc-PF cohort.
Methods: Between 1989–2005, 225 SSc-PF patients were identified with complete clinical data, and stored serum and HRCT at first evaluation. KL-6 analysis was performed by ELISA (donated by Eisai, Tokyo). The extent of SSc-PF on HRCT was determined semi-quantitatively by two blinded radiologists using a well validated scoring system. Clinical data included lung function, autoantibody subgroup including the SSc-specific anti-topoisomerase (ATA), anti-RNA polymerase (ARA) and anti-centromere (ACA), and 99Tm diethylene triamine penta-acetate (DTPA) clearance, the traditional measure of alveolar injury; rapid clearance is associated with progressive SSc-PF.
Results: The extent of fibrosis on HRCT ranged 1–84%, mean 19%. KL-6 concentrations ranged 83–5738, mean 950 U/ml; normal range <500 U/ml. Of 225 patients with SSc-PF, 138 carried SSc-specific autoantibodies: ATA n = 106, ARA n = 20, ACA n = 12. Serum KL-6 was closely linked with HRCT disease extent (r = 0.45, p<0.0001), irrespective of autoantibody subgroup. Inverse correlations between KL-6 and DLco (r = −0.36, p<0.0001) and FVC (r = −0.24, p = 0.0003) were demonstrated. KL-6 inversely correlated with DTPA clearance, (r = −0.38, p<0.0001).
Conclusion: This study provides compelling evidence that serum KL-6 is strongly associated with SSc-PF severity in all autoantibody subgroups, suggesting that alveolar epithelial injury is a unifying pathogenetic mechanism. The use of HRCT scores provides a robust morphological anchor of disease severity, in contrast to lung function alone, which can be affected by other co-morbidities. As a prognostic tool, KL-6 is suitable for serial evaluation. Previous studies have linked disease progression to baseline severity; we propose that epithelial injury may be a driver for disease progression. This will be explored in future studies.
INCREASED SYSTEMIC INFLAMMATORY CYTOKINES IN PATIENTS WITH IDIOPATHIC PULMONARY FIBROSIS
R. Shakespeare1, A. Schwappach1, C. E. Bolton2, G. Dunseath3, D. J. Shale2, B. D. M. Hope-Gill4. 1University of Wales College of Medicine; 2Department of Respiratory Medicine, School of Medicine, Cardiff University; 3Diabetes Research Unit, School of Medicine, Cardiff University; 4Department of Respiratory Medicine, Cardiff and Vale NHS Trust, UK
Background: Idiopathic pulmonary fibrosis (IPF) is characterised by chronic inflammation and fibrosis of the alveolar airspaces and pulmonary interstitium. Median survival is less than three years. In other progressive pulmonary conditions elevated serum levels of interleukin-6 (IL-6), tumour necrosis factor-α (TNF-α) and its soluble receptors (TNF-α srI and TNF-α srII) are associated with altered body composition and a poor prognosis. It is not known whether patients with IPF have raised serum inflammatory cytokines compared with healthy controls.
Methods: 23 patients (18 male), mean age (SD) 72 (11.8) years, with well-characterised IPF were recruited and sub-divided into patients treated with combined corticosteroid/immunosuppressive therapy (4/23) and non-steroid groups (19/23). All patients underwent full pulmonary function testing and had body composition assessed using body mass index (BMI) and bioelectrical impedance for fat free mass (FFM). Serum levels of IL-6, TNFα, TNF-α srI and TNF-α srII were measured using quantitative ELISAs and compared with measurements from 20 age and gender matched historical healthy controls.
Results: Circulating IL-6 (p<0.001) and TNF-α srII (p<0.01) were higher in patients with IPF compared with controls with no difference in serum levels of TNF-α (p = 0.23) and TNF-α srI (p = 0.32). (see table).
Both TNF-α srI (r = −0.425, p<0.05) and TNF-α srII (r = −0.467, p<0.05) in IPF patients were inversely related to six minute walk distance (6MWD). Systemic inflammation was not related to BMI, however, serum TNF-α was inversely related to FFM (r = −0.57, p<0.01). There was no correlation with any lung function variable.
Conclusion: While previous research has revealed evidence of inflammation at a local level within the lung, this study demonstrates the existence of systemic inflammation in IPF with significantly higher serum concentrations of IL-6 and TNF-α srII in patients compared to healthy controls. The negative correlation between the systemic inflammatory mediators, FFM and 6MWD may represent muscle adaptations to the inflammatory load. This requires further review.
Sleep disordered breathing: beyond sleepiness
SLEEP DISORDERED BREATHING, A CAUSATIVE FACTOR IN THE DEVELOPMENT OF SEVERE DIABETIC RETINOPATHY?
S. P. Merritt, J. Moxham, A. Wong, J. Steier, P. Carroll, A. J. Williams. Sleep Disorders Centre, St Thomas’ Hospital, London, UK
Introduction: Sleep disordered breathing (SDB) is common in patients with type 2 diabetes mellitus (T2DM), and both disorders are increasing as the population becomes more obese. Diabetic eye disease is the most common cause of preventable visual loss in people of working age in the UK. Its pathogenesis is not fully understood, however retinal hypoxia is considered to play an important contribution. We hypothesised that SDB is more common in T2DM patients with sight threatening (pre-proliferative and/or proliferative retinopathy) eye disease than those with non-severe retinopathy (background changes or normal).
Method: T2DM patients, diagnosed for more than 5 years, with a BMI of >25.1 kg/m, were randomly recruited using the Diabeta 3® database at our hospital. The subjects were divided into 2 groups depending on the severity of their retinopathy, using digital retinal photographs performed in the 6 months prior to recruitment. Weight, height and blood pressure (BP) were measured. Each patient was instructed on the use of the Minolta 300i® pulse oximeter which was taken home and used that night. The following day blood was taken for HbA1c and the data from the oximeter downloaded. The number of dips in oxygen saturation ⩾4% (ODI 4%) and the percentage of the night spent with oxygen saturations of <90% were used as markers of severity of SDB. Each oximetry trace was also visually examined to determine as to whether the typical “saw tooth” pattern characteristic of obstructive sleep apnoea (OSA) was present. The Mann Whitney U test was used to look for significant differences between the groups with regards to the continuous variables and the χ2 test to look for differences in smoking status.
Results: 44 adults with T2DM participated, mean age 60.5 (9.7). There was no difference, between the groups, in the variables already known to influence the development and progression of diabetic retinopathy, namely HbA1c, duration of known diabetes, BP and smoking. The sight threatening eye disease group had significantly more sleep disordered breathing (mean 4% ODI 13.6 (16.5)) than the non-sight threatening group (mean 4% ODI 3.8 (3.1)), p value 0.03. It was also evident that the sight threatening group spent significantly longer with O2 saturations of less than 90%, 12.6% (19.7) of the night compared to 1.8% (2.6), p value 0.03. From the typical oximetry traces it is thought that much of this SDB is as a result of OSA.
Conclusion: This study suggests that SDB may play an aetiological role in the development and/or progression of diabetic retinopathy. In addition to this extra burden of hypoxia to an already ischaemic retina, the recurrent activation of the sympathetic nervous system and the fluctuating BP that are characteristic of SDB may be additional contributing factors. These results suggest that obese patients with T2DM should be screened for SDB using overnight pulse oximetry, especially if retinopathy is already present.
This research was funded by an unconditional educational grant from ResMed UK.
SLEEP DISORDERED BREATHING IN PATIENTS WITH UNILATERAL PARALYSIS OR SEVERE WEAKNESS OF THE DIAPHRAGM
J. Steier1, C. Jolley1, J. Seymour1, S. Kaul1, K. Ward1, Y. M. Luo2, M. I. Polkey3, J. Moxham1. 1King’s College London; 2Guangzhou Medical College, Guangzhou Institute of Respiratory Diseases, China; 3Royal Brompton Hospital, London, UK
Background: Patients with respiratory muscle weakness can develop sleep disordered breathing (SDB), in particular during rapid-eye-movement (REM) sleep. It has been described that patients with bilateral diaphragm paralysis are at risk of SDB when there is an additional load on the respiratory muscle pump, while patients with hemidiaphragm paralysis or weakness are presumed to seldom develop SDB. We hypothesised that patients with unilateral diaphragm weakness do not develop SDB.
Patients and methods: We studied 36 patients referred with a clinical diagnosis of hemidiaphragm paralysis. After placing balloon catheters to measure oesophageal and gastric pressures, we measured diaphragm strength (sniff and twitch transdiaphragmatic pressures (Pdi)). Twitch Pdi was measured following anterolateral magnetic stimulation of the phrenic nerves. In 16 patients we confirmed unilateral diaphragm paralysis. 10 patients agreed to undergo a polysomnography with measurement of the transoesophageal electromyogram of the diaphragm (EMGdi) and surface EMG of other respiratory muscles (sternocleidomastoid, parasternal intercostals, rectus abdominis). We compared the data to 10 normal, healthy young subjects.
Results: We studied 10 patients (5m, age 56 (10.4), BMI 29.0 (2.7)) with hemidiaphragm paralysis or severe weakness (twitch Pdi 3.2 (1.8) cmH2O). They had a mean (SD) respiratory disturbance index (RDI) of 7.6 (10.5)/h during non-REM sleep, and an RDI of 27.0 (18.4)/h (p = 0.003) during REM sleep (control group 0.2 (0.3) and 0.7 (0.9)/h, respectively). EMGdi (%max) was doubled compared to the control group in NREM sleep (18.1 (8.5) %max) and increased in REM sleep (21.5 (8.9) %max), while the normal subjects had a reduction of EMGdi during REM sleep (8.5 (4.5) and 5.2 (2.8) %max; p<0.001). Accessory muscles (parasternal intercostals) did not show REM-related atonia in the patients. All dimensions of quality of life as measured by the Saint George’s Respiratory Questionnaire and the Chronic Respiratory Disease Questionnaire were reduced compared to controls.
Conclusion: Some patients with unilateral diaphragm weakness are at risk of developing REM-related SDB, in particular when there is an additional load on the respiratory muscle pump like an elevated body mass. Neural drive to their diaphragm is doubled compared to normal subjects, and increases in REM sleep. Accessory respiratory muscles have increased activation to compensate for hypoventilation during sleep. In those with SDB respiratory related symptoms affect the quality of life.

SLEEP DISORDERED BREATHING AND LEFT VENTRICULAR EJECTION FRACTION IN PATIENTS WITH STABLE MODERATE HEART FAILURE, WHO ARE ON OPTIMAL MEDICAL TREATMENT
J. A. Benjamin, C. Wynne-Williams, K. E. Lewis. Prince Phillip Hospital, Swansea, UK
Introduction: Sleep disordered breathing (SDB) is becoming increasingly recognised in heart failure (HF) occurring in 40–80% of patients. Central sleep apnoea and Cheyne–Stokes respiration is particularly associated with a poorer prognosis. Most of these prevalence studies were performed before the introduction of current HF guidelines and particularly the widespread use of β-blockers and spironolactone. We wanted to note the effects of current medical treatment on SDB in HF.
Methods: Following LREC approval, we approached 32 patients attending cardiology and heart failure (of any aetiology) clinics. All had New York Heart Association (NYHA) symptoms grade II–III. All were deemed clinically stable and on appropriate medications, prescribed at maximal tolerated doses by a cardiologist, for at least 3 months.
Exclusions: NYHA stage IV (deemed too unstable and bedbound to attend sleep studies/echos), known sleep apnoea (n = 0), age >80 years, FEV1<50% predicted (n = 0), ejection fraction >50% (or unreliable images, n = 5), cardiac hospital admission within previous 3 months (n = 3), withdrawal (n = 1). Sleepiness was assessed with the Epworth Sleepiness Score (ESS). Total apnoea hyponoea index (AHI) was estimated using a multichannel home sleep study (Stardust® II, Respironics Inc, Monroeville USA). Updated ejection fraction was estimated with transthoracic echocardiogram according to standard guidelines. We had complete data on 23 patients (20 males), mean (SD) age 61.9 (12.7) years, mean BMI 31.8 (5.7) kg/m.
Results: 4 from 23 (17%) had ESS >10. 17 from 23 (74%) patients had an AHI>10 events per hour during sleep. Correlation between AHI and ejection fraction, Spearmans Rho = −0.25, p = 0.25. (R linear = 0.11)
Conclusion: The prevalence of SDB remains high in (mobile) patients with moderate HF, despite being stable and after optimising cardiac medication, using modern prescribing regimes. There is a negative weak correlation between the AHI and ejection fraction, suggesting SDB is more severe with poorer left ventricular function. This was not statistically significant and only accounted for 10% of the variance in AHI, suggesting other factors are also important. The clinical significance of SDB in this group of patients and direction of causality needs to be addressed in interventional trials.
ENDOTHELIAL FUNCTION IN PATIENTS WITH MILD–MODERATE OBSTRUCTIVE SLEEP APNOEA
M. Kohler1, S. Craig1, D. Nicoll1, P. Leeson2, J. R. Stradling1. 1Oxford Centre for Respiratory Medicine; 2Department of Cardiology, John Radcliffe Hospital, Oxford, UK
Background: Flow mediated dilation (FMD) of the brachial artery and augmentation index are methods to assess vascular endothelial function. Both are influenced by vascular risk factors common in patients with obstructive sleep apnoea (OSA). Which of the techniques is better suited to assess endothelial function in large scale randomised controlled trials of continuous positive airways pressure (CPAP) for OSA is controversial.
Study objectives: To investigate if there are relationships between the 2 measures of vascular function in an OSA population, and if they are correlated to well accepted predictors of cardiovascular risk such as blood pressure, or the Framingham index.
Methods: Framingham index was calculated from individual patients risk factors (BMJ 2001;323:75–81). Brachial artery diameter (AD) was measured by ultrasonography at baseline, and during reactive hyperaemia after 5 minutes of forearm ischaemia in order to determine FMD (% increase from baseline). Simultaneously blood pressure was measured and augmentation index was determined by pulse wave analysis (PWA) of the radial pulse. Both these indices are thought to measure aspects of vascular endothelial function and be early markers of cardiovascular risk.
Results: In 45 patients (mean (SD) age, 60.0 (6.8) years, 6 females) with mild to moderate OSA (mean (SD) oxygen desaturation index, 24.1 (16.8)/h), mean (SD) blood pressure was 99.0 (10.4) mm Hg, Framingham index 37.6 (6.2), and mean baseline brachial artery diameter 4.9 (0.7) mm. Forearm ischemia induced FMD was 3.3 (3.3)%, pulse wave analysis could be performed in 42 patients, mean augmentation index was 28.5 (10.4). Framingham-index was positively correlated with baseline AD (r = 0.55, p = 0.00009), and negatively with FMD (r = –0.41, p = 0.005), but not with augmentation index (r = 0.1, p = ns). Mean blood pressure was positively correlated with augmentation index (r = 0.37, p = 0.02) but not with FMD (r = 0.06, p = ns). No correlation was found between FMD and augmentation index (r = 0.13, p = ns).
Conclusion: Measurements of FMD by brachial artery ultrasonography, and augmentation index by PWA, are suitable to assess endothelial function and cardiovascular risk in patients with OSA since they are correlated to the Framingham index and to blood pressure, respectively. FMD and augmentation index seem to reflect different properties of vascular function and therefore both should be measured to evaluate aspects of endothelial function.
SLEEP APNOEA: A MARKER OF VISCERAL OBESITY?
J. Stradling, G. Robinson, D. Smith, B. Langford. Oxford Centre for Respiratory Medicine, Oxford, UK
Introduction: In cross sectional studies, obstructive sleep apnoea (OSA) is associated with a variety of vascular morbidities and mortalities, such as hypertension, insulin resistance, atrial fibrillation (AF), cerebrovascular accidents (CVAs) and myocardial infarctions (MIs). Because obesity, and particularly upper body obesity, cause both OSA and the insulin resistance critical to the metabolic syndrome, it has been difficult to tease out whether OSA might be an independent contributor to these vascular outcomes. In such cross sectional studies, allowance for obesity, or upper body obesity, always lessens the apparent role of OSA, but in many studies it does not abolish it. However, it is always possible that all confounders have not been allowed for. There is a possibility that some confounder associated with OSA could be providing a misleading signal, in the same way vitamin C levels in cross sectional studies led to erroneous conclusions that anti-oxidant therapy might reduce vascular risk. It is possible that OSA might be a better marker of the central obesity causing insulin resistance than conventional indices such as waist/hip or waist/height, which themselves only account for about 30% of the variance in visceral obesity compared to the gold standard of CT measurements. Thus OSA may indirectly be coding for the obesity pattern that causes insulin resistance better than non-invasive estimations of visceral fat do.
Methods: A prospective study of 86 patients with sleep study proven OSA and sufficient daytime symptoms to warrant treatment with continuous positive airways pressure (CPAP) was carried out. A particular >4% SaO2 dip rate and Epworth Sleepiness Score (ESS) were not trial entry criteria, thus providing a spread of disease severity. Measurements were made of insulin resistance (HOMA), OSA severity (>4%SaO2 dips/hour, time below 90% SaO2 and number of pulse rate rises/hr), and obesity indices (waist, height, BMI, W/Hip, W/Ht, neck circumference).
Results: Subjects (86% male) had moderately severe OSA and decreased insulin sensitivity. Sixty-four subjects had satisfactory estimates of insulin sensitivity (HOMA) and were not receiving insulin. The best predictor of insulin sensitivity (and only independent predictor in multiple linear regression incorporating all measurements described in the Methods) was neck circumference, suggesting that this is a better correlate of visceral fat than conventional surface measurements. Neck circumference, waist and weight were also the best predictors of OSA severity.
Conclusion: Thus it is quite possible that OSA codes for upper body obesity in a way that would make it erroneously appear as an independent predictor of vascular risk in cross sectional studies.
Basic mechanisms in COPD
HYPOXIA DECREASES HDAC2 IN U937 CELLS AS A POSSIBLE MECHANISM FOR GLUCOCORTICOID RESISTANCE IN COPD
V. Kumar, C. E. Charron, P. J. Barnes, K. Ito. Airway Disease, NHLI, Imperial College London, UK
Introduction: Chronic obstructive pulmonary disease (COPD) is a major global health burden. The disease is a chronic inflammatory disorder, associated with exposure to cigarette smoke and other noxious stimuli. The pathogenesis of COPD includes destruction of the lung parenchyma, progressive inflammation of the peripheral airways, and goblet cell hyperplasia. Patients with COPD suffer from an accelerated decline in lung function, and the inflammation is largely corticosteroid resistant. Previous studies have demonstrated that impairment of histone deacetylase 2 (HDAC2) in lungs of COPD patients can contribute to the inflammation and corticosteroid resistance seen (Ito K et al, NEJM 352, n19, 1967–76; Ito K. et al. JEM 203, 7–13). Many patients with severe COPD suffer from prolonged exposure to hypoxaemia adding to the morbidity and mortality associated with the condition. However, little is known about the effect of hypoxia on HDAC function and on the inflammation and corticosteroid resistance.
Methods: In this study U937 cells, a human monocytic cell line, were exposed to hypoxia (1% oxygen, 5% carbon dioxide, nitrogen balance) and hypoxia mimic (0.5 mM CoCl2) followed by measurements of HDAC2 mRNA, protein and activity in nuclear extracts. A reduction in total HDAC activity was observed after 20 hours of exposure to hypoxia and 0.5 mM CoCl2 (74±20% and 43.5±12% of normal, p<0.05). Using Western blotting, HDAC 2 expression was decreased under the same treatments within nuclear extracts. This correlated with an increased stabilisation of HIF-1α, confirming that the treatments were leading to a normal hypoxic response.
Results: To examine the effect of hypoxia on inflammation, cells were stimulated overnight with TNF-α after a 24 hour exposure to low oxygen. Hypoxia significantly increased both non-stimulated and TNF-α-stimulated IL-8 secretion (normoxia: 0.2 ± 0.2 pg/ml, TNFα 1005.4±293.4 pg/ml, Hypoxia: baseline, 224±45.2 pg/ml (p<0.05) TNF-α 3909.8±694.7 pg/ml (p<0.05)) as measured by ELISA. Dexamethasone treatment under hypoxia failed to return IL-8 to basal levels. This correlated with lower total HDAC activity in similarly treated cells. The decrease in HDAC2 protein and activity seems to be mediated at the transcriptional level as hypoxia and 0.5 mM CoCl2 decreased the levels of HDAC 2 mRNA, while increasing the levels of VEGF mRNA (a known target of Hif1-α) as measured by RT-QPCR.
Conclusion: We have found that hypoxia causes a reduction in HDAC2 mRNA, protein and total HDAC activity. This is associated with enhanced inflammation and corticosteroid resistance. This is a novel mechanism for HDAC impairment and may provide new targets in the treatment of COPD.
SPUTUM INTERLEUKIN-5 IS ELEVATED IN COPD SUBJECTS WITH EOSINOPHILIC AIRWAY INFLAMMATION AND DECREASES IN RESPONSE TO TREATMENT WITH ORAL CORTICOSTEROIDS
S. K. Saha1, R. Siva1, M. Mccormick2, W. Monteiro1, P. Rugman2, I. D. Pavord1, P. Newbold2, C. E. Brightling1. 1Institute for Lung Health, Leicester, UK; 2AstraZeneca R&D Charnwood, UK
Background: Eosinophilic inflammation is reported in 20–40% of subjects with stable chronic obstructive pulmonary disease (COPD). Eosinophilic inflammation in airways disease including COPD suggests a favourable response to corticosteroid therapy. Interleukin-5 (IL-5) is a cytokine involved in eosinophil expansion, priming, recruitment, and prolonged tissue survival. To date sputum IL-5 has not been reported in COPD and therefore its relation with eosinophilic inflammation within the COPD paradigm is currently unknown.
Methods: Sputum supernatants were identified from subjects with clinically stable COPD who participated in a previous study. Sputum IL-5 was measured using the Meso-Scale Discovery multi-array platform. The assay was validated by measuring % recovery of spiked standard to sputum plugs from subjects with COPD (n = 4) or to PBS and then processed as per sputum. The relation of sputum IL-5 with eosinophilia was assessed by comparing sputum IL-5 concentration in COPD subjects with (n = 19) and without (n = 29) a sputum eosinophilia (>3% non-squamous cells). Within subject repeatability was determined by measuring sputum IL-5 on 2 occasions (n = 20). To assess modulation with corticosteroid therapy, sputum IL-5 was measured before and 1 month after prednisolone 10 mg daily (n = 9).
Results: The mean % recovery of the exogenous spike to COPD sputum samples compared to control was 81%. The mean (SEM) sputum IL-5 concentration was increased in those COPD subjects with a sputum eosinophilia 2.58 (0.71) pg/ml compared to those without a sputum eosinophilia 0.70 (0.19) pg/ml (p<0.005). The sputum IL-5 within subject repeatability was good (mean (SEM) difference 2.20(1.43); r = 0.6, p<0.01). Sputum IL-5 concentration decreased following corticosteroid treatment from 2.94(1.2) to 0.65(0.39) (mean difference 2.30 pg/ml; 95% CI 0.3 to 4.3; p = 0.03).
Conclusion: We have validated the measurement of sputum IL-5 in subjects with COPD. Sputum IL-5 was increased in subjects with COPD with a sputum eosinophilia. The measurement of sputum IL-5 was repeatable and in those COPD subjects with a sputum eosinophilia IL-5 decreased in response to treatment with systemic corticosteroids. Our findings support the view that IL-5 is associated with eosinophilic airway inflammation in COPD and raises the possibility that specific therapies directed at IL-5 may have a role in the treatment of some patients with COPD.
THEOPHYLLINE RESTORES CORTICOSTEROID SENSITIVITY IN COPD CELLS VIA AN INHIBITORY EFFECT ON PI3K SIGNALLING
D. Coutts, Y. To, M. Ito, K. Ito, P. J. Barnes. NHLI, Imperial College, London, UK
Although corticosteroids are the most effective anti-inflammatory agents in asthma, patients with chronic obstructive pulmonary disease (COPD) are corticosteroid-insensitive. Here we showed that low concentrations of theophylline (Theo) restore corticosteroid sensitivity in COPD cells in vitro, via modification of phosphatidylinositol-3 kinase (PI3K) signalling. Peripheral blood mononuclear cells (PBMCs) collected from moderate COPD patients (COPD: n = 20) and healthy volunteers (HV: n = 8) were stimulated with TNF-α (1 ng/ml) for 16 h in the presence or absence of dexamethasone (Dex) (10-12–10-6M) with or without Theo (10-6M, equivalent to 0.18 g/l). IL-8 concentrations in supernatant were determined by ELISA. The inhibitory concentration (IC)50 value of Dex (Dex-IC50: 158±32 nM, p<0.05) in COPD was significantly higher than that of HV cells (41±11 nM), suggesting COPD patients were more corticosteroid-insensitive than HV at cellular level. Treatment with Theo significantly reduced Dex-IC50 value in COPD cells (Dex-IC50: intact, 158±32 nM vs Theo, 76±11 nM, p<0.05). A non-selective PI3K inhibitor, LY294002 (LY, 10-8M) (Dex-IC50: intact, 158±32 nM vs LY, 67±17 nM) also restored corticosteroid sensitivity in COPD cells. There were responders and non-responders for either drug, and % enhancement of IC50-Dex by Theo, which was calculated as the ratio of IC50-Dex versus IC50-Dex with Theo, significantly correlated with that with % enhancement by LY (r = 0.5385, p = 0.047), suggesting that responders to theophylline are nearly identical to the responders to LY. As a surrogate marker of PI3K activation, phosphorylation of the downstream target enzyme Akt (pAkt) was determined by Western blotting and normalised to total Akt protein. Theo completely inhibited H2O2-induced phophorylation of Akt in U937 cells, a human macrophage-like cell line (IC50, 0.68µM) and Theo itself also inhibited activity of immunoprecipitated PI3K-δ isoform directly (IC50 2µM). Furthermore, Theo increased activity of phosphatase and tensin homolog detected on chromosome 10 (PTEN), which antagonises PI3K-dependent cell activation by dephosphorylation of PIP3, a PI3K product. Taken together, modification of PI3K signalling by PI3K inhibition and PTEN activation is the main molecular mechanism of Theo for restoration of corticosteroid sensitivity in COPD.
This work has been supported by GSK, Wellcome Trust and MRC
LIGANDS FOR TLR-3 AND TLR-4 INITIATE DISTINCT CYTOKINE CASCADES IN HUMAN LUNG PARENCHYMAL TISSUE
D. R. Howell, J. A. Warner. University of Southampton, UK
Introduction: Toll-like receptors (TLRs) are known to play a major role in triggering inflammation in infectious exacerbations of chronic obstructive pulmonary disease (COPD) and asthma. Poly I:C is synthetic single stranded RNA that activates TLR-3, mimicking viral infection in the lung. We have examined the inflammatory response from human lung explants following stimulation with poly I:C and have compared this to a known inflammatory stimulus, lipopolysaccharide (LPS), a ligand for TLR-4 activation. We have analysed TNFα, IL-1β, epithelial cell-derived neutrophil-activating protein-78 (CXCL5), macrophage inflammatory protein 1β (CCL4) and IL-8 (CXCL8).
Methods: Human lung tissue (n = 19) was obtained from patients undergoing resection for cancer at Guy’s Hospital London. Tissue fragments taken from the normal margin were stimulated with either buffer control, 100 µg/ml poly I:C or 100 ng/ml LPS. Supernatants were harvested at 1, 2, 4, 6, 24 and 48 hours and the tissue was removed and weighed. Both the tissue and supernatants were stored at −80°C until analysis. Cytokine concentrations in the supernatant were determined using ELISA.
Results: Release of pro-inflammatory cytokines TNFα and IL-1β were significantly elevated in LPS stimulated lung at 4 hours, peaking at 24 hours for TNFα (75.5 pg/mg tissue versus 9.5 pg/mg compared to control tissue, p<0.05) and 48 hours for IL-1β (8.0 pg/mg tissue versus 0.66 pg/mg respectively, p<0.05). Poly I:C, however, had no significant effects on either TNFα or IL-1β production over 48 hours. In contrast, we found that poly I:C was as effective a stimulus as LPS for chemokine production (see table). Both CXCL5 and CXCL8 production significantly increased from 24 hours and continued to rise up to 48 hours for both LPS and poly I:C respectively. The poly I:C response for CCL4 was significant from 24 hours and continued to increase up to 48 hours, though the LPS response peaked and plateaued from 24 hours.
Conclusion: These results demonstrate both LPS and poly I:C significantly increase chemokine production; however, poly I:C fails to stimulate the inflammatory cytokine production of TNFα and IL-1β.
THE CONTRIBUTION OF GROWTH RELATED ONCOGENE ALPHA TO CHEMOTAXIS IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE AND ALPHA 1 ANTITRYPSIN DEFICIENCY
E. Sapey1, D. Bayley2, R. A. Stockley2. 1University of Birmingham; 2University Hospital Birmingham NHS Foundation Trust, UK
Background: Neutrophil recruitment to the airway is thought to be of great importance in the development and progression of chronic obstructive pulmonary disease (COPD). Growth related oncogene alpha (GROα) is raised in sputum from patients with COPD and in vitro studies have shown an enhanced chemotactic response of peripheral blood monocytes to the CXC chemokine. Interleukin 8 and leukotriene B4 each account for approximately 30% of the chemotactic activity of sputum. The chemotactic activity of GROα in sputum has not been assessed.
Methods: The chemotactic activity of sputum from patients with stable COPD, with (n = 11) and without (n = 12) alpha1 antitrypsin deficiency (A1ATD) (PiZ) was assessed using the under agarose assay. The contribution of GROα was assessed using a monoclonal antibody. Levels of GROα were measured in sputum samples.
Results: The mean (SE) contribution of GROα (expressed as % n-formylmethionyl leucylphenlalanine) in COPD with A1ATD was 4.9% (3.4%) and without A1ATD was 9.0% (5.0%). When all the subjects were considered together, the mean (SE) contribution of GROα was 7.2% (SEM 3.04%) (95% CI 0.9 to 13.5, p = 0.027).The median (IQR) GROα concentration was 11.6 nM (4.4–18.5 nM). There was no correlation between GROα concentrations and chemotactic indices.

Conclusion: GROα contributes a small but significant chemotactic effect for neutrophils towards sputum in COPD, but this contribution is much smaller than the reported contribution of interleukin 8 and LTB4.

VARIATION IN THE SURFACTANT PROTEIN B GENE IS ASSOCIATED WITH DEVELOPMENT OF EMPHYSEMA IN ALPHA 1 ANTI-TRYPSIN DEFICIENCY
A. M. Wood, M. J. Simmonds, P. R. Newby, S. C. Gough, R. A. Stockley.University of Birmingham, UK
Introduction: Polymorphisms in a number of genes, including surfactant protein B (SFTPB), have been associated with features of chronic obstructive pulmonary disease (COPD). The only widely accepted genetic risk factor is alpha one antitrypsin deficiency (AATD), which is caused by a number of deficiency alleles, most commonly the PiZ allele. There is considerable variation in the clinical phenotype of patients with AATD, even when comparing subjects with the same AATD genotype. Previous family studies have suggested that there may be additional genetic influences, as yet unknown. We hypothesised that polymorphisms in SFTPB may affect specific clinical phenotypes within AATD patients.
Methods: 424 patients with the PiZZ genotype were selected from the UK National Registry for AATD. All had full phenotypic information and smoking history available. DNA was extracted from whole blood using a modified Nucleon Bacc II kit (Tepnel Life Sciences), quantified using Picogreen® (Molecular Probes Inc). 480 DNA samples from healthy, ethnically matched, control subjects were also selected and prepared similarly. A haplotype tagging method, using information from HapMap to capture all SNPs with r>0.8 and MAF >0.05, resulted in 2 tags (rs2118177 and rs1130866) needed to assess SFTPB. Genotyping for both tags was performed using TaqMa® (Applied Biosystems) genotyping technologies.
Statistical analyses: Comparisons of genotype and allele frequency between controls and AATD subjects with 4 distinct phenotypes—(1) FEV1/FVC <70%, with FEV1 <80% predicted; (2) Emphysema on HRCT; (3) Bronchiectasis on HRCT; (4) Chronic bronchitis—were carried out using χ. Logistic regression allowed comparison of AATD subjects with and without each phenotype, accounting for differences in smoke exposure. Power calculations showed we were powered to detect an allele conferring an odds ratio (OR) of developing airflow obstruction or emphysema of 1.5 relative to controls. Both SNPs were in Hardy Weinberg equilibrium in both cases and controls.
Results: There was a trend towards a difference in rs2118177 genotype (see fig) between patients with emphysema and controls, such that the CC genotype was less common in those with emphysema (p = 0.094), but no different between AATD subjects who did not have emphysema and controls (p = 0.871). The allele frequency analysis was not significant between the groups (p = 0.276).
The CC genotype of rs2118177 was significantly associated with the airflow obstruction phenotype within AATD, showing a protective effect in the AATD regression analysis (p = 0.010). There was a trend towards protection from emphysema, though this did not reach statistical significance (p = 0.099). The odds ratios (OR) of developing airflow obstruction or emphysema in AATD with the CC genotype relative to TT genotype, after regression for smoking, are shown in the table. No other analyses were statistically significant.
Conclusion: Our results support the existence of a genetic influence upon phenotype in AATD within the haplotype block containing rs2118177, and confirm that genes shown to influence usual COPD may have similar effects in AATD. They also suggest a role for SFTPB in the pathogenesis of emphysema. Low levels of this protein have been observed in the lungs of rats with emphysema, but this finding has yet to be confirmed in humans. Replication of our results in an independent patient population would confirm their importance.
Cystic fibrosis treatment responses and consequences
UK CF GENE THERAPY CONSORTIUM TRACKING STUDY: CHANGE IN SPUTUM PROPERTIES IN RESPONSE TO IV ANTIBIOTICS
U. Griesenbach1, S. B. Jeswiet1, M. D. B. Larsen1, Y. Bakar1, N. W. G. Voase1, F. M. Gammie1, K. E. Mullard1, D. M. Geddes1, J. C. Davies1, E. W. F. W. Alton1, C. Marriott2, R. Gray3, A. Horsley3, M. Imrie3, M. Dewar3, A. P. Greening3, A. Innes3. 1Department of Gene Therapy, Imperial College London; UK CF Gene Therapy Consortium; 2Department of Pharmacy, Kings College, London, UK; 3Scottish Adult CF Service, Western General Hospital Edinburgh; UK CF Gene Therapy Consortium, UK
In preparation for our gene therapy clinical trial programme we are currently assessing a number of sputum biomarkers including viscosity, elasticity, total solids, DNA content and 24 hour sputum weight. We tracked and correlated these biomarkers in CF patients (12 years and over) during a course of IV antibiotics (Ab) by collecting samples on several occasions (visit (V)1: at the start of Ab treatment, V2: at the end of Ab treatment (generally after 2 weeks) and interim periods). To ensure adequate reproducibility of the results viscosity/elasticity measurements were carried out in triplicate using a CSL 100 Rheometer which required a comparatively large volume (5 ml) of spontaneously expectorated sputum. Because of this requirement paired samples could only be obtained from approximately 50% of the patients. There was no change in viscosity/elasticity (n = 15) or DNA (n = 18) content when comparing samples at the beginning and end of IV Ab. Sample size calculations indicated that based on data generated here several hundred subjects would be required for these end points to achieve statistical significance in a paired study. In contrast, 24 hour sputum weight was significantly (p<0.05) lower at the end of the Ab treatment (visit 1: 54.67±12.59 g, visit 2: 47.35±20.30 g, n = 19) and there was a trend towards reduction in solid content (visit 1: 5.15±0.68%, visit 2: 4.3±0.48%, n = 18, p = 0.06). Sample size calculations indicated that approximately 50 subjects would have been required to achieve significance in this assay. We also correlated these assays with each other and various assays carried out as part of the tracking study. There were significant correlation between solid content and viscosity/elasticity (r = 0.8, p<0.0001), sputum IL1β (r = 0.52, p<0.0001), sputum IL-8 (r = 0.42, p<0.001) and sputum calprotectin (r = 0.51, p<0.0001). 24 hour sputum weight correlated modestly with % predicted FEV1 (r = −0.37, p<0.05), patient scored symptom severity (r = −0.42, p<0.001) and white blood cell (WBC) (r = 0.33, p<0.016). WBC also correlated with DNA content (r = 0.41, p<0.0001). Sputum elasticity and viscosity correlated with IL1β (r = 0.50, p<0.0001), IL-8 (r = 0.37, p<0.01) and sputum calprotectin (r = 0.54, p<0.0001). Interestingly, 24 hour sputum weight and viscosity/elasticity were correlated with the extent of bronchiectasis as assessed by CT (r = 0.48, p<0.001 and r = 0.32, p<0.03, respectively). Surprisingly, sputum DNA content did not correlate with viscosity/elasticity, despite being generally thought of as a contributor to viscosity, which may in part be related to the assay not being able to discriminate between free and cell-enclosed genomic DNA. In summary, after a course of IV antibiotics which lead to significant subjective and objective (FEV1) improvement the overall quantity of expectorated sputum was significantly reduced but, based on analysis available to date, none of the other parameters (viscosity, elasticity, solid and DNA content) changed significantly, but correlated with other more routinely used assays. Considering the difficulties we encountered in collecting sufficient sputum during this period of an exacerbation and sample size consideration, sputum viscosity/elasticity measurements may not be feasible parameters to measure in a gene therapy trial to which stable patients are likely to be recruited. This study was funded by the CF Trust.
UK CF GENE THERAPY CONSORTIUM TRACKING STUDY: RESPONSE OF CLINICALLY AVAILABLE ASSAYS TO INTRAVENOUS ANTIBIOTICS
J. C. Davies1, N. Voase1, M. Dewar2, K. Mullard1, F. Gammie1, C. Saunders1, A. Horsley2, R. Gray2, K. Macleod3, L. Somerton1, T. Higgins1 , J. Donovan1, N. Cornish1, D. Ashby4, D. Geddes1, A. Greening2, S. Cunningham1, A. Innes2, E. Alton1. 1Imperial College; 2Western General Hospital, Edinburgh, UK; 3Hospital for Sick Children, London, UK; 4Queen Mary, University of London, London, UK
Introduction: In our forthcoming clinical trial of CFTR gene therapy, the UK CF Gene Therapy Consortium will use both established assays and more novel, specifically-designed measures. In this study, we examined the performance of these assays in the context of an infective exacerbation treated with IV antibiotics. This abstract will report the response of established, clinically-available assays; available data from novel assays will be reported separately.
Methods: Children (12 years and above) and adults with CF were recruited from three centres at the time of a clinician-defined infective exacerbation requiring IV antibiotic treatment. A panel of assays was performed at the start and end of treatment, which was most commonly 14 days. Data are presented as mean (SD) or median (range). Clinical assays included spirometry, sputum microbiology, sputum cell count and differential, serum inflammatory markers (CRP, white blood cell (WBC) count,). Patients also completed a symptom score sheet.
Results: Forty patients (mean age 24.2 (7.5) years, 21 male) have paired data available from the start and end of the course of IVs. At baseline, 24 were infected with P aeruginosa, 8 with B cepacia complex organisms and 14 with S aureus (2 MRSA). Significant changes from baseline were observed in FEV1 (53.3 (15.1) to 62.4 (17.5)% predicted; p<0.001), sputum P aeruginosa colony count (log10 CFU 6.3 (0.8) to 5.1 (1.3); p = 0.01), WBC (10.2 (2.5) to 8.7 (3.2)×109/l; p<0.05), CRP (19 (1–249) to 3.5 (1–165) mg/L; p<0.001) and symptom score (–6.2 (4.2) to 2.6 (5.4); p<0.001). In contrast, neither sputum total cell count nor sputum neutrophils changed significantly. There was a significant correlation between change in FEV1 and symptom score (R = 0.4; p<0.05). Although baseline FEV1 correlated significantly with several inflammatory/infective markers (including CRP, WBC, P aeruginosa CFU), changes in none of these parameters correlated with improvement in FEV1.
Conclusion: The clinical response to any novel intervention—for example, CFTR gene therapy—is difficult to predict. Prior testing of experimental assays in a study such as this provides data on the variability of the measurements within the disease population and the degree of change observed with an intervention known to lead to clinical benefit. This should aid the design of rational, powered clinical trials.
COMPUTED TOMOGRAPHY IN INFECTIVE EXACERBATIONS IN CYSTIC FIBROSIS: SERIAL CHANGE AND OBSERVER AGREEMENT
Z. A. Aziz1, A. Wells2, M. Meister3, P. Tyler3, J. Davies4, E. Alton4, A. Innes5, R. Gray5, A. Horsley5, D. Hansell3. 1Department of Radiology, Barts and the London NHS Trust; 2Department of Interstitial Lung Disease, Royal Brompton Hospital; 3Department of Radiology, Royal Brompton Hospital; 4UK CF Gene Therapy Consortium; 5UK CF Gene Therapy Consortium
Introduction: Computed tomography (CT) is a potential outcome measure in clinical intervention trials of patients with cystic fibrosis (CF) lung disease. The ability to reproducibly demonstrate and quantify change are important criteria for the validation of an imaging biomarker. The purpose of this study was to determine whether changes in CT features could be identified in patients with CF following treatment for an infective exacerbation. Secondary objectives were to determine the observer agreement of a semi-quantitative scoring system designed to detect subtle changes in CT features and to compare two methods of scoring serial CTs.
Methods: Thirty-six patients with CF had a CT on admission with an infective exacerbation (CT1) and at 2 weeks following standard treatment (CT2). CTs from the first and second visits were scored randomly by two independent observers blinded to patient identity and timing of the scan. CT features for each lobe were scored using a semi-quantitative graded scoring system for extent and severity of bronchiectasis, bronchial wall thickness, small and large mucus plugging. Air trapping, consolidation and ground glass opacification were scored as a percentage. In a second scoring method, observers evaluated paired CTs as a “side-by-side” comparison. Observers were blinded to the date of the scans and used a graded score (1–5) to indicate whether certain CT features were better, worse or had not changed. Differences between CT1 and CT2 were compared with either parametric or non-parametric analysis as appropriate. Observer variation was assessed using weighted kappa or the single determinant standard deviation.
Results: A significant decrease was seen in wall thickness, small mucus plugs, large mucus plugs and air trapping on the second CT. Interobserver variation for individual CT features was excellent (see table). The “side-by-side” comparisons also demonstrated statistically significant improvement from baseline (CT1) in bronchial wall thickness, small and large mucus plugs, air trapping, consolidation and ground glass opacification. Weighted kappas ranged from 0.68–0.94 (good to excellent).
