Article Text

Abstract
Background: In occupational asthma continued workplace exposure to the causative agent is associated with a poor prognosis. However, there is little information available on how rapidly lung function declines in those who continue to be exposed, nor how removal from exposure affects lung function.
Methods: Forced expiratory volume in 1 second (FEV1) was studied in 156 consecutive subjects with occupational asthma (87% due to low molecular weight agents) using simple regression analyses to provide estimates of the decline in FEV1 before and after removal from exposure.
Results: In 90 subjects in whom FEV1 measurements had been performed for at least 1 year before removal from exposure (median 2.9 years), the mean (SE) rate of decline in FEV1 was 100.9 (17.7) ml/year. One year after removal from exposure FEV1 had improved by a mean (SE) of 12.3 (31.6) ml. The mean (SE) decline in FEV1 was 26.6 (18.0) ml/year in 86 subjects in whom measurements were made for at least 1 year (median 2.6 years) following removal from exposure. The decline in FEV1 was not significantly worse in current smokers than in never smokers, nor was it affected by the use of inhaled corticosteroids.
Conclusion: FEV1 declines rapidly in exposed workers with occupational asthma. Following removal from exposure, FEV1 continued to decline but at a slower rate, similar to the rate of decline in healthy adults.
- FEV1, forced expiratory volume in 1 second
- PEF, peak expiratory flow
- occupational health
- asthma
- lung function
- exposure
Statistics from Altmetric.com
Forced expiratory volume in 1 second (FEV1) is an important measure of disease severity in obstructive lung disease and is a strong predictor of long term outcome. The rate at which FEV1 declines is also a prognostic marker and has been shown to be a predictor of survival independent of FEV1.1 FEV1 has been found to decline at a rate of about 25 ml/year in healthy adults, about 40 ml/year in asthmatic subjects,2 and about 60 ml/year in smokers with chronic obstructive pulmonary disease (COPD).3 In occupational asthma, continued exposure to the causative agent is recognised as being associated with a poorer outcome.4 It is frequently assumed that removal from exposure leads to an improvement in asthma, but it is unclear how removal from exposure influences FEV1. Pirilla et al5 reported a mean rate of decline of 40 ml/year in 91 selected subjects with isocyanate induced occupational asthma, although only 12 of these continued to be exposed to the causative agent in the workplace during the period of follow up. The aim of this study was to determine how removal from exposure to the causative agent in workers with occupational asthma influenced the rate of change in lung function.
METHODS
Subjects
Subjects previously diagnosed as having occupational asthma were retrospectively identified from the SHIELD database (occupational asthma reporting scheme for the West Midlands region of the UK). The subjects included in the study were all seen at the Birmingham Chest Clinic with a clinical history suggestive of occupational asthma and reported to SHIELD with a date of diagnosis between 1 January 1993 and 15 July 1999, and had a serial peak expiratory flow (PEF) record diagnostic of occupational asthma (Oasys-2 score >2.5).6 A total of 158 subjects were identified, two of which were excluded as there was evidence of coexisting interstitial lung disease.
Study protocol
Subjects with a diagnosis of occupational asthma are routinely followed up at the Birmingham Chest Clinic even after they are removed from exposure. Spirometric tests were performed at all visits. Results of pre-bronchodilator FEV1 from the time of first diagnosis were retrospectively sought from clinic notes in all study subjects and entered into a database along with the date of measurement. Spirometric recordings were checked for acceptability and reproducibility. If there was documented evidence of a respiratory tract infection in the clinic notes on the date of spirometry, the reading was ignored. All study subjects were interviewed between July 1999 and November 2001 and the date of removal from significant exposure to the causative agent was identified. Evidence taken into consideration for deciding the date of removal from exposure included:
-
The subject’s own recollection of events, with particular emphasis on when work related respiratory symptoms by and large ceased and dates of relocation.
-
The place of work, level of exposure, and presence of work related respiratory symptoms as recorded in clinic notes by the attending physician at follow up clinic appointments.
-
PEF records performed subsequent to the one used for diagnosis; an ongoing work related deterioration was seen as evidence of ongoing exposure.
-
Correspondence pertaining to removal from exposure from an occupational physician and/or human resources for the place of work.
