Article Text

Statistics from Altmetric.com
We wish to share our experience in an unusual case presentation of pulmonary hypertension. A 48-year-old Caucasian female with a history of hypothyroidism and smoking presented with progressive dyspnoea on exertion for 3 years, markedly worse during the past 6 months. She also had arthralgias, Raynaud’s phenomena, night sweats and a 25-pound weight loss over 6 months. Chest computed tomography scan showed diffuse mediastinal lymphadenopathy. Lymph node biopsy showed non-necrotising epithelioid granulomas compatible with sarcoidosis. Symptoms worsened despite treatment with prednisone.
Pulmonary function tests showed mild restrictive disease, reduced diffusion capacity and desaturation during a 6-min walk. Echocardiogram showed a severely dilated and hypokinetic right ventricle. Right heart catheterisation showed pulmonary artery pressure 79/38 mm Hg (mean 46 mm Hg), cardiac output 6.7 l/min and cardiac index 3.7 l/min/m2. There was no significant response to inhaled nitric oxide at 20 ppm.
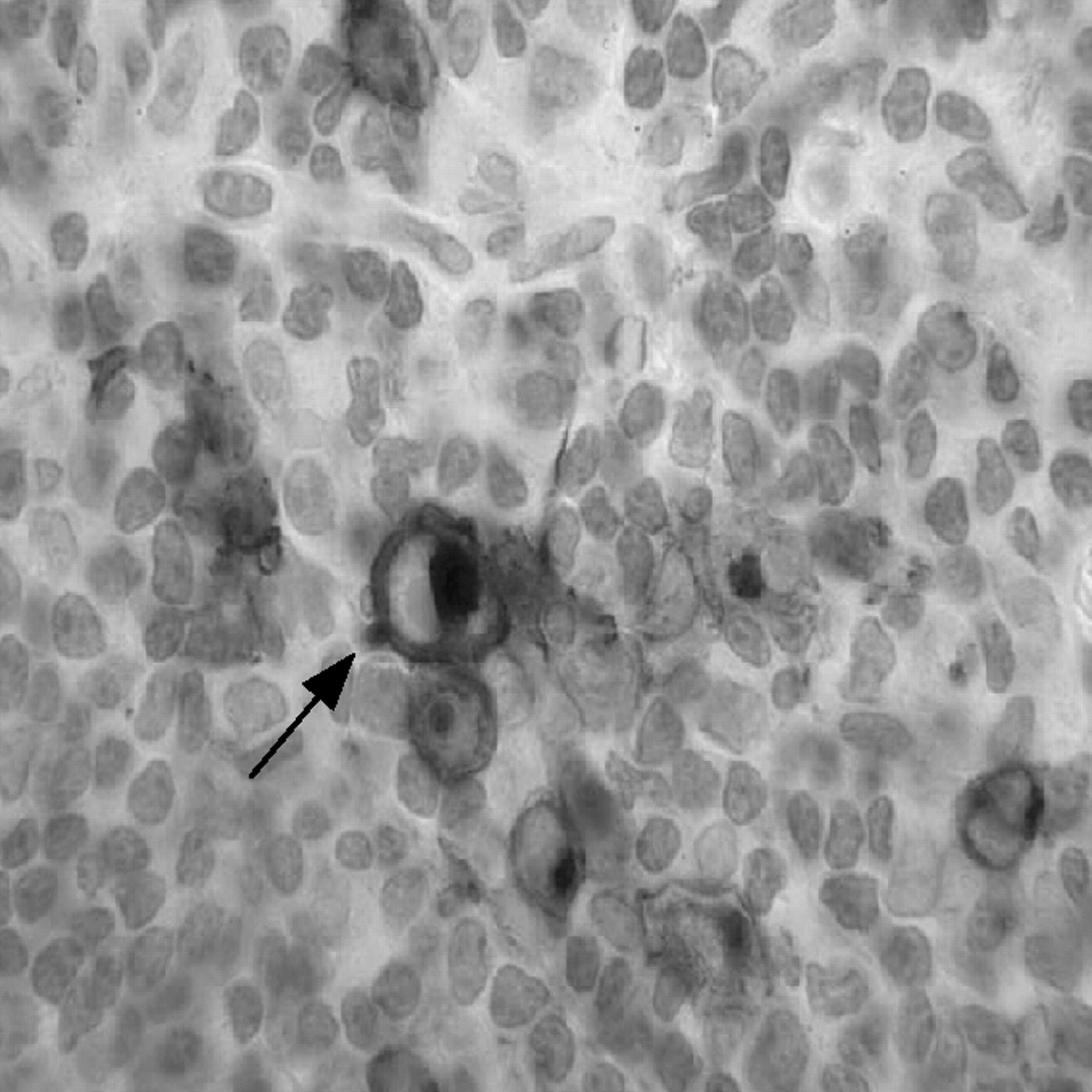
A retrospective review of her pathology showed a dominant reaction pattern consistent with sarcoidosis, small foci of paracortical infiltration by large mononuclear and binucleated haematopoietic elements, and a concomitant background of tissue eosinophilia. Immunohistostaining was consistent with mixed cellularity Hodgkin’s lymphoma (fig 1⇓).