Conclusion: CT can demonstrate significant morphologic changes over a relatively short time period and in the situation of an infective exacerbation, these correspond with the expected response to treatment. Interobserver variation of both scoring methods was either good or excellent. The relatively simple and quick method of direct comparison is a useful and robust alternative to the scoring of individual CTs in studies involving large numbers of patients.
FUNCTIONAL AND STRUCTURAL CHANGES IN THE CYSTIC FIBROSIS LUNG FOLLOWING ANTIBIOTIC TREATMENT FOR EXACERBATION
A. R. Horsley1, Z. Aziz2, K. A. Macleod3, C. J. Saunders4, M. Meister5, P. Tyler5, M. Dewar1, R. Gray1, N. Voase4, S. Cunningham3, A. P. Greening1, J. C. Davies4, E. W. F. W. Alton4, D. Hansell5, J. A. Innes1. 1Western General Hospital, Edinburgh, UK; 2Department of Radiology, Barts & London NHS Trust; 3Department of Child Life & Health, Royal Hospital for Sick Children; 4Department of Gene Therapy, Royal Brompton Hospital; 5Department of Radiology, Royal Brompton Hospital, London, UK
Introduction: Lung clearance index (LCI), a measure of ventilation heterogeneity, can be calculated from multiple breath washouts. The measurement is thought to be sensitive to small airways dysfunction and is a more sensitive measure of early airway disease in CF than spirometry.
Methods: CF patients presenting with an exacerbation were recruited as part of the UK CF Gene Therapy Consortium “Tracking Study”. Lung HRCT was performed within 24 hours of the start of intravenous antibiotics. CT features for each lobe were scored for seven independent features by two independent blinded observers. LCI was assessed in triplicate by multiple breath washout of 0.2% SF6. Both assessments were repeated at end of treatment.
Results: 29 patients (15 male) completed both LCI and CT assessments. Mean age (range) was 21 (11–40) years, mean FEV1% predicted was 50% at first visit. Mean (SD) LCI improved from 15.2 (2.8) to 14.4 (2.3), p = <0.002. At both pre- and post-treatment visits, CT score for gas trapping showed the strongest correlation with LCI (Spearman r = 0.61 and r = 0.64, respectively, both p<0.001). Weaker correlations were seen for scores for overall extent of bronchiectasis. For FEV1, the strongest correlations were with wall thickness and presence of large mucus plugs. Overall, CT score for gas trapping improved by 11.2%, p = 0.04, n = 28. Change in CT score for gas trapping and change in LCI were not significantly correlated with each other, but the analysis was skewed by a single outlier (p = 0.18, but p = 0.045 after removal of outlier).
Conclusion: LCI can be used to demonstrate changes in lung function after antibiotics. LCI correlates strongly with gas trapping, the CT score component that most specifically reflects small airways function. FEV1, however, is most strongly associated with CT components that reflect large airway function. We have also shown improvement in CT score for gas trapping after antibiotics. Although not statistically significant, there is a trend for this improvement to correlate with improvement in LCI. The results suggest that both LCI and CT scoring may be useful tools in assessing small airways response to novel therapies, such as gene therapy, in patients who are clinically stable.
This work was funded by the Cystic Fibrosis Trust.
A CASE CONTROL STUDY OF ACUTE RENAL FAILURE IN CYSTIC FIBROSIS PATIENTS IN THE UK
A. Smyth1, C. Bertenshaw1, S. Lewis2, I. Choonara1, J. Mcgaw1, A. Watson3. 1Division of Child Health, University of Nottingham; 2Division of Respiratory Medicine, University of Nottingham; 3Department of Paediatrics, Nottingham University Hospitals NHS Trust, UK
Introduction: There has been a recent increase in the number of reported cases of acute renal failure (ARF) in cystic fibrosis (CF). The incidence risk of ARF in CF patients is between 4.6 and 10.5 cases/10 000 CF patients/year. We conducted a case control study to determine which factors which are associated with an increased risk of ARF.
Methods: Our initial survey confirmed 24 cases of ARF in CF patients from 20 UK CF Centres, presenting between 1997 and 2004. Using the UK CF database, we identified sex and age matched controls. Informed consent was sought from the control patients/parents for access to the case notes. Analysis of risk factors was by conditional logistic regression, using STATA (version 9) and Mantel Haenzsel analysis.
Results: There were 24 cases of ARF (12 male, median age 10 years, range 4 months–32 years) and 43 controls (22 male, 9 years, 10 months–32 years). In the group of patients with ARF, 21/24 had received an aminoglycoside at the time of their episode of ARF or in the preceding week, compared with only 3 of the controls for the same time period (p<0.001). In the year prior to the episode of ARF, significantly more cases than controls received gentamicin (19/24 cases vs 1/43 controls, p<0.001). In contrast, the numbers receiving tobramycin were similar (9/24 cases and 15/43 controls). The median lifetime exposure to aminoglycosides among the cases was 11 courses (range 0–72) vs a median of 2 courses (range 0–26) in the control group. The odds ratio for ARF was 1.20 (95% CI 1.04 to 1.38) per aminoglycoside course (p = 0.011). A clear risk factor for ARF (prior renal disease, acute dehydration or long term nephrotoxic drug treatment) was present in 18/24 cases and 8/43 controls (OR 23.52, 95% CI 3.02 to 183.01, p = 0.003).
Conclusion: Cumulative, exposure to aminoglycosides, particularly gentamicin, increases the risk of CF patients developing ARF. Most patients who develop ARF have clear risk factors which indicate the need to withhold aminoglycosides or monitor them more closely.
Supported by UK Cystic Fibrosis Trust Grant PJ465 and an unrestricted educational grant from Forest Laboratories.
Tuberculosis treatment
DO MICRONUTRIENTS USED AS SUPPLEMENTATION TO STANDARD TREATMENT SPEED RESOLUTION OF TUBERCULOSIS?
P. D. O. Davies1, L. Lawson2 , F. Lawson2, I. Olajide2 , L. Cueves1 . 1Cardiothoracic Centre, Liverpool, UK; 2Zankli Clinic, Abuja, Nigeria
Introduction: Several studies have suggested that the addition of zinc and vitamin A to standard treatment may speed the resolution of tuberculosis (TB). This may be of value in resource poor settings when the addition of cheap supplements may reduce the time needed for TB treatment.
Methods: The study was carried out in Abuja, Nigeria. A total of 350 smear positive patients were enrolled in a double blind randomised prospective placebo controlled three arm study. Group A (the placebo arm) received standard 8 months therapy: isoniazid, rifampicin, pyrazinamide and ethambutol for 2 months followed by isoniazid and ethambutol for 6 months. Group B received the same anti-tuberculosis chemotherapy but with zinc supplement in addition; and group C, standard treatment plus zinc plus vitamin A. Assessment of a number of factors, including symptomatology, weight, sputum smear and culture conversion, radiographic improvement and biochemical results, was carried out at the start of treatment, at 2 and 6 months of therapy.
Results: A total of 261 patients completed the study, 91 in group A (35 HIV+ve), 89 in group B (42 HIV +ve) and 81 in group C (30 HIV +ve). Only two factors showed a statistically significant difference between the groups: sputum smear conversion on average took 1 week longer (4 weeks compared with 3 weeks) in the placebo arm compared with the two supplementation arms. Secondly the mortality was greater in the two supplementation arms: one death in group A compared with 9 deaths each in groups B and C. All patients who died during the study were HIV +ve.
Conclusion: This study has shown no overall benefit of giving zinc and vitamin A supplements to patients receiving treatment for tuberculosis. In fact possible harm may have resulted as seen by the increased mortality. This may have resulted from an immune reconstitution effect caused by immunological boosting by the micronutrients. Supplementation with these micronutrients cannot be recommended on the basis if this study.
OUTCOMES OF A TRIPLE THERAPY REGIMEN FOR NON-TUBERCULOUS MYCOBACTERIAL PULMONARY INFECTION
M. Murray1, R. Forsythe2, A. Hill1. 1Royal Infirmary of Edinburgh; 2University of Edinburgh College of Medicine, UK
Aims: There are few randomised controlled trials providing evidence for efficacious treatment regimens for non-tuberculous mycobacterial pulmonary infection (NTM) and success rates remain low. This study aimed to assess outcomes in patients receiving a standard triple therapy regimen of rifampicin and ethambutol and clarithromycin or ciprofloxacin over 24 months for NTM. End points included microbial clearance, systemic inflammation and symptomatology.
Methods: A retrospective review of case notes, microbiological and haematological data for all patients diagnosed with culture positive NTM and managed with rifampicin and ethambutol and clarithromycin or ciprofloxacin over 24 months between 1998–2007 was undertaken. Patients who were HIV positive, had cystic fibrosis or were receiving chemotherapy were excluded. At baseline, 6, 12, 18 and 24 months, sputum microscopy (AFB and full culture status), ESR and symptomatology were recorded.
Results: 38 patients (20 male, 18 female) were eligible for inclusion. The mean (SD) age was 60.5 (16.0) years. 25 patients had completed therapy, with 13 still currently receiving treatment (mean (SD) timepoint,13.7 (8.1) months). All patients were confirmed to be sputum culture positive for NTM: Mycobacterium malmoense 37.5%, M avium complex 32.5%, M xenopi 10%, M intracellulare 5%, M kansasii, M abscessus, M bovis, M interjectum 2.5%, respectively, and as yet unidentified NTM 5%. Main adverse treatment effects were nausea (7%), visual disturbance (3.5%) and peripheral neuritis (3.5%). There were no cases of significant hepatotoxicity (⩾3 times the upper limit of normal ALT range). Two patients died during treatment (one at 12 months due to pulmonary embolism and one at 14 months due to respiratory failure). One patient was lost to follow up at 3 months. The table shows the effects on sputum microbiology, systemic inflammation and symptomatology.
Conclusion: Treatment of NTM with a standard triple therapy regimen of rifampicin and ethambutol and clarithromycin or ciprofloxacin for 24 months significantly improves microbial clearance, reduces systemic inflammation and improves reported symptomatology. These outcomes are superior to rifampicin and ethambutol ± isoniazid from historical data, but randomised controlled trials are needed.
IS THE WORLD HEALTH ORGANIZATION REGIMEN OF THRICE WEEKLY CATEGORY 1 (NEW SPUTUM SMEAR POSITIVE PATIENTS) TREATMENT SUFFICIENT FOR PATIENTS WHO HAVE A HIGH DENSITY OF ACID-FAST BACILLI IN THE SPUTUM?
C. Tenzing1, A. Kujur1, P. D. O. Davies2. 1Nav Jivan Hospital, Satbawra, India; 2TB Unit, Liverpool, UK
Aim: To prove that patients with more than 2+ AFBs in sputum are more likely to fail to sputum convert at the end of the intensive phase of the World Health Organization recommended thrice weekly regime.
Introduction and background: The Nav-jivan Hospital is a unit of Emmanuel Hospital Association, an NGO, based in the Palaumu district of Jharkhand. It has played an important part in the provision of tuberculosis services in the region hand-in-hand with the government as per the revised national tuberculosis programme’s public–private mix initiative. This study has been made from the records of the tuberculosis register of the unit starting from the 1 January 2006 until 31 April 2007. Category 1 patients are new sputum smear positive patients. They are commenced on standard therapy of isoniazid, rifampicin, pyrazinamide and ethambutol. If they have not converted to sputum smear negative at the end of 2 months a further month of intensive therapy is given.
Method: The data are the analysis of the report from the TB register of Nav-jivan district microscopic centre. It was observed that a substantial number of patients were failing to sputum convert at the end of the intensive phase and most of these had had 3+ AFBs in the sputum at diagnosis. Therefore new sputum positives who failed to convert were scrutinised and found to have the following results.
Results: Seventy-one sputum positive patients were diagnosed during that period out of which 58 were new (category 1) sputum positives. Twenty-seven patients had 3+AFB in their sputum at the time of diagnosis. Sixteen patients out of the 58 new sputum positive patients failed to convert at the end of the intensive phase. Out of the 16 patients who failed to convert, 13 (81%) had 3+AFBs at the time of diagnosis. Of the 42 who did convert at the end of the intensive phase 14 (33%) were 3+.
Conclusion: We can conclude that patients with 3+ AFBs in sputum at the time of diagnosis have an increased chance of failing to convert at the end of the intensive phase of the thrice weekly category 1 regimen of WHO compared with other sputum smear positive patients. Patients who do not convert from sputum smear positive to sputum smear negative after 2 months of intensive phase treatment are given a further month of the intensive phase necessitating an extra and usually unexpected supply of drugs. If it is assumed that at least half of category 1 3+ smear patients will require 3 months of intensive phase therapy rather than two, drug supplies can be planned and obtained well in advance. This is an important provision in a resource poor setting.
ARE ALL PATIENTS STARTING ETHAMBUTOL THERAPY RECEIVING ADEQUATE OPTIC NERVE FUNCTION SCREENING?
D. M. Gore1, J. Forbes1, S. Tamne2, D. Creer2. 1Royal Free Hospital, London, UK; 2Barnet & Chase Farm NHS Trust, London, UK
Introduction: Ophthalmologists have traditionally performed baseline assessments for ethambutol optic neuropathy. Following an increase in TB cases, the Eye Clinic had encountered problems providing baseline checks at short notice so specialist TB nurses were trained using a specific protocol.
Method: A retrospective audit of newly diagnosed TB patients over eight months was performed, including Snellen visual acuity (VA) and Ishihara colour vision. VA of less than 6/12 or reduced colour vision warranted referral to the Eye Clinic. Randomly selected “quality control” cases were subsequently seen by ophthalmologists.
Results: 52 newly-diagnosed patients underwent baseline screening. 43 (83%) were screened by nurses in the clinic, the remaining nine (17%) by medical staff while in-patients. Four nurse-screened patients were referred, where ophthalmologists duplicated initial abnormal findings. Of these, three red-green colour defects consistent with congenital colour blindness were identified (two of which were new diagnoses) and one old ischaemic optic neuropathy. One in-patient was confirmed to have previously diagnosed congenital colour blindness. Including randomly selected “quality controls”, a total of 9 (20%) nurse-screened patients were examined by an ophthalmologist; no inconsistencies in VA or Ishihara colour vision scores were found.
Conclusion: This study demonstrates nurse-led screening for optic nerve function to be robust. Current British Thoracic Society guidelines do not recommend assessment of colour vision prior to ethambutol treatment, yet colour vision defects have been found to provide a better indicator and enable early detection of ethambutol toxicity. Correlating with this study, approximately 8% of men in the general population are congenitally colour blind; although there is no evidence that those with pre-existing colour defects either present later or suffer worse toxicity, the usefulness of colour vision testing to diagnose or monitor optic nerve dysfunction in those who subsequently develop vision changes is severely reduced
In addition, as in our female patient diagnosed with an ischaemic optic neuropathy, colour vision screening has the additional benefit, particularly in females, of identifying potentially serious ophthalmic and systemic disorders.
We recommend BTS guidelines for screening of ethambutol treatment be amended to incorporate colour vision.
BARRIERS TO INITIATING ANTIRETROVIRAL THERAPY IN HIV INFECTED PATIENTS WITH TUBERCULOSIS CO-INFECTION
D. N. Chilton1, P. Pellegrino1, S. G. Edwards1, R. F. Miller2. 1Mortimer Market Centre; 2UCL Centre for Sexual Health, London, UK
Background: Concurrent treatment for tuberculosis (TB) and HIV is complicated by overlapping toxicities, drug–drug interactions and risk of immune reconstitution inflammatory syndrome (IRIS). It has been suggested that early initiation of antiretroviral therapy (ART) reduces mortality and prevents opportunistic infection (OI) in severely immunocompromised HIV infected individuals. However, the risk of IRIS is also highest in this group. A balance has to be struck between the risk associated with concurrent treatment of TB and HIV and the risk of HIV disease progression. Although questions still remain about the optimum time to commence ART in co-infected patients, the British HIV Association (BHIVA) has published treatment guidelines for management of HIV infected patients with tuberculosis which are based on available evidence.
Objectives: To describe factors affecting initiation of ART in patients with HIV/TB co-infection and audit our clinical practice against the BHIVA treatment guidelines.
Methods: Retrospective case note review of all co-infected, ART-naïve patients attending an HIV/TB service between January 1994 and June 2007. Data collected included demographics, drug history, CD4, time of ART initiation and reason for delay. ART delay was considered to have occurred if ART was not started within the following parameters: if the CD4 count was <100 cells/µl, within 2 weeks of commencing TB treatment; if the CD4 count = 100–200 cells/µl, after the induction phase of TB treatment; if the CD4 count >200 cells/µl, after completion of TB therapy.
Results: Ninety-one patients were identified. Median CD4 count at presentation with TB = 100 cells/µl (range 10–970). In 15/91 patients, ART could not be started. Information was missing in five. Of the remaining 70, initiation of ART was within BHIVA guidelines in 13/70 (19%) rising to 25/70 (36%) and 48/70 (69%) by 1 and 3 months, respectively. Reasons for delay in initiating ART were: physician concern regarding toxicity and IRIS = 6/57; patient fear of side effects = 3/57; patient refusal = 9/57; TB therapy intolerance/toxicity = 10/57; concomitant AIDS defining OI = 4/57; TB medication adherence issues = 4/57; other = 13/57, reason not documented = 14/57. Concern regarding toxicity, IRIS and side effects was highest in the group with CD4 <100 cells/µl: 7/32(21%), compared with CD4 = 100–200 cells/µl group: 2/12(16%) and CD4 >200 cells/µl group: 0/13(0%). Two patients had IRIS, both in the CD4 <100 cells/µl group; neither had delayed ART initiation. There were five deaths. Four deaths occurred in the CD4 <100 cells/µl group, all had delayed ART; no deaths could be attributed to delayed ART initiation. One death occurred in the CD4 >200 cells/µl group; the patient had been treated within BHIVA guidelines.
Conclusion: Our study highlights the complexity of initiating ART in co-infected patients. Although most patients did not start ART within guidelines, the majority started within 3 months. Despite this, outcome was good. There were no relapses of TB before initiation of ARV. The four cases who had a concomitant OI were diagnosed before ART would have been initiated following HIV/TB guidelines. Common reasons for delay were concern regarding toxicity and IRIS, and intolerance/toxicity of TB medication.
THE TREATMENT OF ISONIAZID RESISTANT TUBERCULOSIS WITH PREDOMINANTLY A 9 MONTH REGIMEN (2RZE/7RE)
L. P. Ormerod, S. A. Haines. Royal Blackburn Hospital, UK
Background: Treatment Guidelines from the JTC (1988) and subsequently from NICE (2006) recommend for isoniazid resistant TB, an initial phase of 2 months rifampicin, (R) pyrazinamide (Z) and ethambutol (E), with a continuation phase of 7–10 months rifampicin and isoniazid.
Methods: 38 patients with proven or presumed isoniazid (H) resistance were treated between 1989–2006. 14 were female, all of South Asian ethnic origin (4 UK born), mean age 28.9 (range 3–59). 24 were male, 2 white, 1 Afghan, and 21 South Asian (2 UK born), mean age 28.7 years (range 12–72). One boy of 12 and 2 girls of 3 and 9 were treated on presumption as household contacts.
Results: Of the culture-confirmed cases, 15 had pulmonary disease, 11 sputum smear and culture positive, 4 smear-negative culture positive. The other sites were cervical gland (12), abdomen and bone/joint (2), and miliary, mediastinal glands, meningitis and subcutaneous abscess (1). 34 cases were treated with a 9 month regimen of rifampicin and ethambutol, with 2 months initial pyrazinamide (2RZE/7RE). 4 patients were treated with other durations or regimens. All patients self-administered treatment but had regular random urine tests for rifampicin. All were followed up at 6 and 12 months with no clinical or x ray recurrence and then discharged. No patient has subsequently returned with clinical disease.
Conclusion: This small study shows that good clinical results can be achieved with a 9 month 2RZE/7RE daily regimen in patients with close adherence monitoring. These results may not be applicable in other settings, eg, some of the patients in the North London outbreak who have multiple risk factors for non-adherence. Theoretically, however, a thrice weekly supervised regimen could deliver a satisfactory outcome.
Survival and lung cancer
PRE-OPERATIVE CHEMOTHERAPY IN PATIENTS WITH RESECTABLE NON-SMALL CELL LUNG CANCER: THE MRC LU22/NVALT/EORTC 08012 MULTICENTRE RANDOMISED TRIAL
D. Gilligan1, M. Nicolson2, I. Smith3, H. J. M. Groen4, C. Manegold5, J. Van Meerbeeck6, P. Hopwood7, M. Nankivell8, C. Pugh8, R. J. Stephens8. 1Addenbrookes Hospital, Cambridge, UK; 2Aberdeen Royal Hospitals Trust; 3The Royal Marsden Hospital, London, UK; 4University Hospital, Groningen, The Netherlands; 5University Medical Centre, Mannheim, Germany; 6University Hospital, Ghent, Belgium; 7Christie Hospital NHS Trust, Manchester, UK; 8MRC Clinical Trials Unit, UK
Aims: Although surgery offers the best chance of cure for patients with non-small cell lung cancer (NSCLC), the overall 5 year survival rate is modest, and improvements are urgently required. This intergroup trial was designed to investigate whether, in patients with operable NSCLC of any stage, neo-adjuvant platinum-based chemotherapy prior to surgery would improve outcomes.
Methods: Patients were randomised to receive either surgery alone (S), or 3 cycles of platinum-based chemotherapy prior to surgery (CT-S).
Results: 519 patients were randomised (261 S, 258 CT-S) from 70 centres in the UK, the Netherlands, Germany and Belgium. The median age of the patients was 63 years, 72% were male, 59% were PS 0, and 50% had squamous cell histology. The majority were clinical stage I (17% Ia, 45% Ib, 3% IIa, 29% IIb, 7% IIIa), and 12% received mitomycin/vinblastine/cisplatin (MVP), 7% mitomycin/ifosfamide/cisplatin (MIC), 45% vinorelbine/cisplatin, 12% carboplatin/docetaxel, and 25% cisplatin/gemcitabine. The trial showed that neo-adjuvant chemotherapy was feasible (76% of patients received all 3 cycles of chemotherapy), resulted in a good response rate (4% CR, 45% PR, and only 2% PD), appeared to cause down-staging in about 20% of patients, and did not affect the type of surgery performed, the postoperative complication rate, or quality of life. However, there was no evidence of a benefit in terms of progression-free survival (299 events, HR 0.96, 95% CI 0.77 to 1.21, p = 0.74) or overall survival (244 deaths, HR 1.02, 95% CI 0.80 to 1.31, p = 0.86), and more patients were reported as having brain metastases in the CT-S group (30 CT-S vs 11 S patients). Exploratory analyses showed no evidence that any subgroup of patients benefited from the addition of neo-adjuvant chemotherapy. The current result is statistically consistent with previous published trials of neo-adjuvant chemotherapy, and updating the systematic review suggests a 5% absolute survival benefit with neo-adjuvant chemotherapy at 5 years (1507 patients, HR 0.88, 95% CI 0.76 to 1.01, p = 0.07).
Conclusion: This intergroup trial, which is the largest trial of neo-adjuvant chemotherapy in patients with resectable NSCLC, indicated that the addition of neo-adjuvant platinum-based chemotherapy did not lead to a benefit in overall survival. However, a 20% survival benefit or a 31% detriment cannot be excluded, but when this result is combined with previous neo-adjuvant trials it indicates a survival benefit similar to that seem with adjuvant chemotherapy.
TWENTY-EIGHT DAYS FROM REFERRAL TO TREATMENT FOR PATIENTS WITH NON-SMALL CELL LUNG CANCER
J. Maguire1, J. Maguire2, V. Kelly1, R. Page1, H. Bonwick3, M. Carr1, C. Smyth1, M. Ledson1, M. Walshaw1. 1Liverpool Lung Cancer Unit; 2Clatterbridge Centre for Oncology; 3Marie Curie Hospice Liverpool, UK
Introduction: NSCLC is the most common fatal lung cancer in Britain. The average survival time for patients diagnosed as having NSCLC in the UK is only between 4 and 5 months. Therefore, even if patients with lung cancer commence treatment in the present government target time of 62 days from GP referral, on average more than 40% of a lung cancer patients’ life expectancy maybe spent undergoing diagnostic tests and waiting for treatment.
Methods and results: In the Liverpool Lung Cancer Unit and Clatterbridge Centre for Oncology, using a rapid access lung cancer diagnostic system and a modernised oncology treatment pathway for patients with lung cancer we have demonstrated that in a trial 1 month period 93% (20/32) of patients can commence definitive treatment with either surgery 15.5%, chemotherapy 35%, radiotherapy 35.1% or palliative care 14.4% within 28 days of initial referral from general practice. The key components in the achievement of a 28 day referral to treatment time were: utilisation of a 1 day rapid access diagnostic service, immediate review of CT scans and performance status data by an oncologist to determine the requirement for PET CT scanning, rapid access to chemotherapy facilitated by use of oral chemotherapy for day 8 treatment, redesign of the planning process for radical radiotherapy to allow patients to proceed from planning to treatment without an interposed planning verification stop, and a parallel clinic arrangement with adjacent respiratory medicine, thoracic surgery, oncology and palliative care colleagues working simultaneously to allow immediate specialists without a paper referral process.
Conclusion: We believe that 28 days from referral to treatment represents a new “gold standard” of care for patients with NSCLC and we plan to maintain and review our redesigned system from September to November 2007 to demonstrate the sustainability of these improvements in service.

ANALYSIS OF A LUNG CANCER COHORT FOR VARIATION IN SURVIVAL OVER A 7 YEAR PERIOD
N. Navani1, B. North2, A. Berry3, J. Brown1, F. Bowen3. 1Hammersmith Hospital; 2Imperial College; 3Charing Cross Hospital, London, UK
Background: Lung cancer is the primary cause of cancer mortality worldwide. Despite advances in treatment, survival from lung cancer remains poor. Five year survival rates are reported as 5% in the UK compared to rates of up to 15% in other European countries.
Methods: We collected data from consecutive patients diagnosed with lung cancer from 2000–3 and 2004–7. Our primary aim was to measure the 1, 3 and 5 year survival rates and compare these to national data. Our secondary aims were to determine how mortality was affected by gender, performance status, year of diagnosis and stage at presentation. Data were obtained from MDT documentation. Kaplan–Meier graphs were plotted to calculate survival. Analysis of individual clinical attributes (eg, performance status) was performed using Cox’s regression model.
Results: There were 746 patients. A histologically proven diagnosis was obtained in 679 (91%) and WHO performance status (PS) was recorded in all but 3 patients. Survival at 1 year was 42.0%, at 3 years 17.8% and 5 years 9.5%. Survival was related to performance status (p<0.001), histological type (p<0.001) and stage at presentation (p<0.001) but not to age (p = 0.077). Patients with stage 1 disease at presentation have a 5 year survival rate of 49%. For an increase of 1 in performance status, the death rate multiplies by 1.73 (95% CI 1.60 to 1.87). Similarly, an increase in stage results in an increase in mortality rate by 1.85 (95% CI 1.67 to 2.05). Survival was improved in the 2004–7 cohort compared to the 2000–3 group (p = 0.006).
Conclusion: Our 1, 3 and 5 year survival data exceed the national average. The data emphasise the importance of performance status as well as stage and cell type as independent variables in determining prognosis. Improved survival in 2004–7 may be due to increased access to a new cross-site expanded multidisciplinary team and consequently an increased uptake of newer generation chemo-radiotherapy regimens.
SURVIVAL FOR PATIENTS WITH LUNG CANCER: THE IMPORTANCE OF PATIENTS WITH NO HISTOLOGICAL DIAGNOSIS
O. K. Kankam, B. Jayaraman, J. Kelly, R. D. Barker. Department of Respiratory Medicine, Kings College Hospital NHS Foundation Trust, London, UK
Background: There are relatively few accurate survival data for lung cancer patients, based on detailed clinical databases. Establishing key determinants of survival would help clinicians offer a prognosis and facilitate understanding of international comparisons of survival. Broad sub-categories of lung cancer have been defined but those without a histological diagnosis are not consistently included. We explored survival for lung cancer with a particular focus on those without a histological diagnosis.
Methods: All patients with lung cancer seen at a teaching hospital in south-east London between 1 July 1999 and 1 January 2007 were included in the study. Patients were separated into those with small cell lung cancer (SCLC), non-small cell lung cancer (NSCLC) and those with presumed lung cancer but without histological confirmation . For some analyses those without histological confirmation were combined with NSCLC to form a group probable NSCLC. Performance status was recorded at diagnosis according to ECOG criteria. Staging for NSCLC was grouped into early (1a–2b), locally advanced (3a and 3b) and advanced (4). Vital status was confirmed by reference to the Thames Cancer Registry, Hospital PMI, GP practices and the NHS tracing service. Only those with a confirmed vital status were included. Univariate survival analysis was undertaken with the Kaplan–Meier method using the log-rank test to establish statistically significant differences. Other univariate analyses used appropriate non-parametric analyses and tests of proportions. We used SPSS version 14.
Results: 944 patients were registered with lung cancer and a confident vital status could be established for 909 (96%). The median age was 71 years (<65 years: 30%, 65–74 years: 34%, >75 years: 36%). There were 602 male patients (65%). There were 107 SCLC (12%), 604 NSCLC (66%) and 198 (22%) had no histological confirmation. Comparisons revealed significant differences in survival between SCLC and NSCLC, SCLC and probable NSCLC, NSCLC and those with unconfirmed histology. There was no difference in survival between SCLC and probable NSCLC. Patients with lung cancer but without histological confirmation had worse performance status (n = 819, median 2 vs 1; p<0.001), were older (n = 909, median 77 vs 69; p<0.001) and had worse airflow obstruction (n = 379, FEV1 median 1.07 vs 1.61; p<0.001). For those with NSCLC the failure to obtain a tissue diagnosis was associated with metastatic disease (n = 748, 101/175 (58%) vs 261/573 (46%)).
Conclusion: Patients without a histological diagnosis have significantly worse survival than other patients with lung cancer perhaps because they have other poor prognostic indicators. This should be taken into account when comparing lung cancer survival between diagnostic units and between countries.
NO IMPROVEMENT IN SURVIVAL FOR NON-SMALL CELL LUNG CANCER BETWEEN 1999 AND 2007: THE EXPERIENCE OF AN INNER LONDON TEACHING HOSPITAL
B. Jayaraman, O. K. Kankam, J. Kelly, R. D. Barker. Department of Respiratory Medicine, Kings College Hospital NHS Foundation Trust, London, UK
Background: It was hoped that with the introduction of multidisciplinary team working and greater access to potentially curative treatment, that survival for patients with lung cancer would improve. This view has been supported by colleagues from a nearby hospital who reported a significant improvement in survival for patients with histologically proven non-small cell lung cancer (NSCLC) over a 6 year period to 2004. We wanted to see whether there had been a similar improvement in survival for our patients with NSCLC.
Methods: The patients were all diagnosed with lung cancer at an inner city teaching hospital in south-east London between 1 July 1999 and 1 January 2007. Patients with histologically proven NSCLC and patients with a clinical diagnosis, but without tissue confirmation, were included, and for this study have been categorised as NSCLC. Performance status was recorded at diagnosis according to ECOG criteria. Staging for NSCLC was grouped into localised (1a–2b), locally advanced (3a and 3b) and advanced (4). Age was categorised into those less than 65 years, 65–74 and 75 and over. A record was made as to whether the patient received a potentially curative resection. The patients were divided into four, 2 year epochs. Vital status was confirmed by reference to the Thames Cancer Registry, Hospital PMI, GP practices and the NHS tracing service. Only those with a confirmed vital status were included. Survival was censored at 1 January 2007. Univariate survival analysis was undertaken with the Kaplan–Meier method using the log-rank test to establish statistically significant differences. Multivariate analysis was done using forward stepwise regression and Cox’s proportional hazards model. We used SPSS version 14.
Results: 802 patients were included. There were 538 men (67%). 239 (30%) were aged <65 years, 271 (34%) 65–74 years, 292 (36%) ⩾75. Of 748 with documented staging, 138 (18%) had localised disease, 248 (33%) locally advanced, and 362 (45%) advanced disease. Of 724 with a performance status 0 = 156 (22%), 1 = 226 (31%), 2 = 156 (22%), 3 = 118 (16%), 4 = 68 (9%). 80 (10%) underwent a surgical resection. 604 (25%) had confirmed histology. In univariate analysis survival was not related to sex or epoch. Survival was related to age group, histological confirmation, stage of disease, performance status and whether the patient underwent resection.
Conclusion: There was no evidence of an improvement in survival with time for patients with NSCLC. Age was not a predictor of survival once adjustment had been made for other relevant factors. There was evidence for a beneficial effect of surgical resection. Unconfirmed histology acted independently of resection, performance status and age and may be a surrogate for co-morbidity.
SURVIVAL IN 176 PATIENTS WITH INOPERABLE NON-SMALL CELL LUNG CANCER TREATED INITIALLY WITH CHEMOTHERAPY IN A DISTRICT GENERAL HOSPITAL
A. H. N. Gerratt1, S. Ahmad1, K. Graham1, S. P. Patel2, J. R. Webb1, T. C. Stokes1. 1Queen Elizabeth Hospital NHS Trust; 2Health & Social Care, University of Greenwich, London, UK
In advanced non-small cell lung cancer (NSCLC) platinum based chemotherapy with second generation drugs improves median survival (MS) to 8 months and 29% and 10% at 1 and 2 years. Platinum with a third generation drug can improve survival further (BMJ 1995;311: 899) (Spiro et al. Thorax 2004;59:828 Big Lung Trial; N Engl J Med 2003;346:92 ECOG study). NICE now recommends chemotherapy with platinum and a third generation drug for inoperable NSCLC as the first treatment modality.
Methods: We audited survival of 176/461 consecutive patients referred for at least 3 courses of platinum and either gemcitabine or vinorelbine from July 2001 to December 2005. Minimal follow up 17 months. Chemotherapy was given on site. Radical radiotherapy for stage IIIA, palliative radiotherapy and second line drugs were given as felt appropriate.
Results: 64% were male. 30 (17%) were <55 years ; 66 (37.5%) age 55–65 years; 63 (35.8%) aged 66–75 and 16 (9.1%) >75 years. 5 (2.8%) were stage II; 46 (26%) stage IIIA; 68 (38%) stage IIIB and 55 (30.8%) stage IV. 68 (38%) had 0– 2 courses; 63 (36%) 3 courses and 44 (25%) had 4 or more.
Survival: For the 157 (89%) patients who died, median survival was 283 days. The 18 survivors had 925 days. Median overall survival (OS) was 334 days (95% CI 258 to 410). One year OS was 46.3% (95% CI 38.9 to 53.7). Two year OS was 18.9% (95% CI 13.1 to 24.7). MS in stage IIIA was 465 days (95% CI 352 to 578), stage IIIB was 307 days (95% CI 100 to 514) and MS in stage IV was 239 days (95% CI 155 to 323). Survival for stage IV vs (IIIA and IIIB) is significant (p<0.0005) but not between IIIA and IIIB (p = 0.658) (Cox’s proportional hazard). Survival was optimal with three courses of chemotherapy. Older patients tended to survive longer but not significantly so.
Conclusion: Our results indicate that chemotherapy can be successfully and effectively given to eligible patients with NSCLC. The survival figures are comparable to published data. In the district general hospital setting there is the added benefit to patients of having treatment close to home.
Molecular mechanisms of respiratory disease
THE ROLE OF ACTIVATOR PROTEIN-1 (AP-1) FAMILY MEMBERS IN THE INDUCTION OF INTERLEUKIN (IL)-8 BY CYCLIC MECHANICAL STRAIN IN LUNG EPITHELIAL CELLS
L. Pinhu, W. Yao, M. Griffiths. NHLI, Imperial College, London, UK
Rationale: Over-distension of the lung by mechanical ventilation contributes to the mortality of patients with acute lung injury. Mechanical forces enhance the release of mediators that exacerbate lung damage (ventilator-associated lung injury: VALI) and contribute to systemic inflammation and death. The neutrophil chemokine IL-8 (CXCL-8) has been implicated in the pathogenesis of ALI clinically and in animal models. Cyclic mechanical strain (CMS) applied to A549 cells (a human alveolar epithelial cell line) and primary cultures of human alveolar type 2 cells, models of alveolar over-distension, was associated with IL-8 production that was dependent on extracellular signal-related kinase (ERK1/2) activity. Furthermore, DNA binding of the AP-1 transcription factor cFos was prevented by inhibition of the ERK1/2 pathway by U0126. The induction of cFos and other immediate early response genes to mechanical stimuli is well established. IL-1β-induced IL-8 is mediated in part by cFos and inhibited by Fra-1 through displacement of cFos from the IL-8 promoter and recruitment of HDAC1. The following experiments were performed to determine the role of cFos and other AP-1 family members (Fos-related antigen-1 [Fra-1], cJun, JunB, JunD) in the induction of IL-8 by CMS.
Methods and results: The application of CMS to A549 cells for 30 minutes induced mRNA for cFos, Fra-1, cJun, and JunB, but not JunD. The induction of cFos and Fra-1 mRNA, but not cJun was abolished by the MEK1/2 inhibitor U0126. Chromatin immunoprecipitation (ChIP) analysis of the AP-1 site of the IL-8 promoter using antibodies against cFos after CMS in the presence and absence of U0126 (10 μM), U0124 (inactive: 10 μM) and AS602868 (IKK-2 inhibitor: 3 μM) confirmed ERK1/2 dependent binding of cFos (see fig 1). Finally, siRNA-mediated knockdown of cFos specifically abolished the effect of CMS on IL-8 induction in A549 cells confirming the absolute requirement for this transcription factor (see fig 2).
LP is supported by the Dr Hadwen Trust for Humane Research.
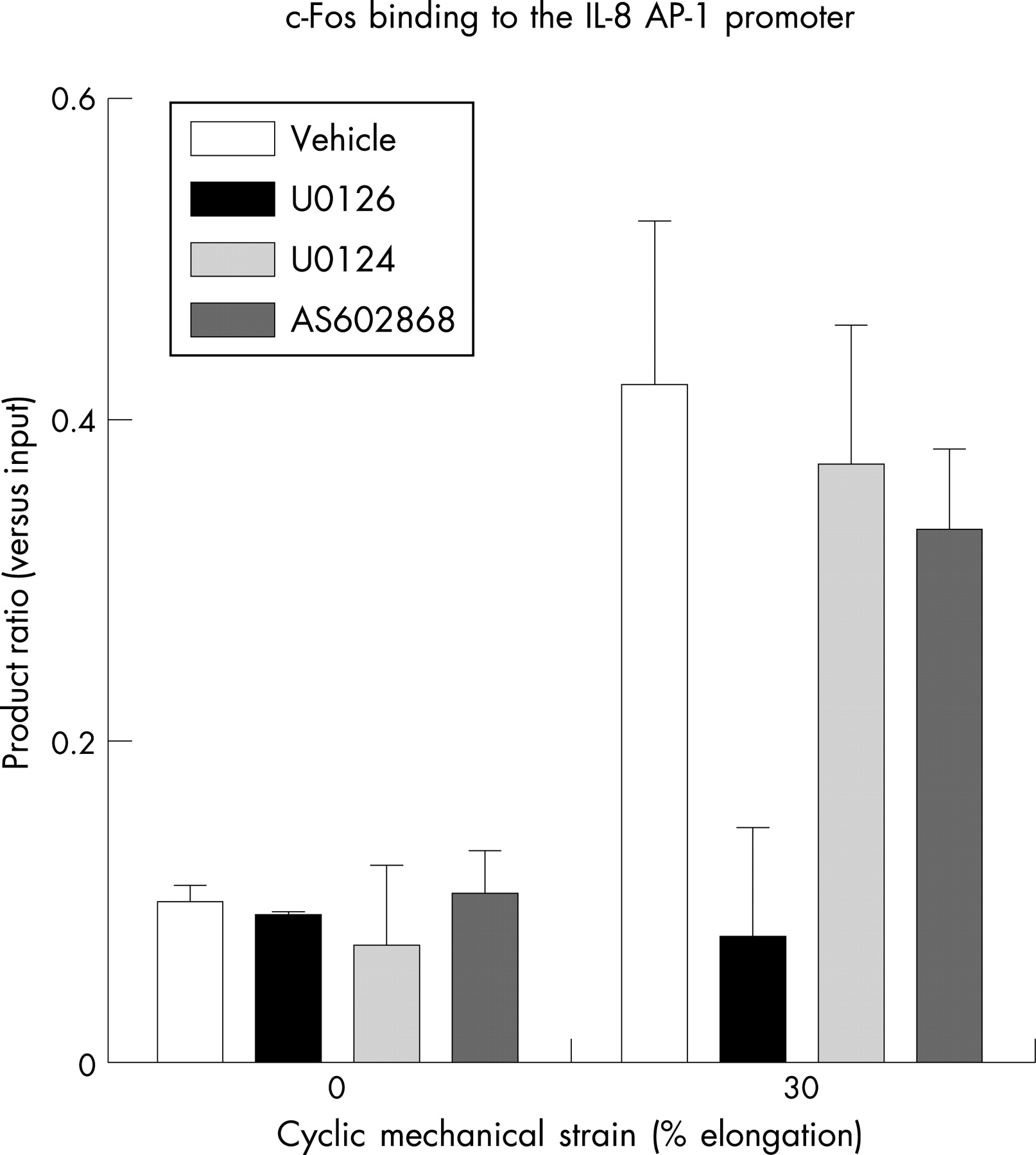

Conclusion: Certain AP-1 family members are rapidly induced by CMS in A549 cells and play a crucial role in regulating the induction of IL-8 by the ERK1/2 MAPK pathway.
LUNG-MARGINATED MONOCYTES PLAY A CENTRAL ROLE IN A TWO-HIT LPS-ZYMOSAN MODEL OF ACUTE LUNG INJURY IN MICE
K. P. O’Dea, M. R. Wilson, J. O. Dokpesi, M. Takata. Imperial College London, UK
Introduction: Although margination and activation of neutrophils within the lungs play an important role in the development of acute lung injury (ALI), the contribution of monocytes is unknown. During subclinical endotoxaemia in mice, large numbers of the inflammatory Gr-1high monocyte subset marginate to the pulmonary microcirculation and respond vigorously to secondary septic challenge, expressing high levels of membrane tumour necrosis factor-alpha. Here we assessed recruitment of Gr-1high monocytes from the bone marrow reservoir to the pulmonary microcirculation during subclinical endotoxaemia and their contribution to pulmonary vascular leak in a 2-hit LPS-zymosan model of ALI.
