Article Text

Abstract
This case report describes the treatment of reperfusion lung oedema after pulmonary thromboendarterectomy using intravenous iloprost infusion in a 52-year-old woman diagnosed with chronic thromboembolic pulmonary hypertension.
- CTEPH, chronic thromboembolic pulmonary hypertension
- Fio2, fraction of inspired oxygen
- NO, nitric oxide
- Pao2, arterial oxygen pressure
- PAP, pulmonary artery pressure
- PTE, pulmonary thromboendarterectomy
- PVR, pulmonary vascular resistance
- RLE, reperfusion lung oedema
Statistics from Altmetric.com
- CTEPH, chronic thromboembolic pulmonary hypertension
- Fio2, fraction of inspired oxygen
- NO, nitric oxide
- Pao2, arterial oxygen pressure
- PAP, pulmonary artery pressure
- PTE, pulmonary thromboendarterectomy
- PVR, pulmonary vascular resistance
- RLE, reperfusion lung oedema
Chronic thromboembolic pulmonary hypertension (CTEPH) is the result of chronic obstruction of the pulmonary arteries by thrombi which ultimately leads to right heart failure and death. Pulmonary thromboendarterectomy (PTE) has emerged as a standard therapeutic approach.1 Reperfusion lung oedema (RLE), which presents as acute deteriorating oxygenation and postoperative pulmonary hypertension, is the single most frequent complication of PTE. Mechanical ventilation and inhaled nitric oxide (NO) have been advocated to improve RLE, but this treatment does not work in all patients.2 We describe a case of RLE after PTE who responded poorly to mechanical ventilation and inhaled NO but was successfully treated with intravenous iloprost given for 7 days.
CASE REPORT
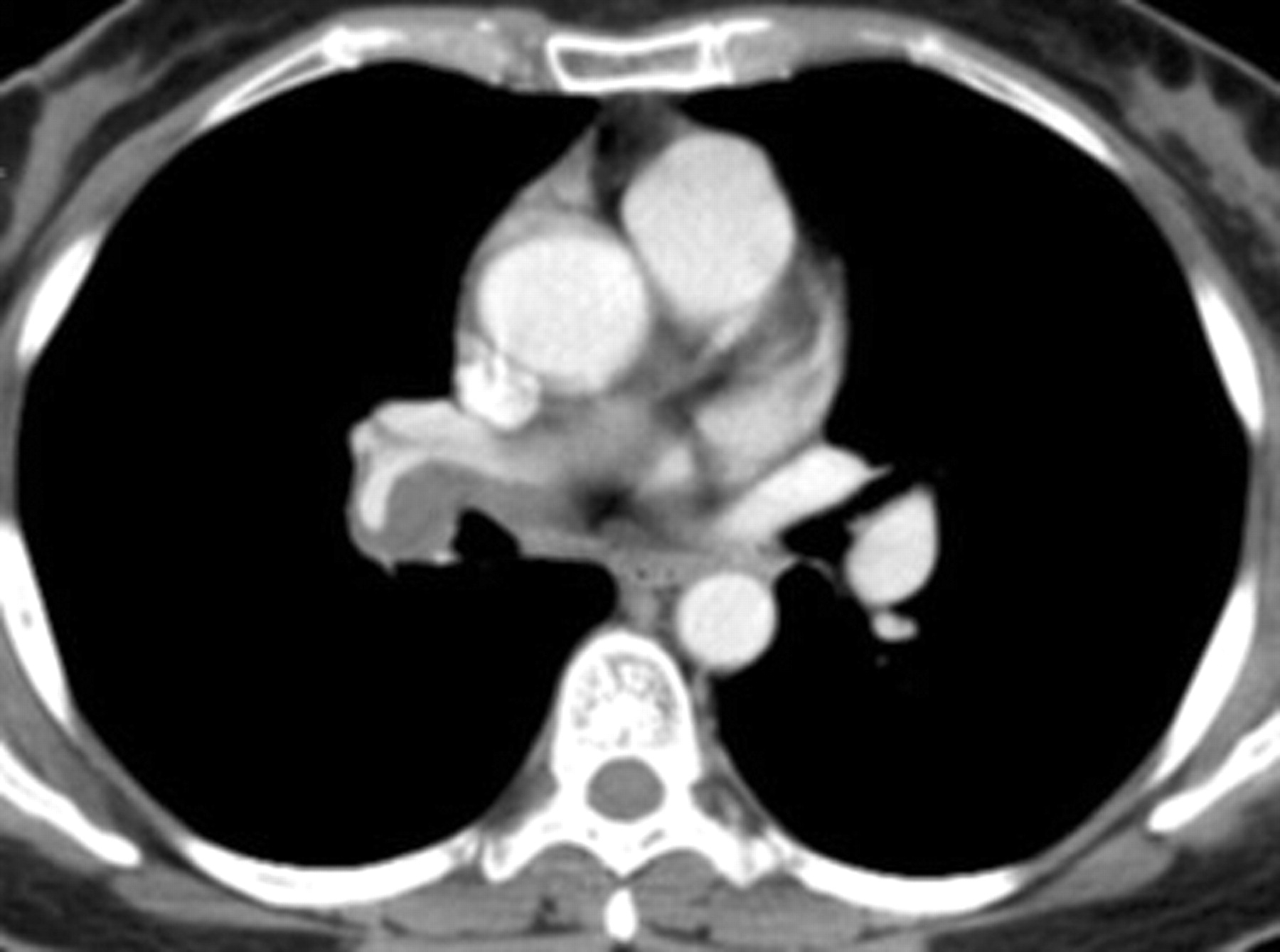
A 52-year-old woman presented at the hospital with severe exercise limitation and worsening dyspnoea. A chest radiograph showed bilateral prominent hilar shadows and a spiral chest CT scan revealed a large pulmonary embolism in the right main pulmonary artery, extending to the right middle and right lower lobar arteries (fig 1). A lung scan showed a global decrease in perfusion to the right lung, with additional defects involving the right middle and lower lobes. The ventilation scan was normal and there was no laboratory evidence of deep venous thrombosis. CTEPH was diagnosed, and treatment was started with high-dose