Article Text

Abstract
Background: Cigarette smoke is a major source of free radicals and oxidative stress. With a significant proportion of women still smoking during pregnancy, this common and avoidable exposure has the potential to influence infant oxidative status, which is implicated in the increased propensity for airway inflammation and asthma. The aim of this study was to examine the effects of maternal smoking on markers of infant oxidative stress.
Methods: The level of oxidative stress (using urinary F2-isoprostanes as a marker of lipid peroxidation) was compared in infants of smokers (n = 33) and non-smokers (n = 54) at 3 months of age. These groups were balanced for maternal atopy and socioeconomic status. Infant urinary cotinine levels were also measured as an indicator of early postnatal cigarette smoke exposure.
Results: Maternal smoking was associated with significantly higher infant cotinine levels, despite the fact that most smoking mothers (83.8%) claimed not to smoke near their baby. Maternal smoking was associated with significantly higher markers of oxidative stress (F2-isoprostane) at 3 months of age. There was also a positive correlation between urinary F2-isoprostanes and infant urinary cotinine levels.
Conclusions: Although this study does not separate the prenatal and postnatal effects of smoking, these findings indicate that environmental tobacco smoke in the early postnatal period adversely affects pro-oxidative/antioxidative status within weeks of life in very early infancy.
Statistics from Altmetric.com
Oxidative status is a complex balance between oxidative burden and antioxidant capacity. Local tissue stress from adverse oxidative balance is a central issue in asthma and allergic disease, not only as a consequence of chronic inflammation in established disease but also as a potential factor in primary development of disease. This latter notion arises from an emerging hypothesis that environmental changes have led to adverse changes in oxidative balance, thereby increasing the propensity for allergy and other immune diseases.1 This hypothesis has been supported by epidemiological studies linking lower dietary antioxidant intakes or serum levels with a higher prevalence of asthma or allergic disease.2–6 It is equally possible that parallel increases in the environmental oxidative burden from oxidising pollutants (including cigarette smoking) could be contributing to the increased risk of allergic disease in early life.
An adverse oxidative balance occurs when oxidative stress (inflammation) occurs in excess of the total antioxidative capacity, as is commonly seen in chronic inflammatory states such as asthma. In this situation, increased levels of reactive oxygen species produced in the airways are reflected by increases in markers of oxidative stress in the airspaces, sputum, breath, lungs and blood.7 Reactive oxygen species may promote inflammation directly or via the formation of lipid peroxidation products (acrolein, 4-hydroxy-2-nonenal and F2-isoprostanes) which activate stress kinases (JNK, MAPK, p38, phosphoinositide 3 (PI-3)-kinase/PI-3K-activated serine-threonine kinase Akt) and reduction-oxidation (“redox”) sensitive transcription factors such as nuclear factor-κB and activator protein-1.7 Oxidative stress and pro-inflammatory mediators can also alter nuclear histone acetylation/deacetylation, allowing transcription factor binding and enhanced pro-inflammatory gene expression in lung cells.7
Exposure to tobacco constituents during pregnancy and early postnatal life is perhaps the most ubiquitous avoidable noxious environmental exposure. A large body of literature links both prenatal maternal smoking and environmental tobacco smoke exposure in early childhood to decreased lung growth8,9,10 and increased rates of respiratory tract infections,11 otitis media12–14 and childhood asthma.15 Cigarette smoke is a major source of free radicals and oxidative stress. To our knowledge, this is the first study to examine the effects of maternal smoking on urinary F2-isoprostanes as a measure of oxidative stress in very young infants.
METHODS
Study population
This is a postnatal follow-up study of an existing pregnancy cohort (n = 122) recruited to examine the effects of maternal smoking in pregnancy on fetal immune development. In this study, 87 women (33 smokers and 54 non-smokers) consented to attend a 3 month follow-up visit to assess the effects of postnatal exposure on infant oxidative stress. The original population was recruited from both hospital antenatal clinics and obstetricians’ rooms (including St John of God Hospital, King Edward Memorial Hospital and Osborne Park Hospital, Perth). All infants were born at term after otherwise uncomplicated pregnancies. Maternal allergic status was assessed by skin prick tests to common allergens (house dust mite, grasses, moulds, cat, dog, feather and cockroach). The resulting groups were balanced for maternal atopic status and socioeconomic status (as defined by educational level) (table 1).