Methods: Bone marrow mobilisation of monocytes and margination to the lungs was assessed in C57BL6 mice after subclinical, low-dose i.v. LPS challenge, using flow cytometry and in vivo BrdU labelling of dividing bone marrow monocytes. The contribution of LPS “pre-marginated” monocytes to i.v. zymosan-induced changes in pulmonary vascular permeability was determined by measuring extravascular leak of labelled albumin and its modulation by clodronate-liposome mediated depletion of monocytes.
Results: Early mobilisation of bone marrow Gr-1high monocytes and their margination to the lungs during subclinical endotoxaemia was evident from a reduction of their numbers in the bone marrow (3.0±0.4×106 to 1.8±0.2×106/femur+tibia, p<0.01) and an increase in BrdU-labelled cells in the lungs at 2 h after low-dose LPS challenge. LPS priming-dependent increases in vascular permeability after zymosan challenge were attenuated by depletion of monocytes (see fig). However, this protective effect was reversed at 48 h post-clodronate treatment, when LPS-induced Gr-1high monocyte margination to the lungs had returned to normal levels. n = 4–6/each group.
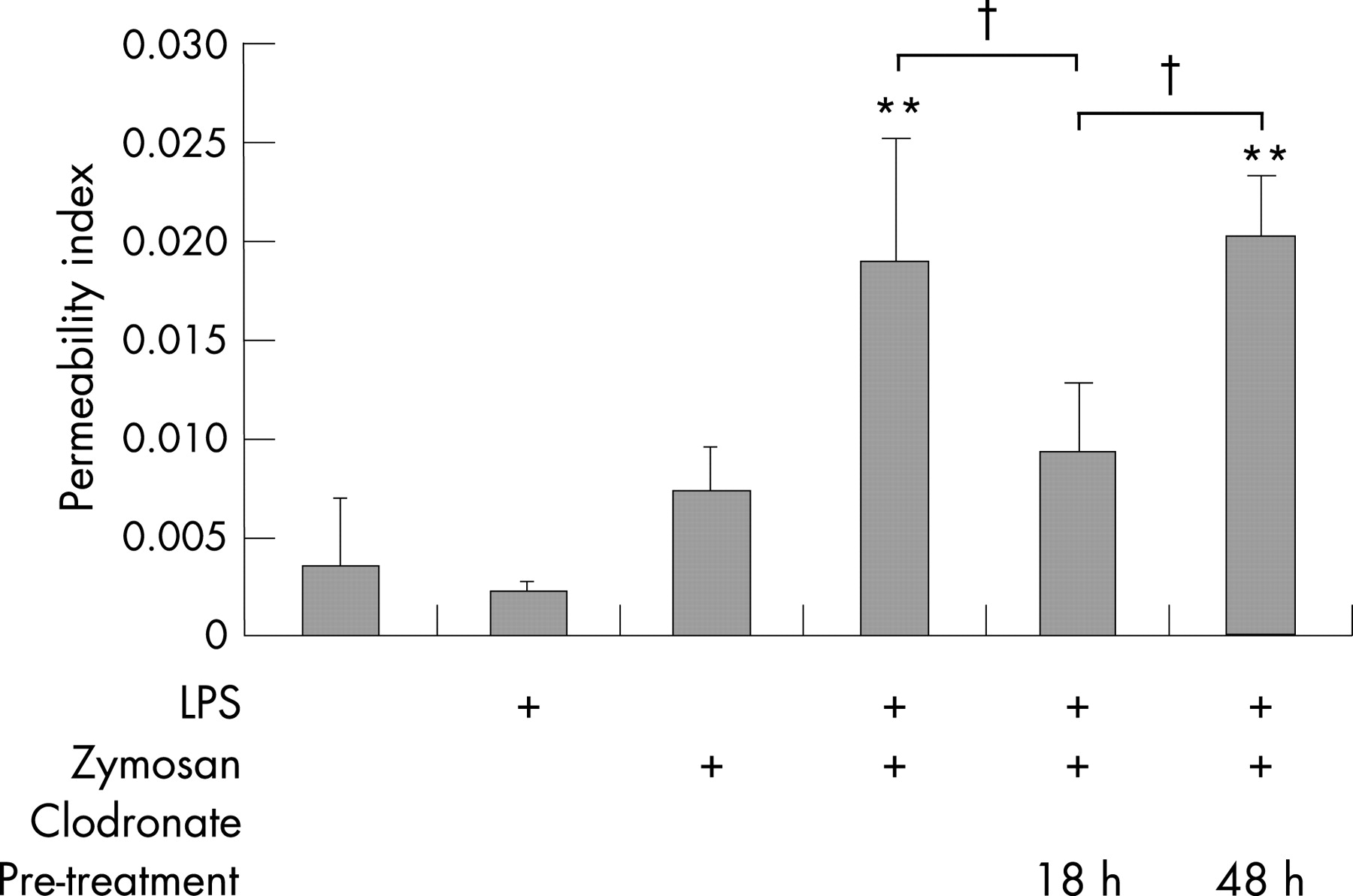
Conclusion: These results suggest that recruitment of bone marrow Gr-1high monocytes to the pulmonary microcirculation during subclinical endotoxaemia transforms the lungs into a “primed” state. Upon further systemic septic challenge, these pre-marginated monocytes could play a crucial role in the development of sepsis-related ALI.
This study was supported by grants from Biotechnology and Biological Sciences Research Council and Medical Research Council UK.
TRANSFORMING GROWTH FACTOR BETA (TGFβ) INDUCES CELLULAR SENESCENCE IN PRIMARY BRONCHIAL EPITHELIAL CELLS: A POSSIBLE ROLE IN AIRWAY REMODELLING
S. M. Parker, M. R. Gorowiec, L. A. Borthwick, J. L. Lordan, C. Ward, P. A. Corris, G. C. Saretzki. University of Newcastle, UK
Introduction: The profibrotic cytokine transforming growth factor beta (TGFβ) has been implicated in the pathogenesis of obliterative bronchiolitis (OB) after human lung transplantation. TGFβ has pleiotropic actions including the development of cellular senescence in fibroblasts and cell lines, however the relevance of this process to airway epithelium is unclear. Cellular senescence is a fundamental cellular response to stress, cells adopt a characteristic morphology and are growth arrested with a proinflammatory phenotype. Consequent lack of tissue regenerative capacity and release of proinflammatory mediators could contribute to an aberrant response to airway injury and subsequent remodelling seen in OB.
Aim: To examine whether TGFβ can induce cellular senescence in primary bronchial epithelial cells (PBECs) derived from lung transplant recipients.
Methods: PBECs (n = 4) grown from stable lung transplant recipients were treated for 72 hours with TGFβ (10 ng/ml). Cellular senescence was assessed by looking at cell phenotype and staining paraformaldehyde fixed cells for senescence associated beta galactosidase. Cellular proliferation was assessed by Ki 67 immunofluorescence. Levels of the cell cycle inhibitor proteins p16 and p21 were assayed by western blotting. Intracellular reactive oxygen species (ROS) were measured on FACS by staining with mitoSOX and dihydrorhodamine.
Results: A proportion of cells treated with TGFβ (10 ng/ml) for 72 hours adopted an enlarged senescent like morphology with increased SA β gal staining (mean number SA β gal positive cells: control 6.6±1.4%, TGFβ 28±4.7%, p<0.05) and fewer Ki 67 expressing proliferating cells (mean number Ki 67 positive cells: control 73.5±5.78%, TGFβ 13.4±8.73%, p<0.05). Levels of p16 were significantly elevated (mean fold increase in treated cells compared to control 1.58±0.25, p<0.05) as were levels of p21 (mean fold increase compared to control 2.75±1.37, p = ns). Intracellular ROS were increased (mean fold increase compared to control mitoSOX 1.68±0.48, dihydrorhodamine 1.66±1.47 p<0.05 for both).
Conclusion: TGFβ can induce features consistent with cellular senescence in PBECs and this is associated with an increase in intracellular oxidative stress. An accumulation of senescent cells in the airway could contribute to the development of OB and other airway diseases associated with remodelling.
ADAM33 IN LUNG DEVELOPMENT AND THE EFFECT OF MATERNAL ALLERGY
H. M. Haitchi1, J. P. Bassett2, X. Gao2, S. T. Holgate1, D. E. Davies1. 1Roger Brooke Laboratory, Division of Infection Inflammation & Repair, University of Southampton, UK; 2Department of Fundamental & Applied Sciences, Wayne State University, Detroit, USA
Rationale: Polymorphisms of ADAM33 are strongly associated with asthma and bronchial hyperresponsiveness (BHR) (Van Eerdewegh P et al. Nature 2002). The murine homolog for ADAM33 has also been associated with BHR (BHR1 locus) (De Sanctis et al. Nat Genet 1995). SNPs in ADAM33 predict impaired lung function in young children (Simpson A et al. AJRCCM 2005). To investigate a role for ADAM33 in early life, we studied the expression of ADAM33 in mouse embryonic lungs from healthy and allergic mothers.
Methods: MF-1 mouse lungs were harvested at embryonic day (ED) 11–19 and day 1 and day post partum (PD) (n = 5–8). A/J mice (BHR1 positive) were sensitised with ovalbumin (ova), time-mated and exposed to ova or saline (1 hour, 3 times/week). ED15 and 18 and PD5 lungs and newborn lungs (n = 4–19) were harvested from normal and allergic mice. Samples were processed for mRNA analysis of ADAM33 and α-smooth muscle actin (αSMA) by RT-qPCR.
Results: ADAM33 mRNA expression increased in 4 significant (p<0.002) steps during mouse lung development. These corresponded to the recognised stages of lung development. The greatest increases in ADAM33 expression occurred from ED11–12 and postpartum. A similar pattern of expression was observed for α-SMA. In the Ovalbumin allergen challenge mouse model, ADAM33 mRNA expression was significantly (p = 0.03) depressed and α-SMA mRNA showed a tendency (p = 027) for suppression in PD5 offspring from allergic A/J mice.
Conclusion: The increase in ADAM33 in the early stages of lung development and postpartum suggest that it might be induced by tubular contraction that starts in the pseudoglandular stage and mechanical stretch from breathing after birth. The down regulation of ADAM33 in newborn mice from allergic mothers suggests, for the first time, a link between environmental influences associated with Th2 type inflammation and a locally acting asthma susceptibility gene.
Funded by: AAIR Charity, British Lung Foundation & Roger Brooke Charitable Trust (UK).
STRUCTURE AND FUNCTIONAL ANALYSIS OF LIPOPOLYSACCHARIDE AND LIPID A OF BURKHOLDERIA MULTIVORANS STRAINS ISOLATED FROM CYSTIC FIBROSIS TRANSPLANT RECIPIENTS
A. Silipo2, T. Ierano2, C. Aldridge1, A. De Soyza1, D. Garrozo2, A. Molinaro1, P. A. Corris1. 1University of Newcastle, UK; 2University of Napoli, Italy
Background: The Burkholderia cepacia complex (BCC) is a group of Gram negative bacteria of nine phenotypically similar but genetically distinct species or genomovars. All BCC genomovars have been reported as opportunistic pathogens for humans in cystic fibrosis (CF) patients. The most prevalent and also most virulent strains isolated from CF centres are B cenocepacia and B multivorans. Pre-transplant infection with B cenocepacia is associated with poor outcomes following lung transplantation whereas infection with B multivorans does not. Lipopolysaccharide (LPS) molecules are potent virulence factors in Gram negative bacteria. The cystic fibrosis airway is believed to induce specific LPS changes in both Pseudomonas and Burkholderia spp. A complete analysis of the bacterial endotoxins’ structure to biological activity may offer new therapeutic avenues.
Methods: Strains from our transplant programme were screened. We investigated and compared the structures of LPS and lipid A-core regions from clonally identical Burkholderia multivorans strains isolated pre- and post-lung transplantation through compositional analysis, mass spectrometry and 2D NMR spectroscopy. Prior pulsed field gel electrophoresis data confirmed clonal identity of the strains. The pro-inflammatory activity of extracted LPS was tested as a stimulant of human myelomonocytic U937 cell cytokine (TNF) induction.
Results: In one clonal pair there were LPS migration differences on SDS gels and significant lowering in TNF induction capacity of the post transplant strain. The predominant structural differences in these strains were found in the lipid A portion. The core oligosaccharide sequence of B multivorans species investigated was quite different to that of B cenocepacia. The lipid A from B multivorans pre-transplantation had significant structural motifs associated with activity against airway immunity including the lipid A acylation status and amino-arabinose residues conferring resistance against defensins. Interestingly the post-transplant strain demonstrated a decreased lipid A acylation status consistent with the reduction in TNF cytokine induction capacity.
Conclusion: Such structural variations may contribute to the bacterial survival and persistence of infections despite the loss of a CF milieu following lung transplantation. This phenomenon was not noted for B vietnamiensis or B cenocepacia strains tested raising the question of differential responses between genomovars.
K5, A KAPOSI SARCOMA HERPESVIRUS GENE PRODUCT, TARGETS BONE MORPHOGENETIC PROTEIN RECEPTOR II FOR UBIQUITINATION AND ENDOSOMAL DEGRADATION
H. J. Durrington1, P. Upton1, N. W. Morrell1, P. Lehner2. 1Department of Medicine, Addenbrooke’s Hospital, Cambridge University; 2Cambridge Institute of Medical Research, UK
Introduction: 70% of patients with familial pulmonary arterial hypertension (PAH) have a mutation in the gene encoding bone morphogenetic protein receptor-II (BMPR-II). Penetrance of BMPR-II mutations varies from 15–50%, suggesting additional genetic/environmental events are required to cause disease. Kaposi sarcoma herpesvirus (KSHV) has been identified as a possible aetiological agent in PAH pathogenesis (Cool et al. N Engl J Med 2003). KSHV expresses a protein, K5, which acts as an E3 ubiquitin ligase, targeting cell surface receptors (MHC class 1) for degradation, allowing the virus to establish latent infection. We previously demonstrated that HeLa cells stably transfected with K5 possess reduced cell surface 125I-BMP4 binding sites and reduced activation of BMP stimulated Smad1/5 signalling compared with control cells. We hypothesise that K5 targets BMPR-II at the cell surface, reducing protein stability, by causing its degradation via ubiquitination.
Methods: Expression of BMPR-II protein was determined by Western blotting in: (1) HeLa cells stably expressing K5 compared with wild type HeLa cells; and (2) in HeLa cells transiently transfected with K5 or mutant K5m, lacking ubiquitin ligase activity. We determined the subcellular localisation of BMPR-II in the stable cell lines by immunofluorescence and confocal microcroscopy. Concanomycin A, an inhibitor of endosomal degradation, was used to treat stable K5 HeLa cells and control cells, prior to blotting for BMPR-II.
Results: BMPR-II protein was markedly reduced in stable K5 HeLa cells compared to control cells. This effect was seen after transient transfection of K5 into HeLa cells (at 48 hours), but not after transfection with K5m. Immunofluorescence microscopy for BMPR-II demonstrated a reduction in BMPR-II protein expression in K5 HeLas compared to wild type. Treatment of K5 HeLa cells with Concanomycin A, rescued the reduction in BMPR-II (see fig).
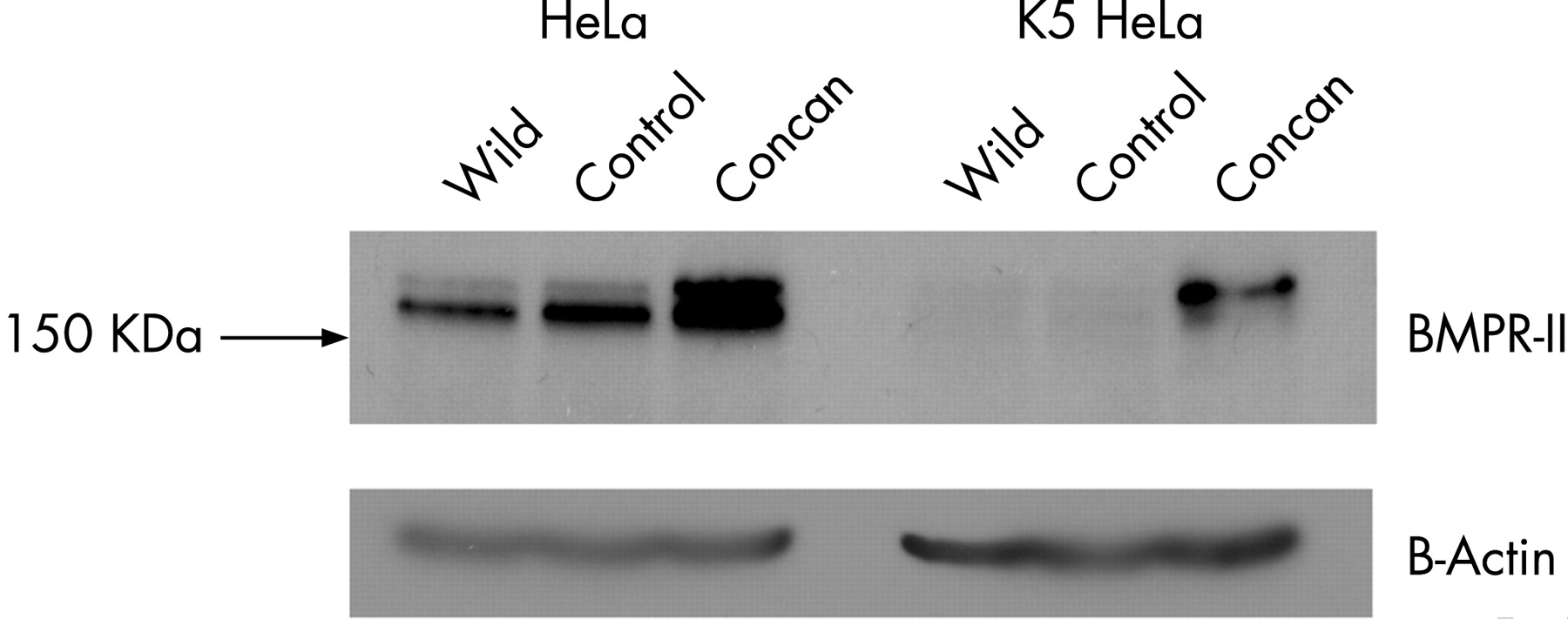
Conclusion: These experiments demonstrate that BMPR-II is a cellular target of KSHV K5 and suggest that K5 degrades BMPR-II by ubiquitination via an endosomal pathway.
Paediatric asthma: bedside and bench
CHARACTERISATION OF CHILDREN WITH DIFFICULT TO TREAT ASTHMA
L. Fleming1, M. Bracken2, P. Hall2, N. Wilson2, A. Bush1. 1Imperial College; 2Royal Brompton Hospital, London, UK
Background: Difficult asthma (DA) is that which is poorly controlled despite maximal doses of conventional therapy. Our current DA protocol provides a systematic approach to assessment and subsequent management.
Aim: To characterise children referred for the DA protocol and evaluate underlying contributing factors following initial assessment.
Methods: All children referred to our DA protocol from March 2005–June 2007 are included. Children were reviewed during an outpatient hospital visit and a nurse led home visit. At these visits an assessment was made of atopy (skin prick tests, SPTs), inflammation (exhaled nitric oxide (FeNO50), spirometry pre- and post-bronchodilator (BD), psychosocial background, adherence and clinical history. Following discussion at an interdisciplinary meeting, underlying contributing factors were identified and appropriate interventions made. Only those whose control did not improve following initial intervention went on to undergo further evaluation including bronchoscopy.
Results: 63 children (26 boys), median age 12.5 years (range 5.3–17 years) were assessed. 12 (19%) had a previous life threatening episode of asthma requiring ventilation. 18 were prescribed maintenance oral steroids. The median dose of inhaled corticosteroids was 960 μg/day, fluticasone equivalent (range 240–2000 μg). 86% were atopic (⩾1 positive SPT for common allergens). 23 had a positive SPT for house dust mite. 24 had pets of whom 46% had a positive SPT to their own pet. 31 children were referred to a psychologist. 27 children went on to have further investigations including bronchoscopy.
Conclusion: Children with DA are a heterogeneous group both in terms of contributing factors and underlying pathology. Careful evaluation will reveal potentially remedial causes for poorly controlled symptoms avoiding the necessity for further, more invasive investigations.
AIRWAY EPITHELIAL CELL MEDIATOR RELEASE IS ASSOCIATED WITH WHEEZING BUT NOT ATOPY IN CHILDREN
C. M. McDougall, M. G. Blaylock, P. J. Helms, G. M. Walsh. University ofAberdeen, UK
Introduction: Although airway epithelial cells (AEC) are key contributors to immune function in the lungs and to the inflammatory response seen in asthma in adults, little is known about their role in childhood wheezing. Having established that nasal AEC cytokine release correlates with that of bronchial AEC, we aimed to study AEC responses in different childhood wheezing phenotypes.
Methods: After ethical approval and informed consent, nasal AEC cultures were established from children (0.6–14.9 years) undergoing elective surgical procedures under general anaesthetic, categorised as atopic asthmatics (n = 12), virus-induced wheezers (n = 8) or healthy controls (n = 32) using questionnaire and serum IgE levels. All subjects were free of current respiratory symptoms. Mediator release by resting and stimulated (IL-1β + TNFα at 10 ng/ml for 24 hours) AEC monolayers at passage 2 was determined by cytometric bead array assay (IL-8, IL-6, VEGF, G-CSF, MCP-1, RANTES) or ELISA (MMP-9, TIMP-1) of culture supernatants and corrected for cellular protein content.
Results: Successful AEC cultures were established from 81% nasal brushings and maintained to passage 2 for 41 (79%) subjects. AEC from children with a history of wheeze produced significantly less IL-8, IL-6, MCP-1 and G-CSF than AEC from healthy controls (see table). When the wheezing phenotypes were considered separately, AEC from atopic asthmatic children released significantly less IL-8, IL-6, MCP-1 and G-CSF than AEC from controls but there were no significant differences between AEC mediator release from children with virus-induced wheeze and either atopic asthmatics or controls. Similar results were found for cytokine-stimulated AEC. In non-wheezy subjects, there were no differences in AEC mediator release between atopic and non-atopic individuals. There were no differences between the study groups in the percentage increments in mediator release in response to stimulation. In multivariate analysis, taking into account age, gender, passive smoke exposure, use of inhaled corticosteroids, total serum IgE and specific IgE responses to inhaled aeroallergens as possible confounders, wheeze was the only significant predictor of AEC mediator release.
Conclusion: An in vitro model of respiratory epithelium, suitable for functional studies, can be established from nasal brushings from children. AEC are a potent source of inflammatory mediators and are capable of responding to proinflammatory stimuli. There are intrinsic differences in AEC from children with a history of wheeze compared to healthy controls which appear to be independent of atopic status. This may reflect a defect in cytokine production by asthmatic AEC in vivo or an altered state of differentiation of cultured asthmatic AEC compared to normal AEC.
DO LUNG FUNCTION TESTS AT 4–6 YEARS OF AGE IN SEVERE PRESCHOOL WHEEZERS CORRELATE WITH ENDOBRONCHIAL BIOPSY IN EARLY PRESCHOOL YEARS?
S. Sonnappa1, C. Bastardo1, S. Saglani3, S. Mckenzie2, A. Bush3, P. Aurora1. 1Great Ormond Street Hospital for Children and Institute of Child Health; 2Royal London Hospital; 3Royal Brompton Hospital and Imperial College, London, UK
Background: Non-reversible conductive airways (Scond) heterogeneity has been reported in adults with asthma. The aim of this study was to measure specific airways resistance (sRaw) and measures of ventilation inhomogeneity, with bronchodilator reversibility, at 4–6 years of age in children who had been investigated for severe wheeze with endobronchial biopsy (EBB) at median age 2.5 years (range 3 months–5 years).
Methods: Children between 4–6 years with a history of severe recurrent wheeze before 3 years of age, previously investigated with EBB underwent clinical and lung function assessments before and after bronchodilator. sRaw was measured by whole body plethysmography, and lung clearance index (LCI); functional residual capacity; Scond and acinar contribution to ventilation inhomogeneity (Sacin) measured by multiple breath washout. Pre-bronchodilator measurements were compared to healthy controls and correlated with reticular basement membrane thickening (RBM), subepithelial eosinophilic inflammation and total inflammation as previously measured on EBB. Subgroup analysis was performed by current atopic/non-atopic phenotype and wheeze status defined as transient (asymptomatic in previous year) or persistent.
Results: Children with a history of recurrent wheeze (n = 25, median age 5.1 (range 4–6.9) years; atopic (n = 11); persistent wheeze (n = 16)) were compared to age-matched healthy controls (n = 31). Scond was significantly higher in both groups of wheezers compared to controls (0.059 vs 0.022, mean diff −0.037 (95% CI −0.022 to −0.052) p<0.0005). There was no significant difference in the other pre-bronchodilator lung function parameters. There was no correlation between lung function and previous EBB findings. Measurements after bronchodilator showed significant improvement in sRaw (1.276 vs 1.030, −0.245 (95% CI −0.130 to −0.360) p<0.0005) and Scond (0.059 vs 0.036, −0.022 (95% CI −0.007 to −0.037) p<0.005), but Scond values remained higher than in controls (0.036 vs 0.022, −0.014 (95% CI −0.003 to −0.031) p<0.012). There was no difference in lung function parameters between atopic and non-atopic or persistent and transient wheezers. Persistent wheezers were more likely to have had RBM thickening (p = 0.028).
Conclusion: Conductive airways heterogeneity, only partially responsive to bronchodilator, is already present in severe preschool wheezers, irrespective of resolution of symptoms, suggesting continued structural changes in the airways. RBM thickening in early preschool years is associated with persistent wheeze in late preschool years.
EVIDENCE OF PERSISTENT SMALL AIRWAYS DISEASE MEASURED BY LUNG CLEARANCE INDEX IN WELL-CONTROLLED ASTHMATIC CHILDREN WITH NORMAL FEV1
K. A. Macleod1, A. Horsley2, J. A. Innes2, S. Cunningham1. 1Royal Hospital for Sick Children; 2Western General Hospital, Edinburgh, UK
Introduction: In asthmatic patients, conventional spirometry (FEV1, PEFR) is known to be relatively insensitive to small airways function. Lung clearance index (LCI), a simple measure of non-uniformity of ventilation, can be calculated from multiple breath inert gas washouts and is thought to reflect heterogeneity of disease in the small airways. We have used a novel gas analyser (Innocor) for multiple breath washout measurements in well-controlled asthmatic children and healthy age-matched controls.
Methods: This randomised double-blind study involved asthmatic children completing 3 multiple breath washouts from SF6 before and after inhaled salbutamol (200 μg) or placebo. Standard spirometry and exhaled nitric oxide (FeNO) were performed at the same time. At the second visit subjects repeated the process with the other intervention. Healthy volunteer controls completed 3 washouts at one visit only. Well-controlled asthmatic children on regular preventer therapy (n = 31, mean age 10.6, range 5–15) were compared with healthy controls (n = 29, mean age 11.2, range 5–16).
Results: The measurement of LCI was well tolerated by all children. Agreement was good between 3 washouts. Mean (SD) LCI at first baseline visit was significantly higher in asthmatic children, 6.85 (0.92) vs controls, 6.38 (0.51), p = 0.02. Mean (SD) FEV1 % predicted was not significantly different between asthmatics and controls (85.6 (17.1) vs 90.8 (11.75), p = 0.17). There was no correlation between baseline LCI and FeNO or FEV1 in either asthmatics or controls (p>0.05). After inhaled salbutamol there was no significant change in FEV1 (p = 0.31) or LCI (p = 0.46). Mean LCI post-bronchodilator was 6.81, remaining significantly higher than healthy controls (p = 0.01).
Conclusion: LCI is a simple, reproducible measure of ventilation efficiency that is easy to perform in children using the modified Innocor device. LCI was significantly higher in well controlled asthmatics compared with controls. Post-bronchodilator LCI was still higher than in baseline controls indicating that residual airways abnormality, not responsive to inhaled β2 agonist and not detected by routine asthma monitoring methods (FEV1, FeNO), can be detected by LCI.

CAN DAILY EXHALED NITRIC OXIDE MEASUREMENTS PREDICT A CLINICAL RESPONSE TO SYSTEMIC CORTICOSTEROIDS IN CHILDREN WITH DIFFICULT ASTHMA?
L. Fleming1, N. Regamey1, C. Bossley2, N. Wilson2, A. Bush1. 1Imperial College; 2Royal Brompton Hospital, London, UK
Background: Levels of exhaled nitric oxide (FeNO50) have been shown to fall in response to corticosteroids in children with asthma and can be used as a surrogate measure of underlying airway inflammation and steroid responsiveness.
Aim: To assess whether daily recordings of FeNO50 measured from the time of triamcinolone administration can predict clinical responsiveness.
Methods: Our difficult asthma protocol involves a 3 stage assessment. Following initial assessment (stage 1) only those for whom remedial factors have not been identified and symptoms improved go on to have further investigations (stages 2 and 3). Children undergoing bronchoscopy had inflammation measured (FeNO50, sputum eosinophils (eos)), spirometry (pre- and post-bronchodilator (BD)) and clinical evaluation (asthma control test (ACT)) on the day of bronchoscopy (stage 2) and 1 month later (stage 3). They were issued with NiOX MINOs, a hand held device for measuring FeNO50, and were asked to record measurements daily.
Results: 10 children (3 boys), median age 14.4 years, range 8.7–16.6 years, were issued with MINOs. At stage 3, 5 reported a good clinical response to i.m. triamcinolone (subjective improvement in symptoms, no courses of oral steroids); 5 reported a partial response (improvement in symptoms for ⩽2 weeks) or poor response (no improvement in symptoms and/or requiring oral steroids prior to review).
Conclusion: Children with difficult asthma who have an improvement in their clinical symptoms following systemic steroids appear to have an immediate fall in FeNO50 which is then sustained over a period of at least 2 weeks. This is also reflected in a fall in sputum eosinophils. In those with a poor or no response, although the FeNO50 appears to drop initially it soon rises again, and there can be day to day variability. If measurements of FeNO50 are used as a marker of inflammation and hence response to steroids, the timing of the measurements needs to be taken into account and greater information may be gained from more frequent measurements.
Lung cancer staging and surgery
IMPACT OF FDG-PET SCAN ON THE PREVALENCE OF BENIGN LESIONS AT THORACOTOMY
K. Mohan, J. Mcshane, R. Page, M. J. Ledson, M. J. Walshaw. The Cardiothoracic Centre-Liverpool, UK
Introduction: FDG-PET scan is increasingly used to diagnose malignant pulmonary lesions, and a “positive” scan (standardised uptake value, SUV >2.5) has a high specificity for lung cancer. However, a number of these scans may be falsely positive, such that patients with benign lesions may be subjected to unnecessary surgery.
Methods: To test the impact of FDG-PET on the (false) operative rate for benign lesions, we compared their prevalence at surgery for two consecutive two-year groups: patients undergoing surgery in 2003–5 (before FDG-PET availability) with those after its introduction (2005–7). We reviewed clinical, radiological and histological data on patients with resected benign lesions where the scan had been misleading.
Results: 1233 consecutive patients underwent focal pulmonary lesion resection: between 2003–5, 44/626 were benign (7%). 301 of 607 patients (50%) resected during 2005–7 underwent FDG-PET: in 18 (6%) the histology was benign despite a “positive” scan. There was no difference in resection rates for benign lesions pre and post commencement of the use of FDG-PET (χ2 = 0.358, p = 0.5). The latter group of patients had a mean age 61 years (49–74), 17 (94%) were smokers (mean 42 pack-years), 6 (33%) had asbestos exposure and 11 were male. In addition to bronchoscopy, 4 had undergone a non-diagnostic CT guided biopsy and 2 a negative rigid bronchoscopy. At CT scan, the mean size of the lesion was 2.6 cm (1–5), 89% had a solid consistency and 55% had irregular margins. Mean FDG-PET SUV was 4.8 (2.6–12.7). However, following thoracotomy (9 lobectomies, 8 wedge resections and 1 open & close (biopsy)); the final pathological diagnoses were tuberculosis (3), COP (2), fibrosis (2), aspergilloma (2), rheumatoid nodule (2) hamartoma (1), chronic inflammation (1), bulla (1), infarct (1), abscess (1) and ILD (1).
Conclusion: Thus, we have shown that the use of a new advanced imaging technique (FDG-PET) does not prevent unnecessary thoracotomies in patients who ultimately have benign lesions: the rate of these did not change following its introduction. This study illustrates the continuing difficulty in managing patients with suspected chest malignancy, where many patients have existing comorbidities which complicate the diagnostic process.
DOES THE USE OF PREOPERATIVE CT-PET IMPROVE THE SURGICAL MANAGEMENT OF THE SOLITARY PULMONARY NODULE?
M. H. Chamberlain, A. Martin-Ucar, S. Muller, J. Entwistle, D. A. Waller. Glenfield Hospital, Leicester, UK
Background: The availability of positron emission tomography (CT-PET) in our practice has altered the strategy for the investigation and management of the solitary pulmonary nodule (SPN). There is still debate whether the additional information from CT-PET alters surgical management if an aggressive excisional biopsy strategy is already employed.
Objectives: We aimed to evaluate if basing the decision to operate on a positive preoperative CT-PET increased the yield of malignant SPN at excisional biopsy.
Methods: Patients were offered CT-PET followed by video assisted thoracoscopic (VATS) excision with intraoperative frozen section if the CT-PET was positive. Percutaneous biopsy was not performed. Over a 30-month period, 24 patients underwent excisional VATS biopsy of a SPN following a positive CT-PET scan (PET group). Outcome was compared with 24 case-matched patients who had undergone VATS excision of SPN prior to the introduction of CT-PET (NON-PET group) based on CT scan alone. Cases were matched according to age, sex and lobar position of SPN. Histological diagnosis and immediate outcome of the two groups following surgery was compared.
Results: Each group comprised 14 female and 10 males, mean age 68 (range 49–84) years. In the PET group, 87% (21/24) of resected nodules were malignant (52% adenocarcinoma, 38% squamous) which was significantly higher than the 58% (14/24) in the NON-PET group, (p = 0.02). In the NON-PET group the 10 benign SPN included: granulomata, hamartomata and an aspergilloma. In the PET group the benign SPN were all granulomata. In both groups 58% underwent VATS resection and 42% open lobectomy. There were no false-positive frozen section results and no resection was performed for benign disease. Pathological stage distribution for PET vs NON-PET was: stage I (38% vs 63%), stage II (33% vs 0%), and stage III (5% vs 37%). Five SPN (24%) in the PET group were found to be metastastic. There was no operative mortality in either group.
Conclusion: Our early results support the routine use of CT-PET in the preoperative management of SPNs and question the additional benefit of obtaining preoperative histological confirmation.
IS SURGERY CONTRAINDICATED FOR PATIENTS WITH SMALL CELL LUNG CANCER AND CLINICAL N2 DISEASE?
E. Lim, E. Belcher, Y. K. Yap, A. G. Nicholson, P. Goldstraw. Royal Brompton Hospital, London, UK
Background: Chemo-radiation is considered the gold standard for the management of limited disease small cell lung cancer (SCLC) but cumulative results from 25 years of North American chemo-radiation trials report median survival of 17 months and data from the Surveillance, Epidemiological and End results programme report an overall five-year survival of 10%. In general, surgery as a treatment option has been abandoned because of poor overall survival, but many small series report good results (in selected patients). Currently only patients with very limited early stage disease are offered surgery as an option. We sought to determine survival across a spectrum of T and N stage to explore the impact of complete surgical resection for SCLC.
Methods: A retrospective review was undertaken of patients who underwent surgery between 1980 and 2006. Patients were staged according to the 6th edition of the TNM classification of lung cancer, and actuarial survival estimated with Kaplan-Meier methods and comparisons undertaken using Cox regression.
Results: We identified 59 patients who underwent complete resection with nodal dissection for SCLC. The mean age (SD) was 62 (11) years and 41 (69%) were men. Clinical staging information was available in 53, listed by stage with IA (n = 9), IB (n = 21), IIA (n = 0), IIB (n = 13), IIIA (n = 9), IIIB (n = 1). The median time to follow-up (1st to 3rd quartile) was 2.8 (0.79–8.65) years with an overall survival (95% CI) at 1 and 5 years of 76% (65 to 88), 52% (40 to 68). There were no clear differences in the survival of patients in clinical T categories (p = 0.366) and good overall results in patients across the spectrum of nodal disease from N0 to N2 (p = 0.498).
Conclusion: Our results demonstrate excellent survival for stage I to III patients who underwent lung resection with nodal dissection for SCLC. With improved preoperative and intraoperative staging these results supports the need to re-evaluate surgery as primary treatment and the use of conventional clinical TNM criteria in the selection of patients with very limited disease for surgery. The presence of clinical N2 disease per se should not be a contraindication to surgery.
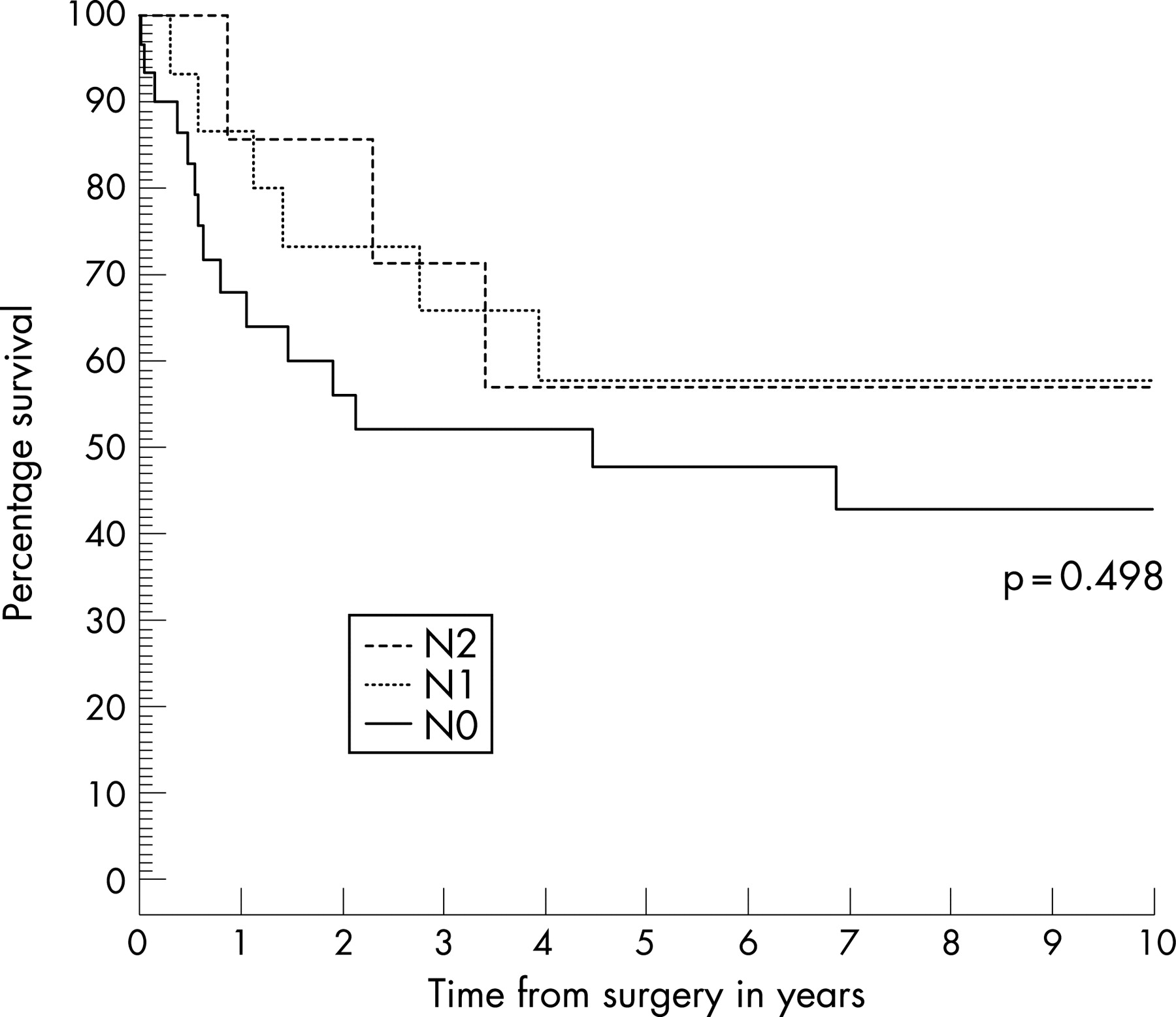
IMPLICATIONS OF ENDOBRONCHIAL ULTRASOUND-GUIDED TRANSBRONCHIAL NEEDLE ASPIRATION OF MEDIASTINAL LYMPH NODES FOR STAGING LUNG CANCER: A COST AND TIME-TO-TREATMENT PROJECTED ANALYSIS
M. E. J. Callister, A. Gill, P. K. Plant. St James’s University Hospital, Leeds, UK
Introduction: Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) of mediastinal nodes is a safe, effective technique for lung cancer staging. It may reduce the number of mediastinoscopies and PET scans performed, and reduce time from referral to treatment. Leeds Teaching Hospitals (LTH) does not currently offer an EBUS-TBNA service. By reviewing mediastinoscopies performed as staging procedures for lung cancer during 2006, we sought to determine the implications of establishing a service from both cost and time-to-treatment perspectives.
Methods: We determined the proportion of staging mediastinoscopies positive for malignancy, and the sensitivity of EBUS-TBNA for malignancy according to published series. We estimated the number of mediastinoscopies and CT-PET scans that would be avoided by EBUS-TBNA. The fixed equipment costs of EBUS-TBNA were determined. NHS tariff and unit-based costs were calculated for mediastinoscopy, PET and EBUS-TBNA. The cost implications for the local NHS and for LTH trust were estimated. Time between initial bronchoscopy and mediastinoscopy was determined for patients referred from within the trust.
Results: Of 47 staging mediastinoscopes performed, 27 showed malignant disease. Sensitivity of EBUS-TBNA for malignancy was 92.3%. Fixed equipment costs for EBUS-TBNA were £104,465 over five years. Tariff payments were £2157 and £975 for mediastinoscopy and PET respectively. EBUS-TBNA does not currently attract an additional payment above standard bronchoscopy. Unit-based costs for mediastinoscopy and EBUS-TBNA (projected) were £2464 and £561 respectively. PET-CT is provided by an independent contractor. We estimated EBUS-TBNA would result in an NHS budget saving of £65,086 per year (19 months to recover fixed cost). Taking into account NHS tariff payments and referral routes of patients to LTH, an EBUS-TBNA service would save LTH trust £6336 per year (16 years to recover fixed cost). EBUS-TBNA would reduce time from referral to treatment for internal referrals by a mean of 31 days (median 19 days).