intravenous heparin followed by oral anticoagulation therapy. A repeat lung scan and chest CT scan 12 months later showed no resolution of the thrombus. The NYHA functional class deteriorated from III to IV and the patient was referred to our institution for surgical intervention. An uneventful right PTE was performed. The patient was admitted to the ICU and extubated smoothly on the first postoperative day. Prostaglandin E1 and nitroglycerin were given and adjusted during the operation and throughout the ICU stay. The mean pulmonary artery pressure (mPAP) and pulmonary vascular resistance (PVR) decreased from 50 mm Hg and 422 dyne/s/cm5 preoperatively to 25 mm Hg and 240 dyne/s/cm5 postoperatively, and the ratio of arterial oxygen tension to fraction on inspired oxygen (Pao2/Fio2 ratio) increased from 139 to 317 (table 1). On postoperative day 2 the chest radiograph revealed dense opacity in the right lung field, in the regions of the lung recently supplied by blood from arteries opened by endarterectomy (fig 2A). There were no signs of active infection or pneumonia. The mPAP and PVR increased to 42 mm Hg and 395 dyne/s/cm5, respectively, and the Pao2/Fio2 ratio was only 70 (table 1). A diagnosis of RLE was made and the patient was reintubated and inhalant NO administered at 20 parts per million (ppm). After 1 h of inhaled NO the patient experienced little improvement: mPAP 40 mm Hg; PVR 387 dyne/s/cm5; Pao2/Fio2 ratio 110 (table 1). Intravenous iloprost (Ilomedin, 20 μg/ml, Schering AG, Berlin, Germany) was initiated and maintained at a dose of 0.5 ng/kg/min. After 30 min of treatment with iloprost the clinical parameters were greatly improved: the Pao2/Fio2 ratio increased to 408 and the mPAP and PVR were reduced to 30 mm Hg and 265 dyne/s/cm5, respectively (table 1). The patient was successfully weaned from the ventilator on postoperative day 4 and the iloprost dose was tapered off on postoperative day 8. Chest radiography performed on postoperative day 8 revealed a nearly clear lung field (fig 2B) and the patient was discharged on postoperative day 14. At follow-up 1 month later the patient’s functional status was improved from NYHA class IV to I and the 6 min walk distance increased from 195 m preoperatively to 432 m postoperatively.