{kind=link}
The neoplastic cell populace shows characteristic CD30 positivity (arrow) manifesting a sharp, cytoplasmic, membrane-like and perinuclear staining pattern (avidin biotin dibenzidine ×1000).
She was initiated on epoprostenol by continuous infusion. Owing to her pulmonary and cardiac disease, she received six cycles of chlorambucil, vinblastine, procarbazine and prednisone. She achieved a complete response and remains in remission 20 months after chemotherapy. She continues on epoprostenol therapy with improved exercise tolerance. Repeat right heart catheterisation showed pulmonary artery pressure 48/21 (mean 30 mm Hg), cardiac output 7.8 l/min and cardiac index 4.6 l/min/m2. Attempts to wean epoprostenol were unsuccessful.
Sarcoid-like reactions are defined as areas of non-caseating granulomas seen on biopsy in patients without symptoms of systemic sarcoidosis. Radiographically, patients with intrathoracic sarcoid-like reactions may present with hilar or mediastinal adenopathy, ground-glass infiltrates or a perivascular nodularity mimicking sarcoidosis.1 Among the various conditions associated with a sarcoid-like diathesis are infections, hypersensitivity reactions, and solid or haematological malignancies.
In malignancy, this pathology can be seen at the primary tumour site, particularly in T cell lymphoma and Hodgkin’s disease, in lymph nodes draining the region, or in distant organs such as the spleen, liver or bone marrow. Up to 4.4% of patients with carcinoma, 7.3% of patients with non-Hodgkin’s lymphoma and 13.8% of patients with Hodgkin’s disease will feature sarcoid-like reactions.2
Pulmonary arterial hypertension (PAH) develops in up to 28% of patients with sarcoidosis.3 The aetiology of PAH in sarcoidosis is generally presumed to be secondary to parenchymal fibrosis and hypoxaemia.4 However, PAH may develop in patients without extensive parenchymal destruction secondary to perivascular or intravascular granulomatous inflammation, granulomatous angiitis, extrinsic compression of the main or peripheral pulmonary arteries by mediastinal lymph nodes or fibrosis with resultant pulmonary stenosis.5
The response of PAH secondary to sarcoidosis in the treatment for sarcoidosis is uncertain; in a case series, the haemodynamic response to steroid therapy was found to be lagging behind the radiographic and pulmonary function test improvement, and was not universally seen.6 In a small study, patients with severe PAH secondary to sarcoidosis were found responsive to vasodilator therapy.3 PAH in association with sarcoid-like reactions is not described, and management is unproven.
No cases of PAH secondary to a sarcoid-like reaction or Hodgkin’s disease have been reported previously. This case underscores the association of lymphoma and sarcoid-like reactions, and the possibility that PAH in these patients may be underappreciated. This case also emphasises the importance of a systematic evaluation for lymphoproliferative disease in patients with lymphadenopathy presumed to be sarcoidosis.
Footnotes
Competing interests: None declared.