Conclusion: EBUS-TBNA offers significant time reductions between referral and treatment for lung cancer patients. It is cost effective for the NHS as a whole, but the current tariff structure acts as a disincentive for trusts to establish a service. This analysis would support the introduction of an additional tariff for EBUS-TBNA to encourage greater uptake of this technique.
ENDOBRONCHIAL ULTRASOUND: A COMPARATIVE STUDY BETWEEN CONVENTIONAL TBNA AND EBUS-GUIDED TBNA
R. Naseer1, W. L. Williams2, J. Howells1, J. Edwards1, J. Mills1, M. Munavvar1. 1Lancashire Teaching NHS Trust; 2University of Manchester, UK
Introduction: Prognosis is related to the stage of lung cancer and therefore effective staging procedures are required to help determine treatment and prognosis. Many lung cancers usually metastasise to hilar and mediastinal lymph nodes first and so sampling of these play an important role. Conventional transbronchial needle aspiration (c-TBNA) was first used in the 1980s to increase the yield of bronchoscopic procedures. It is still a relatively underused procedure with only one third of chest physicians performing the procedure (Munavvar M et al. Survey of the Practice of Interventional Bronchoscopy in the UK. Thorax 2004;59(Suppl II); c-TBNA yield can vary between 20–80% and is dependent on operator experience and site of lesion. Endobronchial ultrasound (EBUS) was first developed in Japan in the mid 1990s to more accurately image mediastinal lymph nodes. This procedure is performed using a specially designed curved linear array bronchoscope with a transducer at the tip to perform EBUS guided TBNAs, to try and further increase the yield of bronchoscopic procedures, and so far has shown good results (Yasufuku K et al, Chest 2004;126:122–8; Rintoul RC et al, Eur Res J 2005;25:416–21; Herth FJ et al, Thorax 2006;May 31-epub). In this retrospective study we looked to compare the diagnostic yield of c-TBNA and EBUS-TBNA in a Lancashire Teaching Hospital. We also looked at whether the lymph node station from which the EBUS-TBNA was taken alters diagnostic yield.
Methods: The EBUS service was started in May 2006. We looked at all the bronchoscopy reports of patients who had EBUS-TBNA between May 2006 and May 2007 and recorded the site of sample (selected by CT appearances) and cytology results. We then compared this with all the c-TBNAs done between May 2004 and May 2005. All procedures were performed by a single operator (MM) and done in the endoscopic suite of a teaching hospital. The c-TBNA and EBUS-TBNA results were compared to the lung cancer MDT result and a diagnostic yield was defined as correlation between the final diagnosis at the MDT and the TBNA findings (that is, diagnostic yield includes both true positives and true negatives)
Results: Endoscopy-related complications included two self-limiting bleeding episodes (one in each group) and one patient in the EBUS group with excessive coughing. None of the complications required further treatment. In the c-TBNA group there were 33 patients (22 male, 11 female) with a mean age of 65.1. The EBUS-TBNA group contained 52 patients (38 male, 14 female) with a mean age of 64.2. In the EBUS group, two patients had no samples taken due to intolerance to the procedure. Three patients in the EBUS group were from a different Trust and were not discussed at our MDT and therefore were excluded, as no final diagnosis was available. EBUS samples were taken from different nodal areas: left hilar (LH), right hilar (RH), right paratracheal (RP), subcarinal (SC), mass (M), or other—not stated in notes (O). Diagnostic yield: c-TBNA, 42% (14/33); EBUS-TBNA, 66% (31/47).
Conclusion: EBUS guided TBNA in this study increased the diagnostic yield of TBNAs by 24%, which is a relative increase of more than 50%. Therefore we can conclude that EBUS-TBNA is a better diagnostic choice of bronchoscopic procedure where available. However c-TBNA still has an important role to play as it helps increase the yield of routine bronchoscopic procedures. Both c-TBNA and EBUS-TBNA are relatively safe procedures and reduce the need for invasive methods of lymph node sampling, which are more expensive, complicated and have greater risks associated with them. Site-dependent yield for EBUS-TBNA does seem to vary, with lymph node sampling from the left hilar region and subcarinal region providing the greater yield.
Techniques and outcomes in bronchoscopy and lung biopsy
THE USE OF THE DIODE LASER IN THERAPEUTIC BRONCHOSCOPY: AN INTEGRAL PART OF MODERN RESPIRATORY PRACTICE
M. W. Khalil, A. Bagga, S. A. Solly, D. A. Waller. Glenfield Hospital, Leicester, UK
Objective: To review the impact on clinical practice of our five-year experience with therapeutic laser bronchoscopy.
Methods: Between 2002 and 2007 a total of 120 bronchoscopic laser procedures were carried out in our centre. During the experience, the number of laser procedures done by our unit has been steadily increasing to a current rate of 28 procedures in the present year (2007). The diode laser was used in all of our cases in a standard operating theatre with the patient under general anaesthesia in conjunction with interventional radiologists where necessary. The patient population, indications for treatment and immediate results were retrospectively analysed.
Results: A total of 120 procedures were performed on 84 patients (62% male), mean age 65.9 (30–86 years). The mean energy dosage was 4264 (310–12545) J. Ablation was performed in the main bronchi in 58 procedures, the trachea in 31, combined trachea and right main bronchus in 4, and lobar bronchi in 27. The main indication for treatment was primary lung cancer with 51 procedures including: 29 for inoperable tumours to achieve symptom control; 15 for recurrence of tumour after previous lung resections and 7 in patients thought to be inoperable who subsequently went to resection. Benign inflammatory stenoses formed the next most common indication with 45 procedures, including 12 following previous lung resections and 8 following tracheostomy. A single laser bronchoscopy was successful in treating the presenting problem in 73% of cases; 36 repeat procedures were carried out on 23 patients. Benign stenosis was also the most common indication for repeat laser ablation (23 procedures). Benign tumours, including carcinoids, were removed in 12 procedures. Eight procedures included concomitant insertion of airway stents. Complications related directly to the procedure were rare: one patient bled requiring re-bronchoscopy and resuscitation, and one developed pneumothorax which resolved. The average hospital stay was three days. There were no hospital deaths.
Conclusion: Therapeutic bronchoscopy is an invaluable and integral part of modern respiratory practice. The use of the diode laser under general anaesthetic has allowed for safe treatment of virtually all indications.
PHYSICIAN AND PATIENT PERCEPTION OF TOLERANCE TO FIBREOPTIC BRONCHOSCOPY
M. Thirumaran, S. Faruqi, S. P. L. Meghjee, P. Blaxill, S. E. Williams. Pinderfields General Hospital, Mid Yorkshire Hospitals NHS Trust, UK
Introduction: Fibreoptic bronchoscopy (FOB) is a commonly performed invasive diagnostic procedure. Despite the direct relevance to the patients, there is paucity of data regarding patients’ experience of FOB and the factors affecting the same. The patients’ experience of health care is recognised as a valid and significant outcome of care. The objective of this study is to assess the patient’s perception of comfort during FOB and compare that with the physician’s perception of patients’ tolerance to the procedure. Other factors which could influence tolerance were also assessed.
Methods: A structured questionnaire was used to collect data from the patients undergoing FOB and the physicians performing it. This questionnaire included tolerance score of 1–5, 5 being very comfortable. Data regarding other factors which may have a bearing on the tolerance of the procedure like dose of Midazolam, performance status, route of intubation were included on the questionnaire. Informed consent was obtained. The physician performing the FOB filled in the questionnaire immediately after the procedure.
Results: Sixty three patients agreed to participate in the survey and 37 returned questionnaire (males, 25). The response rate was 59%. The general tolerance to the procedure was very good with the mean patient’s tolerance score being 4.2. This was not significantly different from physicians perception of patients tolerance, 4.3 being their mean score. 73% of patients who received more than 3 mg of Midazolam gave the best rating of 5. Among those who received 3 mg or less only 27% rated the procedure very comfortable. Patients with better performance status found the procedure more comfortable. Age, route of intubation and person performing the procedure (Specialist Registrar or Consultant) did not influence patients’ comfort. Surprisingly 38% of the patients remembered most of the details of the procedure. The mean duration before the patients felt their normal self was 8 h. All the patients said if necessary they will be happy to have the procedure done again.
Conclusion: Contrary to general perception, FOB is a reasonably well-tolerated procedure. The perception of comfort by the patient and the physician performing the procedure are similar. Higher doses of Midazolam and better performance status had a positive correlation with patient’s tolerance of the procedure.
CT-GUIDED LUNG BIOPSY: 150 CASE REVIEW
M. Asim, N. Sinnott, S. Durairaj, A. Prakash, C. M. Smyth, M. J. Walshaw. The Cardiothoracic Centre Liverpool, UK
Introduction: Percutaneous CT-guided lung biopsy can aid the diagnostic yield in patients with suspected lung cancer where bronchoscopy is unhelpful. We were interested in assessing the diagnostic and complication rate using this technique in our large lung cancer unit (400 cases per year).
Methods: We audited the last 150 CT-guided percutaneous lung biopsies (mean patient age 70 years (range 25–90), mean FEV1 73% (range 24–131)), 79 male), looking for delays in access, the type of biopsy and number of samples taken, the grade of the operator, and any complications.
Results: Mean time from request to biopsy was 7.8 days (range 0–34). 147 were performed as outpatients, using day case facilities. Biopsies were taken using a co-axial needle in 132 cases (88%): 86 (57%) by single pass, 24 (16%) two-passes and 3 (2%) three-passes. 83 biopsies (55%) were performed by consultant radiologists who biopsied smaller and deeper lesions than junior staff (p<0.01). All patients had a chest x ray (mean time 1.3 h (range 1–3) post-biopsy). 45 patients (in 32 the operator was a consultant radiologist) had a pneumothorax on this film, not related to the patient’s pulmonary function, age or gender, or the number of passes or chest wall thickness. The pneumothorax rate was greater in those with smaller lesions (p<0.001) and in those further from the chest wall (p<0.001). Treatment was conservative in 29 cases (62%), by aspiration in 7 (13%) and via intercostal tube drainage in 9 (20%). There was minimal pulmonary haemorrhage in 6 patients (4%) but none required blood transfusion. No patient had an air embolism or haemothorax, and there were no deaths. As regards diagnostic yield, 108 (72%) were positive for malignancy.
Conclusion: More technically difficult biopsies are associated with a higher complication rate and tend to be done by the more experienced radiologists (consultants). The diagnostic yield is similar to that reported in the literature. This technique is suitable for outpatients using a day case facility and can help to speed up the diagnostic pathway for patients with suspected lung cancer.
INTRODUCING LIQUID BASED CYTOLOGY INTO ROUTINE BRONCHOSCOPY FOR PATIENTS WITH SUSPECTED LUNG CANCER
C. Bloom, F. A. Mauri, A. R. Benjamin, E. F. Bowen. Hammersmith Hospitals NHS Trust, London, UK
Introduction: The introduction of liquid based cytology (LBC, ThinPrep) in 1996 increased the sensitivity of cervical smear evaluation. This increase is related to a number of factors: the preservation of cellular architecture, smaller requirement of sample size immunocytochemical staining, automatic fixation and machine analysis of the sample, and reduced compromise from excessive blood. LBC has been successfully applied to other cancers such as colorectal, breast and renal. Only case reports and small studies allude to the usefulness of LBC in bronchoscopic samples.
Methods: In 2006 LBC was introduced into our Trust for non-gynae cytology. We undertook to apply LBC within bronchoscopy for cytological samples taken from patients with suspected lung cancer. Using LBC, cytology brushings and TBNA samples were placed directly into ThinPrep solution as opposed to staff making smears of each directly onto slides for fixing. The cytology brush was cut off and left in the vial. If a BAL was heavily blood stained an aliquot of the lavage was placed into the LBC vial. We audited the first year’s results and compared them to historical data from 2003–4 when brush and TBNA samples were smeared by hand onto slides by nursing staff and fixed. All lists during both reporting periods were supervised by the same consultants and all patients underwent a CT before bronchoscopy.
Results: The introduction of LBC into the routine use of bronchial brushings and TBNA samples has resulted in an improved diagnostic rate by these modalities. There has been an improvement in bronchoscopist and nurse assistants’ time and safety. It was time consuming to make slides and there were issues about poor slide preparation and drying artefacts. Placing the TBNA needle directly into LBC rather than over multiple slides reduces the chance of possible needle stick injury and inhalational exposure. The small additional cost of LBC (£10 per sample) is offset by the increased diagnostic rate and subsequent reduction in additional invasive procedures.
Conclusion: We have shown that LBC can enhance the endobronchial diagnosis of lung cancer when applied to bronchial brushings and TBNA samples. This change in practice is safe, time and cost efficient.
DIAGNOSTIC VALUE AND RISKS OF TRANSBRONCHIAL LUNG BIOPSIES
M. Murray, A. Hill. Royal Infirmary of Edinburgh, Edinburgh, UK
Aims: The aim of this study was to assess the diagnostic value and risk of transbronchial lung biopsies (TBB).
Methods: The authors retrospectively evaluated TBB carried out in the Royal Infirmary of Edinburgh between 2001–6. Outcomes included complications (risk of pneumothorax, life-threatening haemoptysis, admission with pneumonitis or death) and the percentage of transbronchial lung biopsies that confirmed the final diagnosis.
Results: 75 patients had undergone investigation with tranbronchial lung biopsies. The mean (SD) age was 52.7 (14.3) years and the mean number of tranbronchial lung biopsies taken was 4.2 (1.9). 10.7% developed a pneumothorax within 24 h of the biopsies. Of these, 37.5% required an intercostal chest drain. All pneumothoraces resolved and no patients required thoracic surgical intervention. There were no episodes of major haemoptysis, no admissions with pneumonitis and no mortality. The diagnostic accuracy of TBB is shown in the table. No patients with usual interstitial pneumonia (UIP) had TBB. A definitive diagnosis was achieved by TBB in 77%. 21% patients needed other procedures for a definitive histological diagnosis. A further 2% had samples that were insufficient for examination and were not further investigated.
Conclusion: In conclusion, transbronchial lung biopsies were found to be a safe procedure with the main complication being pneumothorax, although all these were manageable without surgical intervention. TBB had a high diagnostic yield except in patients with vasculitis and no patients with UIP were investigated in this study.
RANDOMISED CONTROLLED TRIAL OF THE EFFECT OF STANDARD AND DETAILED CONSENT FORMS FOR BRONCHOSCOPY ON PERI-PROCEDURE ANXIETY AND SATISFACTION
M. Uzbeck, I. Saleem, C. Quinn, P. Cotter, S. O’Keeffe, J. J. Gilmartin. Merlin Park University Hospital, Galway, ROI
Introduction: Deciding what risks to disclose prior to a procedure is often challenging for clinicians. Although patients must receive sufficient information to make a decision, undue emphasis on rare complications may lead to anxiety and discourage patients from accepting beneficial interventions. Also, a significant proportion of patients ask not to be informed of all risks. We compared the effects of using a standard and a more detailed consent form on anxiety and satisfaction levels in patients undergoing elective bronchoscopy.
Methods: Consecutive patients who agreed to participate underwent a baseline assessment consisting of the Degner Control Preferences Scale and a 100 mm anxiety visual analogue scale (VAS). They were randomised to the standard or explicit information sheet and given 30 min to read it. The VAS was then repeated. Following the procedure, they completed a post-procedure satisfaction questionnaire consisting of four questions on a five-point Likert scale.
Results: Of 132 patients asked, 120 agreed to participate and 117 (73 men, mean age 57.5 years and 35% aged 65 years or more) completed the study. At baseline, there were no significant differences between the groups in demographic data in indications for bronchoscopy or in anxiety or information preference scores. Those who received the explicit form were significantly more anxious at the second assessment (mean (SD) VAS 52.5 (30.5) vs 41.0 (28.3); p = 0.04) and, although satisfaction levels were high in both groups, reported significantly less satisfaction (5.4 (2.7) vs 4.4 (2.4); p = 0.03).
Conclusion: Although the goal of adequate informed consent may demand giving more information about risks to patients about interventions, this may come at the cost of increased patient anxiety and less satisfaction.
Pulmonary fibrosis: clinical observations
SIX MINUTE WALK DESATURATION AND MAXIMAL EXERCISE TEST PARAMETERS: RELATION IN PATIENTS WITH FIBROSING LUNG DISEASE
T. J. Corte1, S. J. Wort1, S. Nogrady2, D. Ip1, R. Ellis1, A. U. Wells1. 1Royal Brompton Hospital, London, UK; 2Australian National University, Canberra, Australia
Introduction: Six-minute walk testing (6MWT) is a reproducible prognostic marker for patients with idiopathic interstitial pneumonia (IIP). Oxygen desaturation below 89% during 6MWT has been associated with a much poorer prognosis in patients with IIP. Though the reason for this finding is unclear, it has been suggested that exercise desaturation may denote the development of pulmonary vascular damage, resulting in pulmonary hypertension on exercise (PH). We examine the relation between 6MWT and other key echocardiographic and physiologic markers.
Methods: All patients (n = 92) with fibrosing lung disease who had both 6MW and maximal exercise testing performed concurrently between 2005 and 2007 were included. All patients studied also had concurrent resting pulmonary function tests and echocardiography.
Results: Diagnoses included idiopathic pulmonary fibrosis, n = 10; non-specific interstitial pneumonitis, n = 38; organising pneumonitis, n = 6; chronic hypersensitivity, n = 8; sarcoidosis, n = 8; other, n = 22): mean DLco 53 (13)%; mean FVC 79 (20)%. Three of 51 (6%) had PH on echocardiography (median right ventricular systolic pressure (RVSP) 29.3 mmHg (14.3–83), pulmonary acceleration time (PAT) 126 ms (70–225)). Patients who desaturated to below 89% on 6MWT had (1) higher RVSP (p = 0.03); (2) higher resting AaDO2 (p = 0.02) and Vd/Vt (p = 0.02); (3) higher exercise AaDO2 (p<0.0001), AaDCO2 (p<0.01), Vd/Vt (p = 0.02); (4) lower DLco (p<0.0001), FVC (p = 0.003). End 6MW oxygen saturation correlated with (1) RVSP (r = −0.49, p<0.001); (2) resting AaDO2 (r = −0.33, p<0.01) and Vd/Vt (r = −0.37, p<0.001); (3) maximal exercise PaO2 (r = 0.48, p<0.0001), AaDO2 (r = −0.43, p<0.0001) and Vd/Vt (r = −0.28, p<0.01) and (4) resting pulmonary function (TLC r = 0.34, p<0.01; DLco r = 0.44, p<0.0001; FEV1 r = 0.4, p<0.001, FVC r = 0.35, p<0.001). RVSP also correlated with resting Vd/Vt (r = 0.46, p<0.001) and DLco (r = −0.44, p<0.01), and maximal exercise variables (PaO2 (r = −0.46, p<0.001), AaDO2 (r = 0.49, p<0.001), Vd/Vt (r = 0.49, p<0.001)).
Conclusion: Desaturation below 89% in a 6MWT in diffuse lung disease is associated with more severe functional impairment, higher RVSP, and greater impairment of markers of pulmonary vascular compromise at rest (Vd/Vt) and on exercise (Vd/Vt, AaDCO2). These findings provide indirect support for the hypothesis that desaturation during 6MWT in diffuse lung disease is indicative of pulmonary vascular decompensation.
LUNG TRANSPLANTATION FOR IDIOPATHIC PULMONARY FIBROSIS: RECIPIENT CHARACTERISTICS AND SURVIVAL OUTCOMES IN A SINGLE CENTRE 1987–2007
D. Cooper, J. Kerr, G. Parry, J. H. Dark, J. Lordan, P. A. Corris, A. J. Fisher. Cardiopulmonary Transplant Unit, Freeman Hospital, Newcastle upon Tyne, UK
Introduction: Lung transplantation is the only treatment modality proven to offer a survival advantage to patients with end-stage lung disease due to idiopathic pulmonary fibrosis (IPF). Donor organ shortage limits availability of transplantation for patients with IPF. The International Society of Heart and Lung Transplantation (ISHLT) registry notes a poorer outcome post-transplant in this group compared to cystic fibrosis or COPD. In this study we evaluated our centre experience of lung transplantation for IPF.
Methods: A retrospective review was performed to identify demographics, pre-transplant physiology (Spirometry, TLCO, PaO2 and PASP), functional status (6 minute walk distance) and pre-transplant drug therapy. Subsequently, length of post-transplant survival for each patient was determined.
Measurements and Main Results: Between September 1987 and February 2007, 79 patients (55 males, 24 females) underwent 55 single, 19 bilateral and 2 heart-lung transplantations for IPF. Median age at transplant was 53.9 years (25.6–64.7). Mean pre-transplant pO2 7.88 (1.96), median 6 minute walk distance 210 m (15–570 m), with a median desaturation to 75% (56–91%). Median PASP was 50 mmHg (28–103 mmHg), FEV1 1.5 l/min (0.5–2.75), FVC 1.7 l/min (0.7–4.45) and TLCO 32% predicted (15–49%). Survival analysis shows worse outcome for IPF lung transplant recipients compared to our whole cohort at this centre (fig). Mean survival was 2.76 years (3.47). However, our 50% survival appears higher than current ISHLT data.
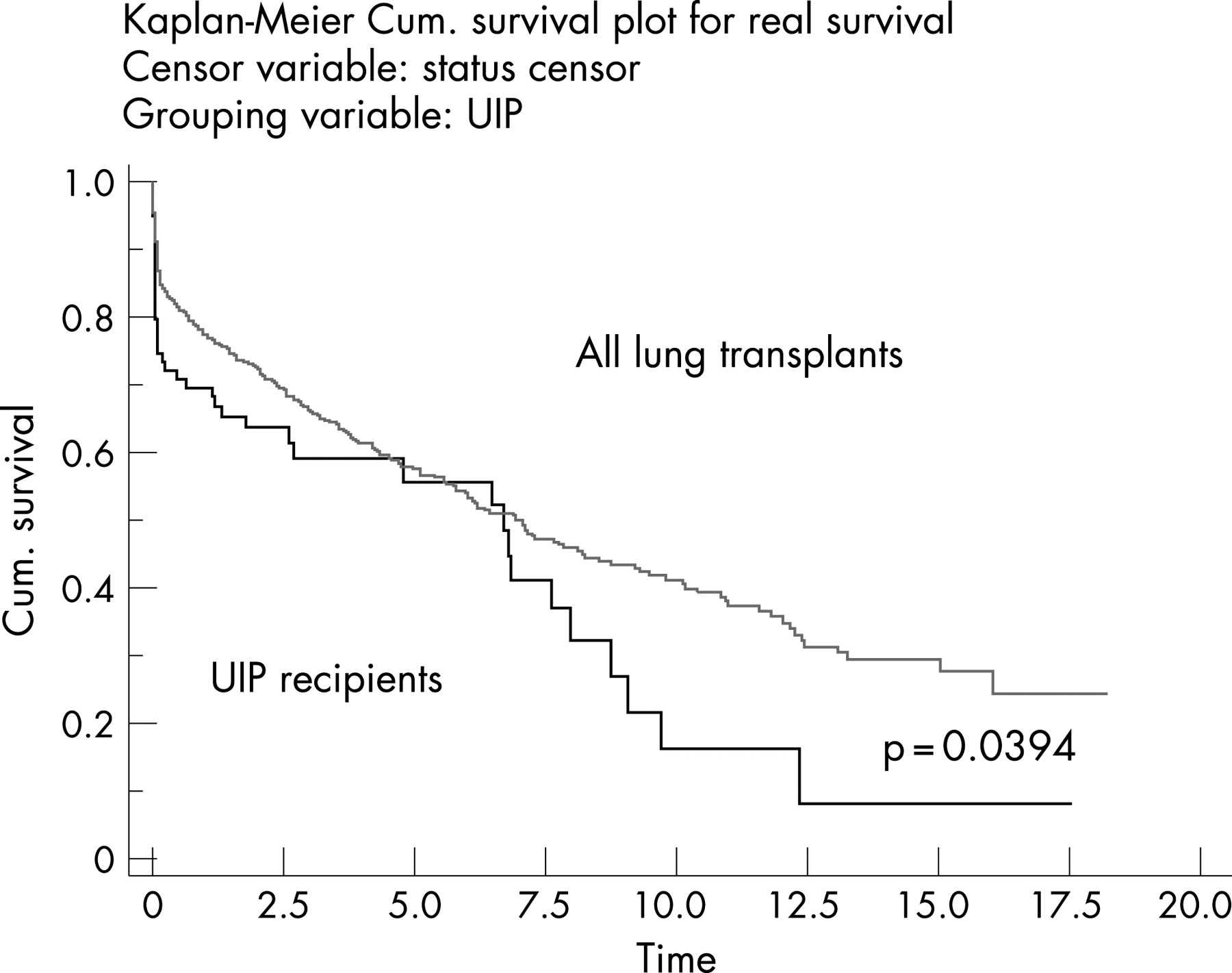
Conclusion: Despite the increased age and comorbidity in this group, meaningful post-transplant survival can be achieved in experienced single centres.
THE RISK OF ACUTE CORONARY SYNDROMES, CEREBROVASCULAR ACCIDENTS AND DEEP VEIN THROMBOSES IN PEOPLE WITH IDIOPATHIC PULMONARY FIBROSIS AND THE GENERAL POPULATION
I. Le Jeune, C. Smith, J. Gribbin, A. Fogarty, R. Hubbard. University of Nottingham, Nottingham, UK
Background: People who have factor V Leiden homozygosity have an increased tendency to clot and also to have restricted lung function.1 This raises the possibility that an increased tendency to clot may be a risk factor for diseases such as IPF. To investigate this further we have quantified the risk of acute coronary syndromes (ACS), cerebrovascular accidents (CVA) and deep vein thromboses (DVT) in people with IPF in comparison to the general population.
Methods: We used The Health Improvement Network (THIN) to identify a cohort of incident cases of IPF and four controls per case matched by age, sex and general practice. We then identified all recorded diagnoses of ACS, CVA and DVT and compared the occurrence of these outcomes between cases and controls before the date of diagnosis of IPF (or appropriate matched date for controls—hereafter termed the index date). We then compared the incidence of new, first time occurrence of these outcomes in the two cohorts after the index date.
Results: The mean age of cases at diagnosis was 71 years and 62% of cases were male. In the time before the index date the risk of having either a DVT or an ACS was increased in people with IPF, but no increase in CVA was present. During the follow-up period there was a marked increase in the incidence of ACS and DVT in people with IPF and a more modest increase in the risk of CVAs.
Conclusion: People with IPF have a marked increased risk of having an ACS or a DVT. These increases may reflect an adverse effect of IPF on these outcomes but could also reflect a common risk factor, such as hypercoagulability, which in turn may highlight a new treatment opportunity for people with IPF.
DOES BODY MASS INDEX INFLUENCE INFLAMMATION AND PLASMA LIPIDS IN PIGEON FANCIERS’ ALLERGIC ALVEOLITIS
S. Brennan1, I. Fraser2, L. Jolly2, C. Lynch2, L. Urquhart2, N. Sattar3, M. R. Adamson1, C. Mcsharry2, K. Anderson1. 1Crosshouse Hospital, Kulmarnock; 2Immunology, University of Glasgow; 3Biochemistry, University of Glasgow, UK
Background: Hypersensitivity pneumonitis (HP) is an immune-mediated interstitial inflammatory disease. The lymphocyte and antibody responses to inhaled antigens appear necessary but not sufficient for disease, and other susceptibility factors are unidentified. The presence of “foamy” lipid-laden histiocytes and lipid clefts in the lung suggests that lipid metabolism may contribute to disease.
Methods: We measured plasma lipids, oxidised-LDL, and body mass index (BMI, kg/m2) in non-smoking 48 pigeon fanciers (23 with symptoms of EAA), and investigated their association with symptoms of EAA and the IgG antibody (μg/ml) to inhaled avian antigen and C-reactive protein (CRP) (μg/ml) (measured by enzyme-immunoassay) and the lipid profile by nephelometry (mmol/l).
Results: Pigeon fanciers with EAA had higher levels of IgG antibody to avian antigen (39.0 (22.2–54.7), 12.0 (2.5–46.0), p<0.01), higher CRP levels (2.8 (1.6–8.0), 1.7 (1.2–6.4, p<0.05), and a trend to higher BMI than those without (mean (SD)) 28.70 (4.97) and 25.52 (4.35), p = 0.078. The BMI levels correlated with CRP (r = 0.353, p = 0.035), with ox-LDL (r = 0.423, p = 0.010), and a trend to higher antibody (r = 0.278, p = 0.1).The plasma triglyceride levels correlated with CRP (r = 0.31, p = 0.008) and IgG antibody (r = 0.32, p = 0.006), and the cholesterol level correlated with the IgG antibody titer (r = 0.32, p = 0.006). There was no significant association between BMI and cholesterol (r = 0.132, p = 0.444), triglyceride (r = 0.157, p = 0.359) and HDL-C (r = −0.183, p = 0.285).
Conclusion: Interstitial foamy histiocytes in HP suggest altered lipid metabolism in this disease. We have found significant changes in the serum lipid profile of pigeon fanciers associated with inflammation (measured by CRP) and specific antigen sensitisation (measured by IgG antibody). The results suggest that HP has a systemic inflammatory component, with factors including BMI and altered lipids which in some way contribute to the pulmonary pathology.
AMBULATORY OXYGEN IN IDIOPATHIC PULMONARY FIBROSIS: OF WHAT BENEFIT?
S. Hicks, L. G. Spencer, A. Duck, E. Barnett, C. T. Leonard. Wythenshawe Hospital, Manchester, UK
Introduction: Exercise limitation/exercise-induced breathlessness is a key problem which limits activities of daily living and reduces self-reported quality of life in patients with idiopathic pulmonary fibrosis (IPF). Ambulatory oxygen (amb O2) is widely prescribed for IPF patients but benefits gained from this practice have not been reported. We set out to assess the benefits of amb O2 in 70 IPF patients in terms of walking distance and dyspnoea (Borg) score.
Methods: Retrospective case note study (n = 70) of IPF patients who were assessed for amb O2 using 6-minute walk test (6MWT) at our hospital between 2004–7. IPF diagnosis was as ATS/ERS guidelines. Data were collected on distance walked, O2 saturations (SpO2) and Borg score pre- and post-test. Forty one patients were already using O2 pre-amb O2 assessment and performed a baseline 6MWT with O2. Reasons for O2 use pre-amb O2 assessment included long-term oxygen therapy, PRN or amb—but need for reassessment identified. Twenty nine patients were not using O2 and performed baseline 6MWT without O2. All patients were required to have resting PaO2 levels >8 kPa to commence test. During walking, if SpO2 fell <90% the test was terminated, patients rested, then test repeated with increased O2 flow rates (2 l/min increments). This procedure continued until patients did not desaturate <90%; that is, optimal O2 flow rates were achieved (optimal O2 walk test).
Results: Patients not on O2 pre-test managed to walk a statistically and clinically significant 81.2 m (mean) further using optimal O2 therapy. Patients already on O2 walked an extra 16.9 m (mean). Borg scores at test end were not statistically different using optimum O2 compared to baseline tests.
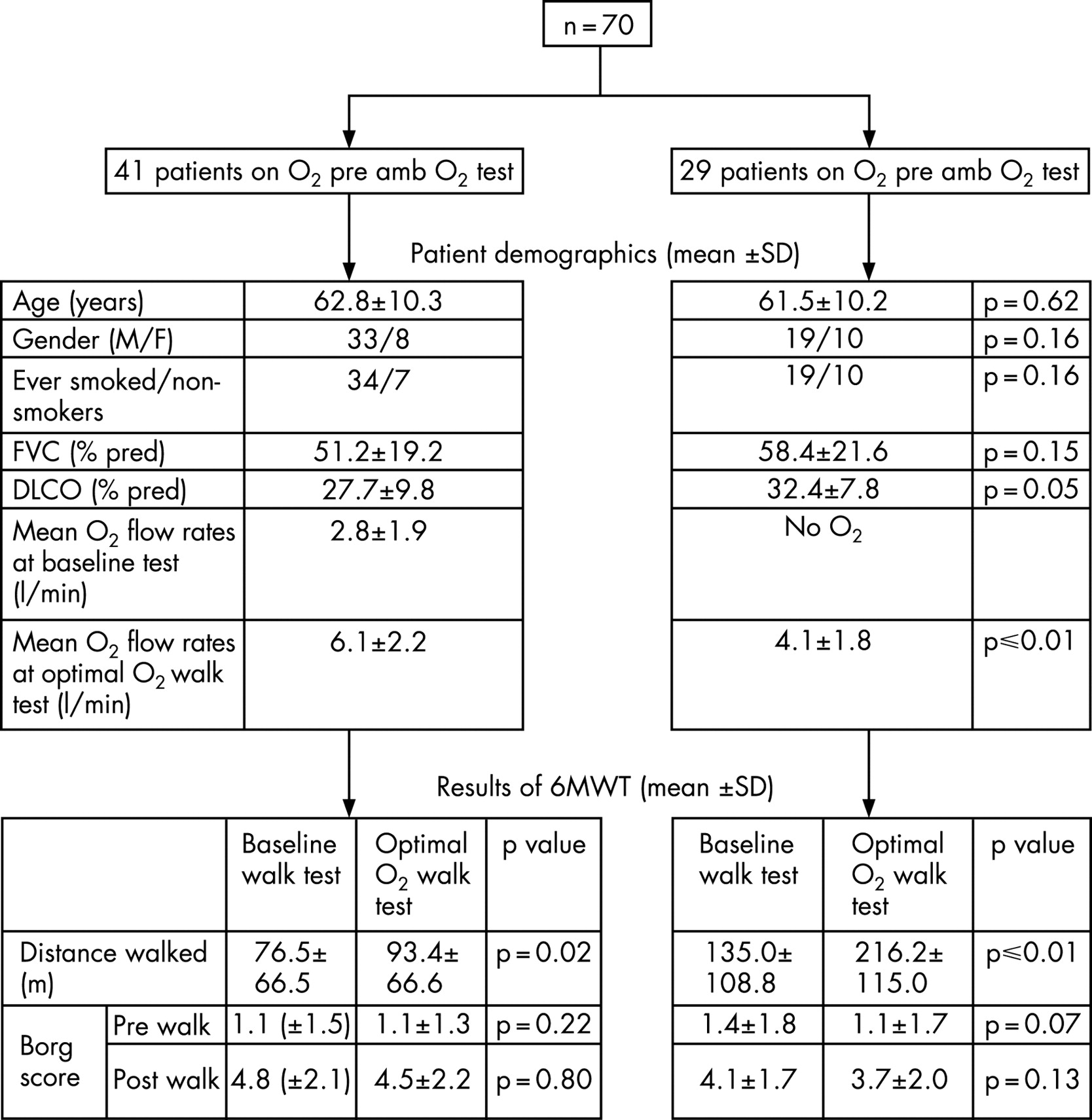
Conclusion: This study shows definitively that IPF patients, regardless of whether on long-term oxygen therapy at rest, benefit from ambulatory oxygen in terms of distance walked, which will translate into quality of life benefits for these patients.
SYSTEMIC SCLEROSIS-RELATED DIFFUSE PULMONARY FIBROSIS QUANTIFIED BY HIGH RESOLUTION COMPUTED TOMOGRAPHY: AUTOANTIBODY AND HLA ASSOCIATIONS
F. A. Woodhead1, H. Sato1, S. R. Desai2, R. K. Hoyles1, A. U. Wells1, K. I. Welsh1, C. P. Denton3, R. M. Dubois1. 1Interstitial Lung Disease Unit, National Heart and Lung Institute, Imperial College, London; 2Department of Radiology, King’s College Hospital; 3Centre for Rheumatology, Royal Free and University College Medical School, London, UK
Background: Systemic sclerosis (SSc) is characterised by microvascular damage, immune activation and fibrosis of the skin and various internal organs including the lung. Although antinuclear antibodies are present in up to 95% of cases the precise antigen cannot be determined in a significant minority of cases. Patients with anticentromere antibodies (ACA) and anti-RNA polymerase I/III antibodies (ARA) have a low average extent of pulmonary fibrosis (PF) while those with antitopoisomerase antibodies (ATA) have a higher average extent. ACA and ATA have distinct associations with human leukocyte antigen (HLA) genes.
Aim: To investigate whether associations with PF are stronger for HLA alleles or autoantibodies.
Methods: 187 patients with SSc assessed at the Royal Brompton Hospital for the presence of PF had high resolution computed tomography (HRCT) performed. HRCTs were quantified by two independent observers for overall disease extent (to the nearest 5%). PF was defined as extent >0%. HLA-DRB1 genotype was determined by polymerase chain reaction using sequence-specific primers (SSP-PCR) in 171. Frequencies were compared using χ2 or Fisher’s exact test where appropriate.
Results: See tables 1 and 2. ACA is associated with HLA-DRB1*04 (p = 0.01) but by multiple regression analysis they remained independently associated with protection from PF.
Conclusion: The strongest predictor of PF remains autoantibody status (with the strongest negative association with ACA); however HLA-DRB1*04 is also independently predictive. This may be particularly relevant in patients with currently undefined autoantibodies.
Treatment trials in chronic obstructive pulmonary disease
EFFECT OF LONG-TERM ERYTHROMYCIN IN COPD TRIAL (ELECT): EXACERBATIONS AND INFLAMMATION
T. M. A. Wilkinson1, T. A. R. Seemungal2, R. Sapsford3, J. R. Hurst3, W. Perera3, J. A. Wedzicha3. 1Southampton University, Southampton, UK; 2University of theWest Indies, Trinidad and Tobago; 3Royal Free and University College School of Medicine, London, UK
Introduction: Chronic obstructive pulmonary disease (COPD) is characterised by heightened airway and systemic inflammation and by frequent exacerbations that are a major cause of hospital admission, mortality and contribute to disease progression. Macrolide antibiotics have been shown to have anti-inflammatory activity and their long-term use may impact upon inflammation and exacerbation risk in subjects with COPD.
Methods: We performed a one-year randomised double-blind placebo-controlled study of erythromycin 250 mg twice daily in COPD patients, with total number of treated exacerbations as the primary outcome and sequentially collected sputum and blood samples to determine effects on airway and systemic inflammation. We recruited 109 COPD outpatients: 69 males, 52 current smokers, mean (SD) age 67.2 (8.6) years, FEV1 1.32 (0.53) l, FEV1% 50 (18)%.
Results: There was no difference in any of these parameters between the two treatment groups at study start. Dropouts (n) were placebo (6) and macrolide arm (7). The total number of treated exacerbations was 233 median (IQR) 1 (0–3). Poisson generalised linear modelling was used to determine the effect of treatment on exacerbation frequency with allowance for time on treatment, smoking status, disease severity, baseline exacerbation frequency, age and gender. Macrolide therapy was associated with a reduction in the incidence of exacerbations, the odds ratio (OR) for exacerbation on placebo compared to macrolide therapy was 1.48 (p = 0.004). No significant effect of treatment was seen on serum CRP, interleukin 6, or on sputum interleukin 6, 8 or myeloperoxidase, at 1, 3, 6, 9 or 12 months (p>0.05). Macrolide therapy was associated with a significant reduction in exacerbations compared to placebo, however no significant affect on airway or systemic inflammation was found.
Conclusion: Further studies are required to determine the mechanism of action of this therapy as it has potential to reduce the clinical burden of exacerbations of this important disease.
ERDOSTEINE IN ASSOCIATION WITH AMOXICILLIN IMPROVES THE OUTCOME OF ACUTE EXACERBATIONS COMPARED TO AMOXICILLIN ALONE IN COPD PATIENTS
A. Morice1, M. Moretti2, M. Ballabio3. 1University of Hull, Castle Hill Hospital, Hull, UK; 2Polyclinic of Modena and Reggio Emilia, Modeno, Italy; 3Edmond Pharma, Milan, Italy
Introduction: Acute infective exacerbations represent an important cause of morbidity and mortality in patients with chronic obstructive pulmonary disease (COPD). The European Chronic Obstructive Bronchitis Erdosteine Study trial has shown that erdosteine in association with amoxicillin can improve symptoms and clinical conditions earlier and more effectively compared to antibiotic monotherapy (Int J Clin Pharmacol Therap 1995;33:612). As entry criteria were mainly based on clinical diagnosis, a post hoc analysis has been performed to confirm efficacy of erdosteine in the subset of patients fulfilling spirometric criteria for COPD diagnosis (diagnosed by FEV1/FVC <70% pred).
Methods: Of 237, 175 patients fulfilled the diagnostic criteria of COPD and were randomised to erdosteine + amoxicillin (E+A) or placebo + amoxicillin (P+A) for 7–10 days. The primary efficacy endpoint was cumulative Global Clinical Assessment (GCA) composed of four-point categorical scores (3 being the worst) evaluating six items at Day 3–4 and Day 7–10: sputum appearance and viscosity, difficulty to expectorate, catarrh rhonchi at auscultation, cough and dyspnoea. Secondary endpoints were the overall physician’s and patient’s judgement of efficacy, and pulmonary function tests (FEV1, FVC, MMEF25–75%). An analysis of covariance (ANCOVA) was performed.
Results: Mean GCA score at baseline was 12.38 in E+A (n = 89) and 12.99 in P+A group (n = 86). At both intermediate and final evaluation GCA was significantly lower in E+A than in P+A group (ANCOVA LSMeans 9.05 vs 10.25 at Day 3–4, and 5.86 vs 7.85 at Day 7–10, respectively; p<0.001). In the overall efficacy assessment a higher percentage of patients treated with E+A rated a return to pre-treatment baseline state (25.8% vs 9.4%) which was consistent with the physicians’ evaluations (21.3% vs 7.1%). Pulmonary function parameters improved in both groups at the end of treatment, being numerically better in patients receiving E+A (FEV1 LSMeans: 1.50 and 1.44 l in two groups, respectively).
Conclusion: Erdosteine plus antibiotics is more effective than antibiotic monotherapy for the treatment of acute infective exacerbations in patients with spirometric-diagnosed COPD. Early and aggressive management may reduce the length of the exacerbation. By the addition of erdosteine to usual care further resolution of symptoms may allow a more rapid recovery.