Changes in haemodynamic parameters before and after pulmonary thromboendarterectomy
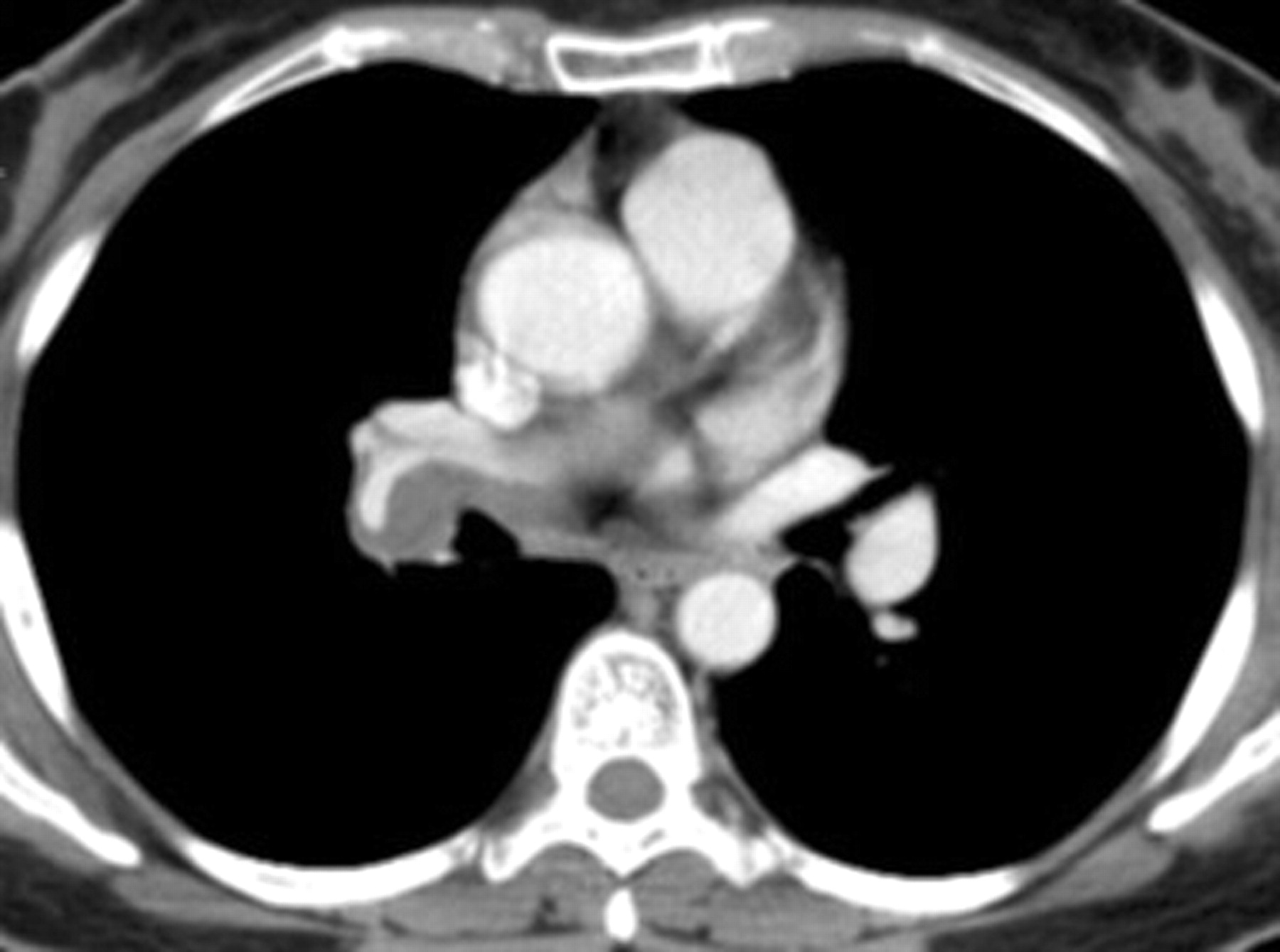
Chest CT scan showing pulmonary thromboembolus extending to the right middle and lower pulmonary arteries.