Characteristics (exposures) at 3 months of age of infants of mothers who did and did not smoke in pregnancy
Data and sample collection
Mothers attended the research clinic with their infants at 3 months of age. Interview questionnaires were used to collect data on smoking and other environmental exposures including infant feeding practices, general health, older siblings and household pets. Infection data were collected prospectively (diary cards) and based on both physician-diagnosed disease and parental recording of symptoms (on diary cards). Children were recorded as having “upper respiratory infections” if they had infections that were limited to coryzal symptoms in the absence of significant chest symptoms. Spot urine samples were collected at 3 months of age via non-invasive paediatric urine bags and frozen immediately at −80°C until analysis of F2-isoprostanes and cotinine was conducted.
Assessment of environmental tobacco smoke exposure
Maternal reporting
Maternal reporting of smoking behaviour was determined by interview questionnaire. Questionnaires were used to categorise women (as determined by pack-years) as either smokers or non-smokers. Pack-years represent the mean number of packs smoked per day multiplied by the number of years of cigarette use. Assessment of maternal-reported passive smoking was determined by interview questionnaire also. Mothers were asked if they were regularly exposed to environmental tobacco smoke, the level of exposure (nil, light or moderate), where and by whom (partner or other), and whether they smoked in close proximity (in the same room) to their infant. Information on smoking behaviour of partners or other household members was also collected.
Cotinine measurements
Exposure to environmental tobacco smoke was also assessed independently using urinary cotinine as an objective measure. Briefly, a total of 2.0 ml infant urine (standard or test sample) and 40 μl internal standard (2-phenylimidazole, 25 μg/ml) were added to 15 ml screw capped tubes. After addition of 1 ml 5 M potassium hydroxide and 5 ml dichloromethane, the tubes were shaken vigorously and then centrifuged at 4000 rpm for 4 min. The supernatants were discarded by aspiration. After evaporation to dryness under a gentle stream of nitrogen at ambient temperature, residues were reconstituted in 300 μl mobile phase. An aliquot (25 μl) was injected into the high performance liquid chromatography system via the automatic sampler.
Standards were prepared in solvent and blank urine and extracted. The standard curve prepared in urine was identical to the curve prepared in solvent. The limit of detection and quantitation, determined at a signal to noise ratio of 10, was 10 ng. Any samples below the level of detection (LOD) were denoted with a zero value.
Measurements of oxidative stress
F2-isoprostanes are generally regarded as one of the most reliable markers of oxidative stress as detected by lipid peroxidation.16,17 Spot urine samples from infants were collected as detailed above. Analysis was kindly performed by Dr Trevor Mori (UWA, School of Medicine and Pharmacology). F2-isoprostanes were extracted, purified and assayed using electron capture negative ionisation gas chromatography mass spectrometry (ECNI-MS) as previously described18 with minor modification. Briefly, urine (0.25 ml) was acidified to pH 4.5 and applied to a Certify II column (Varian) preconditioned with methanol (MeOH; 2.0 ml) and sodium acetate buffer/5% MeOH (pH 7, 2.0 ml). The column was washed with methanol/water (1:1, 2.0 ml) and ethyl acetate/hexane (25:75, 2.0 ml). The F2-isoprostanes were eluted with ethyl acetate/methanol (90:10, 2.0 ml) and evaporated to dryness in a centrifugal evaporator. 8-F2t-IsoP-d4 and 15-F2t-IsoP-d4 were added to all samples as internal standards. Samples were derivatised and analysed on an Agilent 6890 gas chromatograph coupled to an Agilent 5973 mass selective detector. Peaks representing F2-isoprostanes were identified by comparison of retention times. Creatinine was measured by enzymatic colorimetric test (Immunology Department, Princess Margaret Hospital, Perth, Australia) and urinary creatinine levels were used to estimate urinary dilution. Urinary F2-isoprostane levels were reported as pmol/mmol creatinine.
Statistical analysis
All statistical analyses were performed using SPSS software (Version 11 for Macintosh). Comparisons between continuous variables were determined by either the Student’s t test for parametric data or the Mann-Whitney U test for non-parametric data. Non-parametric correlations were determined by Kendall’s tau b to avoid “ties” in the data where a proportion of the variables of interest shared zero values. Multiple regression modelling was used to assess the effects of potential confounding factors. A p value of <0.05 was considered statistically significant for all analyses.
RESULTS
Population characteristics
The characteristics of the population are shown in table 1 for the infants of smokers (n = 33) and non-smokers (n = 54). There were no significant differences between the two groups in perinatal characteristics (including gestation, birth weight or Apgar scores), rates of maternal allergy (as a measure of infant allergy risk) or the number of children who had already developed symptoms of upper respiratory tract infection by 3 months of age. The rate of breastfeeding at 3 months of age was similar in the two groups, although more women in the smoking group had also used supplemental formula feeds. There was a trend for infants of non-smoking mothers to have more older siblings (p = 0.070) than infants of smoking mothers, but this did not quite reach statistical significance.