COST-EFFECTIVENESS OF ERDOSTEINE IN THE TREATMENT OF ACUTE EXACERBATIONS OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE
J. Haughney1, M. Grishchenko2, H. A. Dakin2, M. Ballabio3, G. Caputo2. 1University of Aberdeen, Aberdeen, UK; 2Abacus International, Bicester, UK; 3Edmond Pharma, Milan, Italy
Introduction: Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are associated with reduced quality of life, increased morbidity and mortality. Management of AECOPD is aimed at returning patients to pre-exacerbation pulmonary state as rapidly as possible. Erdosteine is a third-generation mucolytic used in the treatment of AECOPD. Clinical trials involving more than 2500 patients have demonstrated its efficacy and safety.
Objectives: To assess the cost effectiveness of erdosteine + usual care (UC) versus UC alone in the treatment of AECOPD in a primary care setting from the perspective of the UK NHS.
Methods: A cost-utility analysis was conducted. The cost and benefits were assessed over 14 days (a typical treatment and recovery time for AECOPD). The costs associated with treatment alternatives were calculated using a decision-tree approach. Resource use data were derived from a survey of 30 randomly-selected UK clinicians. Costs of erdosteine and primary care consultations were taken from standard UK price tariffs. Efficacy data were based on a post hoc intent-to-treat analysis of the ECOBES (European Chronic Obstructive Bronchitis Erdosteine Study) trial, which demonstrated that 25.8% of erdosteine/amoxicillin-treated patients and 11.1% of placebo/amoxicillin-treated patients returned to pre-exacerbation pulmonary state within 7–10 days (p<0.05; number-needed-to-treat, 7). Quality-adjusted life-years (QALYs) were calculated using published utility data and assuming a logarithmic recovery function.
Results: Erdosteine was found to dominate UC, being both more effective and cost-saving. The total costs of erdosteine were, on average, £3.47/exacerbation lower than those of UC (£104.58 vs £108.05) due to reductions in healthcare use. Erdosteine was also associated with QALY gains over UC (0.02939/exacerbation vs 0.02935/exacerbation) and an additional 0.74 exacerbation-free days. Scenario analyses suggest that treatment with erdosteine dominates UC alone in patients treated with/without a homecare pack, whether they had mild, moderate or severe disease. Extensive sensitivity analyses demonstrated that these conclusions are robust. All parameters were varied within their plausible ranges; none caused erdosteine to generate fewer QALYs than UC alone and only one parameter could cause erdosteine to cost more than £30,000/QALY.
Conclusion: Adding erdosteine to UC in the treatment of AECOPD is highly cost-effective compared with UC alone, generating additional health benefits at lower cost.
FAST ONSET OF ANTIOXIDANT ACTIONS OF ERDOSTEINE AND ITS POTENTIAL USE FOR ACUTE TREATMENT OF COPD EXACERBATIONS
S. A. Kharitonov. Imperial College London, Royal Brompton NHS Trust, UK
Introduction: Increased frequency of exacerbations in patients with chronic obstructive pulmonary disease (COPD) is associated with increased oxidative stress. The average exacerbation recovery time of COPD patients is 10.7 days, with conventional treatment of antibiotics and corticosteroids. A significant proportion of these patients demonstrate incomplete recovery, and frequent exacerbations contribute to decline in lung function and poor health status.
Results: Erdosteine possesses mucolytic, antioxidant and anti-inflammatory properties that prevents the accumulation of reactive oxygen species (ROS) when their production is accelerated and increases antioxidant cellular protective mechanisms. Fast onset of antioxidant action of erdosteine has been demonstrated following acute experimental liver and renal toxicity (5–7 days of treatment), ischemia reperfusion (2 days) and hypoxia-induced lung and pulmonary vasculature damage (2 weeks). Combination of erdosteine and formoterol in patients with COPD might be beneficial in preventing COPD exacerbations. It has been shown that when budesonide and erdosteine were administered in combination, their antioxidative effect on the release of ROS and peroxynitrite by stimulated neutrophils was higher than the effect of a single drug.
Conclusion: This analysis indicates that erdosteine given acutely minimises the impact of oxidative stress during a COPD exacerbation. The antioxidant properties of the drug, considering its fast onset of antioxidant action (table) may play an important role in COPD patients during exacerbations where the oxidant/antioxidant imbalance is higher.
INITIAL EXPERIENCE WITH AN EMPHYSEMA MULTIDISCIPLINARY MEETING FOR THE MANAGEMENT OF PATIENTS FOR LUNG VOLUME REDUCTION
I. F. Oey1, D. A. Waller1, J. Entwisle2, S. J. Singh3, M. C. Steiner1, M. D. Morgan1. 1Department of Respiratory Medicine and Thoracic Surgery, Glenfield Hospital; 2Department of Radiology, Glenfield Hospital; 3Department of Pulmonary Rehabilitation, Glenfield Hospital, Leicester, UK
Objective: It has become common practice to manage lung cancer patients through a multidisciplinary meeting (MDT). We describe our 10-year experience with an emphysema MDT for lung volume reduction surgery (LVRS) and an audit of our results.
Method: We have been performing LVRS since 1995 and established an EMDT in 1997. Patients are initially referred to either a thoracic surgeon or a respiratory physician with special interest in LVRS. Subsequently these patients are discussed at a bimonthly meeting, which is attended by representatives of respiratory medicine, thoracic surgery, radiology and pulmonary rehabilitation. The prior investigations required for each patient include CT scan, quantitative radionuclide perfusion scan and respiratory function tests with body plethysmography and arterial blood gas analysis. Rehabilitation reports are also received. A dedicated coordinator organises the meeting, takes minutes and distributes management plans to the relevant healthcare professionals. Feedback is given to referring physicians. Guidelines are changed according to best medical evidence available and adjusted by continuously auditing our own results.
Results: To date 386 patients have been referred for LVRS. These include 126 patients from Leicestershire and 260 external referrals. So far, 144 LVRS procedures on 131 patients have been performed. Nine patients are currently on our waiting list for LVRS. The figure shows the annual distribution. Although patients for bullectomy are not normally discussed at this meeting 11 patients proceeded to bullectomy. Bronchoscopic LVR has emerged as a new technique and for the last two years we have identified another 15 patients who, although not suitable for surgical LVR, may be candidate for an endoscopic procedure. Since 2005 patients are followed postoperatively at a multidisciplinary emphysema out-patient clinic. If patients are to be considered for further surgery they are re-referred to the EMDT.
Conclusion: Our experience of an EMDT has been favourable and we would advocate its use. It has ensured a regular throughput of patients for LVRS and has helped to refine referrals. The number of patients suitable for surgical volume reduction remains small and is not increasing.
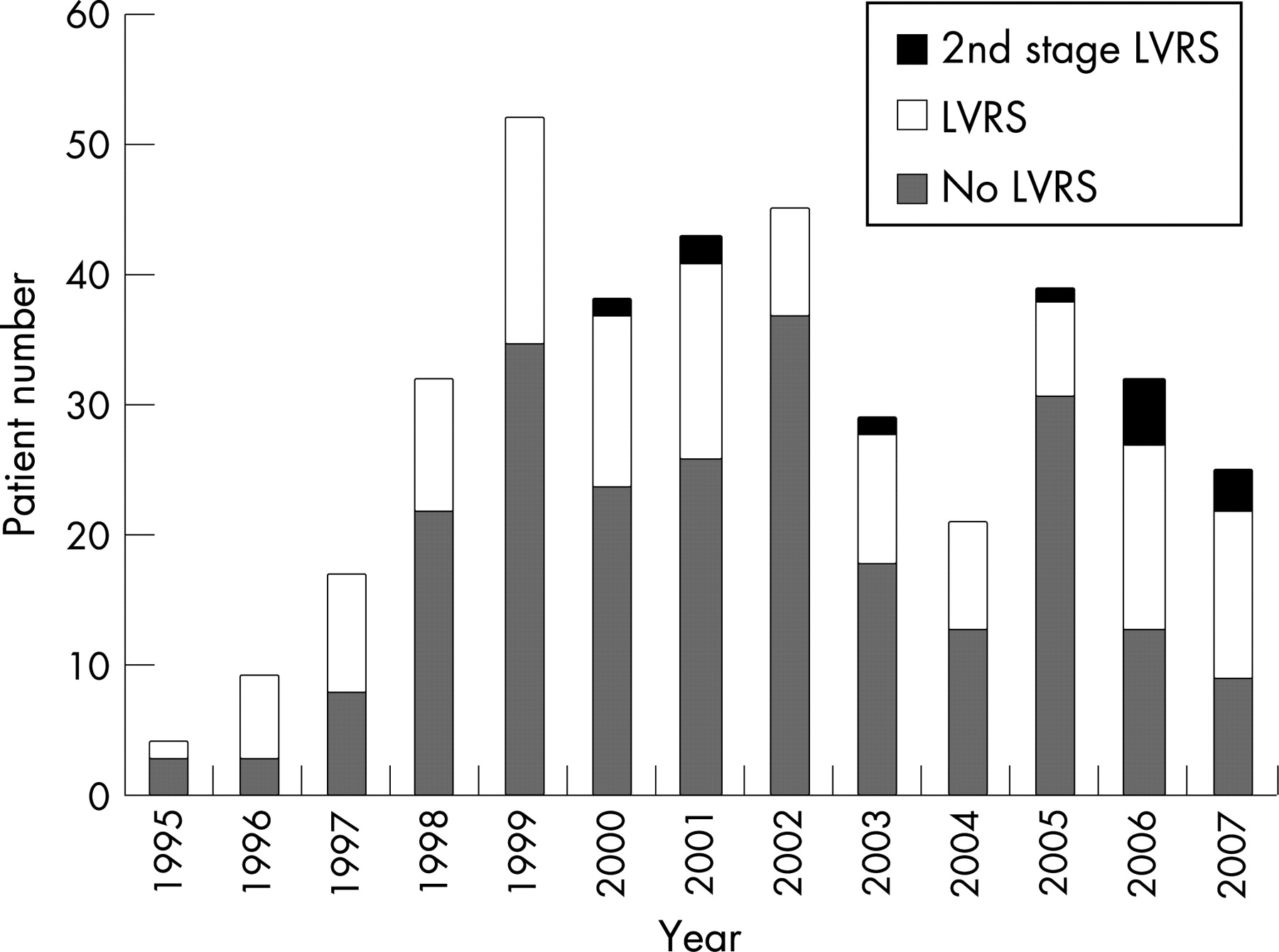
Investigations and interventions in pleural disease
ACCURACY OF PLEURAL FLUID PH MEASUREMENT IS CRITICALLY INFLUENCED BY SAMPLE COLLECTION AND HANDLING
E. Mishra2, N. M. Rahman1, H. E. Davies1, K. Russell1, R. J. O. Davies1, Y. C. G. Lee1. 1Oxford Centre for Respiratory Medicine; 2Norfolk and Norwich University Hospital, Norwich, UK
Background: Significant emphasis has been placed on pleural fluid pH (and glucose) measurement, especially in guiding clinical management of parapneumonic effusion and predicting outcome in malignant effusion. However, there is no standard method to collect pleural fluid for pH measurement. We hypothesise that pleural fluid pH, but not glucose, measurements are susceptible to variations in methods of collection. This study assessed the consistency of pleural fluid pH and glucose measurements in samples contaminated with likely agents from clinical practice.
Methods: Exudative pleural effusions from 63 patients (malignancy, n = 22; infection, n = 7) were included. Samples were collected in commercially available blood gas syringes (with or without residual lignocaine, air or heparin) and analysed immediately using a blood gas machine (Radiometer ABL 700 series, Copenhagen). The plain sample was analysed at 0, 1, 4 and 24 h, and pH and glucose were assayed in all samples. A further sample was sent to the laboratory for glucose analysis.
Results: Pleural fluid pH was significantly affected by leftover lignocaine in a dose-dependent fashion. 0.2 ml of residual lignocaine was sufficient to induce a clinically significant decrease in pleural fluid pH (−0.14 (SD 0.08); 95% CI −0.12 to −0.17; p<0.001). Incomplete expulsion of air from the collection syringe resulted in a significant rise in pleural pH by 0.08 (SD 0.05); 95% CI 0.09 to 0.06, p<0.001. Retaining heparin within the blood gas syringe caused a significant reduction in pleural fluid pH (−0.02 (SD 0.05); 95% CI −0.002 to −0.04, p = 0.03). Pleural fluid pH was stable in samples left at room temperature for 1 h. Significant changes were observed at 4 h (−0.02 (SD 0.08); 95% CI −0.04 to −0.003, p = 0.03) and at 24 h (−0.06 (SD 0.13); 95% CI −0.15 to −0.02; p = 0.001). In contrast, glucose measurements as analysed by blood gas machine were not significantly affected (changes <1 mmol/l) in the presence of lignocaine (up to 0.4 ml), air or heparin, and remained stable after 1, 4 and 24 h. There was a strong correlation between glucose measured by the machine and laboratory measured glucose.

Conclusion: Accuracy of pleural fluid pH measurement is critically dependent on the precise manner under which the sample is collected. This is the first study to show that common variations in collection of pleural fluid, for example, carried over lignocaine (even in minute volumes), presence of air, or delay in pH assay, all lead to significant changes in pH that may alter clinical management. Pleural fluid glucose, however, is more stable and less susceptible to variations in collection details. Strict guidelines on sample collection and preparation are urgently required to ensure accurate measurements of pleural fluid pH.
A RANDOMISED PHASE III TRIAL OF ACTIVE SYMPTOM CONTROL WITH OR WITHOUT CHEMOTHERAPY IN THE TREATMENT OF PATIENTS WITH MALIGNANT PLEURAL MESOTHELIOMA. THE MEDICAL RESEARCH COUNCIL/BRITISH THORACIC SOCIETY MS01 TRIAL
M. Muers1, P. Fisher2, M. O’Brien3, M. Peake4, R. Rudd5, M. Snee6, J. Steele5,M. Nankivell7, C. Pugh7, R. J. Stephens7. 1Leeds General Infirmary; 2Weston Park Hospital, Sheffield, UK; 3Royal Marsden Hospital; 4Glenfield Hospital, Leicester, UK; 5St Bartholomew’s Hospital, London, UK; 6Cookridge Hospital, Leeds, UK; 7MRC Clinical Trials Unit, London, UK
Background: Although chemotherapy is widely used in the treatment of mesothelioma it has never been compared in a randomised trial with active symptom control (ASC) alone.
Methods: Patients with malignant pleural mesothelioma were randomised to ASC alone (including steroids, analgesics, bronchodilators, palliative radiotherapy, etc), ASC+MVP (4 × 3-weekly cycles of mitomycin 6 g/m2, vinblastine 6 mg/m2, and cisplatin 50 mg/m2), or ASC+V (12 weekly injections of vinorelbine 30 mg/m2). 420 patients were required to detect a 3-month improvement in median survival with ASC+CT (both chemotherapy arms combined).
Results: 409 patients were accrued (136 ASC, 137 ASC+MVP, 136 ASC+V). Median age: 65 years, male: 91%, performance status 0: 23%, epithelial histology: 73%, Stage III: 33%, Stage IV: 48%. Good symptom palliation was achieved in all three groups, and no between-group differences were observed in four pre-defined quality of life subscales. A small survival benefit was seen for ASC+CT (349 deaths, HR 0.89, 95% CI 0.72 to 1.12, p = 0.32). Median survival: ASC: 7.6 months, ASC+CT: 8.5 months. Exploratory analyses suggested a survival advantage for vinorelbine compared to ASC alone (232 deaths, HR 0.81, 95% CI 0.63 to 1.05, p = 0.11), with a median survival of 9.4 months, but no evidence of a benefit with MVP (231 deaths, HR 0.98, 95% CI 0.76 to 1.28, p = 0.91).
Conclusions: This is the second largest ever randomised trial in mesothelioma and the first to compare ASC with or without chemotherapy. Although the addition of chemotherapy to ASC did not result in a conventionally significant survival benefit, there was an indication that vinorelbine should be investigated further, and that MVP probably has no role in this disease.
THE RELATION BETWEEN CHEST TUBE BORE, CLINICAL OUTCOME AND TUBE-RELATED ADVERSE EVENTS IN PLEURAL INFECTION
N. M. Rahman1, N. A. Maskell2, E. L. Hedley1, A. J. Nunn3, F. V. Gleeson1, R. J. O. Davies1. 1Oxford Centre for Respiratory Medicine; 2Southmead Hospital, Bristol, UK; 3Medical Research Council, Clinical Trials Unit, London, UK
Indtroduction: The primary treatment modalities of pleural infection are drainage of infected fluid combined with antibiotic therapy. There is no evidence to inform clinicians as to the optimal size of chest tube for this purpose, and practice is based on expert opinion. We have previously shown that smaller bore (<14F), guide-wire inserted chest tubes are less painful than larger bore, blunt dissection tubes (Rahman et al, Thorax 2006;61(Suppl 2):191A). This study addresses whether the size of tube is associated with differential clinical outcome in patients with pleural infection. The primary outcome measure (death and surgery rate combined at one year), and secondary outcomes (FEV1, FVC and CXR abnormality at three months, length of hospital stay, adverse events) were related to the size of the initial chest tube in 405 patients with pleural infection taking part in the UK MRC MIST1 trial.
The death and surgery rate at 1 year (table) did not vary with initial chest drain size, and this outcome did not evolve over time (fig). There was no difference in death/surgical rate when these groups were divided according to pleural fluid purulence. There were no significant differences in any secondary outcomes between chest tube bore groups.
The method of chest tube insertion was not associated with death and surgery rate (guide-wire, death + surgery 97/265 (37%), blunt 57/140 (41%) OR = 1.19, 95% CI 0.78 to 1.81, χ2 1df = 0.66, p = 0.42), nor with any other outcome. Apart from the previously demonstrated greater pain with larger blunt dissection inserted chest tubes (Thorax 2006;61(Suppl 2):191A), tube insertion technique was not associated with a difference in adverse event rate. The initial choice of a small bore, guide-wire inserted, chest tube for pleural infection produces as good a clinical result as a larger, blunt dissection, inserted tube, but causes less pain for the patient.

PREDICTORS OF LONG-TERM POSTOPERATIVE SURVIVAL IN MALIGNANT PLEURAL MESOTHELIOMA: A MULTIVARIATE ANALYSIS IN 300 PATIENTS TREATED IN A SINGLE INSTITUTION
D. S. Trousse1, A. Nakas1, J. G. Edwards2, A. E. Martin-Ucar1, K. J. O’Byrne3,D. A. Waller1. 1Glenfield Hospital, Leicester, UK; 2Northern General Hospital, Sheffield, UK; 3St James’s University Hospital, Dublin, ROI
Background: Current guidelines advocate surgery for malignant pleural mesothelioma (MPM) for symptom control; the role of therapeutic surgery remains controversial. There is non-randomised evidence for a multimodality approach including extrapleural pneumonectomy (EPP) or radical pleurectomy/decortication (P/D) or non-radical by thoracoscopy (VATS P/D) or thoracotomy (open P/D).
Objective: To analyse our single-institution surgical experience with MPM to identify long-term survivors and factors predicting their favourable outcome.
Methods: In a retrospective review of a prospective database of 300 consecutive patients with MPM operated on over a 10-year period long-term overall survival was analysed using the Kaplan-Meier method. Potential prognostic factors were tested in univariate and multivariate analysis.
Results: We operated upon 300 patients (89% male, mean age 61 years). Procedures included: 124 EPP, 51 radical P/D, 74 VATS P/D and 51 open P/D. Epithelial MPM was the most frequent (71%). The overall 30-day and 90-day mortality rates were 6% and 14% respectively. Postoperative complications occurred in 40%. Mean hospital stay and duration of drainage were 14.2 and 10.8 days respectively. Overall 1-year, 2-year, 3-year and median survival rates were respectively 63%, 33%, 18%, 15 months for EPP, 54%, 46%, 40%, 23 months for radical P/D, 55.%, 19%, 9%, 12 months for VATS P/D, and 35%, 13%, 0%, 7 months for open P/D, (p<10−3). On univariate analysis, younger age (p = 0.003), epithelial type cell (p<10−3), radical surgery in favour of radical P/D (p<10−3), negative node staging following mediastinoscopy (p = 0.014), haemoglobin >14 g/dl (p = 0.012), WCC<8.3×109/l (p = 0.005) and adjuvant chemotherapy (p<10−3) or radiotherapy (p = 0.03) were significant good prognostic factors. On multivariate analysis, age >60 years (p = 0.006, HR 1.7), non-epithelial histology (p<10−3) were independent predictors of poor long-term survival. Conversely, haemoglobin >14 g/dl (p = 0.014, HR 0.57), radical P/D (p = 0.047, HR 0.53) and adjuvant chemotherapy (p = 0.002, HR 0.43) were positive predictors of outcome.
Conclusions: Long-term survival in MPM can be achieved by radical surgery in selected candidates aged <60 years, normal haemoglobin level, epithelial histology and negative mediastinoscopy. Radical debulking surgery in the form of decortication/pleurectomy followed by adjuvant chemotherapy appears to be the best therapeutic option.
PNEUMOTHORAX AND PREGNANCY
M. Alhajji, A. G. Arnold. Castle Hill Hospital, East Yorkshire, UK
Introduction: Primary spontaneous pneumothorax (PSP) affects young female patients of childbearing age. Recurrence is a recognised feature of PSP. Several guidelines have been developed to assist the diagnosis and management of this condition, the latest being the BTS guidelines of May 2003, but they do not contain advice on the management of pneumothorax during pregnancy or parturition. PSP might be expected to occur reasonably commonly during pregnancy, but only 43 cases have been reported, with individual series consisting of between one and three patients. These studies describe an increased risk of recurrence both in pregnancy and during childbirth in patients with pneumothorax, and relatively invasive management strategies.
Methods: As the only major hospital in our area, with a stable catchment population of half a million patients, we have collected a database of 250 consecutive pneuomothorax patients over the last decade. We present the largest series reported to date of the management of pneumothorax in pregnancy (seven cases), together with a review of the relevant literature, and offer advice regarding the management of such patients.
Results: See table.
Conclusions: We have reviewed the existing medical literature of pneumothorax during pregnancy and added our own experience, the largest group of patients from a single centre, using less invasive management strategies. Current guidelines do not contain advice on the management of this situation. The potential hazards to the mother and child are such that practising chest physicians, surgeons and obstetricians need awareness of the problem and close cooperation in its management.
PLEURECTOMY/DECORTICATION FOR MALIGNANT MESOTHELIOMA
E. J. Fontaine, P. J. Kenyon, H. M. H. Carr. The Cardiothoracic Centre-Liverpool NHS Trust, UK
Objective: Pleurectomy/decortication offers patient palliation from symptoms of pain and management of pleural fluid in an attempt to improve quality of life. We wanted to assess the effectiveness, safety and survival of patients undergoing surgery.
Methods: A retrospective analysis of 27 patients undergoing pleurectomy/decortication from 1 November 2003 to 30 April 2007 entered in our thoracic database was undertaken. All patients had undergone VATS to establish the diagnosis of malignant mesothelioma.
Results: Twenty two males and five females had undergone pleurectomy/decortication. The age range was 38–80 years with a mean of 66 years. Preoperatively: 6 patients had talc pleurodesis, 6 had chemotherapy, 5 had talc pleurodesis and chemotherapy, and 10 patients had VATS only to establish diagnosis. The commonest presentations of mesothelioma included pleural effusion (n = 13), non-specific shortness of breath (n = 7), chest pain (n = 6), persistent cough (n = 2), weight loss (n = 2), haemoptysis/empyema/pneumonia (n = 1). The histology was 14 epithelioid, 9 mixed, 3 unspecified and 1 sarcomatous. There was 1 in-hospital death from pneumonia 11 days post-op. Of the 26 patients discharged from hospital there are 10 patients alive and 16 have died. From the 16 deaths: the mean survival was 312 days (38–600 days), median 273 days, 4 received post-op chemo with a mean survival of 245 days compared to a mean of 357 days for the 12 patients who did not receive post-op chemotherapy. Of the 10 patients who are alive: 5 were operated in March/April 2007 and the other 5 between February 2004 and August 2006 have survived between 262 and 1182 days (median 342 days).
Conclusions: Pleurectomy/decortication appears to be a safe operation with a postoperative mortality of 3.7%. The survival benefit of radical surgery needs to be evaluated in comparison to other treatment options so all future radical surgery in our unit will be undertaken as part of the MARS trial.
Aspects of respiratory infection
GALACTOMANNAN DETECTION IN EXHALED BREATH CONDENSATE OF NEUTROPENIC PATIENTS WITH SUSPECTED INVASIVE PULMONARY ASPERGILLOSIS
S. R. Doffman1, L. J. Griffiths2, G. R. Athorn1, S. J. Vinnicombe2, J. C. Moore-Gillon2, M. J. Griffiths3, S. G. Agrawal1. 1Queen Mary, University of London; 2Barts and the London Hospital; 3Royal Brompton Hospital, London, UK
Introduction: The mortality from invasive pulmonary aspergillosis (IPA) associated with treatment of haematological malignancies is high and diagnosis can be difficult due to its non-specific clinical features. Galactomannan (GM), a polysaccharide component of Aspergillus spp cell wall, is detectable in serum and bronchoalveolar lavage (BAL) fluid in IPA. The application of exhaled breath condensate (EBC) analysis, a non-invasive technique, has not been explored in this setting. We report on pilot data of the detection of GM in EBC from a subset of patients forming part of a prospective trial into the early diagnosis of IPA in haematological patients at high risk.
Methods: EBC and serum were collected once and twice weekly, respectively, throughout the study period. BAL was carried out in patients with an abnormal HRCT chest after >96 h of persistent fever despite antibiotics. GM was measured in EBC, serum and, where appropriate, BAL fluid using a commercially available kit (Platelia Aspergillus, Bio-Rad, France). The likelihood of IPA was assigned using well-recognised criteria by two investigators blinded to clinical details.
Results: Of 33 patients studied, 7 had proven/probable IPA, 7 possible and 2 unclassified. 17 had no evidence of IPA. Of the 7 patients with proven/probable disease, four of whom had GM-positive sera, EBC and serum GM followed the same trend. In one patient the EBC GM was positive early in the infection, while BAL GM remained negative. In another who developed HRCT evidence of IPA with a positive BAL GM, the EBC GM was positive four weeks earlier. GM was negative in all but one of the serum and EBC samples of patients with possible, unclassified or no evidence of IPA.
Conclusions: GM can be detected in EBC, and follows the same trend as in serum. It may even predate GM detection in BAL fluid, thereby obviating the need for more invasive investigations. Elevated levels early in the course of neutropenia may represent infection and could be applied to the employment of pre-emptive treatment strategies.
VARIATION IN COLONIAL MORPHOTYPE AND ANTIBIOTIC SUSCEPTIBILITY IN PSEUDOMONAS AERUGINOSA IN SPUTA FROM PATIENTS WITH NON-CYCSTIC FIBROSIS BRONCHIECTASIS AND ITS IMPACT ON ANTIBIOTIC SUSCEPTIBILITY TESTING
M. I. Gillham, S. Sundaram, C. R. Laughton, C. Haworth, D. Bilton, J. E. Foweraker. Papworth Hospital, Cambridge, UK
Background: P aeruginosa is a common cause of infection in bronchiectasis. In chronic P aeruginosa infection in cystic fibrosis (CF), various colonial forms (morphotypes) and different antibiotic susceptibilities are present in single sputa. Susceptibility testing is poorly reproducible, with resistant isolates missed. There is little information on phenotypic variability in P aeruginosa in patients with non-CF bronchiectasis.
Aim: To investigate the variability of antibiotic susceptibility and morphotype of P aeruginosa from sputa of patients with bronchiectasis and compare this with other pseudomonal infections.
Methods: P aeruginosa was obtained from sputa from 31 patients, mean age 63 (38–81) years with well-characterised bronchiectasis, either stable (23) or during acute exacerbation (8). The morphotype of each isolate was assessed by size, texture, colour and mucoidity. Antibiotic susceptibility testing of four examples of each morphotype to 12 antibiotics was performed using disc diffusion and the zone of inhibition was measured. This variability in susceptibility was compared with control P aeruginosa from 9 skin swabs and 7 sputa from ventilated patients without bronchiectasis. Antibiotic susceptibility was also tested by the standard method used in a hospital diagnostic laboratory.
Results: Control P aeruginosa isolates were all classical morphotype. The maximum difference in zone diameter between four isolates from each sample was 4 mm. A single morphotype was present in 18 bronchiectasis sputa and mixed morphotypes in 13. In six bronchiectasis sputa, maximum variation in zone size was 4 mm; others had wider variation, up to 24 mm between isolates of the same morphotype in one sputum. There was more variability in antibiotic susceptibility where mixed morphotypes were present. Similar variability was seen in sputa from stable patients and during exacerbations. Routine laboratory methods missed resistance in 10 patients with bronchiectasis.
Conclusions: Some patients with bronchiectasis have a uniform population of P aeruginosa; others show variation in morphotype and susceptibility, similar to CF. Routine antibiotic susceptibility testing may miss resistance once the population is so diverse. The natural epidemiology of P aeruginosa in non-CF bronchiectasis needs further study.
LUNG FUNCTION DOES NOT DECLINE IN AN EIGHT-YEAR SURVEILLANCE STUDY OF BRONCHIECTASIS PATIENTS ATTENDING A REGIONAL SPECIALIST CENTRE
J. French, L. Sharples, C. Haworth, A. Condliffe, A. Exley, D. Bilton. Papworth Hospital NHS Foundation Trust, Cambridge, UK
Introduction: There are limited data demonstrating the long-term outcome of patients, in terms of lung function in adult non-cystic fibrosis bronchiectasis. There is debate (Evans, 1996; Davies, 2006) whether patients colonised with pseudomonas have a faster decline in lung function than non-pseudomonas colonised patients. Evans (1996) confirmed the association of chronic pseudomonas aeruginosa colonisation with poorer and faster decline in lung function. Davies (2006) concluded that infection with pseudomonas aeruginosa was a marker of disease severity but not linked with an accelerated decline in lung function.
Methods: This study evaluates the rate of decline in lung function over an 8-year period in patients attending a bronchiectasis clinic. All patients in the RCT of nurse- versus Dr-led care (Sharples, 2002) were approached. In 1998, 80 patients were recruited, 54 females and 26 males, mean age 58.76 (SD 13.9) years, and defined as having chronic infection with pseudomonas or not. At each yearly point of review lung function data were collected. At study end (2006) 12 patients had died and 11 had returned to their local primary care team.
Results: Baseline lung function in 1998, n = 80, mean FEV1%pred 69.7% (SD 20) and mean FVC%pred 82.2%(SD 16.9). 1998–2006: an average increase in FEV1%pred of 1.2% (SD 1.8%) and FVC %pred average increase of 2.1% (SD 1.4%) which was statistically significant (p<0.01). Subanalysis of lung function of patients colonised (n = 18) and non-colonised with pseudomonas aeruginosa (n = 62) was undertaken. This analysis showed there a significant difference (p = 0.03) in baseline lung function in the pseudomonas cohort (FEV1%pred 60% (SD 18.3) versus non-colonised patients (FEV1%pred 72.5% (SD 19.7). There was no statistically significant difference between the groups in the rate of improvement in lung function (p = 0.35). Pseudomonas cohort: an increase in FEV1%pred of 0.7% per year (SD 2.0) and FVC%pred of 1.8% per year (SD 1.7). Non-pseudomonas cohort: an increase in FEV1%pred of 1.3% (SD 1.8) and increase in FVC%pred of 2.1% per year (SD 1.4%).
Conclusions: Patient with bronchiectasis can be stabilised and decline in lung function prevented, regardless of pseudomonas colonisation, with aggressive management and education of the patient.
COMPLEMENT-MEDIATED IMMUNITY TO STREPTOCOCCUS PNEUMONIAE IS SIGNIFICANTLY IMPAIRED IN SERA FROM PATIENTS WITH HOMOZYGOUS C2 DEFICIENCY
J. Yuste1, A. Sen1, L. Truedsson2, G. Jonsso2, L-S. Tay1, F. Goldblatt1, J. Brown1. 1University College London, London, UK; 2Lund University, Lund, Sweden
Subjects with homozygous deficiency of the classical complement pathway component C2 are highly susceptible to Streptococcus pneumoniae pneumonia and septicaemia. This observation, combined with data obtained using mice with genetic defects affecting different complement pathways, suggests that, surprisingly, the classical pathway is vital for innate immunity to S pneumoniae. However, the role of the classical pathway for complement-mediated immunity to S pneumoniae has not been investigated with human samples or in serum from subjects with C2 deficiency. Using flow cytometry assays and commercial serum depleted in specific complement factors (C1q or factor B) we demonstrate that in human serum the classical pathway is more important than the alternative pathway for complement deposition on three S pneumoniae strains, and this is associated with impaired phagocytosis of these strains in C1q-deficient serum. Both complement deposition and phagocytosis were restored to wild-type levels by addition of exogenous C1q to C1q-depleted serum. To assess the clinical importance of these observations, the C3b deposition and phagocytosis assays were repeated in serum from 10 C2 deficient subjects for three S pneumoniae serotypes. Compared to the results for serum from normal subjects, in the majority of sera obtained from C2−/− subjects C3b deposition was markedly reduced (for serotype 2 strain 12.1% of normal controls, SD 1.6%, p<0.0001) but could be restored to normal or near normal levels by addition of exogenous purified C2 (118% of normal controls, SD 19.0%, p<0.0003 compared to uncomplemented C2−/− sera). Phagocytosis of the three S pneumoniae serotypes investigated was also significantly impaired in C2 deficient sera (for the serotype 2 strain 67.1% of the level obtained in normal serum, SD 9.3%, p<0.0001) and again mainly restored by exogenous C2 (89.2% of results obtained in normal serum, SD 14.8%, p<0.0001 compared to uncomplemented C2−/− sera). These data demonstrate the vital importance of the classical pathway for complement-mediated phagocytosis of S pneumoniae and why subjects with C2 deficiency have such a marked increase in susceptibility to S pneumoniae infections.
MEASUREMENT OF C-REACTIVE PROTEIN AT DAY 4 CAN DETECT FAILURE OF EMPIRICAL TREATMENT IN COMMUNITY-ACQUIRED PNEUMONIA
J. Chalmers, A. Singanayagam, A. Hill. Royal Infirmary of Edinburgh, UK
Introduction: The aim of our study was to investigate whether combined measurement of C-reactive protein (CRP) on admission and on day 4 were predictive of outcome in community acquired pneumonia (CAP).
Methods: We retrospectively studied 570 adult patients admitted with CAP between 2005–7. CRP was measured on admission in all patients and repeat measurement made in those who remained inpatients at day 4. The outcomes of interest were: development of complicated pneumonia (lung abscess, empyema or complicated parapneumonic effusion); need for mechanical ventilation and/or inotropic support; 30-day mortality.
Results: The median age was 62 years IQR (44–76). Patients with chronic lung disease were excluded. 20% of patients had major comorbidities (chronic cardiac disease, stroke, chronic renal failure, diabetes). A CRP level that fails to fall by 50% within 4 days of admission is associated with a significantly increased risk of mortality, invasive ventilation and/or requirement for inotropic support and development of complication pneumonia (table). On multivariate analysis adjusting for age, sex, comorbidity, smoking status and severity of pneumonia (CURB65 score) a CRP that failed to fall by 50% or more at day 4 was associated with: complicated pneumonia OR 12.74 (5.07–32.03) p<0.0001; need for invasive ventilation and/or inotropic support OR 7.80 (2.84–21.37) p<0.0001; mortality OR 13.48 (3.33–54.57) p<0.0001.
Conclusion: C-reactive protein that fails to fall by 50% or more at day 4 is associated with increased risk of complicated pneumonia, need for invasive ventilation and/or inotropic support and 30 day mortality.
DEVELOPMENT OF A NOVEL MURINE MODEL OF PLEURAL EMPYEMA
S. Wilkosz, J. Yuste, M. Fernandez, N. A. Wilson, P. F. Mercer, R. Chambers, J. Brown, Y. C. G. Lee. University College London, UK
Introduction: Post-pneumonic pleural empyema is increasing especially in the paediatric population, and is characterised by the accumulation of pus, inflammatory cytokines and chemokines (for example, monocytes chemotactic protein, MCP-1) and fibrinous adhesions in the pleural space. This study describes the development of a murine model of empyema to aid investigation of the pathogenesis of pleural sepsis.
Methods and Results: Intranasal administration of 107 CFU of S pneumoniae D39 strain consistently induced pneumonia and pleural pus accumulation (80% of mice vs 0% in controls) in CD1 mice by 48 h. There was significant pleural neutrophilic leukocytosis (64.6 (32.0) vs 31.5 (16.4) ×106 cells/ml), and raised MCP-1 levels both in pleural lavage fluid (PLF) (39852 (6943) vs 23 (7) pg/ml, p<0.05) and serum (19249 (12093) vs 393 (93) pg/ml, p<0.05) (determined by ELISA, R&D). Histologically, the lungs were inflamed and haemorrhagic with fibrinous adhesions bridging the visceral and parietal pleural surfaces (Martius Scarlet Blue staining). Fatal infection developed in 75% of mice by 72 h. To induce empyema independent of pneumonia, mice were inoculated intrapleurally with 700 CFU of a less virulent S pneumoniae strain lacking the virulence factors surface protein A and pneumolysin (pspA-/ply-). Intrapleural administration of pspA-/ply- pneumococci caused leukocytosis (16.7 (3.9) vs 10.4 (4.7) ×106 cell/ml) and increased MCP-1 levels in PLF and serum (420 (147) vs 10 (7) pg/ml and 3225 (1127) vs 391 (133) pg/ml, respectively) suggesting that cells within the pleural cavity could induce the inflammatory changes observed. As mesothelial cells are abundant in the pleural cavity, mesothelial cells harvested from C57BL/6 mice and human mesothelial cells (CRL 9444 cell line) were cultured and their ability to produce MCP-1 investigated. In vitro, both murine and human mesothelial cells expressed MCP-1 constitutively. However, stimulation with thrombin, a known inducer of MCP-1, or peptide agonist (TFLLR) of the high affinity thrombin signalling receptor PAR1, demonstrated that mesothelial MCP-1 release was independent of thrombin and PAR1 activation.
Conclusions: In this study intranasal and intrapleural delivery of pneumococci both reliably induced pleural inflammation in mice with macroscopic, immunological and histological features of human empyema, suggesting that pleural mesothelial cells are directly involved in the pathogenesis of empyema.
Management and organisation of respiratory services
POTENTIAL ADVANTAGES OF AN INITIAL TELEPHONE CONSULTATION IN THOSE REFERRED FOR A SPECIALIST RESPIRATORY OPINION
C. Darlow1, N. J. Roberts1, G. Wilson2, M. R. Partridge1. 1Imperial College London, NHLI Division at Charing Cross Hospital; 2Charing Cross Hospital, Department of Respiratory Medicine, London, UK
Background: Telephone consultations have been shown to be an efficient method of following up over 30% of respiratory outpatients. An initial telephone conversation with new patients has the potential to permit better selection and timing of investigations and reduce the number of hospital attendances by patients. This study was designed to determine how accurately necessary investigations could be determined from the GPs’ referral letter and to look at how often follow-up patients currently attend the hospital before receiving a diagnosis.
Methods: Sixty five sequential follow-up patients were interviewed and their notes and investigation records examined to determine how many times they had attended for a consultation or for investigations before they received a firm diagnosis. For 28 new referrals the consultants were asked to list the investigations they thought would be necessary: (1) after reading the letter from the referring GP; (2) after they had taken the history from the patient; and (3) after they had examined the patient. A significant change between (1) and (2) and no change after (3) would suggest a potential advantage to taking the patients’ history over the telephone.
Results: Patients attended the hospital a mean 2.3 times before receiving a diagnosis and management plan. 44% (94/213) of investigations were not performed on the same day as the patients’ clinic visit. With pre-planning, potentially 76% (71/94) of those investigations could have been performed during the same hospital visit. Reading the GP referral letter alone was not sufficient to predict the investigations needed. The clinical history altered the investigations ordered in 64.3% (18/28) of patients. Subsequent clinical examination only rarely led to further changes.
Conclusions: This study suggests that patients being referred to a respiratory outpatient clinic have had several attendances before receiving a diagnosis and management plan. Taking the history by telephone has the potential to permit accurate selection of the investigations that the patient may need. These investigations could then be arranged before, or synchronously with, the first face-to-face consultation and reduce the number of hospital attendances.
AN AUDIT OF PHYSIOTHERAPY AND OCCUPATIONAL THERAPY SERVICES TO MEDICAL PATIENTS IN THE EMERGENCY PORTALS AT UNIVERSITY HOSPITALS OF NORTH STAFFORDSHIRE
E. C. Brown, S. Tudor Ansell, J. Asher. University Hospitals of North Staffordshire, Stoke on Trent, UK
Background: A process-mapping exercise of the medical patient’s journey in relation to therapies highlighted delays in the initiation of therapies on the medical wards at University Hospitals of North Staffordshire (UHNS). Data reflected an average delay in referral to Physiotherapy of 6 days and 10 days for Occupational Therapy. As a result therapies tended to run consecutive rather than in parallel to medical intervention, resulting in increased lengths of stay (LOS). This led to delayed discharge or patients being discharged without therapy interventions being complete. Adverse incident forms and complaints highlighted the resulting unsafe discharges. A Physiotherapy and Occupational Therapy service to the emergency portals (Accident and Emergency Dept, Emergency Assessment Unit and Medical Admissions Unit) was piloted in order to evaluate the impact of early therapy intervention on discharge planning. Respiratory, neurological and mobility patients were assessed in these admission units and therapy intervention initiated earlier. Clinicians facilitated the safe discharge home of patients from the units or referred patients to more appropriate care providers, such as intermediate care or supported early discharge services (COPD services). Admitted patients were referred directly to ward therapists following an admission, thus reducing the number of steps in the referral process, reducing the delay in therapy intervention.
The pilot data proved that the service facilitated direct patient discharge from the emergency portals and markedly improved the signposting of patients to other services for ongoing rehabilitation, as well as ensuring that there was no delay in referral to therapies once the patient is admitted to a ward area. During the pilot 57% (114/202) of patients referred to therapies in these units were discharged, that otherwise would have been admitted onto a ward with LOS for respiratory and mobility patients being reduced by three days. Service improvement (SIP) concluded that the impact of therapies with regards to preventing admissions, managing variation in discharge and increasing the reliability of therapeutic interventions through a “care bundle” approach (HIC 3, 4 and 6) had been significant.
