Article Text

Statistics from Altmetric.com
A 49-year-old man was referred for dizziness and malaise. Echocardiogram showed a 3×2.5 cm mass within the left ventricle. A contrast-enhanced 16-row multislice computed tomography (MSCT) scan with retrospective ECG-gated reconstruction confirmed the mass, without infiltration of the left ventricular wall or marked coronary artery stenosis (fig 1⇓). Surgical resection of the mass was performed, and 6 days later, the patient was discharged from hospital without radiotherapy or chemotherapy.
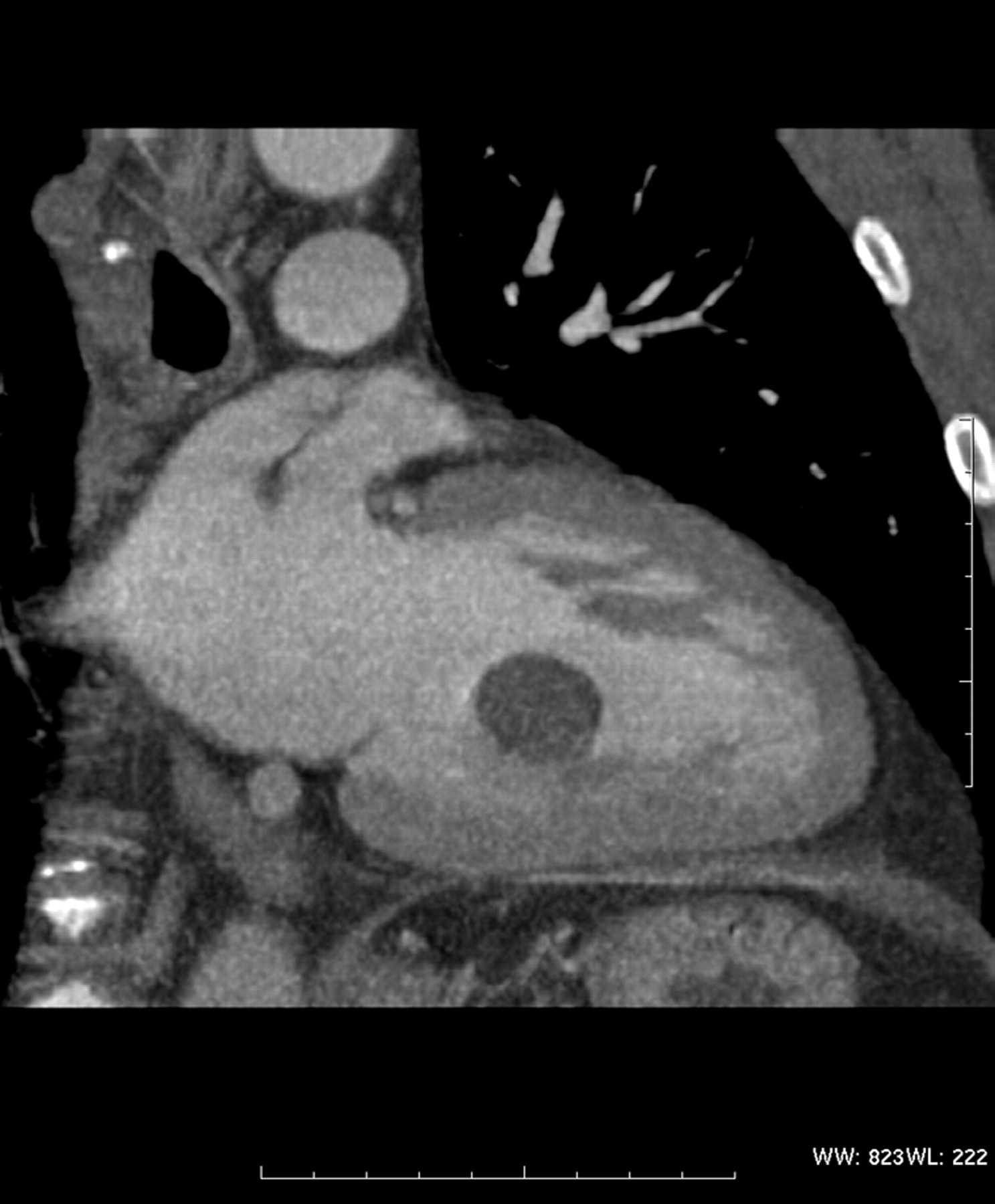
Sixteen slice computed tomographic imaging with retrospective electrocardiogram-gated reconstruction: subvalvular implantation of the tumour pediculated on the posterior papillary muscle, without infiltration of the left ventricular wall.
On pathological examination, the gross appearance was that of a soft, tan–yellow mass with smooth contours. Haemorrhagic areas were noted. The cells exhibited marked pleiomorphism and abundant mitotic figures. The tumour cells were positive for muscle cell antigen/CD34 and smooth muscle actin. Immunohistochemical stains were diffusely positive for vimentin and focally positive for desmin and CD68. These findings are consistent with the diagnosis of primary heart leiomyosarcoma.