Maternal smoking status and infant exposure to environmental tobacco smoke
Maternal smoking behaviour (self-reported) is shown in table 2. All women who smoked in pregnancy continued to smoke in the postnatal period. Similarly, all of the non-smokers continued not to smoke during this same period. Of note, a high proportion (n = 25; 83.8%) of maternal smokers reported smoking “away from the child” (not shown). The rates of maternal-reported passive smoking (partner or other) were also higher if women smoked (table 2).
Characteristics of smoking behaviour and infant cotinine levels in the study population
Because of potential inaccuracies with self-reporting, we also measured urinary cotinine as an objective measure of exposure to environmental tobacco smoke. In this population, cotinine levels correlated with self-reporting (Kendall’s tau b = 0.186; p = 0.038). Infants of smokers had significantly higher urinary cotinine levels than infants of mothers who did not smoke (table 2).
Relationship between maternal smoking and infant oxidative stress
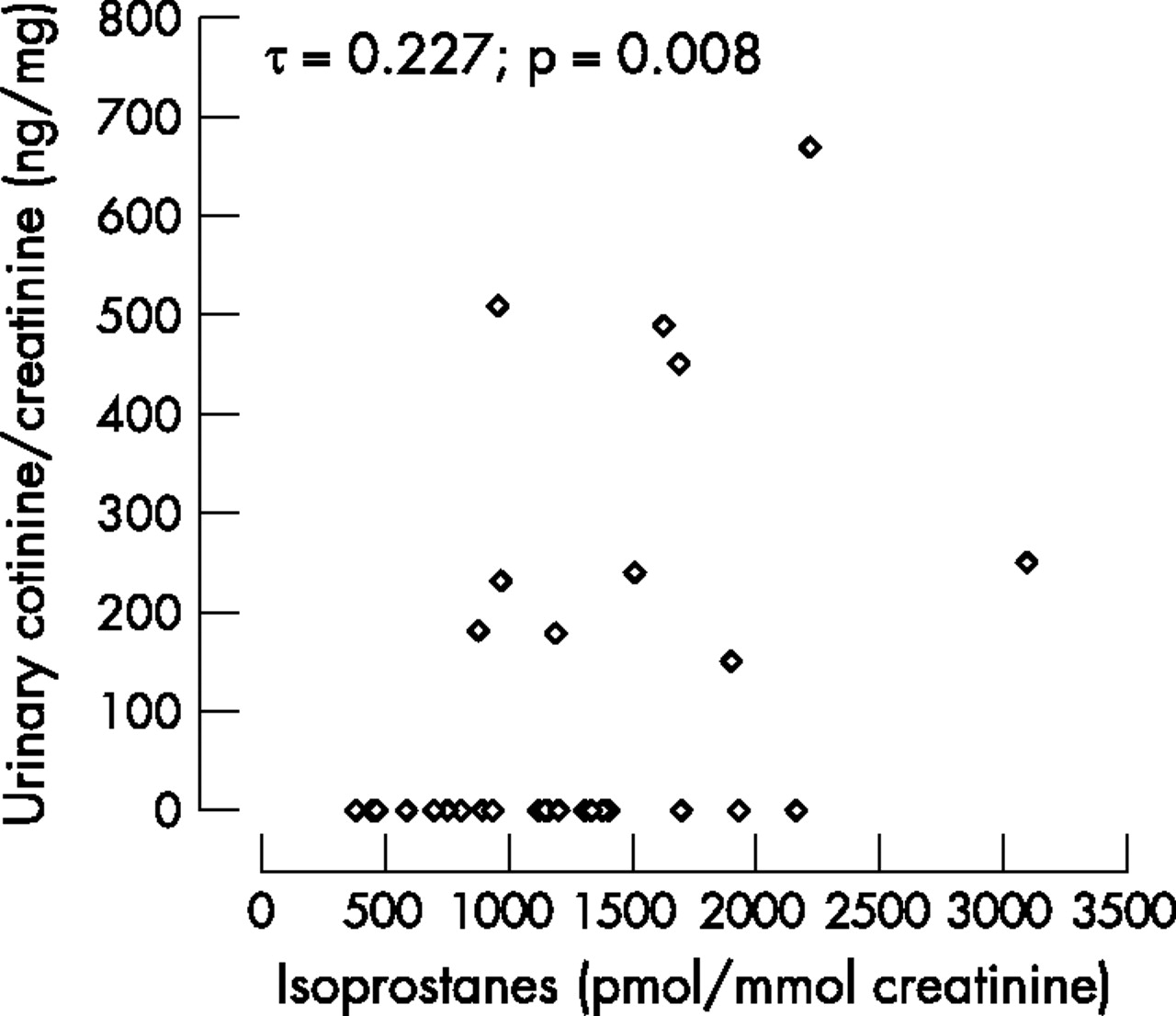
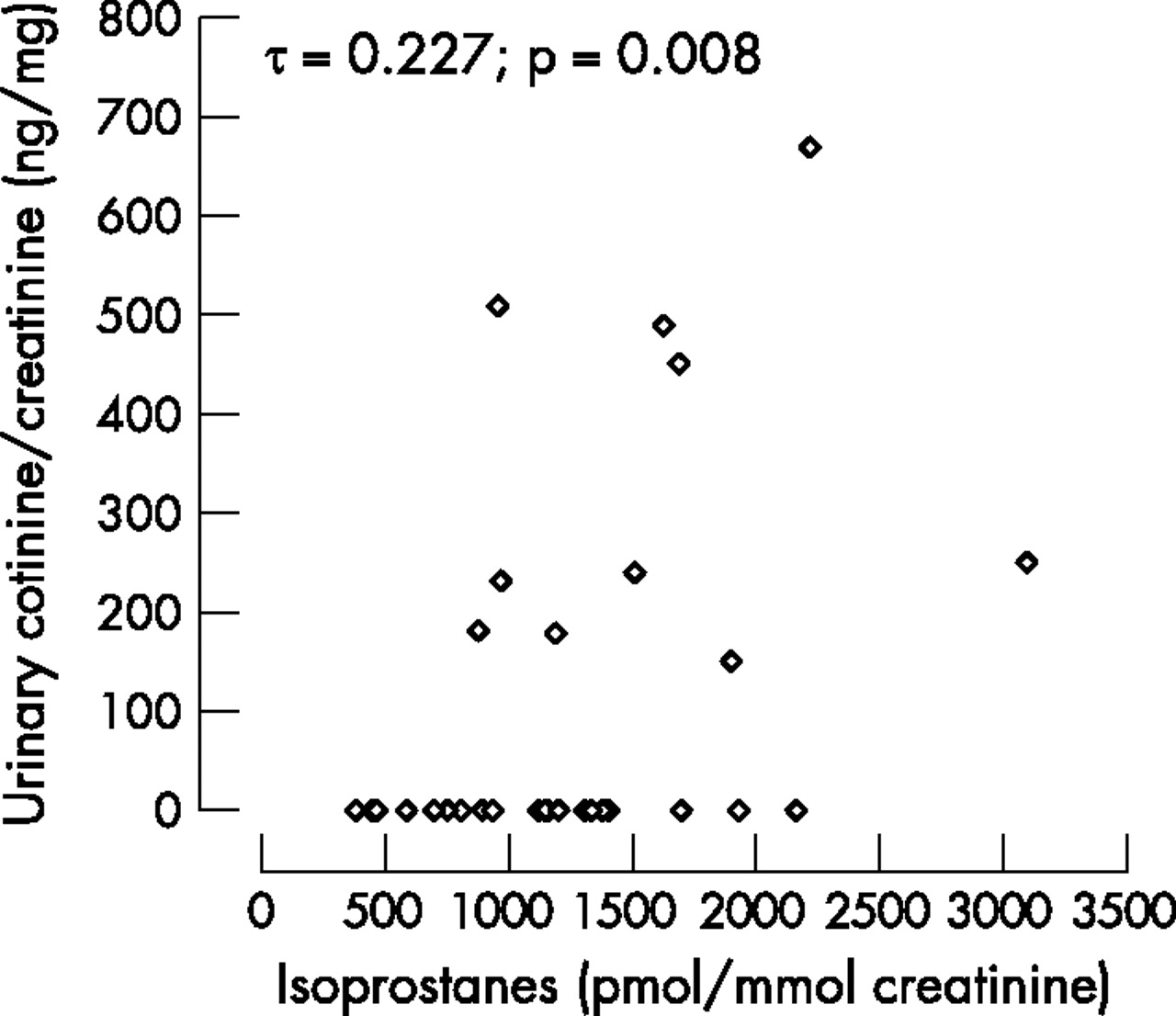
As indicated above, F2-isoprostane levels are the most reliable measure of oxidative stress (as lipid peroxidation). At 3 months of age, maternal smoking was associated with significantly higher infant urinary F2-isoprostanes (p = 0.015, fig 1). There was also a positive correlation between urinary F2-isoprostanes and infant urinary cotinine levels (Kendall’s tau b = 0.227, p = 0.008, fig 2).