Method: SIP and Therapies re-audited this service over a three-month period (December 2005–February 2006) to ensure that this service continued to deliver on its targets of: safe patient discharges, reduced LOS and admission avoidance. An audit tool collated data including referral date, reason for referral, therapy intervention required, reason for admission, discharge date and destination. Patients were followed up after three months to ascertain if they had required further admissions post-therapy discharge. Project controls were adopted to ensure the project collated valid data. This included signatures from doctors stating “this patient would have been admitted if it were not for the presence of therapies” in the emergency portals.
Results: During the audit 308 referrals were made with 206 (66%) admissions avoided as a direct result of therapies intervention; 39% (122/308) were discharged home and 27% (84/308) discharged to intermediate care. 83% of patients referred were assessed with in 4 h. Of the 102 (34%) admissions 16 (15%) were admitted due lack of intermediate care bed (ICB) availability and 10 (10%) were awaiting social services. Average emergency portals re-admission rate pre-therapy services was four visits per patient in the three-month period post-discharge. Post-therapies intervention this dropped to an average of 1.9. A total of 13 patients required emergency respiratory physiotherapy and 62 patients overall benefited from early respiratory physiotherapy intervention. Process-mapping following implementation of the service to MAU and EAU has shown that therapy referrals are communicated more efficiently as treatment is now initiated on the day of admission for physiotherapy and day two for OT on the medical wards. Early initiation of therapy referrals has led to therapies intervention occurring alongside medical intervention, so that when a patient is medically fit for discharge they are physically safe for discharge or can be referred to a more appropriate care provider, such as ICB. This has facilitates better management of variation in discharge planning and reduced length of stay (HIC 3) while ensuring equity in therapy provision.
Conclusion: The impact of therapies in the emergency portals continues to have a significant impact upon preventing admissions, reducing LOS, managing variation in discharge and increasing the reliability of therapeutic interventions through a “care bundle” approach (HIC 3, 4 and 6). These findings support the investment in therapy services in the emergency portals as it is of financial benefit to both primary and secondary care providers while also enhancing the patient’s quality of care.
BENCHMARKING CHRONIC OBSTRUCTIVE PULMONARY DISEASE ACROSS AN INNER CITY PCT-WIDE POPULATION
J. A. Roberts, N. Diar Bakerly. Salford Royal Foundation Trust and Salford PCT, UK
Introduction: Our primary care trust (PCT) population (n = 236 919) has high levels of social deprivation, health inequalities and COPD and comprises 59 practices, structured as eight practice-based commissioning clusters. The COPD register structures COPD consultations in line with current guidelines using a standardised template that sits within existing GP computer systems across the PCT. Anonymised data are collected remotely at three-month intervals. We hypothesised that practices clustered in areas of highest deprivation would have higher rates of COPD, more severe disease and a higher use of NHS resources.
Aims: To establish baseline level of recorded severity of COPD by FEV1% predicted mapped to deprivation across the whole PCT population and by practice cluster. To establish baseline levels of maintenance treatments for COPD, specifically long-acting bronchodilators (LABAs), anticholinergics and inhaled corticosteroids (ICS).
Methods: We retrospectively analysed the baseline data collected from the COPD register: FEV1 % predicted, smoking status, BMI, current medication. We are currently analysing the number of unscheduled COPD admissions from the Department of Health hospital episode statistics data for the year 2006/7. Outcomes for individual practices, aggregated to practice cluster, will be analysed using multiple regression techniques, adjusting for the demographics of the practices.
Results: Data from the preliminary analysis are reported; QOF prevalence 2.3% n = 5501, (range 0.1%–4.7% across all 59 practices). Of 38 practices with available data for analysis: 4534 COPD patients (48.5% male); mean age of 68 years; 41% current smokers, 12.5% never smoked; mean BMI 27 kg/m2; spirometry in the last 15 months recorded on 2577 (57%) patients; mean %predicted FEV1 56%; severity by FEV1% predicted values, 50% mild, 30% moderate, 9% severe (NICE, 2004); 11% had an FEV1 %predicted value >80%. Of 4534 patients: 29% received ICS without LABA; 7% received LABA alone; 35% received both ICS and LABA; 42% were receiving anticholinergics (both short and/or long-acting); % patients who received both ICS and LABA 32% mild, 47% moderate, 58% severe COPD.
Conclusions: In this population prevalence of COPD is higher than the national average and more common in females. COPD is recorded in 12.5% of never smokers and in 11.1% of the population with FEV1>80% predicted. Combined therapy with ICS/LABA is prescribed more frequently in those with moderate to severe disease. Further analysis of these data will provide valuable information for planning service delivery to meet the health needs of this population.
THE FIRST SIX MONTHS OF HOSPITAL AND COMMUNITY-BASED OXYGEN ASSESSMENT SERVICE FUNDED BY A PRIMARY CARE TRUST
K. Pye, C. Stevens, A. Kwok, L. Davies. University Hospital Aintree, Liverpool, UK
Background: In 1999 guidelines for domiciliary oxygen services were published; however deficiencies remained. The Clinical Component for the Home Oxygen Service 2006 recommends that assessment for home oxygen should be the responsibility of a respiratory specialist in secondary care. Funding was devolved to the primary care trusts (PCTs). At Aintree Chest Centre, Liverpool, a nurse-led oxygen assessment service taking referrals from secondary care, on an ad hoc basis, has been operational for five years. In October 2006, Sefton PCT funded an oxygen assessment service to allow assessment of all patients receiving domiciliary oxygen within that PCT.
Methods: In October 2006, with information from Air Products, Sefton PCT established a database of all patients receiving oxygen. 380 patients were identified as receiving either long-term (LTOT) or short burst (SBOT) oxygen therapy.
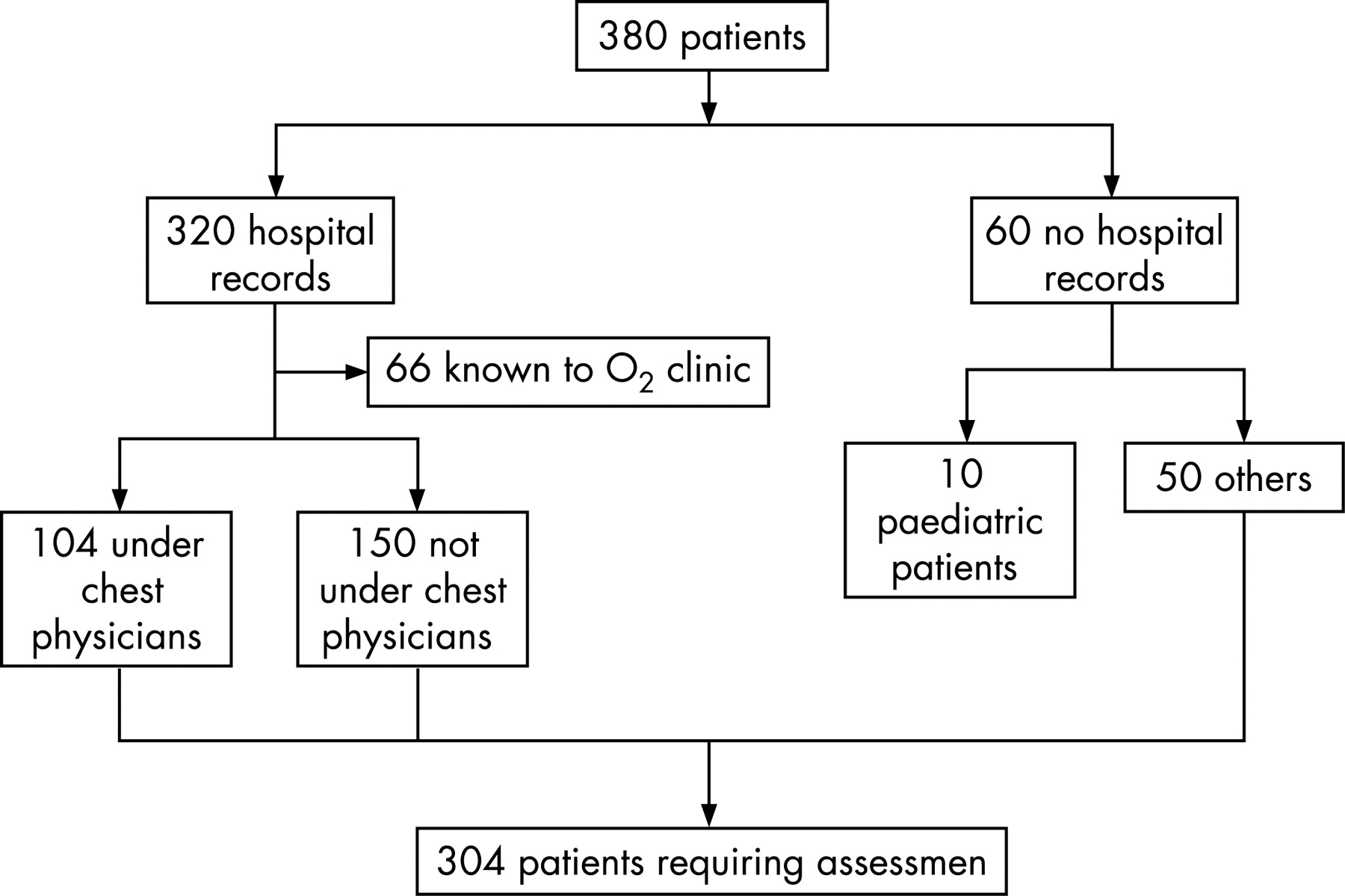
Results: After initial review of the 304: 81 had died since the database was received, 18 palliative care, 11 receiving O2 with NIV, 8 cluster headaches, 13 are still waiting appointment, 4 repeatedly DNA’d, 4 declined appointment, 4 moved away from the area leaving 161 (68 male) assessed. All patients were reviewed by experienced respiratory nurse specialists according to accepted guidelines either in a hospital or primary care outreach oxygen clinic, or at home (n = 17). 86/161 (53%) patients, 54 female, mean (SD) 73 (10) years were outside the criteria for either long-term oxygen therapy (LTOT) or ambulatory oxygen. Of these 70 (81%) had COPD, 5 (6%) had asthma, 5 (6%) pulmonary fibrosis, 3 (3%) obstructive sleep apnoea, 3 (3%) heart disease. Following assessment, four patients on SBOT were subsequently prescribed LTOT.
Conclusions: Nurse-led oxygen assessment is deliverable in the hospital and community setting. Around half of patients receiving domiciliary oxygen are currently receiving this unnecessarily. In our practice, results of assessments were sent to all GPs and the decision to remove the oxygen equipment was left to individual practitioners. We will review whether our recommendations are acted upon and would like to move to a service in which, apart from emergencies, patients are assessed for oxygen therapy before HOOF completion.
AN INTEGRATED HOME OXYGEN SERVICE SAVES £130,000 PER YEAR ON HOME OXYGEN TARIFFS
C. Deeming, L. Ward, J. Townsend, G. Lingam, S. Ansari, D. Powrie, A. Davison. Southend University Hospital, Essex, UK
In February 2006 a new home oxygen service was introduced to improve the assessment of patients on oxygen and allow access to newer technologies such as ambulatory oxygen. Oxygen is provided following completion of a home oxygen order form and is allocated a tariff according to delivery device and usage. There are 54 tariffs ranging from 34 p/day (standard portable cylinder <2 l/min, <1 h/day) to £27.90/day (long-term oxygen therapy plus standard portables >6–8 l/min, >4 h/day). In South East Essex there are 554 patients receiving home oxygen with an annual cost of £668,546.
South East Essex PCT and Southend Acute Trust set up an integrated home oxygen service comprising four respiratory consultants, one respiratory physiotherapist and three respiratory nurse specialists (one community-based). The role of this service is to identify patients requiring home oxygen, to provide formalised oxygen assessments and home or outpatient monitoring once oxygen is ordered.
In order to investigate high oxygen order costs 22 patients with a tariff of more than £5/day were identified from the BOC monthly statement of December 2006 for review. Of these, four had the correct order, three no longer required home oxygen, one was unwilling to change his order and 14 were re-categorised to a lower tariff. This resulted in an annual saving of £76,993. Over the following six months during routine follow-up a further 43 patients had their home oxygen order re-categorised. Eight no longer required home oxygen and 35 were re-categorised with an annual saving of £52,819.
Recognition of the need to regularly re-evaluate patients on home oxygen resulted in a cost saving of £129,812/year. A saving of £76,993 was made by targeting just 22 patients on the highest tariff.
COSTS IMPLICATIONS OF OXYGEN PRESCRIPTION WITHIN A PCT, IF NOT SUPPLIED BY A SPECIALIST RESPIRATORY TEAM
M. Buxton. North West London Hospitals Trust & Brent PCT, London, UK
Introduction: In February 2006, oxygen services changed over to a single provider system. The British Thoracic Society (BTS) working group on Home Oxygen Services published a guidance document in January 2006 on the clinical standards for assessment and prescription of oxygen therapy. Although GPs could still prescribe all forms of oxygen, long-term oxygen therapy (LTOT), short burst oxygen therapy (SBOT) and ambulatory oxygen on the HOOF (Home Oxygen Order Form), the BTS working group recommends that LTOT and ambulatory oxygen should be carried out by specialist respiratory teams, for assessment and ongoing follow-up. This paper aims to look at primary care trust (PCT) cost implications when oxygen is not overseen by a specialist respiratory team.
Method: Between April and May 2006, Brent PCT commissioned a small specialist team headed by the Consultant Physiotherapist, to evaluate all the oxygen prescriptions, with the aim of: (1) converting all Emergency Orders to regular tariff (n = 17); (2) converting all patients on FP10 prescriptions (oxygen previously provided by local pharmacists) over to the HOOF system (n = 84). However, at the time of reviewing the FP10 patients, 28 had been converted via HOOF forms by GPs and 23 were not appropriate for prescriptions. Consequently the final number of FP10 patients to covert to the HOOF system by the respiratory specialist team was 32. All oxygen prescriptions were not evaluated for quality of prescription, as this was a simple cost exercise. Ambulatory oxygen prescriptions were not addressed. Compiling an accurate database on patients within Brent who were receiving oxygen required the comparison of patients’ names from the previous oxygen provider, the GP practices and the Brent Prescribing Team. Emergency tariff patients’ prescription data were obtained from the provider, and this prescription was cancelled and converted into a normal tariff. The respiratory specialist team contacted the FP10 patients and also occasionally their GP to discuss their oxygen usage before completing a HOOF.
Results: Emergency orders (n = 17); days on Emergency Tariff, 8–129 days; FP10 patients GP completed HOOF = 28; not appropriate = 24; final number patients to convert to HOOF = 32. HOOF prescription on FP10 patients: GP prescription n = 28 LTOT = 20, SBOT (concentrators) = 5, SBOT (cylinders) = 3; Specialist Team n = 32 LTOT = 3, SBOT (concentrators) = 3, SBOT (cylinders) = 26. Cost of FP10 patients/year: SBOT (cylinders) n = 29 £4,128.15; SBOT (concentrators) n = 8 £3,533.20; LTOT n = 23 £11,836.95. Actual cost saving for 2006/7 by: cancelling emergency orders and replacing with normal tariff HOOF n = 17, £54,131.46; prescribing cylinders vs concentrators for SBOT (saving of £299.30/patient/year) n = 29, £8,679.70. Actual cost of oxygen prescriptions: total number of oxygen prescriptions in 2006/7 = 175, April 2007 = 280 (increase of 60%); total cost of oxygen prescription for 2006/7 = £173,864.09 (DH funding = £84,000).
Analysis: There is a considerable cost saving in cancelling emergency tariffs, and by prescribing cylinders rather than concentrators for SBOT. However, prescribing LTOT without specialised assessment as recommended by the BTS working group appears to be a common practice in primary care.
Conclusion: Respiratory specialist teams have the knowledge and expertise to assess the need for oxygen in chronic respiratory patients. Oxygen is costing PCTs much more than the funding supplied by the DH; therefore the need for accurate prescription is essential. Incorrect prescription of oxygen is not only costly, it also has serious implications for our patients. Commissioning respiratory specialist teams to provide assessment and follow-up of oxygen prescription within the PCT could have major impacts on cost and improve the appropriateness of prescription and subsequent management of these patients enormously.
Systemic aspects of COPD
QUADRICEPS MUSCLE ENDURANCE AND ITS RELATION TO PHYSICAL ACTIVITY AND EXERCISE CAPACITY IN COPD
S. A. Sathyapala1, G. S. Marsh1, N. S. Hopkinson1, J. Moxham2, M. I. Polkey1. 1Royal Brompton Hospital; 2King's College Hospital, London, UK
Introduction: Quadriceps muscle dysfunction appears to correlate with exercise capacity and activity in COPD. However, quadriceps endurance (Qend) has previously been assessed with volitional tests and activity with questionnaires which quantify activity poorly. We have described a non-volitional test of Qend using repetitive magnetic stimulation.
Aim: To investigate, in COPD patients and healthy controls, relations between non-volitional Qend and (1) activity quantified by a motion sensor (2) exercise capacity.
Methods: Thirty GOLD Grade II-IV COPD patients and 13 healthy controls had lung function, arterialised capillary earlobe blood gases and right leg isometric quadriceps maximal voluntary contraction (MVC) measured. Right leg Qend was assessed with a magnetic stimulator (Magstim, UK), powered to generate 20% of MVC, delivering 50 trains of 30 Hz magnetic stimulation with a 0.4 duty cycle through a mat coil over the muscle body. Time until the force-time product (FTP) fell below 80% of the initial FTP (T80) was noted. Activity was measured with a tri-axial accelerometer (Dynaport, McRoberts, The Netherlands) worn for 12 h/day for 2 days and the results averaged. Exercise capacity was assessed by symptom-limited incremental cycle ergometry with metabolic testing and a 6 minute walk test (6MW). Analysis of group differences was performed using the unpaired Student t test and Mann-Whitney U test according to data distribution and correlations by simple regression analysis.
Results: T80 was (40%) shorter in COPD patients than controls. T80 correlated positively with FEV1, TLCO, PaO2 (r = 0.46 p = 0.04, r = 0.34 p = 0.046, r = 0.37 p = 0.03) and negatively with RV/TLC (r = −0.36 p = 0.03) in patients but not controls. With patients and controls together (but not separately), T80 correlated positively with time spent walking (r = 0.40 p = 0.02) and Mi (r = 0.38 p = 0.03) and negatively with time spent seated (r = −0.40 p = 0.02). T80 correlated with peak VO2 (r = 0.41 p = 0.01) but not 6MW distance.
Conclusion: Qend is reduced on average by 40% in patients with COPD compared to controls rather than by 70–80% reported with volitional tests. Qend appears to be associated with daily duration and intensity of movement and correlates with performance on a cycling test but not on a 6MW test.
EMPHYSEMA SEVERITY IS ASSOCIATED WITH ARTERIAL STIFFNESS, A MARKER OF CARDIOVASCULAR RISK
D. A. Mcallister, J. D. Maclay, N. L. Mills, G. Mair, J. J. Miller, D. Anderson, J. T. Murchison, D. E. Newby, J. T. Murchison, W. Macnee. University of Edinburgh, Edinburgh, UK
Rationale: More patients with COPD die from cardiovascular causes than from respiratory, and patients with COPD have increased morbidity and mortality from coronary heart disease. Arterial stiffness independently predicts cardiovascular risk and is increased in COPD patients compared with controls matched for cardiovascular risk factors. Elastin fragmentation and changes in collagen are found in the connective tissue of both emphysematous lungs and stiff arteries, but it is not known whether the severity of arterial stiffness in patients with COPD is associated with the severity of emphysema.
Objective: To identify whether the extent of arterial stiffness is associated with emphysema severity.
Methods: We measured pulse wave velocity (a validated measure of arterial stiffness), blood pressure, smoking pack years, glucose, cholesterol and C-reactive protein and assessed emphysema using quantitative CT scanning in a subgroup of 73 patients with COPD.
Results: We found that emphysema severity was associated with arterial stiffness (r = 0.476, p<0.001, fig A), more closely than FEV1% predicted (fig B). The association was independent of smoking, age, sex, FEV1% predicted, highly sensitive C-reactive protein and glucose concentrations, cholesterol:HDL ratio, and oxygen saturations.
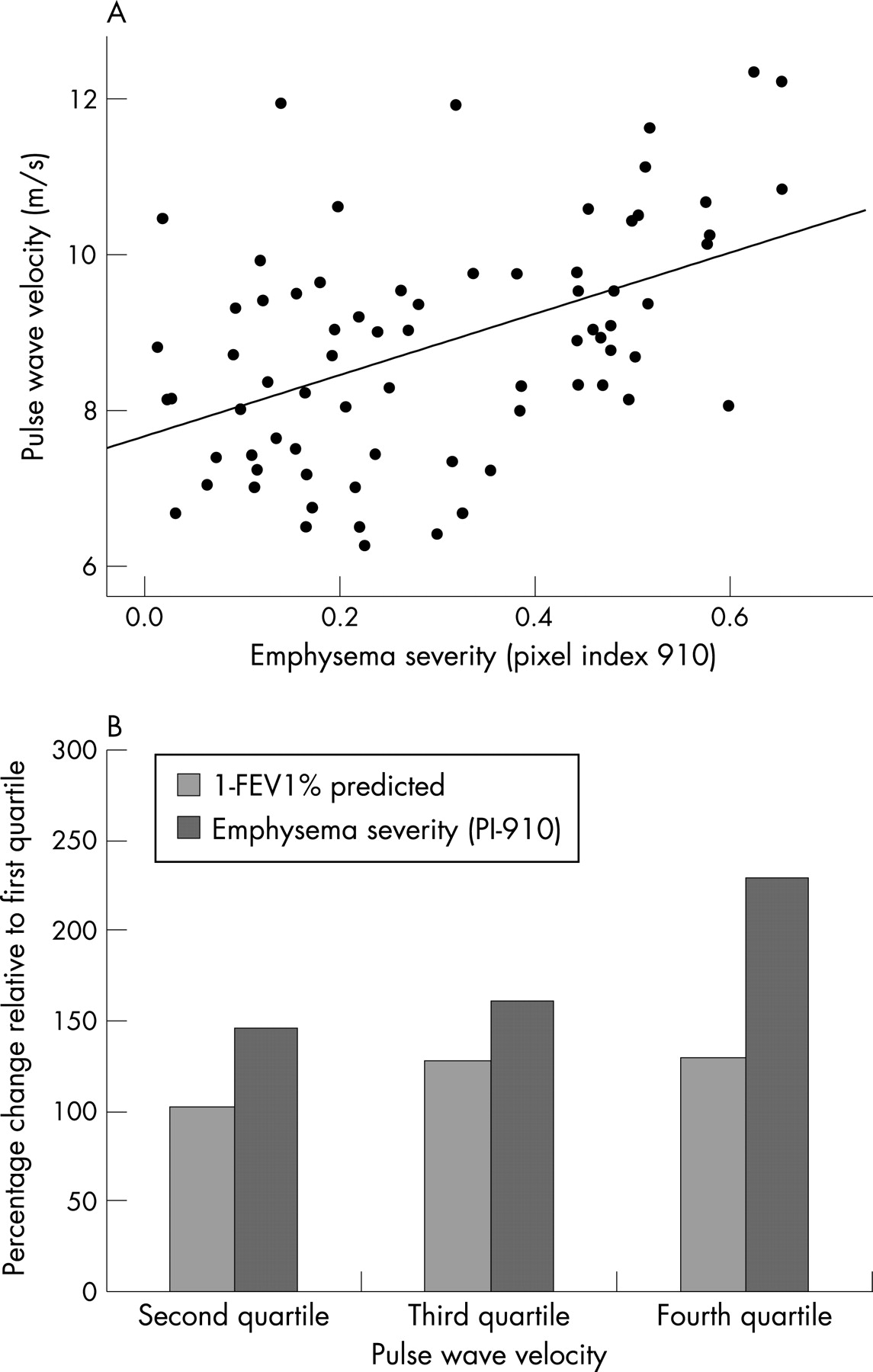
Conclusion: In this, the first study to relate emphysema to any marker of cardiovascular risk, emphysematous patients appear to be at increased cardiovascular risk. This result needs to be confirmed longitudinally and mechanistic studies are required to identify the underlying pathophysiology.
PREVALENCE OF ANAEMIA IN STABLE STATE AND DURING EXACERBATION IN A COHORT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATIENTS
M. S. Anwar, K. Ibrahim. Whipps Cross University Hospital, London, UK
>Background: Chronic obstructive pulmonary disease (COPD) is considered to be primarily a respiratory disease but there is now increasing evidence of the systemic effects involved in this condition. The historic COPD literature demonstrates an association of COPD with polycythaemia secondary to chronic hypoxemia. Some recent studies have suggested that anaemia is also prevalent in COPD. It has been reported that the prevalence of anaemia in a US study of a large cohort of COPD patients is as high as 33%. This is a similar figure to that observed in patients with chronic rheumatoid disease and chronic renal and heart failures. The suggestion is that the observed anaemia is a consequence of systemic inflammatory mediators. No studies have yet been reported from the UK and no studies have to date compared the prevalence of anaemia in COPD patients in the stable clinical state with those during an exacerbation when systemic inflammation may be significantly increased.
Method: We designed a retrospective, observational study to explore the prevalence of anaemia in a cohort of COPD patients measured both in the stable clinical state and also during a hospitalised exacerbation. A cohort of 1325 patients with a coded primary discharge diagnosis of COPD admitted to a University Hospital in London from January 2004 to December 2005 was selected. Of these, 458 patients had spirometry results available that could be used to confirm the presence of significant airflow obstruction. 147 of these patients were further excluded from subsequent analysis as they had concurrent medical conditions known to cause anaemia. A further 19 patients were excluded as their spirometry results did not meet the criteria for COPD diagnosis. The remaining 292 patient (168 males) results were analysed.
Results: The overall prevalence of anaemia was 15.2%, during the stable state and rising to 21.8% in the same patients during exacerbation. In stable COPD patients, anaemia (defined as haemoglobin (Hb) <12 g for females and <13 g for males) was significantly more prevalent in females (16.1%) than males (14.3%) (p<0.001). However, during COPD exacerbations, this difference was reversed with 18.6% of females and 25% of males exhibiting anaemia (p<0.001). In stable COPD state, anaemia was normocytic in 90% of females and 95.8% of males. During COPD exacerbation the anaemia was normocytic in 87% of females and 88.1% of males. During stable state, 5% of females and 2% of males had polycythaemia (defined as haematocrit >0.48 in females and >0.54 in males). This has not changed significantly during exacerbations. During stable state, haematocrit was low in 15.3% of females and 14.3% of males while during exacerbation, it was significantly lower; 21% in females and 27.4% in males. In both stable and exacerbation states we found that haematocrit, albumin and to a lesser degree creatinine correlated positively with the degree of anaemia (p<0.001, p<0.005 and p<0.031 respectively). However there was no significant correlation between Hb level and CRP in both stable and exacerbation states. We did find some, but not statistically significant, correlation between FEV1% predicted and the degree of anaemia.
Conclusion: This study has shown a significant prevalence of anaemia in our stable patients, albeit a lower level than reported in the US series. During an exacerbation the prevalence of anaemia rises, with the haematocrit dropping significantly. The fall in Hb and haematocrit were both more prominent in the men studied than the women. It is notable that we found no significant correlation between all levels of Hb and the measured FEV1 in both stable and exacerbation states.
COPD IS ASSOCIATED WITH ABNORMAL VASCULAR ENDOTHELIAL FUNCTION
J. D. Maclay, D. A. Mcallister, N. L. Mills, E. Drost, D. E. Newby, W. Macnee. University of Edinburgh, Edinburgh, UK
Introduction: Patients with COPD have increased cardiovascular morbidity and mortality, independent of traditional risk factors including smoking (Sin et al, Circulation 2003). Systemic inflammation is a well-recognised feature of COPD and inflammation plays a central role in the pathogenesis of atherosclerosis. We have previously shown that acute systemic inflammation causes impairment of vascular endothelial function (Chia et al, J Am Coll Cardiol 2003). Thus we believe that patients with COPD will have abnormal endothelial function which may contribute to their increased cardiovascular risk.
Methods: Twelve male ex-smokers with COPD and seven healthy ex-smokers were recruited for this pilot study with no history of cardiovascular disease, diabetes or inflammatory disorders, and not taking statins, ACE inhibitors or anti-inflammatory drugs. These groups were matched for age and smoking history. Using venous occlusion plethysmography, we measured change in forearm blood flow following infusion of the endothelium-dependent vasodilator acetylcholine (5–20 μg/min) and the endothelium-independent vasodilator sodium nitroprusside (2–8 μg/min) into the brachial artery.
Results: There was no difference in resting forearm blood flow between patients and controls. There was a dose dependent increase in forearm blood flow in response to both vasodilators (p<0.0001), however the response to acetylcholine was reduced in COPD patients (peak response, 5.2 (3.1) vs 7.5 (2.8) ml/100 ml of tissue/min; two-way ANOVA p<0.01). There was no difference in sodium nitroprusside mediated vasodilatation (peak response, 9.5 (1.8) vs 10.2 (2.1) ml/100 ml of tissue/min; two-way ANOVA p = 0.30); see fig.
Conclusion: In this preliminary study we have shown that patients with COPD have impaired endothelial vasomotor function compared to controls matched for age, sex and smoking history. In ongoing studies, we will determine whether other aspects of vascular function including endogenous fibrinolysis are altered in COPD.

SUBCLINICAL BI-VENTRICULAR DYSFUNCTION IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE
R. Sabit1, C. E. Bolton1, J. M. Edwards2, P. H. Edwards1, J. R. Cockcroft2, A. G. Fraser2, D. J. Shale1. 1Respiratory Medicine, Cardiff University; 2Department of Cardiology, Cardiff University, UK
Background: Cor pulmonale occurs with severe airways obstruction and hypoxaemia in late stage COPD and indicates a poor prognosis. Other cardiovascular complications in COPD include increased arterial stiffness and atherosclerosis, even when confounders are accounted for. We hypothesised that subclinical left (LV) and right ventricular (RV) dysfunction occurs in milder severity COPD reflecting pulmonary and systemic haemodynamic impacts of the disease.
Methods: Thirty six clinically stable patients with COPD (19 male) and 14 age and sex matched smoking controls were studied. All subjects were free of overt cardiovascular disease and had no clinical evidence of left or right ventricular failure. Subjects underwent spirometry, tissue Doppler echocardiography (measuring velocities and deformation) (Vivid 7), measurement of aortic pulse wave velocity (PWV) (SphygmoCor) and arterialised capillary PaO2 (patients only).
Results: Patients, mean (SD) age 66.5 (8.9) years had a mean (SD) FEV1 of 1.46 (0.58) l and a mean (range) PaO2 of 70 (57–88) mmHg. Compared with controls, patients had evidence of global diastolic and regional LV systolic dysfunction, with a longer isovolumetric relaxation time (IVRT) (p<0.001) and lower LV strain (p<0.01) and peak systolic strain rate (p<0.001). Aortic PWV was greater in patients (11.5 (2.9) m/s) than controls (9.5 (1.3) m/s). Patients had evidence of RV regional systolic and diastolic dysfunction with a lower RV peak systolic velocity (p<0.05), strain (p<0.001), peak systolic strain rate (p<0.001), and a greater RV myocardial relaxation time (p<0.001). Pulmonary acceleration time (p<0.01), post-systolic strain index (PSSI) and Tei index (both p<0.001) were greater in patients compared with controls suggesting increased RV afterload. LV and RV systolic and diastolic dysfunction was present in patients with milder airways obstruction (FEV1>50% predicted) compared with controls. In multiple regression analysis, aortic PWV was the only predictor of LV IVRT (r2 = 0.22, p<0.01), while FEV1 was a predictor of both Tei index (r2 = 0.25, p<0.01) and RV myocardial relaxation time (r2 = 0.22, p<0.01).

Conclusions: Patients with mild severity COPD have evidence subclinical LV and RV dysfunction suggesting early occurrence in the disease process. RV dysfunction is related to the severity of lung disease, while LV dysfunction is related to increased aortic stiffness.
Acknowledgement: Supported by GlaxoSmithKline.
Pulmonary rehabilitation in practice
CAN SENSEWEAR ACTIVITY MONITORS DETECT SLOW SPEEDS OF WALKING IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE?
R. D. Smith1, L. Sewell2, O. Cain2, S. Singh2, M. Morgan2. 1Coventry University; 2University Hospitals of Leicester NHS Trust, UK
Background: One aim of pulmonary rehabilitation is to increase the daily physical activity for patients with COPD. The SenseWear activity monitor (BodyMedia Inc, Pittsburgh, PA, USA) is a device that measure activity in energy expenditure (kcals) and metabolic equivalents (METS). It is a small, light device worn on the back of the upper arm. The usefulness of the SenseWear activity monitor has not been established in patients with COPD at their slow walking speeds. We aimed to investigate if SenseWear activity monitors can accurately measure activity at slow walking speeds and discriminate between different speeds using the incremental shuttle walk test (ISWT) in patients with COPD.
Method: Twenty six patients (18 male) mean (SD) FEV1 47.12 (26.21)% predicted, age 71 (9) years, BMI 26.03 (5.32) kg/m and median MRC grade 3 (range of 1–5) were recruited from the pulmonary rehabilitation programme. Patients wore the activity monitor 2 min prior to completing the ISWT. 11 subjects repeated the test. Outcome measures reported are minute-by-minute METS. To explore the difference between speeds ANOVA and Tukey post hoc was employed; repeatability was examined with the intra-class correlation (ICC).
Results: All 37 ISWT completed the first level (at 1.8 km/h) of the ISWT, 31 of those completed level 2 (2.44 km/h), 28, 20, 16 and 11 completed levels 3 (3.03 km/h), 4 (3.63 km/h), 5 (4.25 km/h) and 6 (4.86 km/h) respectively. Mean ISWT was 201 (127) m (range 30–560 m). An increase in activity was recorded with an increasing walking speed (fig 1). ANOVA identified a statistically significant difference between METS values between the walking speeds (p<0.005). Post hoc analysis identified that each walking speed generated a statistically significant difference for MET values compared to all of the speeds (p<0.005) except between 3.63 km/h and 4.25 km/h (p = 0.019). ICC was r = 0.95 (p<0.005).
Discussion: The SenseWear activity monitors can detect activity at slow speeds of walking and can also distinguish differences in estimated energy expenditure at different walking intensities employed in the ISWT. The SenseWear activity monitor is an acceptable method of measuring activity in patients severely disabled by COPD.

ELIGIBILITY FOR AMBULATORY OXYGEN ASSESSMENT CHANGES FOLLOWING A PULMONARY REHABILITATION PROGRAMME
J. A. Smith1, N. I. O'Kelly1, E. Hill1, B. J. Smith2. 1Primary Care Trust, Linconshire; 2Birmingham Medical School, UK
Background: The provision of ambulatory oxygen within the National Health Service is a relatively new option for patients with chronic respiratory disease. Consequently, there are few examples of integrated referral pathways for assessment of suitability for this therapy. National guidelines exist that define the eligibility criteria for ambulatory oxygen assessment (SpO2 drops by ⩾4% and to below 90% from baseline), and recommend that this should occur following completion of a pulmonary rehabilitation (PR) programme. Despite this, many patients currently receive ambulatory oxygen therapy (AOT) without an assessment. This retrospective observational quantitative study investigated the impact of PR on the oxygen saturation in patients with chronic obstructive pulmonary disease (COPD).
Method: Patients chosen for this study had completed a PR programme between 2005 and 2007 (n = 177). To determine eligibility for AOT assessment, all patients had pulse oximetry measurements performed before and after an endurance walking test both at the start and on completion of the PR programme. Looking at the retrospective data, patients were divided into four groups depending on their eligibility at baseline and on completion of the PR programme (see table).
Results: See table.
Discussion: Nineteen patients (10.7%) who did not meet the eligibility at baseline subsequently did after the PR intervention. These patients would not have been put forward for formal AOT assessment and thus, may have lost out of the potential benefit of receiving this therapy. Also 12 patients (6.8%) who did meet the eligibility criteria at baseline subsequently did not after completion of the programme. These patients did not require referral for formalised AOT assessment. At a time when financial balance within health economies is paramount, having an efficient pathway to ensure that the correct patients are referred to formalised AOT assessment services is sensible. Incorporating baseline and final assessments of SpO2 within a PR programme may provide a cost efficient solution to this challenge.
Conclusion:The above findings would seem to concur with the AOT guidelines and support the recommendation that patients should be offered PR prior to AOT assessment.
DOES PULMONARY REHABILITATION IN PATIENTS WITH “NON-COPD” CHRONIC RESPIRATORY DISEASE CONFER SIMILAR BENEFITS TO THAT IN PATIENTS WITH COPD?
I. J. Benton1, E. Hilsden1, T. Lines1, D. J. Shale2, C. E. Bolton2. 1LlandoughHospital; 2Respiratory Medicine, Cardiff University, UK
Background: Improved exercise tolerance and quality of life following pulmonary rehabilitation (PR) in patients with COPD is proven through large randomised controlled trials. The gains in other chronic respiratory conditions are less clear, with reports suggesting some benefit. However, these conditions have differing pathophysiology, responses to exercise and nature of symptomatic exacerbations. We explored the effect of PR in different patient subgroups.
Method: We reviewed patients entering PR, comprising a standard 18 session (3/week) course including education, exercise prescription, relaxation and goal setting, over the last 16 months. At the start and completion of PR, an incremental shuttle walk test (ISWT), St George’s Respiratory Questionnaire (SGRQ) and hospital anxiety depression score (HAD) score are performed. Patients were subdivided into “COPD” or “non-COPD”.
Results: Over the observation period, 171 patients were entered for PR of which 166 commenced (96 male), mean (range) age 67.6 (39–88) years. There were 144 with a primary diagnosis of COPD and 22 had “non-COPD” chronic respiratory disease; 12 ILD and 10 bronchiectasis. The two groups had similar SGRQ scores and HAD scores (table 1). There was a trend for shorter ISWT in the non-COPD group (p = 0.06) and the non-COPD group (27%) tended to drop out more compared with COPD (14%), p = 0.1. The gain in ISWT and improvements in SGRQ domains and the total score and the HAD scores were similar in both groups (see table 2).
Conclusion: Determining the benefit of PR in different disease populations is important both for the patient and service development and planning. The groups had similar baseline measurements and improvements were comparable. These data suggest encouraging patients with a range of chronic respiratory disease to enter PR. There is a need to determine why the drop out rate for the non-COPD patients is greater, which may be related to intercurrent infections in bronchiectasis or not meeting the expected goals.
Acknowledgement: With thanks to the Pulmonary Rehabilitation Staff.
ASSESSMENT OF PULMONARY REHABILITATION PROGRAMME WITHOUT THE PHYSICAL TRAINING
C. I. Bloom1, C. Howard2, T. Hargadon2, S. Dupont3. 1Hillingdon Hospital, London; 2Hillingdon Primary Care Trust, London; 3Central and North West London Mental Health Trust, UK
Introduction: The NICE COPD guidelines recommend pulmonary rehabilitation (PR) should be made available to all appropriate patients. The guidelines state grade A evidence that PR should include a programme of physical training, disease education, nutrition education, psychological and behavioural intervention. In many hospitals access to PR is not available because of lack of funding and facilities required for the physical training. This study looked to see if a PR programme without physical training could improve patient’s health status, reduce A&E attendances and reduce length of stay (LOS).
Method: Clinics were run by a multidisciplinary team and were held for two hours every week for four weeks. Patients included fulfilled the same criteria recommended in the NICE guidelines for PR. Carers also attended. Quantitative data were collected using the Hospital Anxiety and Depression (HAD) scale questionnaire and the St George’s Respiratory Questionnaire (SGRQ) at the start of clinic, end of clinic and 6 weeks post clinic. A&E attendances and LOS data were obtained on the study patients and an equal number of case matched control patients, for a six-month period before and after the clinic. The controls were matched for age, sex and FEV1. Statistical analysis was performed using ANOVA.
Results: There were 48 patients eligible, of which 60% were male and the mean (SD) age was 71 (9.6) years. Patients had a mean FEV1 of 32.8 (7.9) % predicted. Nearly half of the patients brought a carer with them. 33 patients attended all four clinics; illness and hospital transport problems were the reasons for non-attendance. The control group had a mean age of 72.9 (10) years and mean FEV1 of 33.3 (5.7) % predicted. The mean scores pre-clinic, at the end of clinic and post-clinic for depression were 8.9, 7.8 and 7.5 (p<0.01), for anxiety 10.7, 10.3 and 9.7 (p>0.05), for SGRQ were 72.2, 67.1 and 67.1 (p<0.05). The total number of A&E attendances was significantly lower in the intervention group vs the control group: at six months pre-clinic this was 43 and 56 respectively, and at six months post-clinic this was 32 and 81 respectively (p<0.001). The total hospital LOS (days) was significantly lower in the intervention group vs the control group: at six months pre-clinic this was 119 and 132 respectively, and at six months post-clinic this was 114 and 199 respectively (p<0.001). The reduction in A&E attendances and LOS gave an estimated total saving of £63,000 compared to the six month running cost of £15,000. Post-clinic evaluation showed over 90% of the participants “moderately to strongly agreed” the clinic was beneficial.
Conclusion: After attending our PR programme there was a significant fall in the SGRQ and depression scores, number of A&E attendances and LOS. Also when compared to the control group there was a significant fall in A&E attendances and LOS. The PR programme was both economically valuable and subjectively valuable to patients and carers. We conclude that patients, carers and the hospital benefit from a PR programme without physical training.
EARLY OUTCOMES OF A PULMONARY REHABILITATION MAINTENANCE PROGRAMME
S. Ives-Lappin2, L. Visker2, W. Mitchell2, S. Martin2, R. C. Buttery1.1Hinchingbrooke Hospital NHS Trust, Huntingdon, UK; 2Cambridgeshire Primary Care Trust, UK
Introduction: Although the benefits of pulmonary rehabilitation (PR) are now well recognised, most programmes are offered as a one-off treatment episode and as yet there are no clear strategies for maintaining these benefits. We report early outcomes on a group of patients undergoing a pulmonary rehabilitation maintenance programme with individually tailored exercise regimes. Pulmonary rehabilitation is defined as a “multidisciplinary program of care for patients with chronic respiratory impairment that is individually tailored and designed to optimise physical and social performance and autonomy” (ATS, 1999). Exercise intolerance is complex and results from: ventilatory limitation, due to hyperinflation and impaired gas exchange; premature muscle failure due to hypoxaemia and lactic acidosis; and skeletal and cardiac muscle deconditioning. Exercise training improves skeletal and cardiac muscle function, and improves mood, motivation and symptoms. There is extensive evidence that PR improves exercise capacity, fatigue, dyspnoea and patients’ perception of control over their disease. The treatment effect of PR on health-related quality of life and functional exercise capacity is greater than other modalities used in COPD, such as bronchodilators, and it is an extremely cost-effective intervention. However, these effects wane from 6–12 months, although quality of life benefits are still detectable at 2 years. Additionally, this group of patients are often socially isolated by their disease and feel it difficult to exercise at local public facilities such as leisure centres. There is thus no easily identifiable mechanism for maintaining fitness for patients who have attended a formal PR programme. We hypothesised that a locally-based exercise programme would offer many benefits for this group: it would present a secure environment for exercising, with paramedical support, and would therefore extend the benefits of pulmonary rehabilitation; it would act as a natural social support group; and it would act as a focal point for early intervention to prevent exacerbations of the underlying lung disease.
