Article Text

Statistics from Altmetric.com
A 69-year-old male non-smoker with a history of atopic asthma of >30 years had recently been diagnosed with pulmonary emphysema (chronic obstructive pulmonary disease, COPD) because of exertional dyspnoea and chronic airflow limitation without bronchodilator responsiveness. A laboratory examination revealed a high serum IgE level (1219 U/ml) and a normal α1-antitrypsin level (142 mg/dl), and the flow-volume curve showed severe chronic airflow obstruction (vital capacity (VC) 2.47 litres (72.3% predicted), forced expiratory volume in 1 s (FEV1) 0.73 litres (27.4% predicted), FEV1%-Gaensler 30.8%). The chest radiograph showed severe hyperinflation (fig 1A), but carbon monoxide transfer factor was within normal limits (15.43 ml/min/mm Hg 98.9% predicted). A chest CT scan revealed the presence of free air predominantly along the bronchovascular sheaths of both lungs with thickened bronchial walls; pulmonary emphysema, pneumothorax and pneumomediastinum were not observed (fig 2A and B). The previous repeated episodes of asthma could be considered as the cause of the pulmonary interstitial emphysema. The patient was treated with inhaled cortico-steroids, long-acting β2 agonists and leucotriene receptor antagonists. A few months later his respiratory symptoms had almost disappeared and the pulmonary function parameters had improved (VC 2.71 litres (78.9% predicted), FEV1 1.04 litres (40.3% predicted), FEV1.0%-G 40.6%). However, the CT findings remained unchanged throughout the 2 year observation period (fig 3).

Chest radiograph before treatment showing hyperinflated lungs and a decrease in pulmonary markings.
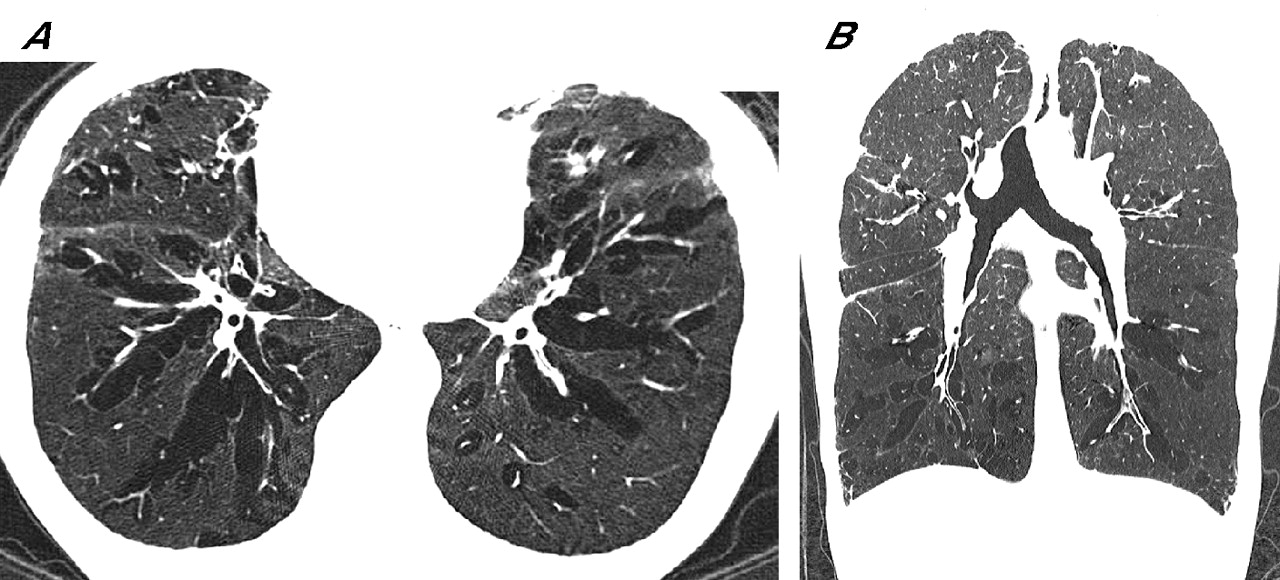
(A) Transaxial and (B) coronal sections of the chest CT scan before treatment showing diffuse pulmonary interstitial emphysema with multiple air lucencies contiguous to pulmonary vessels and bronchi on both lung fields.

{kind=link}
{kind=link}
{kind=link}
Chest CT scan 2 years later still showing diffuse pulmonary interstitial emphysema after treatment.
Pulmonary interstitial emphysema has been reported infrequently, mostly in newborn infants,1 and is associated with the Macklin effect2 which is seen in blunt chest trauma, neonatal respiratory distress syndrome, asthma crises and positive pressure mechanical ventilation. To our knowledge, spontaneous diffuse pulmonary interstitial emphysema in association with persistent asthma has not previously been reported and could be confused with pulmonary emphysema.
Learning points
-
Diffuse pulmonary interstitial emphysema complicated by persistent asthma is extremely rare.
-
The high resolution CT findings are characteristic and should help in differentiating pulmonary interstitial emphysema from pulmonary emphysema (COPD).