Comparison of urinary F2-isoprostane levels in neonates born to mothers who smoked (shaded bars) and non-smoking mothers (clear bars). Data are displayed as median, 5, 25, 75 and 95 percentile ranges and outlying values. Differences between the two groups were determined by the Mann-Whitney U test. Significance levels are shown. p<0.05 is considered to be a significant difference between the two groups.
{kind=link}
{kind=link}
Association between urinary cotinine and F2-isoprostane levels in infants at 3 months of age. Only data from the smoking group were included in this analysis (n = 33). Kendall’s tau b and significance values are shown.
DISCUSSION
To our knowledge, this is the first study to show the effects of maternal smoking on urinary F2-isoprostanes as a robust marker of oxidative stress (lipid peroxidation) at 3 months of age. This effect was seen despite the fact that most mothers reported that they did not smoke “near” the baby.
Preliminary studies by other groups have shown that adverse effects on oxidative balance are likely to begin during gestation. In one small study, cord blood F2-isoprostanes were higher in newborn infants of smokers (n = 13) than in those of non-smoking mothers (n = 28).19 Animal studies have also shown the consequences of oxidative damage in the fetus from maternal environmental tobacco smoke, with oxidative nucleotide alterations and DNA damage.20 In this study, all women who smoked in pregnancy continued to smoke in the postnatal period. Although this study does not attempt to assess the separate effects of antenatal and postnatal cigarette exposure, our results suggest that postnatal exposure is a continued source of direct oxidative stress which is likely to compound the adverse effects of exposure in utero.
The balance between oxidative stress and antioxidant capacity is complex because of the independent variation of these parameters. Oxidative stress may not lead to tissue damage or adverse oxidative status in individuals with high levels of antioxidant function. In contrast, lower levels of oxidative stress could lead to tissue damage if antioxidant function is depleted. In addition to the effects on oxidative stress demonstrated here, others have also shown that maternal smoking is associated with depletion of serum antioxidant parameters (including vitamin C, thiol concentrations and measures of total antioxidant capacity) in infants of a similar age (6–28 weeks).21 Together with our findings, this indicates that parental smoking has significant adverse effects on oxidative balance in the very early postnatal period. These effects of passive smoke exposure are also supported by recent studies in older children which reported that oxidative stress (also measured by plasma peroxide levels) was significantly higher in children (aged 9–13 years) exposed to passive smoking than in children not exposed.22 This study also showed that exposure to environmental tobacco smoke was associated with a reduced total antioxidant response.22 The authors used these values to derive an oxidative stress index which was significantly higher in children exposed to passive smoking than in those not exposed.22
The significance of our findings and those of Aycicek et al21 is that these adverse effects on oxidative balance are evident very early in life when many systems are still developing. As such, the potential adverse effects are potentially greater than in mature systems. In the context of the increase in allergic diseases (namely asthma), there is growing concern that maternal smoking with its negative effects on infant “redox” status could play a role in altering immune development, possibly also by potentiating the effects of other environmental changes. In experimental models, oxidants induce many features of asthma and allergic diseases by inducing the release of pro-inflammatory mediators including cytokines (such as interleukin-6, tumour necrosis factor α and interleukin-1β), chemokines and eicosanoid metabolites. These effects appear to be mediated, at least in part, through oxidant-associated activation of at least two pivotal inflammatory regulators—nuclear factor-κB and activator protein 1. The impact of these effects on the developing immune system is still not clear and is the subject of ongoing investigation.
It should be noted that other studies have provided preliminary evidence that smoking may affect oxidative stress by measuring total peroxide levels.21 We selected F2-isoprostane as an alternative marker based on a recent review17 highlighting the greater utility of measuring this compound as an index of free radical-induced lipid peroxidation. Favourable characteristics include: stable compounds, specific products of lipid peroxidation, present in detectable quantities in all normal biological tissues and fluids and levels are unaffected by lipid content in the diet.
In summary, our findings strongly support the emerging literature that very early exposure to environmental tobacco smoke adversely affects the pro-oxidative/antioxidative status within weeks of life. There is already considerable indirect evidence that smoking has adverse effects on the fetus19 which may be mediated through increased oxidative stress, as well as direct toxic effects. Our findings emphasise the importance of better strategies to prevent exposure to cigarette smoke in early life when the potential for damage is greatest.
Acknowledgments
The authors thank the staff and patients who assisted in this study and the contribution by Elaine Pascoe.
REFERENCES
Footnotes
-
Published Online First 13 March 2007
-
Professor Prescott is funded by National Health and Medical Council (of Australia).
-
Competing interests: None declared.