Methods: All patients in Cambridgeshire Primary Care Trust Huntingdon locality, who had been through a full pulmonary rehabilitation programme (based at Papworth Hospital NHS Foundation Trust) between 6 months and 3 years previously, were invited to attend a six-week PR maintenance programme at a local health centre in Huntingdon. The programme was supported by two respiratory physiotherapy technical instructors and group size was limited to eight patients. The course was centred upon individualised, patient-targeted goals and home exercise plans; pedometers were used throughout the course, with individual weekly targets. Assessments were made at Week 1 and Week 6 of the following: FEV1, FVC and FEV%, SaO2, 6-minute walk, exercise capacity in an individualised exercise circuit, MRC breathlessness score and quality of life score.
Results: Two groups (A and B) have completed the course so far. A total of 8/15 (53%) invited patients have attended and completed the course. Of the seven who declined or failed to complete, 2/7 have declined long term; 4/7 failed as a result of unrelated intercurrent illness and are rebooked to attend later groups; 1/7 attends an alternative local exercise group. Of the eight who have so far completed the course, one persevered despite developing an unrelated severe respiratory condition (excluded from analysis). After 6 weeks, FEV1 improved by a mean of 8.7%, FVC increased by a mean of 6.1%. 6-minute walk distance improved by a mean of 59% and individually-tailored exercise circuit results improved by a mean of 20%. MRC breathlessness score improved by a mean of 23.5%; quality of life scores improved by a mean of 6%. All patients completed a Satisfaction Questionnaire: 100% felt an improvement in the way their breathing affects their lives; 100% felt the group and social support was paramount; 100% requested that this service become permanent. As a direct result there is now an “open extension” of the maintenance programme, running in parallel and on-site with the main group, self-directed by the patients.
Conclusions: These early results suggest that a locally-based exercise programme, supported by rehabilitation assistants, has the potential to have a major benefit in maintaining the confidence and physical fitness of patients with COPD who have previously experienced a formal pulmonary rehabilitation programme. Additionally, it is an inexpensive intervention, which is having a very positive response from the patient population, which seems to be a key factor in its benefit. Further positive results are expected from ongoing groups.
Asthma: basic mechanisms
BRONCHIAL FIBROBLASTS EXHIBIT A PROINFLAMMATORY RESPONSE TO RHINOVIRUS-16 INFECTION BUT LACK A TYPE I INTERFERON RESPONSE
N. J. Bedke, S. Holgate, D. Davies. University of Southampton, Southampton, UK
Introduction: Rhinoviruses (RV) are a major cause of asthma exacerbations. RV infections usually trigger a proinflammatory response accompanied by an innate immune response mediated by the type I interferons (IFNs) which trigger an antiviral response in infected and neighbouring cells to limit viral replication. We have previously reported deficient IFN-β production in response to RV infection by bronchial epithelial cells from asthmatic donors. In this study, we postulated that a deficient Type I interferon response also affects other airways structural cells in asthma.
Methods: Primary fibroblasts were grown from bronchial biopsies from 10 normal and 10 asthmatic patients, and were infected with RV-16 (moi = 0.01–1), using UV-irradiated (UVi) virus as control. Viral replication, IFN-β and cytokine expression were measured by RT-qPCR and ELISA.
Results: Regardless of patient group, bronchial fibroblasts were highly susceptible to RV-16 infection. IL-8 and IL-6 were rapidly induced with RV16 and UVi-RV-16. IL-8 and IL-6 was expression was partially inhibited by a PI3K inhibitor. In contrast, RANTES expression was only induced in the presence of viral replication but this was not accompanied by significant induction of endogenous IFN-β. Exogenous IFN-β was highly protective against viral replication. Fibroblasts respond to RV16 with a vigorous proinflammatory response, some of which may be independent of viral replication. However, RANTES mRNA expression was more sustained and required active viral replication. The absence of IFN-β production in RV16-fibroblasts may explain their high susceptibility to viral infection.
Conclusions: Our data suggest that in asthma where epithelial shedding occurs, the underlying fibroblasts may be vulnerable to RV infection and permissive for viral replication. This will facilitate the persistence of the infection and augment the proinflammatory response, both of which can contribute to asthma exacerbations. Exogenous IFN-β protects fibroblasts against infection and may be a potential therapeutic approach for virus-induced asthma exacerbations.
ALTERED AIRWAY FIBROBLAST COLLAGEN SYNTHESIS IN SEVERE ASTHMA AND THE INVOLVEMENT OF AKT PHOSPHORYLATION
P. N. Sanders, L. C. Lau, D. Sammut, P. H. Howarth. Southampton University, Southampton, UK
Introduction: Fibroblasts in the asthmatic airways are able to secrete increased levels of extra-cellular matrix (ECM) proteins such as collagen I and III, fibronectin and laminin, and this is accompanied by fibroblast hyperplasia, perpetuating the remodelling process. Bronchoalveolar lavage (BAL) contains factors present in the airway lining fluid secreted, in part, by epithelial cells. Epithelial-mesenchymal interactions are believed to play an important role in normal wound repair as well as the remodelling process in asthma. By challenging fibroblasts grown from bronchial biopsies with BAL, a basic model of the airway can be constructed and used to investigate fibroblast behaviour in asthma.
Methods: Fibroblasts from six healthy, six mild asthmatic and six severe asthmatic patients were grown from biopsies and challenged with BAL from six healthy, six mild asthmatic or six moderate/severe asthmatic volunteers. The [3H]-thymidine incorporation assay and TaqMan real-time PCR were used to assess their mitogenic potential and ability to synthesise collagen III mRNA. The phosphorylation status of a variety of MAPKs within healthy, mild asthmatic and severe asthmatic fibroblasts was determined after challenge with moderate/severe asthmatic BAL using the R&D systems MAPK-phosphorylation kit.
Results: Bronchoalveolar lavage stimulated [3H]-thymidine incorporation in fibroblasts grown from biopsies from healthy and mild asthmatics but not in those from severe asthmatics (p<0.0001), indicative of an altered fibroblast mitogenic potential in severe asthma. BAL from those with moderate/severe asthma, however, induced significantly more collagen III mRNA expression by the fibroblasts cultured from severe asthmatics than in fibroblasts cultured from the airways of either healthy subjects (p<0.05) or mild asthmatics (p<0.005). There was a marked increase in Akt1 and Akt2 phosphorylation in severe fibroblasts compared to mild asthmatic fibroblasts after a 30 min challenge with moderate/severe asthmatic BAL, with no Akt1 or Akt2 phosphorylation seen in healthy fibroblasts.
Conclusion: Fibroblasts from severe asthma thus have an altered phenotype favouring a synthetic rather than proliferative phenotype. Signalling pathways influencing Akt phosphorylation are implicated in this process. These findings have relevance to structural airway changes in asthma and processes underlying disease severity.
SELDI-TOF MASS SPECTOMETRY SCREENING OF SPUTUM SUPERNATANTS IDENTIFIES NOVEL BIOMARKERS DISTINGUISHING EOSINOPHILIC FROM NON-EOSINOPHILIC ASTHMA
I. Pavord1, P. Bradding1, K. Molyneux2, S. Pate2, J. Barratt1. 1University of Leicester; 2John Walls Renal Unit, Leicester, UK
Introduction: Asthma affects 10% of the population and is an important cause of morbidity and mortality at all ages. Current treatments are either ineffective or carry unacceptable side effects for a number of patients. We know that applying a management strategy aimed at suppressing the sputum eosinophil count leads to a marked reduction in severe asthma exacerbations compared to current guidelines advocating symptom-guided treatment. However, analysis of induced sputum for eosinophilia is labour intensive and time consuming, and therefore unlikely to be used widely.
Methods: Surface enhanced laser desorption/ionisation time of flight mass spectrometry (SELDI-TOF MS) enables the analysis of complex biological samples through firstly “on-Chip” retentate chromatography followed by detection of captured proteins and peptides by mass spectrometry. We analysed supernatants from induced sputum samples from 40 well-characterised asthmatics (20 eosinophilic (>3% sputum eosinophilia) and 20 non-eosinophilic (<1.8% sputum eosinophilia)) and healthy controls. All sputum samples were stored at −80°C before analysis and samples were normalised by correcting to a common final total protein concentration.
Results: In a biomarker scouting study we found consistent differences in the proteomic profile of sputum from patients with non-eosinophilic versus eosinophilic asthma. Two ProteinChip chemistries were particularly informative: H50 (reverse phase), and IMAC-Zinc (binds proteins with an affinity for the metal ion zinc, such as certain metalloproteinases). Those biomarkers showing most promise were m/z 13,265; 12,749, 10,875 (H50) and 25,581, 12,961, 3,410 (IMAC-Zn).
Conclusions: Biomarker validation studies are now underway using prospectively collected induced sputum samples from a new cohort of patients to confirm these initial findings. The biomarkers thus far identified all have predicted masses of less than 30 kDa, making it extremely likely that they may also be present in urine. We are also therefore analysing urine in parallel as there is increasing evidence that many systemic diseases are associated with the urinary excretion of disease-specific biomarkers. Urine dipstick testing for biomarkers is likely to be more readily integrated into primary and secondary care than regular assessment of induced sputum.
THE ROLE OF GALECTIN-3 IN ASTHMA
D. Sammut, H. M. Haitchi, L. Lau, S. Wilson, J. Holloway, D. Davies, P. H. Howarth. University of Southampton, Southampton, UK
Background: Galectin-3, a galactose-binding lectin has been implicated in fibrotic processes in a number of organs in humans. In vitro studies have shown that it is secreted from epithelial cells and can activate fibroblasts to increase collagen deposition. Human studies in COPD and interstitial lung disease have revealed higher levels of expression of this protein in biopsies and bronchoalveolar lavage fluid (BALF) respectively of patients with these two lung conditions.
Hypothesis: Galectin-3 expression is upregulated in human asthmatic epithelium. It may have a role in airway remodelling by activation of submucosal fibroblasts to secrete more extracellular matrix proteins.
Methods: BALF, bronchial epithelial brushings and biopsies were obtained from healthy controls and asthmatics via fibreoptic bronchoscopy. ELISA for galectin-3 was performed on the BALF. Bronchial biopsies embedded in GMA were stained for galectin-3 and its expression quantitated. RNA was extracted from bronchial brushings and analysed for galectin-3 expression by RT-PCR.
Results: Thirty biopsy samples (7 healthy controls, 15 mild asthmatics, 8 severe asthmatics) were stained for galectin-3 which was detectable in the bronchial epithelium. Quantification of expression by computer-assisted image analysis showed no difference in expression between the groups. RT-PCR for galectin-3 was performed on epithelial brushing mRNA from 17 subjects (6 healthy controls, 2 mild asthmatics, 9 severe asthmatics). No significant difference in expression levels was detected. Galectin-3 was detected in BALF from both normal and asthmatic subjects (25 healthy controls, 41 mild asthmatics, 22 severe asthmatics) but levels were not significantly different. No correlation was found between immunoreactivity for galectin-3 and biopsy eosinophil counts, neutrophil counts, collagen I staining, collagen III staining or basement membrane thickness.
Conclusion: Despite the evidence from in vitro and animal studies, as well as its role in other lung diseases, we have failed to identify significant differences in the expression of galectin-3 at both RNA and protein level between asthmatic and non-asthmatic subjects.
INTERSTITIAL AIRWAY WALL FIBROSIS IN ASTHMA AND ITS RELATION TO DISEASE SEVERITY
L. Shui, S. Wilson, D. Sammut, H. Rigden. University of Southampton, Southampton, UK
Introduction: Tinctorial staining of endobronchial biopsies identifies a dense band beneath the true basement membrane and this has been referred to as sub-basement membrane thickening. It is a characteristic feature of asthma and is appreciated to relate to enhanced collagen deposition. Changes in collagen deeper within the tissue have not been evaluated. Such structural changes may be more likely to alter airway wall behaviour and relate to disease severity than those evident more superficially.
Methods: To evaluate interstitial airway wall collagen deposition, endobronchial biopsies were obtained at fibre-optic bronchoscopy from healthy controls (n = 10) and those with mild (n = 9) and severe (n = 10) asthma. The biopsies, embedded in glycol methacrylate (GMA), were stained with monoclonal antibodies against collagen I (1:500) and collagen III (1:1500). The extent of interstitial staining was calculated in the lamina propria, using a computer image analysis program, excluding areas of smooth muscle and glands and also excluding the superficial sub-basement area of collagen.
Results: Interstitial collagen was present in all biopsies and there was a progressive increase in interstitial collagen I deposition from that seen in healthy bronchial controls to more severe asthma. The differences were significant: p = 0.027 (healthy bronchial controls vs mild asthma), p<0.0001 (healthy controls vs severe asthma) and p<0.05 (mild asthma vs severe asthma). A similar trend was observed in lower airway collagen III deposition, with the respective p values: 0.004, <0.0001 and 0.05. The extent of collagen I and collagen III in biopsies strongly correlated (p<0.0001). The mean FEV1 % predicted for the groups fell progressively from 104.3 (3.6) in the healthy controls to 93.2 (3.5) in the mild asthmatics down to 70.4 (8.3) in the severe asthmatics.
Conclusions: There is interstitial airway wall fibrosis in asthma. This will alter the airway wall properties and is likely to contribute to the decline in lung function as asthma becomes more severe.
CROSS SECTIONAL RELATION BETWEEN TOTAL IGE LEVELS, CIGARETTE SMOKING AND FEV1 IN AN AGEING POPULATION (THE ELSA COHORT)
S. E. Webster1, N. E. Rice2, D. Melzer2, B. D. Patel1. 1Department of Respiratory Medicine. Royal Devon and Exeter NHS Foundation Trust; 2Epidemiology and Public Health Group, Peninsula Medical School, Exeter, UK
Introduction: IgE levels are elevated in smokers and individuals with asthma. Using data from the English Longitudinal Study of Ageing (ELSA) we assessed to what extent smoking and asthma explain the previously reported inverse association between IgE levels and FEV1.
Methods: Blood IgE levels and measurements of FEV1 were obtained in 2001. Predicted values for FEV1 were calculated using regression coefficients for age and height derived independently from male and female lifelong non-smokers without respiratory disease. Where necessary, appropriate methods were used to normalise variables before inclusion in analyses
Results: Total IgE levels and measurements of FEV1 were available for 2365 individuals (47.7% men), mean age 62.7 (9.6) years, 11.9% of who reported diagnosed asthma. There was an inverse relation between ln IgE and FEV1 % predicted (r = −0.12, p⩽0.0001). Median IgE levels were higher in men (35 kU/l (IQR 82)) than women (22 kU/l (54) p⩽0.0001). In both sexes IgE levels were highest in current smokers and in pooled analysis, adjusted for sex and pack years smoked, IgE levels declined with the period of abstinence towards the level seen in non-smokers (mean adjusted IgE 155.3 kU/l (95% CI 133.5 to 177.2) smokers, 106.8 kU/l (78.1 to 135.4) ex-smokers <12 years abstinence, 88.8 kU/l (71.8 to 105.8) ex-smokers >12 years abstinence and 75.1 kU/l (60.2–89.9) non-smokers (adjusted p for trend ⩽0.001)). Sex-specific quartiles of IgE were used to assess the association with asthma. After adjustment for age, pack years and smoking status, the risk of asthma increased with total IgE (OR 1.61 p<0.05, 2.76 p⩽0.001, 5.08 p⩽0.001 for second, third and top quartile relative to bottom). There was a significant inverse association between FEV1 and sex specific quartile of IgE (p⩽0.001 for trend). However, after adjustment for current smoking status and diagnosed asthma, there was no association between total IgE and FEV1 % predicted.
Conclusions: In this population the association between total IgE level and FEV1 is explained by confounding by smoking and diagnosed asthma. The mechanism for elevated IgE levels in smokers is not understood, but the gradual temporal decline with abstinence suggests a direct effect of cigarette smoke on total IgE levels.
Acute lung injury: pathophysiology
CYCLO-OXYGENASE-2 INDUCTION BY CYCLIC MECHANICAL STRAIN IN HUMAN PRIMARY ALVEOLAR TYPE 2 CELLS AND IN MURINE WHOLE LUNG IS DEPENDENT ON ACTIVATION OF ERK1/2
L. Pinhu, M. Wilson, M. Takata, M. Griffiths. Imperial College, London, UK
Background: Mechanical stimulation of the gas exchange surface of the lung is an inevitable consequence of mammalian anatomy. Mechanical forces affect the phenotype and function of cells and tissues, and over-distension of the mechanically ventilated lung contributes to the mortality of patients with acute lung injury. Mechanical forces enhance the release of mediators that exacerbate lung damage, and contribute to systemic inflammation and death—the syndrome of ventilator-associated lung injury (VALI). Cyclic mechanical strain (CMS) increases prostanoid production from several cell types but the reported mechanism has varied between studies. For example, CMS induced cyclo-oxygenase-2 (COX-2) and the availability of arachidonic acid substrate for prostanoid production by increasing the activity of cytosolic phospholipase A2 in fetal lung epithelial cells. Prostanoids affect multiple processes that are relevant to lung injury and repair including: inflammation, wound healing, fibrosis, host defence and control of vascular tone.
Methods and Results: We applied CMS (Flexercell FX2000 apparatus: 0, 30% stretch for 2 h at 20/min) to human primary alveolar type 2 cell (hAT2) monolayers in vitro as a model of lung over-distension in the presence or absence of inhibitors of the NFκB pathway (AS602868: 3 μM), ERK1/2 pathway (U0126 or its inactive counterpart U0124: 10 μM) and JNK (SP600125: 10 μM). COX-2 mRNA (real-time PCR: fig A) and PGE2 (ELISA: fig B) in supernatants collected after 4 and 24 h were increased by CMS. Both effects were attenuated by inhibitors of the NFκB and ERK1/2 pathways, suggesting that CMS-induced COX-2 transcription was dependent on these pathways and contributed to increased PGE2 release. In separate experiments, we have confirmed by western blotting using specific antibodies against phosphorylated intermediates that the ERK1/2 and NFκB (p65) pathways were activated by CMS (30% stretch for 10 min at 20/min). Finally, in an acute murine ventilator-induced lung injury model, injurious mechanical ventilation increased COX-2 mRNA in whole lung and PGE2 in lavage fluid after one hour, but this effect was prevented by pre-treatment with U0126 (30 mg/kg i.p.).
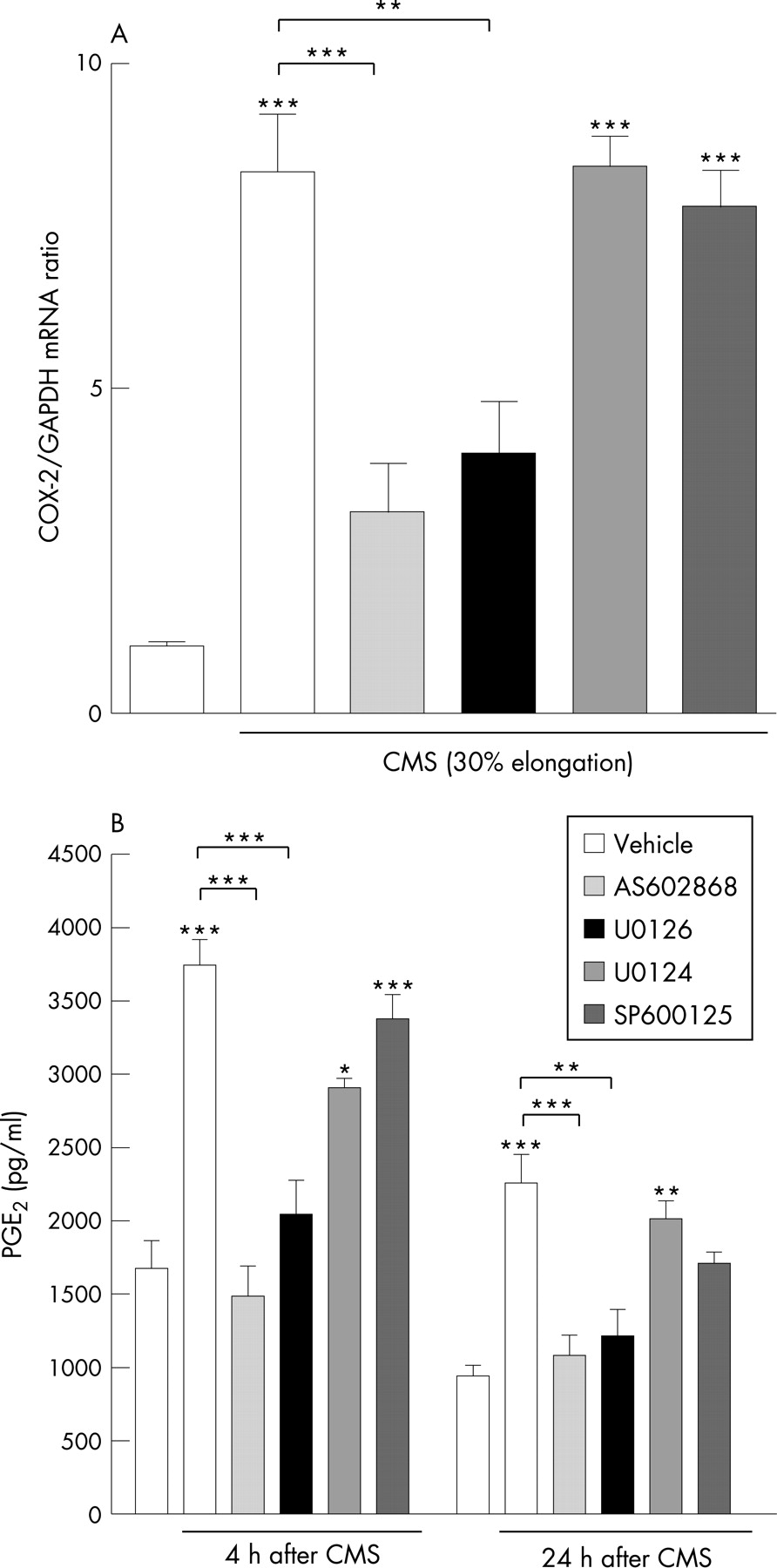
Conclusions: COX-2 induction by mechanical forces in hAT2 cells depended on the activation of ERK1/2 and NFκB signalling pathways, but not on JNK. In the absence of data describing the functional effects of inhibiting COX-2 activity, the significance of these findings in the context of acute lung injury and VALI is uncertain.
Acknowledgement: This work was funded in part by the British Lung Foundation.
MARGINATED MONOCYTES EXACERBATE PULMONARY OEDEMA IN A MURINE MODEL OF VENTILATOR-INDUCED LUNG INJURY
M. R. Wilson, K. P. O'Dea, D. Zhang, A. Dorr, M. Takata. Imperial College,London, UK
Background: High stretch/high tidal volume (VT) mechanical ventilation induces pulmonary oedema and inflammation, characterised by production of soluble mediators and lung leukocyte recruitment. Historically, analysis of leukocyte involvement in ventilator-induced lung injury (VILI) has focused on neutrophils, largely ignoring other leukocytes such as monocytes. Monocytes are cells of the mononuclear phagocytic system, and can be phenotypically divided into resident (Gr-1low) and inflammatory (Gr-1high) classes. Gr-1high monocytes migrate to sites of acute inflammation, and we have previously demonstrated recruitment to pulmonary microcirculation following either systemic endotoxin or high stretch ventilation. It is however unknown whether such ”lung-marginated” monocytes play any role in the development of VILI.
Methods: Anaesthetised male C57BL6 mice were ventilated with high VT (25–30 ml/kg) for 2 h. In some animals, monocytes and neutrophils were pre-marginated to the lungs by a subclinical dose of lipopolysaccharide (LPS; 20 ng, intraperitoneal) before starting ventilation. In order to differentiate the effects of pre-marginated monocytes from neutrophils, monocytes were depleted using intravenous clodronate liposomes in a subgroup of LPS-treated animals. Lung-marginated neutrophils and Gr-1high monocytes were quantified in lung cell suspensions using flow cytometry. Pulmonary oedema formation was assessed by increased peak inspiratory pressure (PIP) and changes in respiratory system mechanics.
Results: LPS pre-treatment enhanced lung margination of Gr-1high monocytes and neutrophils prior to ventilation (p<0.05). LPS pre-treatment also exacerbated stretch-induced pulmonary oedema, shown by increased PIP (fig A) and decreased respiratory system compliance (fig B). Clodronate (clod) pre-treatment depleted lung-marginated Gr-1high monocytes (0.3 (0.2)×105 vs 2.4 (1.4)×105 cells/lungs; p<0.001; mean (SD)) but not neutrophils, and significantly attenuated stretch-induced oedema formation (fig A, B).
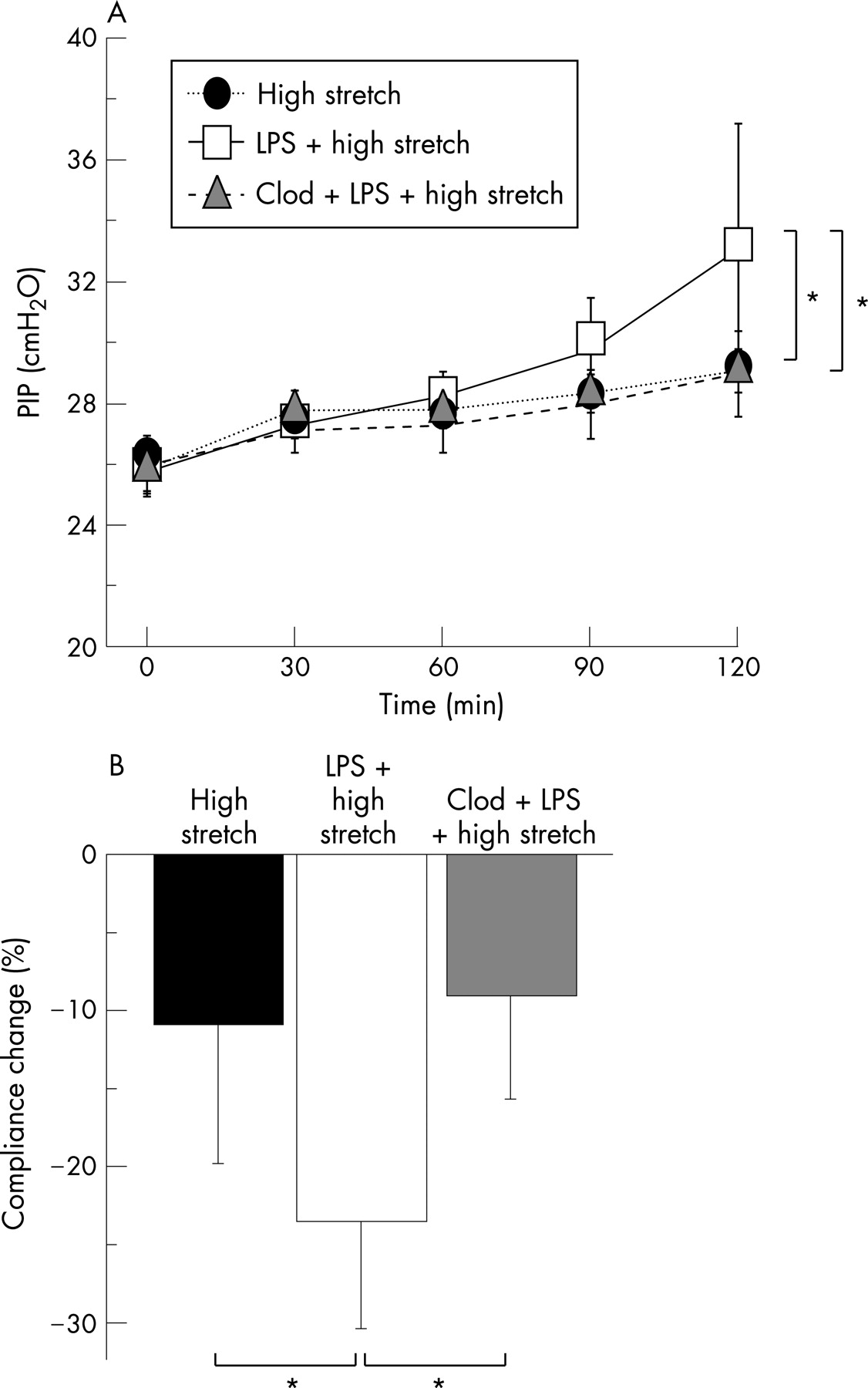
Conclusions: In this clinically-relevant “two-hit” model of VILI, subclinical systemic endotoxaemia sensitised the lungs to the effects of mechanical ventilation, exacerbating pulmonary oedema formation. This was attenuated by clodronate pre-treatment, which depleted lung-marginated Gr-1high “inflammatory” monocytes without affecting neutrophils. These data indicate a previously unexplored role for marginated monocytes in the pathophysiology of VILI.
Acknowledgement: This work was funded in part by the Westminster Medical School Research Trust.
PAR1 SIGNALLING IN LIPOPOLYSACCHARIDE-INDUCED ACUTE LUNG INJURY
P. F. Mercer1, J. D. Moffatt1, C. J. Scotton1, C. K. Derian2, R. C. Chambers1. 1University College London, London, UK; 2Johnson and Johnson, Pennsylvania, USA
Acute lung injury (ALI) is characterised by neutrophilic inflammation of the air spaces, alveolar epithelial damage and severe oedema, caused by increased vascular permeability. This condition is also associated with increased procoagulant activity, characterised by alveolar fibrin deposition and decreased fibrinolysis. Activated coagulation proteinases exert proinflammatory effects via activation of their cellular receptors, the proteinase activated receptors (PARs). Activation of PAR1 has been shown to induce proinflammatory effects including cytokine release, adhesion molecule expression, endothelial barrier dysfunction and vascular permeability in certain disease settings, however the role of PAR1 in ALI remains unknown. The aim of this study was to determine the role of PAR1 in neutrophil recruitment and lung oedema following intranasal challenge with lipopolysaccharide (LPS) using a selective PAR1 antagonist (RWJ58259).
Female BALB/c mice (n = 5/group) were anaesthetised and challenged with LPS (0.1 mg/kg) or saline (50 μl/mouse, i.n.), followed by i.p. administration of RWJ58259 (5 mg/kg) or saline 30 min later. Three hours after LPS challenge, bronchoalveolar lavage (BAL) was performed and BAL leukocytes counted, cytokine levels measured by ELISA and total BAL protein determined. BAL neutrophils were significantly elevated 3 h following LPS challenge (saline: 1.90 (0.55) (SEM); LPS: 179.97 (37.84) × 1000 cells/ml, p<0.001) as were TNFα (saline: 0.35 (0.19); LPS: 8.08 (0.68) ng/ml, p<0.001) and protein levels (saline: 196.41 (11.39); LPS, 236.47 (15.47) μg/ml, p<0.05). RWJ58259 treatment significantly attenuated LPS-induced neutrophil influx (73.63 (21.61) × 1000 cells/ml, p<0.05), BAL protein (189 (13) μg/ml, p<0.05) and TNFα levels (4.87 (0.71) ng/ml, p<0.05). LPS challenge increased lung chemokine levels, including MIP-2 (saline: 0.43 (0.11); LPS: 5.76 (0.8) ng/ml, p<0.001) and MCP-1/JE (saline: not detectable (ND); LPS: 0.089 (0.039) ng/ml, p<0.01). Interestingly, only levels of MCP-1/JE were attenuated by RWJ58259 (ND post RWJ58259). These data demonstrate that PAR1 antagonism in vivo significantly reduces both neutrophilia and microvascular leak in this model of ALI. We propose that therapies aimed at specifically inhibiting coagulation proteinase signalling may prove useful in the treatment of ALI.
THE ROLE OF TNF-RELATED APOPTOSIS INDUCING LIGAND IN ACUTE LUNG INJURY
E. E. Mcgrath, H. M. Marriott, P. G. Hellewell, D. H. Dockrell, M. K. Whyte. University of Sheffield, Sheffield, UK
Rationale: Neutrophils play a central role in a number of inflammatory lung diseases. Since neutrophil apoptosis is essential to the resolution of inflammation, understanding the mechanisms regulating this process in vivo are important, as is the potential to drive apoptosis using appropriate pro-apoptotic stimuli. We showed that a death receptor ligand, TNF-related apoptosis inducing ligand (TRAIL), accelerates neutrophil apoptosis in vitro without associated cell activation (J Immunol 2003;170:1027–33). The aim of this project was to study the role of TRAIL in the regulation of neutrophil apoptosis during pulmonary inflammation in vivo in TRAIL deficient compared with wild-type mice.
Methods: The response of wild-type and TRAIL-deficient mice to lipopolysaccharide (LPS) induced acute lung injury was compared in a total of 106 mice. Mice received intratracheal LPS (0.3 μg) or saline control. Bronchoalveolar lavage (BAL) at 24, 48, 72, 96, 120 and 144 h was analysed for neutrophil numbers and apoptosis on morphology and flow cytometry (Annexin V/ToPro-3).
Results: TRAIL-deficient mice had increased neutrophil numbers and reduced neutrophil apoptosis as absolute count or as % total cell count. At 48 h total neutrophils were 2.6 (0.2)×106 in TRAIL-deficient mice versus 1.1 (0.1)×106 in wild-type mice, n = 10, p<0.05 and at 72 h % apoptotic neutrophil was 2.4 (0.4)% in TRAIL-deficient mice versus 5.2 (0.5)% in wild-type mice, n = 10, p<0.05 and total apoptotic cells were 1.85 (0.5)×104 in TRAIL-deficient mice versus 4.8 (1.1)×104 in wild-type mice, n = 10, p<0.05. Flow cytometry also revealed less Annexin-V/ToPro-3 positive cells in TRAIL-deficient mice compared to wild-type controls. At 96 h % Annexin-V/ToPro-3 positive cells was 14.5 (1.2)% in TRAIL-deficient mice versus 35.2 (6.2)% in wild-type mice, n = 10, p<0.05. Overall, the inflammatory response to LPS was significantly prolonged in TRAIL deficient compared to wild-type mice.
Conclusions: Neutrophil apoptosis and clearance is delayed in TRAIL-deficient mice in this model of resolving inflammation. These results suggest TRAIL may have a role in induction of neutrophil apoptosis in the inflamed airway.

PLATELETS ARE SEQUESTERED IN THE LUNGS OF EXPERIMENTAL TRANSFUSION-RELATED ACUTE LUNG INJURY (TRALI) AND PLATELET DEPLETION PROTECTS MICE FROM TRALI
M. R. L. Looney, C. A. L. Lowell, M. A. M. Matthay. University of California, San Francisco, CA, USA
Introduction: Transfusion-related acute lung injury (TRALI) is the number one cause of transfusion mortality in the USA. We have previously described a mouse model of TRALI based on MHC I antibody challenge that produces severe acute lung injury at two hours and is critically neutrophil dependent. We now report a two-hit model of TRALI focusing on the role of platelets and neutrophil-platelet interactions.
Methods: BALB/c mice (H-2Kd) were primed with intratracheal LPS (0.1 mg/kg) 24 h prior to i.v. challenge with MHC I antibody (H-2Kd mAb, 4.5 mg/kg). Lung injury was measured using the gravimetric method (excess lung water, ELW) and lung vascular permeability to 125I-labelled albumin (extravascular plasma equivalents, EVPE). Neutrophils were depleted with Gr-1 mAb (250 μg i.p.) and platelets were depleted using a rabbit, anti-mouse platelet serum (50 μl i.p.) Corresponding control antibodies were used in all experiments. Platelet sequestration was determined by measuring the radioactivity of 51Cr-labelled platelets and expressed as whole lung/blood (100 μl) counts.

Results: There is a significant increase in platelet sequestration in the lungs of mice challenged with MHC I mAb compared with isotype control mAb (fig 1). There was no difference in the measured blood volume (Qb) in the lungs of the two groups. Neutrophil depletion with Gr-1 mAb decreased platelet sequestration after MHC I mAb-challenge (fig 1). Platelets were 90% depleted with the rabbit, anti-mouse platelet serum leading to significant protection from TRALI (fig 2).
Conclusions: Experimental TRALI is characterised by lung neutrophil and platelet sequestration and neutrophils appear to be critical to the sequestration of platelets. Platelet depletion leads to significant lung protection and is an attractive, potential therapeutic target in TRALI.