Results of spirometric tests or non-specific bronchial hyperresponsiveness were not used as evidence for identifying the date of substantial removal from exposure. FEV1 measurements (either at the Chest Clinic or at the place of employment where hard copies were available) were defined as being made while exposed or after removal from exposure on the basis of the date of removal from exposure. The smoking status of study subjects was categorised as current if they were smoking at the time of final follow up, ex-smoker if they had stopped smoking for at least 1 month at final follow up, and never smoked if they had smoked less than 100 cigarettes in total.
Data analysis
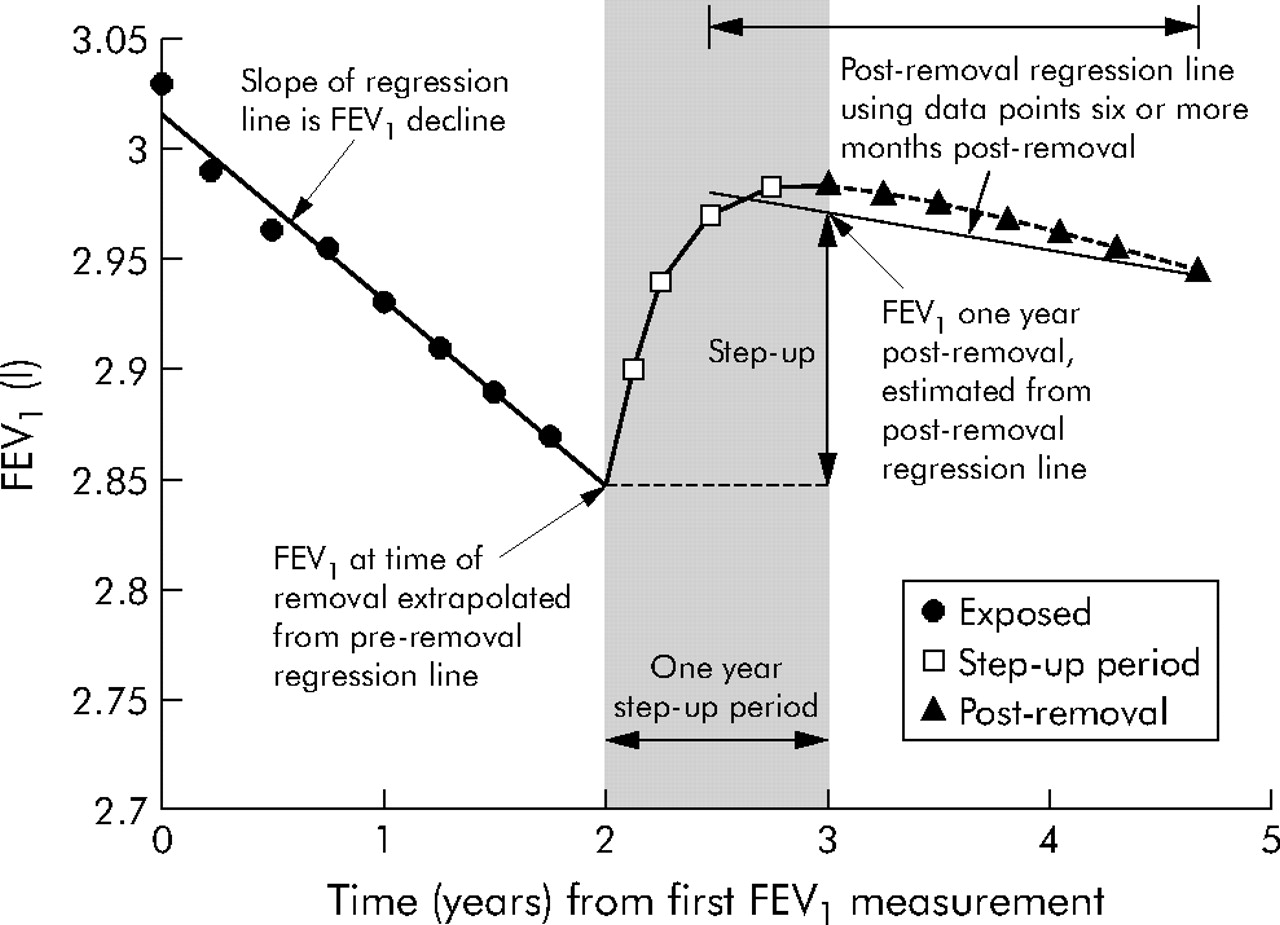
The model used for the analysis of FEV1 decline is shown diagrammatically in fig 1. The mean annual rate of decline in FEV1 was calculated separately for the exposed period and for the period after removal from exposure using simple linear regression for each subject. FEV1 measurements made before the age of 25 years were not included in regression estimates for any individual. The decline in FEV1 was only determined in subjects who had readings over at least 1 year for the relevant pre- or post-removal period. In addition, for the post-removal period, readings taken less than 6 months after removal were excluded. The model also includes an uplift effect on FEV1 occurring over 1 year following cessation of exposure. This uplift effect