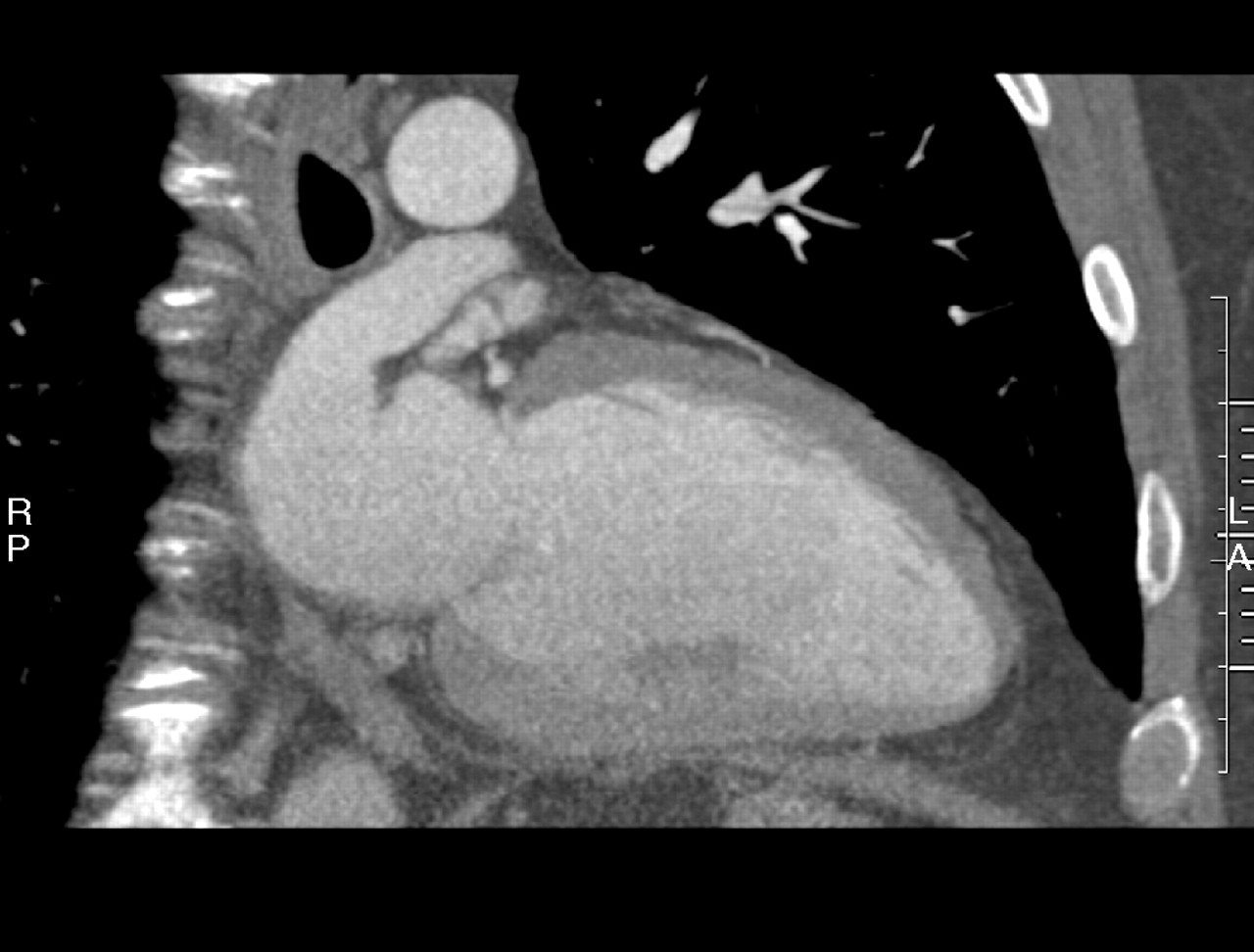
After 18 months, a heart MSCT examination showed absence of recurrence of the tumour (fig 2⇓). After 3 years, the patient is doing well with a normal echocardiogram and MSCT.

{kind=link}
{kind=link}
Sixteen slice computed tomographic imaging 18 months after the surgical treatment: absence of recurrence of the tumour.
Primary cardiac tumours are uncommon, with an incidence ranging from 0.001% to 0.03%.1 Leiomyosarcomas are about 9% of primary malignant cardiac tumours, and are highly aggressive and locally invasive. Leiomyosarcomas are uncommon malignancies of soft tissue associated with a poor prognosis owing to local and metastatic disease. Extra cardiac localisations are in the retroperitoneum, gastrointestinal tract, uterus, skin and vessels. Chemotherapy or radiotherapy gives poor results and are controversial.1,2 Surgical treatment offers the best chance of cure.
Learning points
Multislice computed tomography with retrospective echocardiogram-gated reconstruction provides an excellent anatomical definition of the cardiac tumour demonstrating the surgical resection possibilities.
Surgical treatment of cardiac tumours offers the best chance of cure, if it is possible and complete.
Echocardiograms are mainly used in the diagnosis of cardiac tumours. Our reported case illustrates the value of MSCT imaging in providing an excellent anatomical definition of the tumour, the screening of all cardiac chambers and the depiction of coronary artery vessels.
Footnotes
Patient consent was not obtained for publication of details in this article.