SALBUTAMOL DRIVES UPREGULATED MMP-9 ACTIVITY IN THE ALVEOLAR SPACE IN ACUTE RESPIRATORY DISTRESS SYNDROME
S. T. Mckeown1, C. M. O'Kane1, G. D. Perkins2, K. Pettigrew3, F. Gao2, D. R. Thickett3, D. F. Mcauley1. 1Queen's University, Belfast; 2University of Warwick; 3Birmingham University, UK
Background: Acute respiratory distress syndrome (ARDS) is characterised by damage to the alveolar-capillary barrier with leak of protein-rich fluid into the alveolar space. Matrix metalloproteinases (MMPs) are enzymes that degrade extracellular matrix including basement membrane and tight junction proteins. MMPs are inhibited in vivo by the tissue inhibitors of metalloproteinases (TIMPs). Several studies have implicated increased MMP-2/-9 in pathogenesis of ARDS. In the BALTI trial 40 patients with ARDS were randomised to placebo or intravenous salbutamol. Salbutamol reduced extravascular lung water but not inflammatory cytokines or neutrophil recruitment. We hypothesised that salbutamol downregulates MMP activity in the alveolar space in ARDS.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
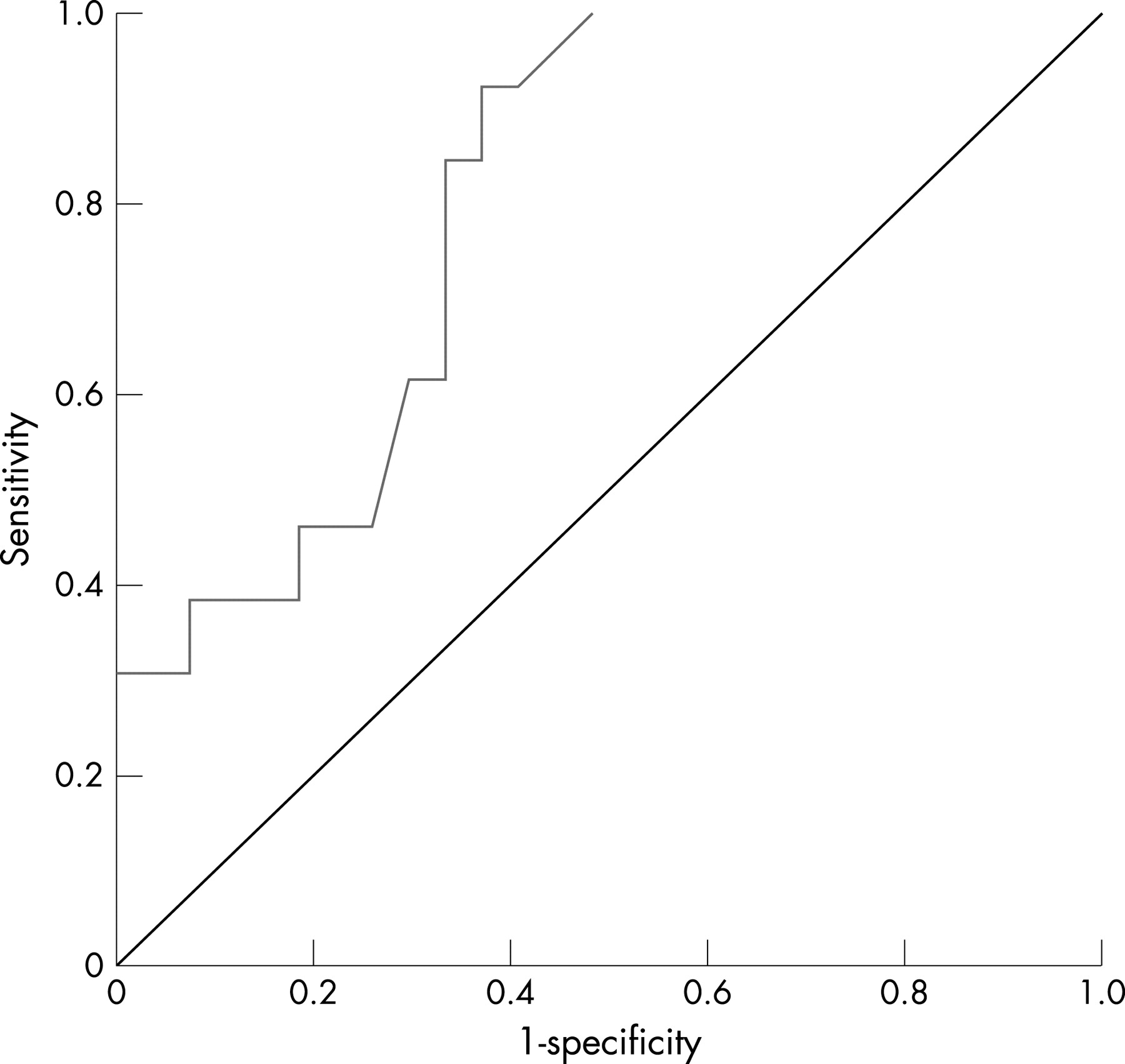{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
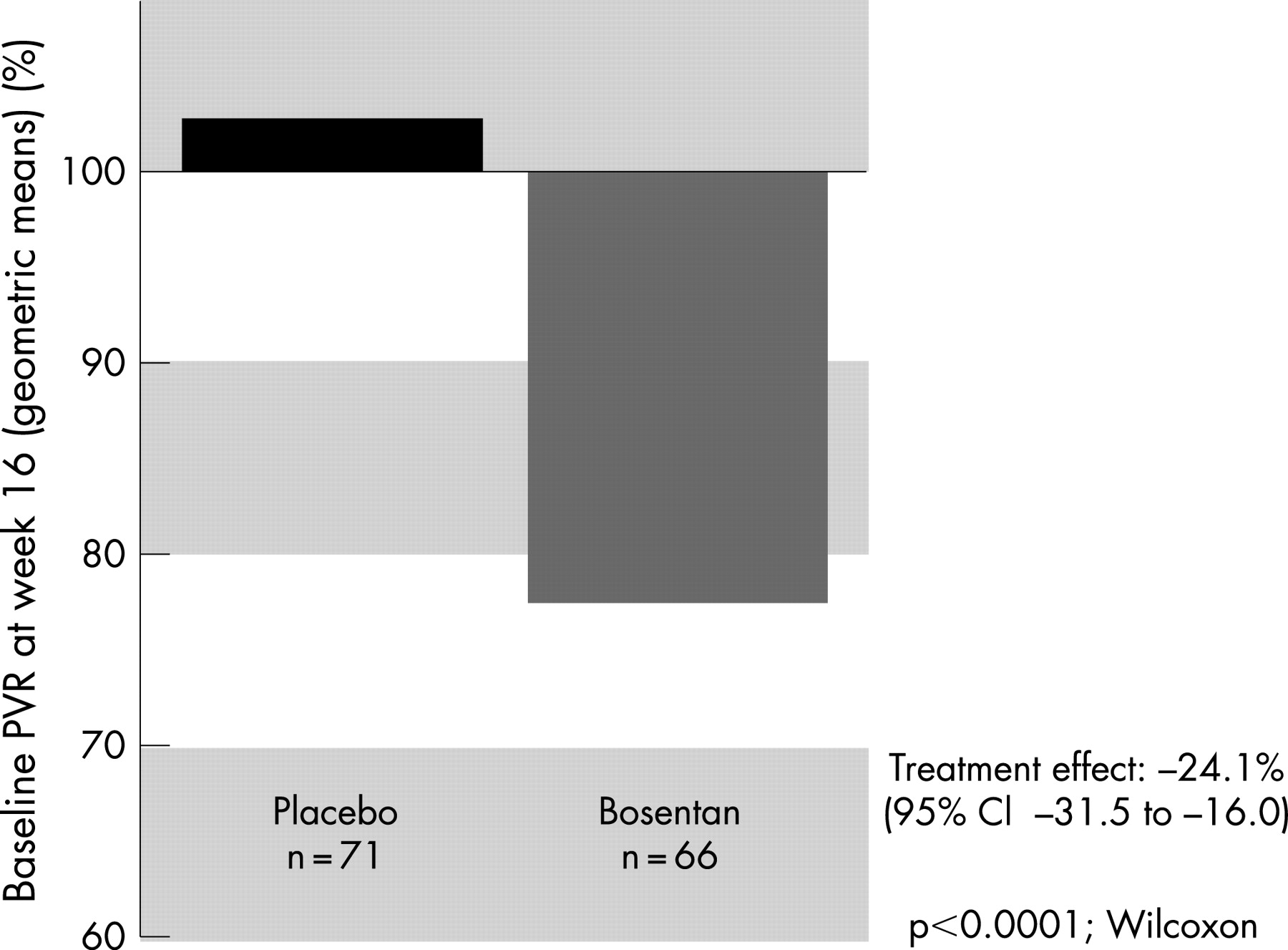{kind=link}
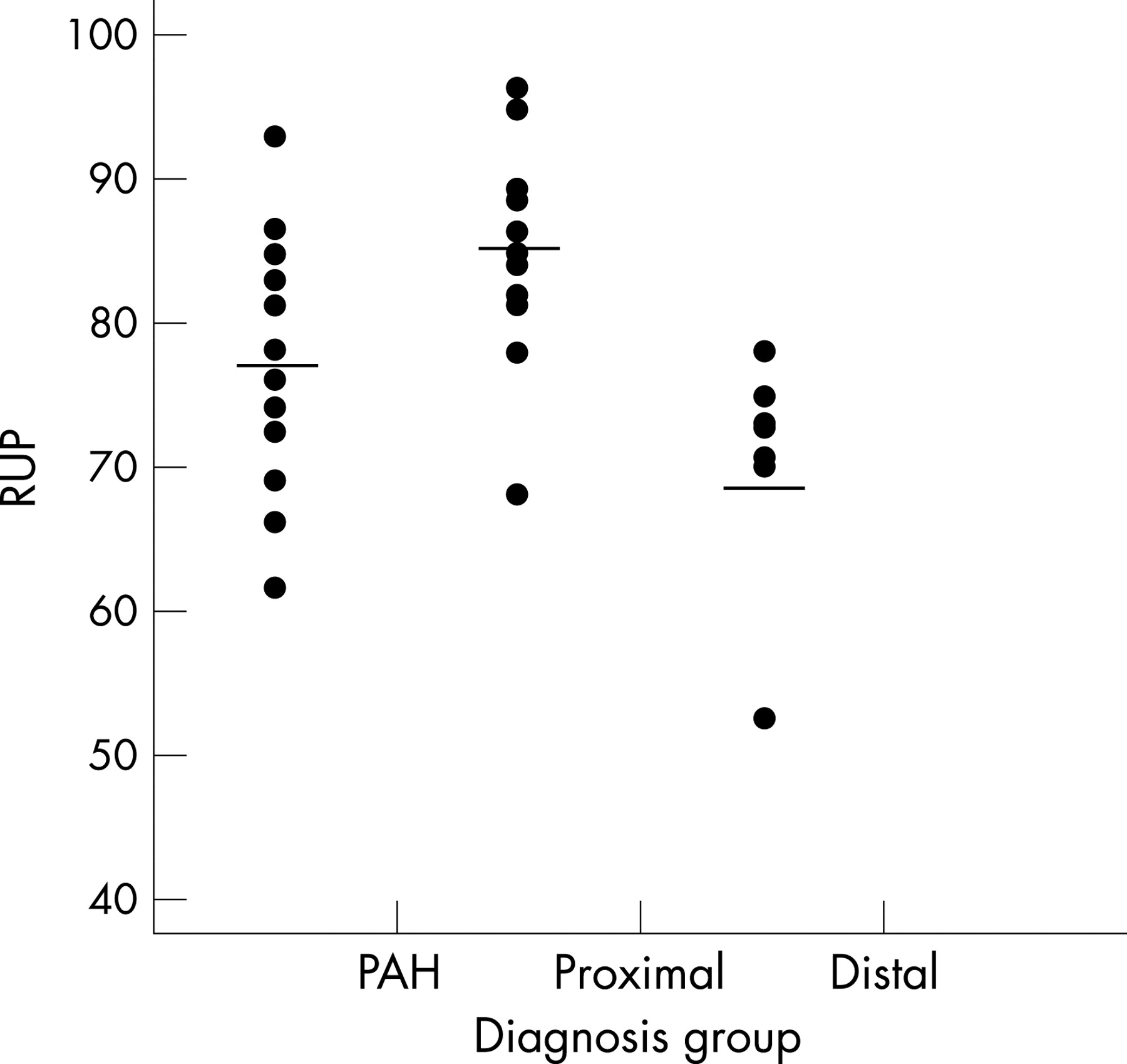{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
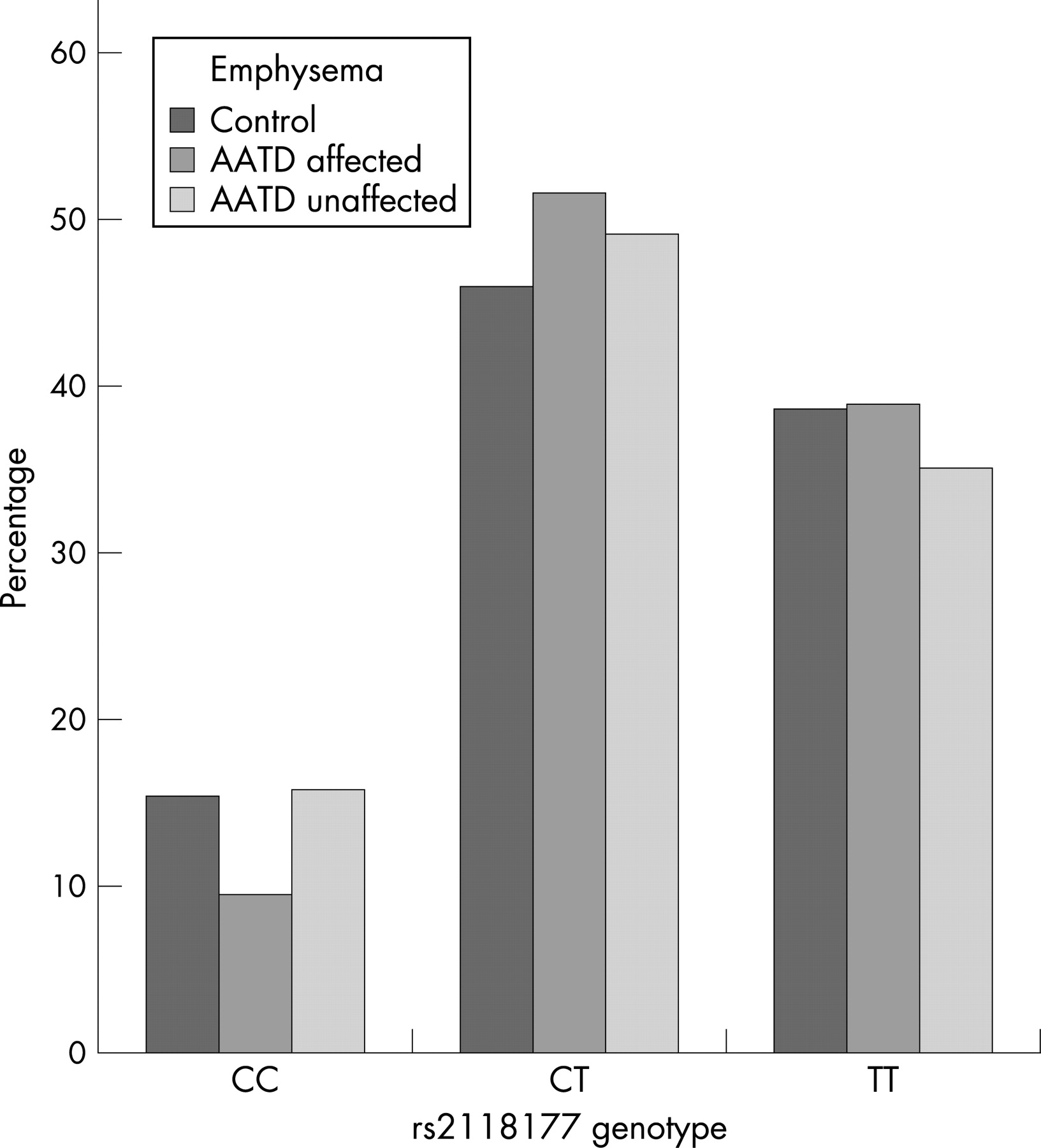{kind=link}
{kind=link}
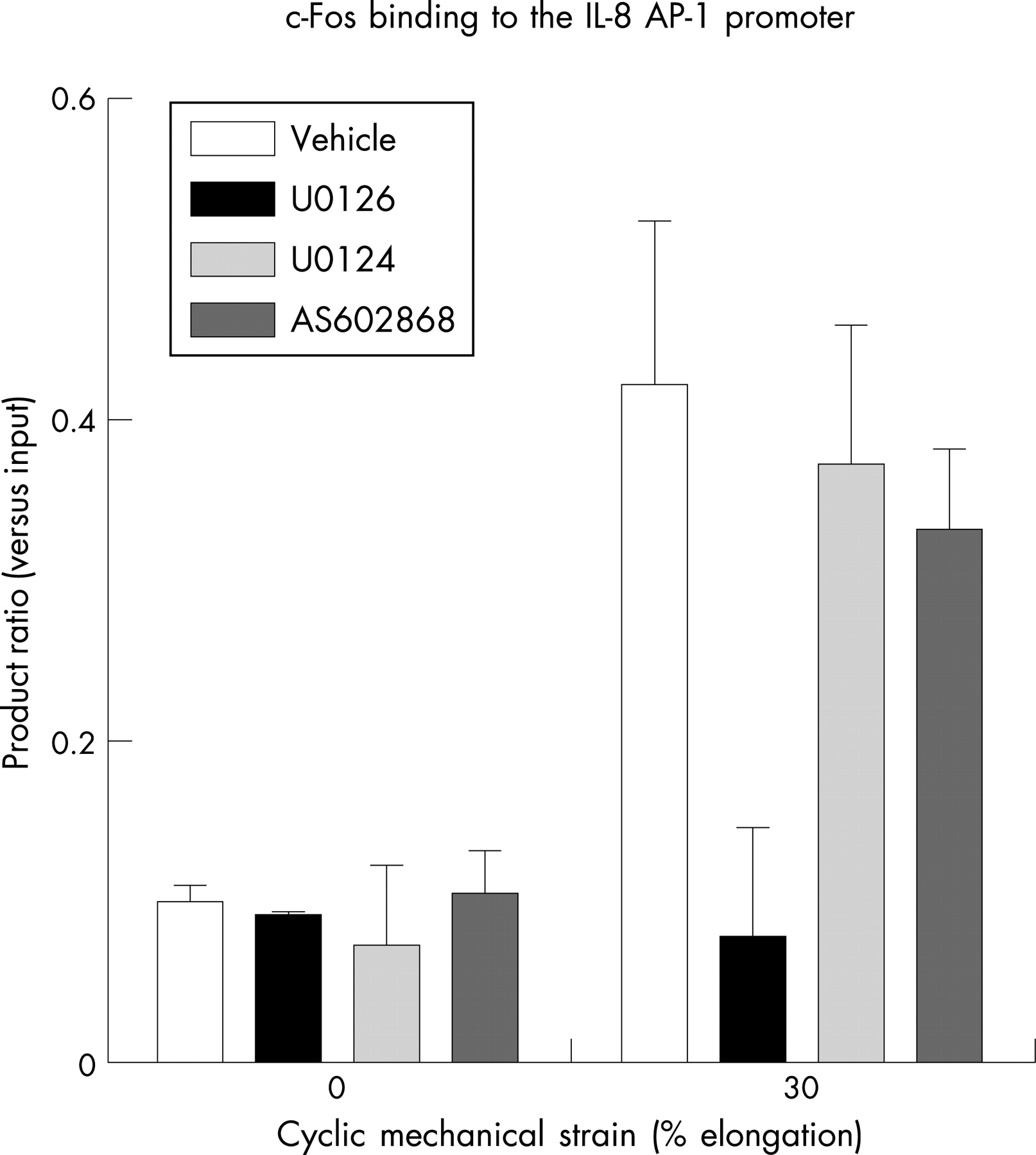{kind=link}
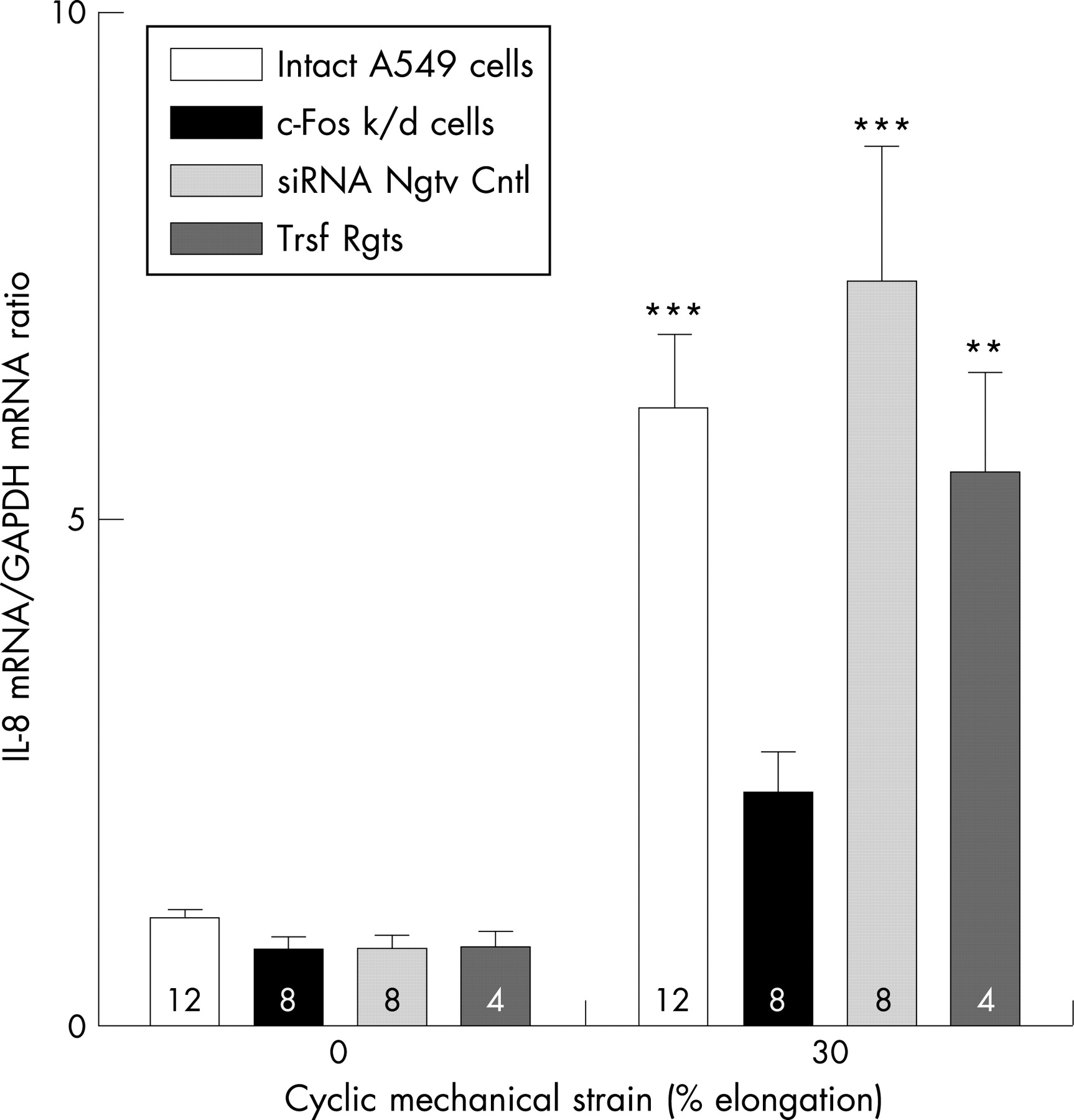{kind=link}
{kind=link}
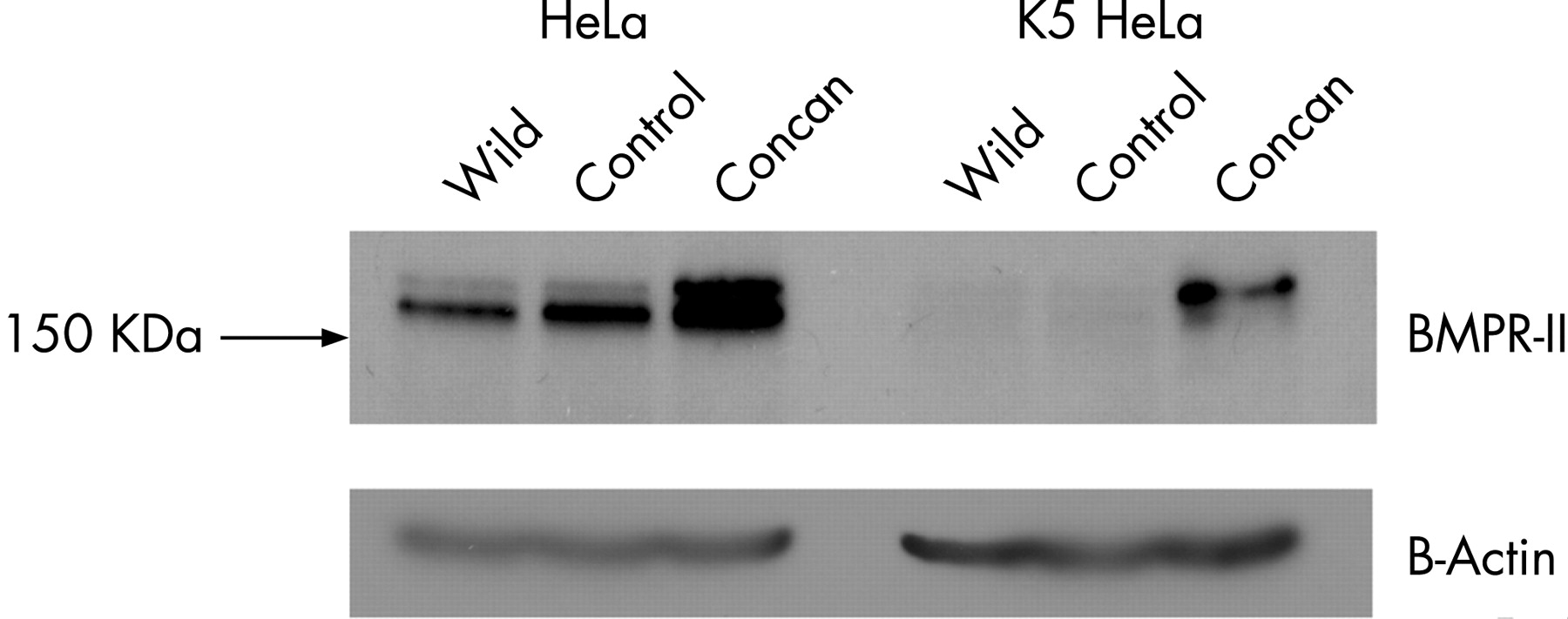{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
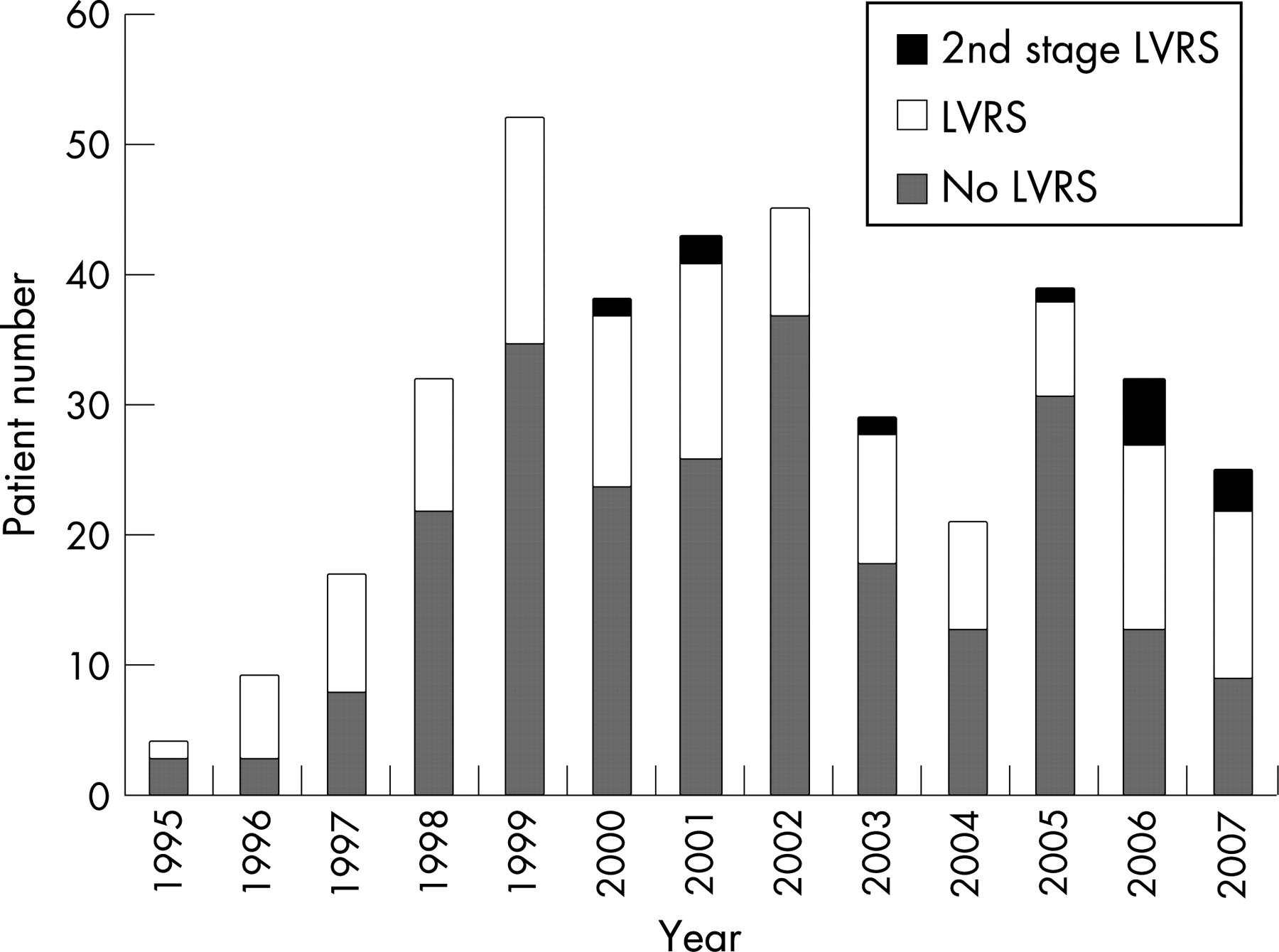{kind=link}
{kind=link}
{kind=link}
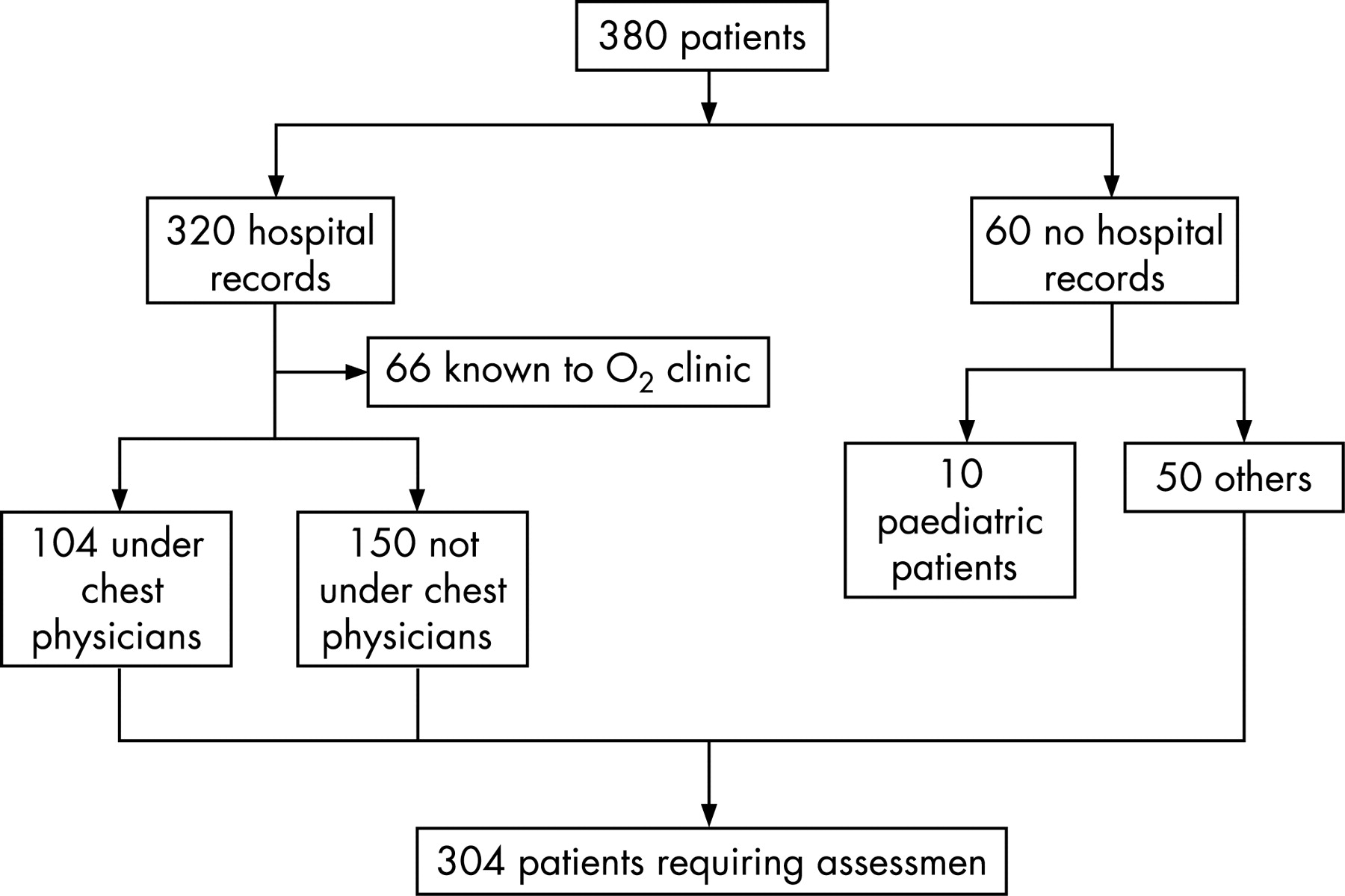{kind=link}
{kind=link}
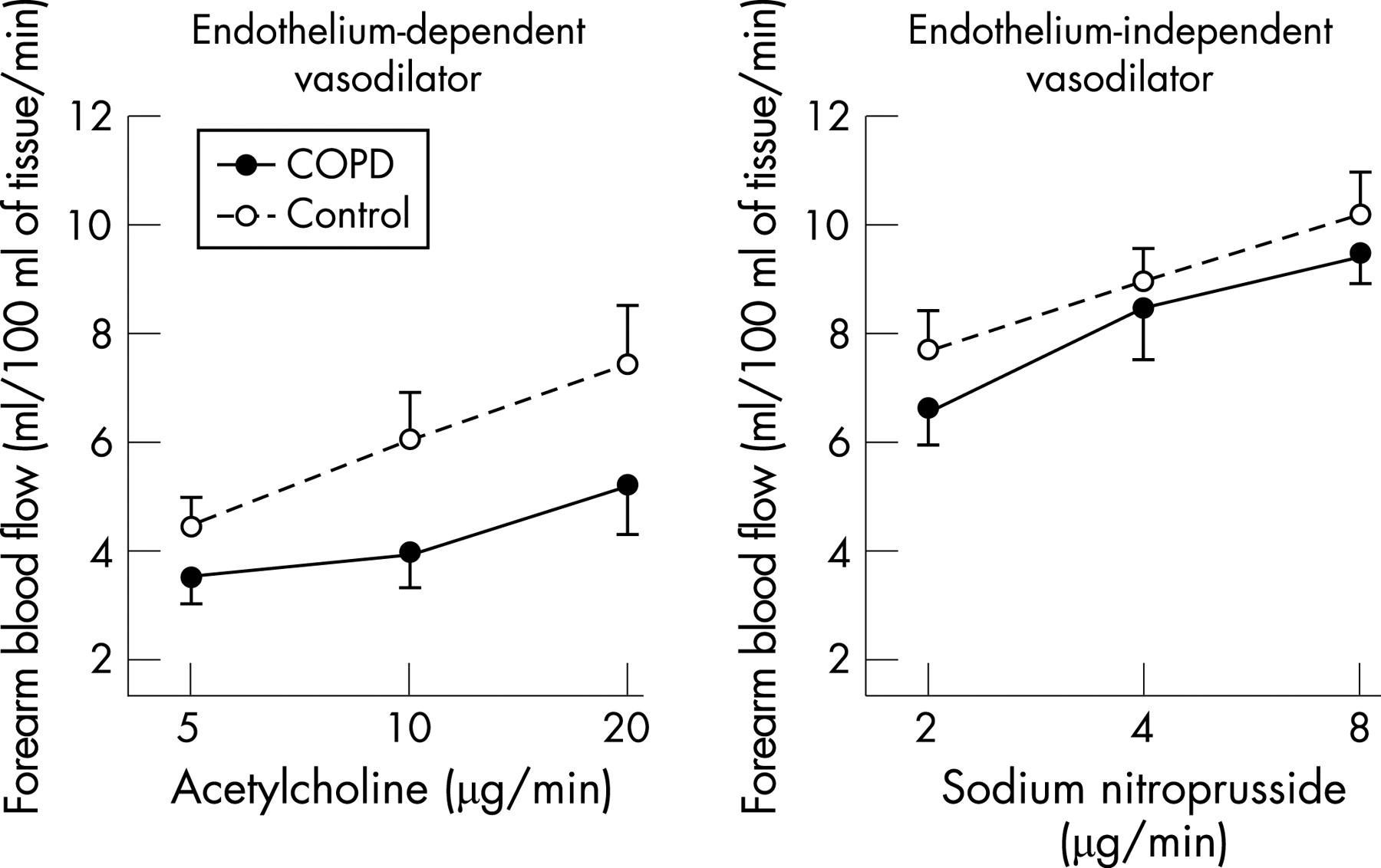{kind=link}
{kind=link}
{kind=link}
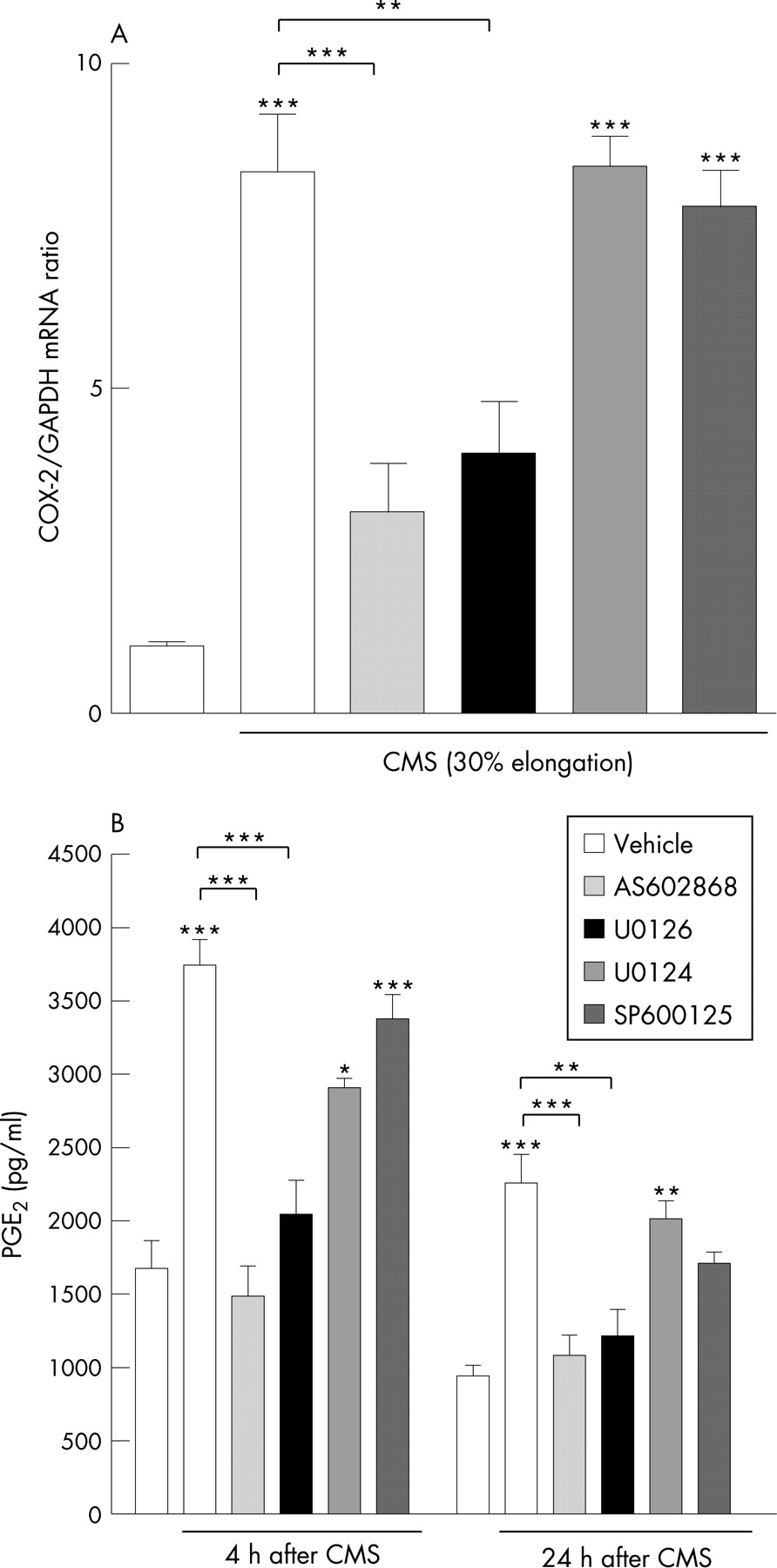{kind=link}
{kind=link}
{kind=link}
{kind=link}
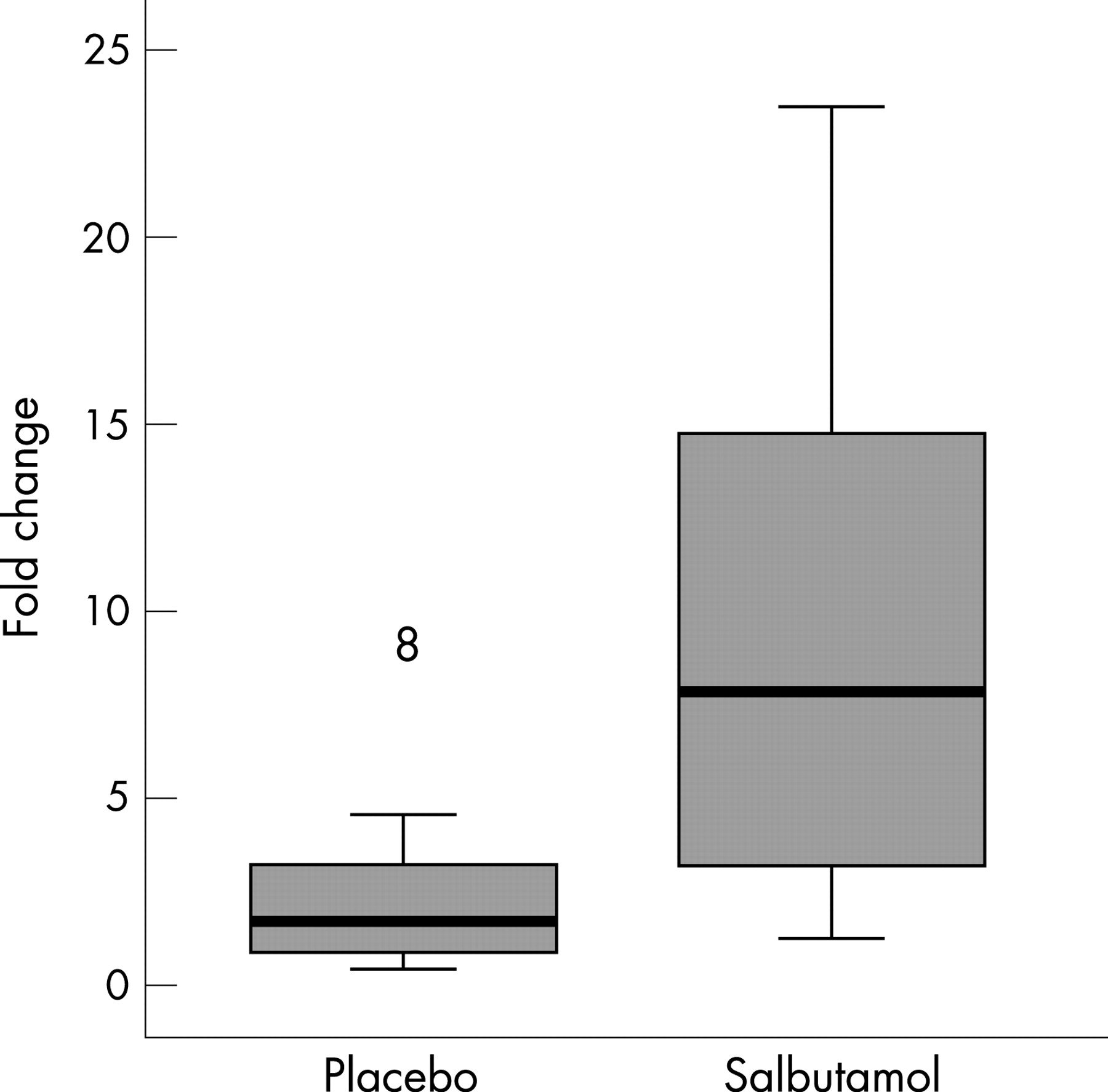{kind=link}
{kind=link}
Methods: MMP-1/-2/-3/-7/-8/-9/-12/-13 were measured in supernatants of distal lung epithelial cells (DLECs) or BAL fluid of patients from the BALTI study by multiplex bead array, TIMPs-1/-2 by ELISA, and lipocalin-associated, and pro-/active forms of MMP-9 were measured by gelatin zymography. Net MMP-9 activity was measured using MMP-9 fluorokine assay (R&D).
Results: BAL fluid from patients with ARDS in the BALTI study showed a non-significant reduction in MMP-1/-2/-3 and a trend to increased MMP-8/-12/-13 by day 4. MMP-9 was significantly upregulated by day 4 compared with baseline, and the upregulation was unexpectedly augmented by salbutamol (fig 1). Salbutamol had no effect on any of the other MMPs studied. Salbutamol induced a 13.2-fold (IQ range 3.9–35.7) upregulation in BAL fluid lipocalin-associated (neutrophil-derived) MMP-9 at day 4 from baseline, compared with 1.3 (0.9–2.7)-fold increase from baseline in placebo group, p = 0.01. Salbutamol dose-dependently induced MMP-9 secretion by DLECs (fig 2). Salbutamol did not affect BAL fluid TIMP-1/-2. Net MMP-9 activity (accounting for the effect of TIMPs/other inhibitors in BAL fluid) was 2.1 (1.5–8.8)-fold upregulated by day 4 from baseline in the salbutamol group but unchanged in the placebo group (1.0-fold; IQ range 0.9–1.1).
Conclusion: Salbutamol appears to specifically upregulate MMP-9 activity both in vitro and in vivo in patients with ARDS. Since salbutamol reduced extravascular lung water in the BALTI patients, these data suggest that MMP-9 may play a previously unrecognised role in alveolar epithelial repair in ARDS.