is the difference in FEV1 estimated at the time of removal and the estimated FEV1 1 year after removal from exposure. The estimated FEV1 at the time of removal was calculated by extrapolating the exposed regression line to the time of removal. The estimated FEV1 1 year after removal was calculated using a regression line fitted to readings more than 1 year after removal. However, as there were generally fewer readings taken more than 1 year after cessation of exposure, data obtained at least 6 months after removal were also included in this regression line. This was to minimise variability in the magnitude of the step-up and slope of the post-removal regression line at the expense of slightly underestimating the step-up and post-removal slope. Where there were insufficient data to calculate a slope for the pre- and post-removal regression lines—for example, readings not spread over at least 1 year—a step-up was still calculated using the average of readings for pre- and/or post-removal periods as necessary. However, in these cases the pre- and/or post-removal FEV1 slope could not be calculated.

Model of change in FEV1 over time in response to exposure and removal from exposure.
Paired t tests were used to compare the step-up against the rate of decline before removal from exposure in subjects in whom both values were available. The null hypothesis was that the step-up over the 1 year period after removal was no different from the mean rate of decline during exposure—that is, removal from exposure had no effect. Similarly, the rate of decline after removal from exposure was compared with the rate of decline during exposure in subjects in whom both values could be calculated.
RESULTS
One hundred and fifty six subjects were identified with occupational asthma confirmed by PEF records; the main causative agents are listed in table 1. In 90 workers FEV1 measurements were made for at least 1 year before removal from exposure. The step-up in FEV1 after 1 year of removal from exposure could be calculated in 114 subjects and the decline in FEV1 following removal from exposure could be determined in 86. Forty four subjects had measurements in all three phases. The number of subjects with sufficient data for FEV1 regression estimates to be determined for exposed, step-up, and follow up periods is shown in fig 2. Demographic data for the whole group and for the subgroups were similar and are shown in table 2.
Main causative agents
Demographic data of whole group and subgroups of follow up study population
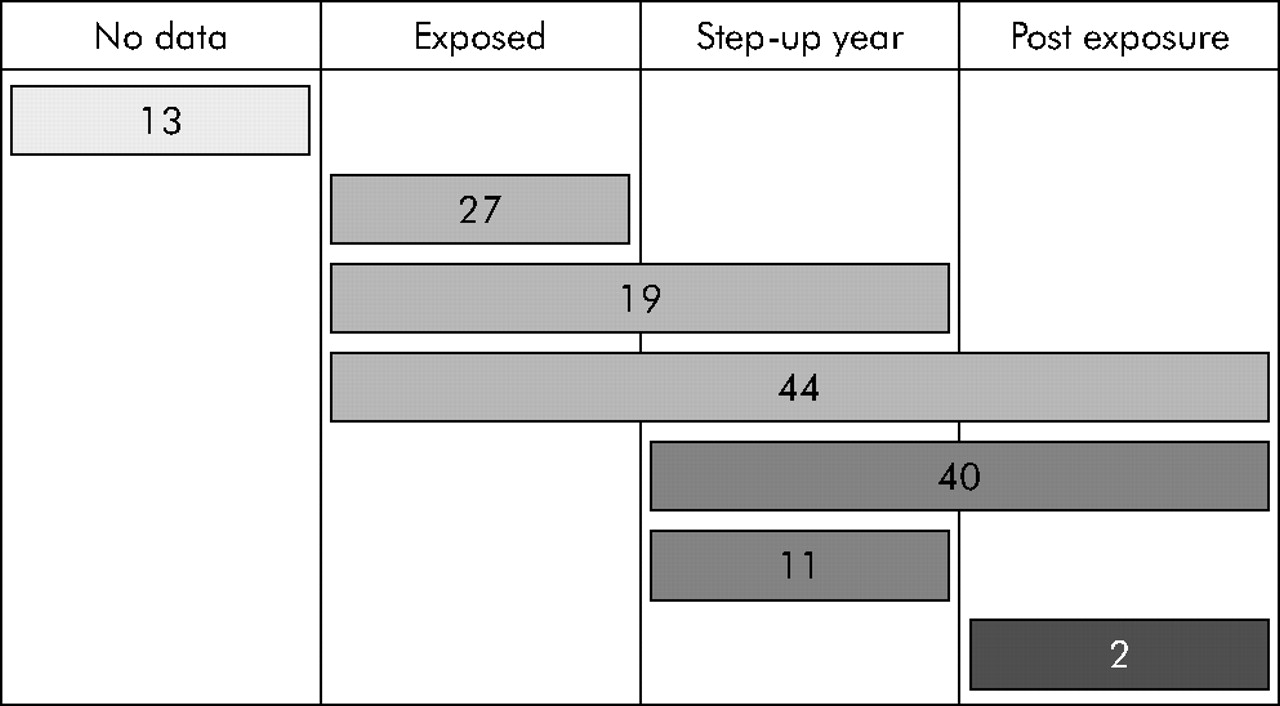
Subject inclusion diagram showing numbers according to sufficiency of data to determine FEV1 decline during exposed, step-up, and follow up periods.
Mean annual change in FEV1 while exposed to causative agent
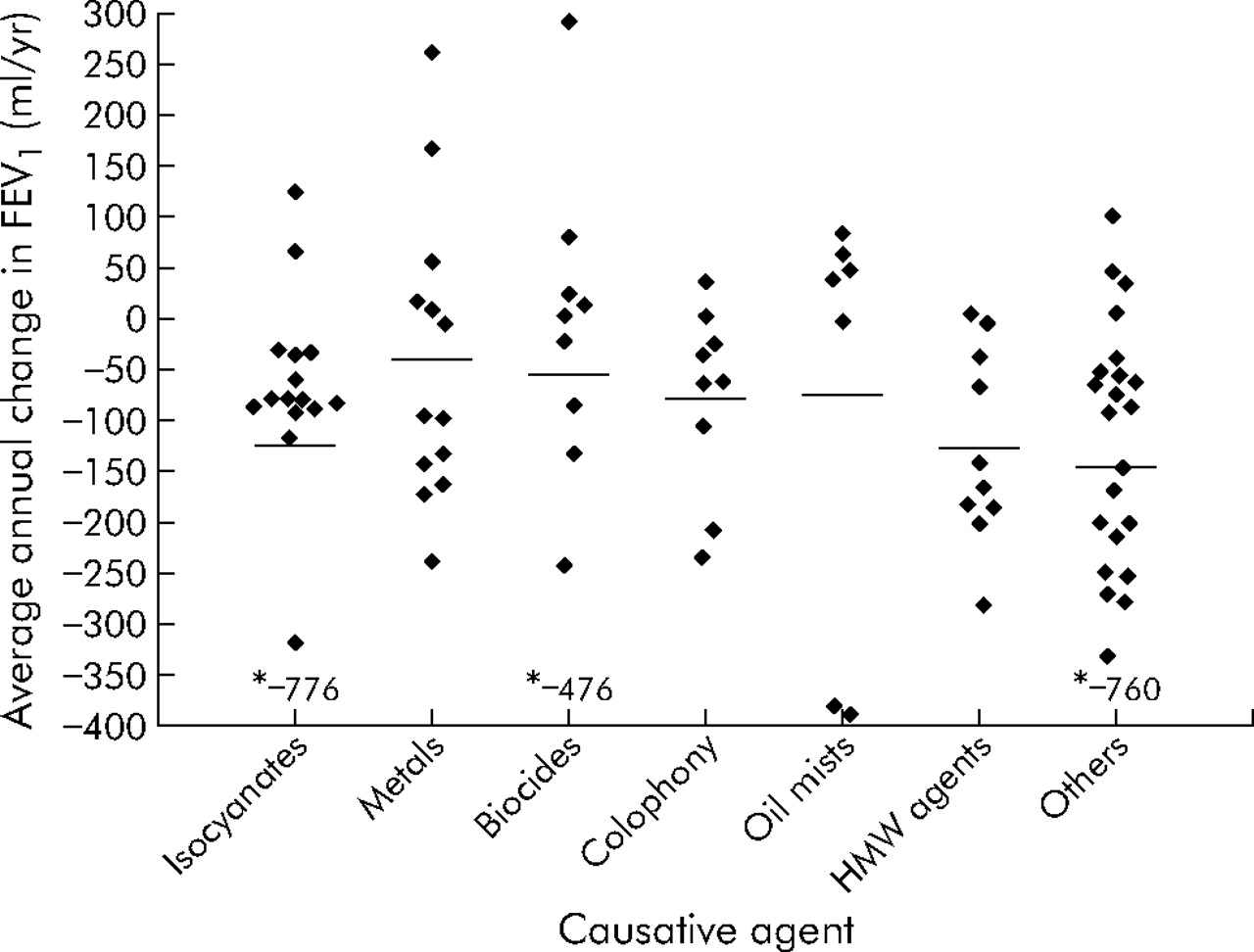
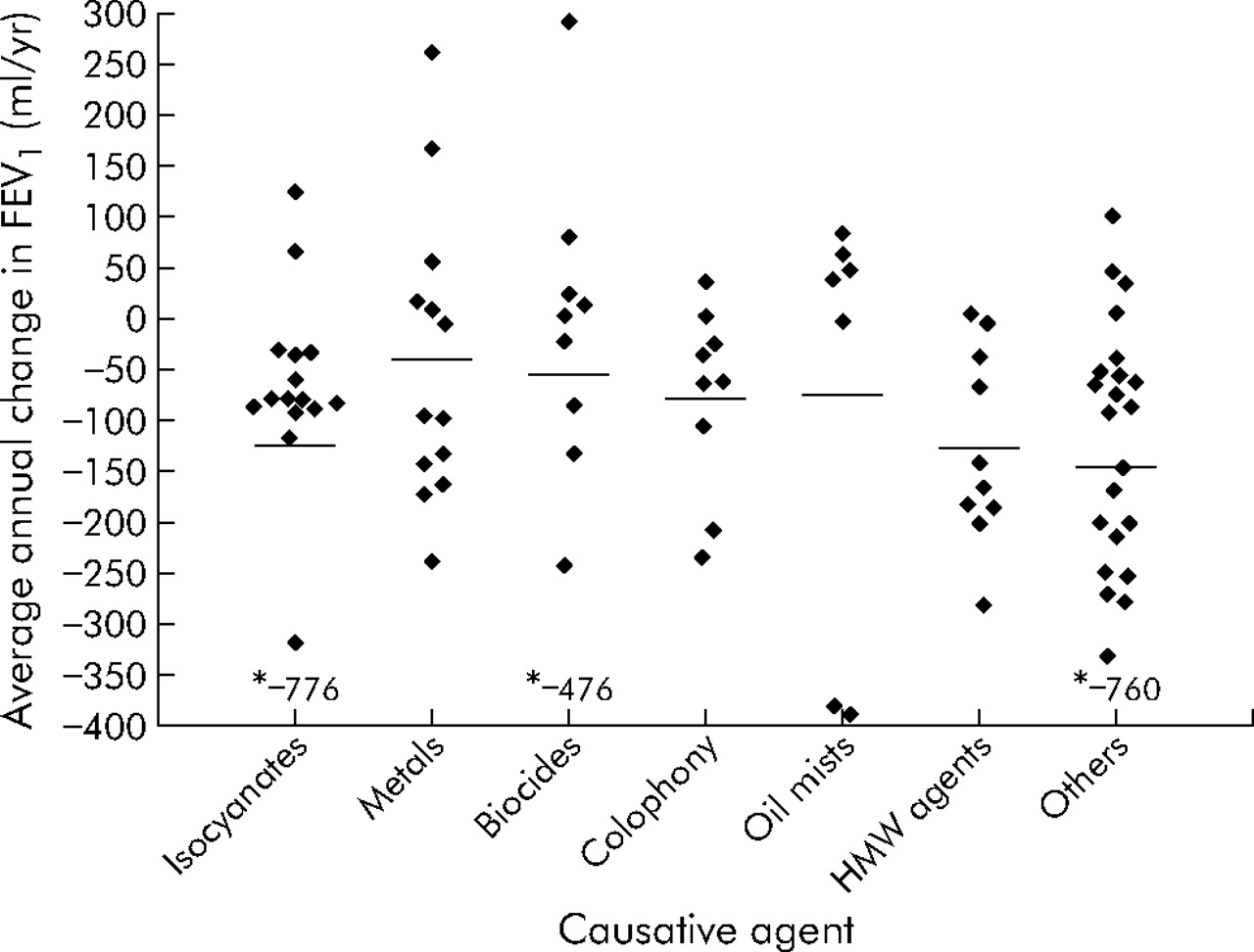