{kind=link}
{kind=link}
(A) Chest radiograph on postoperative day 2 showing a dense opacity in the right lung field following pulmonary thromboendarterectomy. (B) Chest radiograph on postoperative day 8 showing a nearly clear lung field after 7 days of treatment with intravenous iloprost.
DISCUSSION
The most important factor complicating the early postoperative period after PTE is RLE.1,2 Case studies have reported the advantages of inhalant NO in the treatment of RLE,3 but a recent randomised controlled study found no response in these patients.4 Furthermore, rebound pulmonary hypertension and possible build-up of oxygen radicals limit the use of NO. Therefore, in patients with RLE not responsive to inhaled NO and mechanical ventilation, the dilemma remains as to how to resolve poor oxygenation, high PVR, and critical pulmonary hypertension.
Iloprost, a stable analogue of prostacyclin, has a selective vasodilator effect on the pulmonary vasculature and markedly lowers PVR.5 Olschewski et al6 showed that long-term inhalation of aerosolised iloprost in patients with CTEPH resulted in improvement in the clinically important end points of exercise capacity, NYHA class, and overall clinical condition. Kramm and colleagues7 reported that aerosolised iloprost improved the early postoperative haemodynamics and reduced RLE in patients with CTEPH following PTE. However, a major drawback of this inhalation therapy is the relatively short duration of action, with the haemodynamic effects detectable for only 30–60 min after each inhalation. Theoretically, a minimum of 12 inhalations per 24 h would be required to achieve “continuous” haemodynamic efficacy for treatment of critical RLE. Furthermore, in intubated patients, a special inhalation device and jet nebuliser is needed to administer and aerosolise the drug. Concern has therefore been raised that the inhaled form of iloprost may be less effective and practical than the intravenous form. In our case, intravenous iloprost was administered instead of intravenous epoprostenol, since iloprost is much more stable and the longer half-life makes iloprost potentially safer than epoprostenol.5
It is reasonable to doubt the beneficial effect of iloprost infusion since most cases of RLE recover with supportive care. However, Daily et al reported that the most significant cause of death after PTE in 149 patients was respiratory failure, a consequence of RLE associated with 59% of deaths.8 Furthermore, Levinson and colleagues reported that 5 of 21 patients who developed RLE needed more than 2 weeks for the pulmonary infiltrates to clear on the chest radiograph under supportive care, and 3 of them required more than 3 weeks to recuperate.9 We were able to wean our patient off mechanical ventilation 3 days after intravenous iloprost treatment. Subsequent chest radiographs showed that the opaque area of RLE was quickly resolved. This implies that both the time to clearance of RLE and the duration of mechanical ventilation might be reduced with intravenous iloprost.
There may be some concern as to whether inhalation of 20 ppm NO for 1 h is enough to achieve maximal vasodilation; that is, whether the concentration or the duration of treatment is sufficient. Recent investigations have shown that the maximum effect on PAP is achieved with NO concentrations between 10 and 20 ppm, and higher concentrations do not augment the vasodilatory action.10 Imanaka et al3 reported that inhaled NO at 20 ppm administered for 30 min after PTE improved oxygenation and decreased PVR. In our case there was no sign of clinical improvement after inhalation of 20 ppm NO for 1 h. It is therefore reasonable to assume that the RLE did not respond to NO treatment. However, the reasons for the ineffectiveness of inhaled NO remain unclear.
In summary, continuous intravenous iloprost appears to be effective in improving postoperative hypoxia and decreasing raised pulmonary hypertension and PVR associated with RLE following PTE when mechanical ventilation and inhaled NO fail. In specific cases such as ours, short-term treatment with low-dose continuous intravenous iloprost can make a major and safe contribution to the management of these postoperative complications.
Acknowledgments
The authors thank Shu-Fang Hsiao, Yu-Mei Lai and Pi-Ru Tsai for providing technical assistance and secretarial support.
REFERENCES
Footnotes
-
Funding: None.
-
Competing interests: None declared.