One hundred and forty three subjects had 952 FEV1 measurements before removal from exposure to the causative agent, although only 90 subjects had FEV1 measurements made over a period of at least 1 year (median 2.9 years, interquartile range (IQR) 1.8–4.8) before removal. In these 90 subjects the mean (SE) rate of decline in FEV1 was 100.9 (17.7) ml/year. Individual regression estimates by class of agent are shown in fig 3.
{kind=link}
{kind=link}
{kind=link}
Individual regression estimates of mean annual FEV1 decline in subjects with measurements over at least 1 year (median 2.9 years) during exposure according to class of causative agent.
The rate of decline did not correlate with age at baseline (r = −0.17, p = 0.13) or sex (98 ml/year in men, 107 ml/year in women, p = 0.81). The rate of change in FEV1 did not correlate significantly with initial FEV1 percent predicted (r = −0.12, p = 0.28). The mean rate of decline in atopic subjects was 128 ml/year compared with 72 ml/year in non-atopic subjects (p = 0.16). The rate of decline was 129.2 ml/year in current smokers, 132.8 ml/year in never smokers, and 43.7 ml/year in ex-smokers (95% CI of difference between current and ex-smokers 2 to 159 ml/year, p = 0.023). The mean (SE) rate of decline was 104.9 (17.9) ml/year in those treated with inhaled corticosteroids and 83.7 (51.7) ml/year in those not treated with inhaled corticosteroids; this difference was not statistically significant (p = 0.63). The rate of decline was not related to the latent interval between first exposure and first symptoms (Spearman’s rho = −0.07, p = 0.52).
Step-up in FEV1 on removal from exposure
A value for the step-up in FEV1 1 year after removal from exposure was calculated in 114 of the 156 subjects. The mean (SE) step-up for the group as a whole was +12.3 (31.6) ml. Step-up was not related to age (r = 0.06, p = 0.54), atopic status, or smoking status (p = 0.42, one way ANOVA), nor was it related to the latent interval between first exposure and first symptoms (r = −0.13, p = 0.16), duration of symptomatic exposure (r = 0.05, p = 0.6), or initial FEV1 percent predicted (r = 0.03, p = 0.79). Treatment with inhaled corticosteroids before removal from exposure did not influence the step-up in FEV1, nor was there any evidence that the addition of inhaled corticosteroids after removal from exposure had a major beneficial effect on step-up in FEV1:
-
8 subjects on inhaled steroids before removal had stopped treatment before final follow up, their median step-up was +67.5 ml;
-
19 subjects had a significant increase in inhaled steroids, their median step-up was −9 ml;
-
56 subjects had no major change in treatment, their median step-up was +45 ml;
-
In 31 subjects it was unclear whether significant changes in treatment occurred; 22 were known to be on inhaled corticosteroids before removal, median step-up was +13.5 ml;
-
9 were known not to be on inhaled corticosteroids before removal, median step-up +10 ml.
Mean annual change in FEV1 after removal from exposure
One hundred and thirty seven subjects had 684 FEV1 measurements after removal from exposure, although only 86 subjects had FEV1 measurements made over a period of at least 1 year (median 2.6 years, IQR 1.7–4.6), ignoring measurements made within the first 6 months following removal from exposure.
The mean (SE) rate of FEV1 decline after removal from exposure was 26.6 (18.0) ml/year. The rate of decline after removal from exposure was not related to duration of symptomatic exposure or to the latent interval between first exposure and first symptoms (p = 0.52 and p = 0.49, respectively), nor was it related to smoking status (current smokers 27.1 ml/year, ex-smokers 19.7 ml/year, never smokers 22.7 ml/year).
Comparison of FEV1 decline before removal and subsequent step-up in FEV1
There were 63 subjects with FEV1 measurements performed for at least 1 year before removal from exposure and in whom an FEV1 step-up could be calculated; their demographic characteristics are shown in table 2. The mean (SE) rate of change in FEV1 before removal was −111.6 (23.5) ml/year. The step-up in FEV1 1 year after removal was +57.7 (45.2) ml. Paired t tests showed a mean difference of 169.2 ml/year (95% CI 52 to 286), p = 0.005. This shows that there was a significant step-up in FEV1 following removal from exposure.
Comparison of decline in FEV1 before and after removal from exposure
Forty four subjects had FEV1 measurements made for at least 1 year before and 1 year after removal from exposure (excluding the first 6 months after removal); the demographic characteristics of these subjects are shown in table 2. The mean (SE) rate of change in FEV1 before removal was −119.8 (26.3) ml/year compared with +9.8 (31) ml/year after removal. Paired t tests showed a mean difference of −129.6 (95% CI of difference −217 to −42), p = 0.005. The rate of decline following removal from exposure was significantly less than during exposure.
DISCUSSION
We have shown that, in occupational asthma, FEV1 declines rapidly at a rate of about 100 ml/year while the worker is exposed to the causative agent in the workplace. According to the model of FEV1 used in this study, removal from exposure to the agent results in an uplift in FEV1 of about 12 ml in the first year, followed by a subsequent decline at a rate of 26 ml/year. The nature of the causative agent, current smoking, or treatment with inhaled corticosteroids did not appear to influence the rate of decline in FEV1.
The study population included all workers seen at the Birmingham Chest Clinic who were reported as having occupational asthma to SHIELD (the West Midlands reporting scheme) with a date of diagnosis between 1 January 1993 and 15 July 1999 and a positive PEF record. It is unclear how representative this group of workers is of all workers with occupational asthma. All respiratory physicians and most occupational physicians within the region regularly notify cases to SHIELD, and this would tend to reduce bias. Cases that are often missed include young people in whom occupational asthma develops quickly on starting a job (such as hairdressers) and who often leave soon after respiratory symptoms first occur without even consulting a doctor. Those who stay at work and are exposed are likely to be least affected. There may be a tendency for more severe cases to be referred and those from known high risk industries. The reported incidence of occupational asthma in the West Midlands region is the highest in the UK. This suggests that selection bias due to under-reporting is likely to be less in the West Midlands region than anywhere else in the UK.
The model of FEV1 decline used assumes three components: a decline in FEV1 while exposed followed by a step-up in FEV1 over a year, after which there is a decline in FEV1 , the rate of which may change. The rationale for choosing a 1 year period during which the step-up occurs is that data from snow crab workers suggested that maximal improvement in FEV1 occurred by about 1 year after removal from exposure.7 As the first follow up visit in this study was at 12 months after removal from exposure to the causative agent, it is possible that the plateau in FEV1 could have occurred much earlier than at 12 months. Our model assumes a definite time point at which significant exposure ceased. In practice, determining this point in time is subject to significant error. After the diagnosis and recommendations regarding removal from exposure have been made, there is often a period where there is reduced or intermittent exposure that can last for many years. There was a large degree of subjective input by the worker in determining the time point of significant removal from exposure, apart from those who lost their jobs, and faulty recollection of events is likely to increase error further. The exact time point chosen is likely to have a significant influence on all three components of the FEV1 decline model. Use of spirometric measures to support the choice of the time point that exposure ceased would bias the model, so this was avoided.
Simple regression analyses were used to provide individual estimates of the decline in FEV1 before and after removal from exposure. Intra-individual variability in spirometric measures tend to be large over short periods of time and accurate estimates of individual FEV1 decline require monitoring over long periods of time, preferably at least 5 years. Few subjects have measurements over this period of time, particularly with respect to the exposed period, and it was necessary to specify a shorter minimum period over which measurements were made. Although a shorter period would make individual estimates of FEV1 decline less reliable, group estimates should still to be reasonably reliable. A minimum of a 1 year period of spirometric measurements for determining the decline in FEV1 was felt to be a reasonable compromise in allowing inclusion of more subjects but, at the same time, trying to minimise the error of individual regression estimates. Inclusion of only subjects with longer periods of follow up would also introduce bias because of the “healthy survivor” effect—that is, the result would probably underestimate the true FEV1 decline of the group as a whole, as those with more severe disease and a rapid decline in FEV1 are more likely to have been removed from exposure and thus excluded from the analysis. FEV1 measurements made before the age of 25 years were not included in regression estimates for any individual as maximally attained lung function is not reached until about this age, hence a linear model is inappropriate.
Estimates of the decline in FEV1 after removal from exposure were even less reliable than during exposure. There are several possible reasons for this. Firstly, follow up tended to be less intensive after removal from exposure and there were fewer data points over any given period of time. Secondly, the model estimated a linear decline following the step-up period. It is likely that there is considerable intra-individual variation in the pattern of recovery that would make this model incorrect for many subjects. As there were fewer data points in the post-removal period, data points after 6 months removal from exposure were included in the regression estimates in order to minimise the standard error of the regression estimates. Assuming the step-up occurred in a non-linear manner, this would lead to a small underestimate in calculating the step-up value and possibly the post-removal regression slope.
There are several difficulties with using individual regression estimates to calculate the decline in FEV1 for the whole group. All the data are not used (such as in subjects with only one FEV1 measurement within an exposed or unexposed period), thus reducing the power of the analysis. Each regression coefficient is given equal weighting within the analysis, despite the fact that subjects who have more data points are likely to have less error in their estimates than those with fewer data points. There are other models that might overcome some of the disadvantages of simple regression estimates such as multilevel hierarchical linear models (mixed models). Unfortunately, they are also biased by weighting in favour of those who are exposed for longer (these subjects are likely to be less seriously affected).
For the group as a whole, the decline in FEV1 appeared to be very rapid during exposure in the workplace with a mean rate of decline of about 100 ml/year. The actual rates of decline have large confidence intervals and lack precision. With a standard error of 17.7, this means that, at best, this value is likely to be at least 65.5 ml/year which is a considerably faster rate of decline than that reported in non-occupational asthma,2 and at least as bad as that reported in chronic obstructive pulmonary disease.3 Potential confounders such as sex, age, and baseline FEV1 did not influence the rate of decline. Current smoking also had no effect, although ex-smokers had a significantly less rapid decline in FEV1, possibly related to ongoing benefits from having stopped smoking. The lack of effect of current smoking is perhaps not surprising, considering the relatively small additional influence this has on FEV1 decline in asthmatic subjects (an additional 9–14 ml/year in asthmatic men).8
There was a high degree of variability in the step-up in FEV1 but, among those in whom both a pre-removal decline and a step-up in FEV1 could be calculated, the step-up in the year after removal was significantly better than the prior rate of decline. The rate of change in FEV1 thereafter was significantly better than during exposure. In the small number of workers with pre-existing asthma, the pattern of FEV1 decline while exposed and following removal from exposure was not significantly different from in the rest of the study group (data not shown).
In conclusion, in this group of workers with occupational asthma, FEV1 declined rapidly at a rate of about 100 ml/year during exposure in the workplace. Removal from exposure was associated with a step-up in FEV1 of about 12 ml in the first year, following which FEV1 declined at a rate similar to healthy non-smoking adults.
Acknowledgments
The authors thank Sally Spencer for statistical advice.
Footnotes
-
Published Online First 2 May 2006
-
This project was funded by the European Chemical Industry Council (CEFIC). Dr Anees was also supported by a grant from the COLT Foundation.
-
Competing interests: none declared.