Article Text

Statistics from Altmetric.com
Non-invasive ventilation (NIV) is the treatment of choice for persistent hypercapnic ventilatory failure during acute exacerbations of chronic obstructive pulmonary disease (AECOPD), despite optimal medical treatment.1,2 Assessment of the partial arterial pressure of carbon dioxide (Paco2) is the “gold standard” for the evaluation of the adequacy of alveolar ventilation in this setting. However, repeated intermittent invasive arterial puncture carries inherent risks, including pain.3 Transcutaneous measurement of carbon dioxide (TcPco2) theoretically appears more appropriate for monitoring Paco2. This measurement is based on the observation that CO2 has a high tissue solubility and diffuses through the skin. While available data as to the precision of TcPco2 measurements have given conflicting results,4–6 no study has attempted to assess simultaneous recordings of TcPco2 and Paco2 in patients requiring NIV for AECOPD.
We prospectively studied the agreement between TcPco2 and Paco2 measurements in 22 consecutive patients with AECOPD admitted to the respiratory support unit (RSU) from the emergency department with persistent ventilatory failure (Paco2 ⩾6 kPa) requiring NIV treatment. Paired arterial blood gas samples taken from the radial artery and TcPco2 measurements were made on arrival in the RSU and 1 and 4 hours after commencing NIV. Patients were also given bronchodilators by nebuliser, corticosteroids, and antibiotics. Each subject gave their informed consent following a detailed presentation of the study objectives and protocol.
Thirteen women and nine men of mean (SD) age 72 (10) years and mean (SD) body weight 67 (13) kg were enrolled in the study. On arrival at the RSU, mean (SD) systolic blood pressure (BP) was 138 (33) mm Hg and diastolic BP was 70 (14) mm Hg. No patient received vasopressor or inotropic support. Arterial pH on arrival at the RSU was 7.27 (0.06). TcPco2 measurements were performed with a capnograph (Tosca Monitor; Linde Medical Sensors, Basel, Switzerland). The monitor measures TcPco2 using a Stow-Severinghaus electrode with a single ear sensor which works at 42°C to enhance blood flow in capillaries below the sensor. TcPco2 is measured by determining the pH of an electrolyte solution. The change in pH is proportional to the logarithm of the change in TcPco2. Reassembly of the sensor—which constitutes an electrolyte solution, a spacer, and a gas permeable Teflon membrane—has to be done every 14 days. The monitor displays when the sensor needs a new membrane. The system is equipped with an integrated unit for fully automatic calibration before measurements. In vitro response times are typically below 50 seconds.
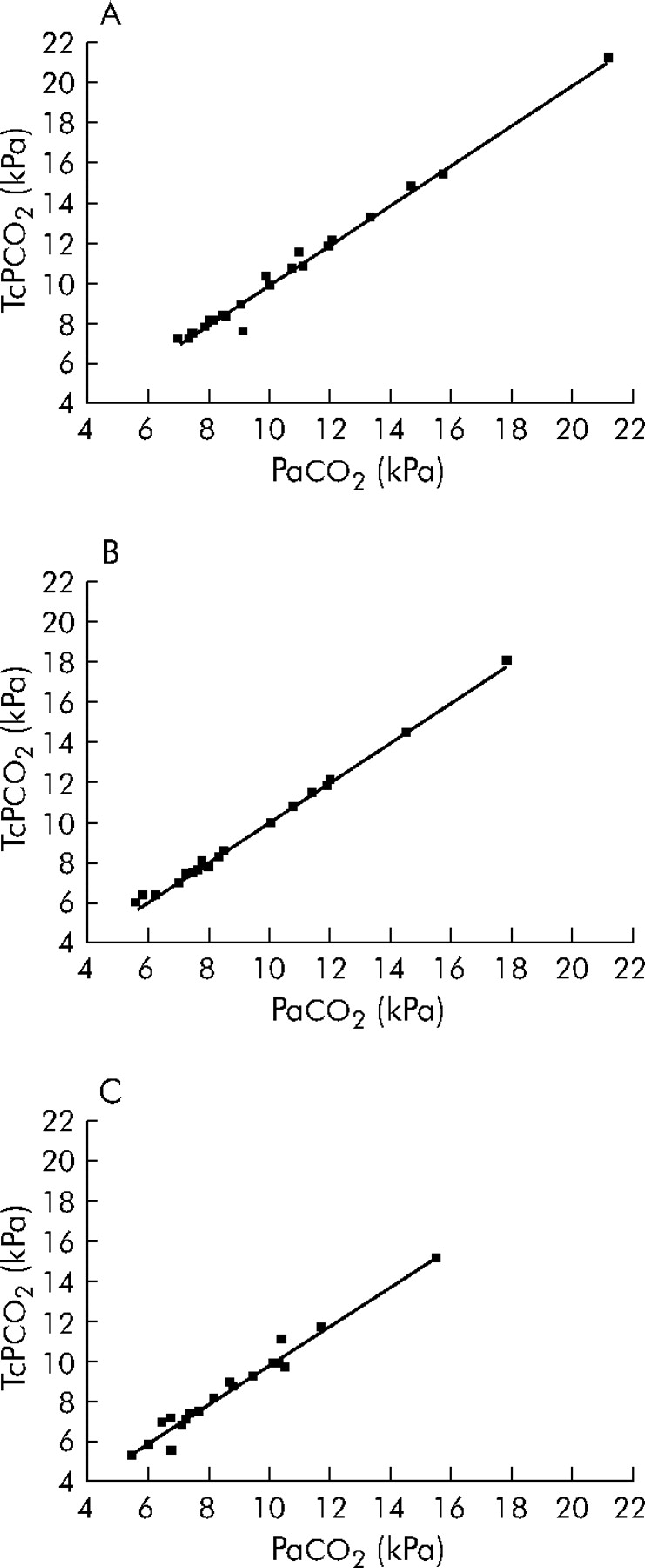
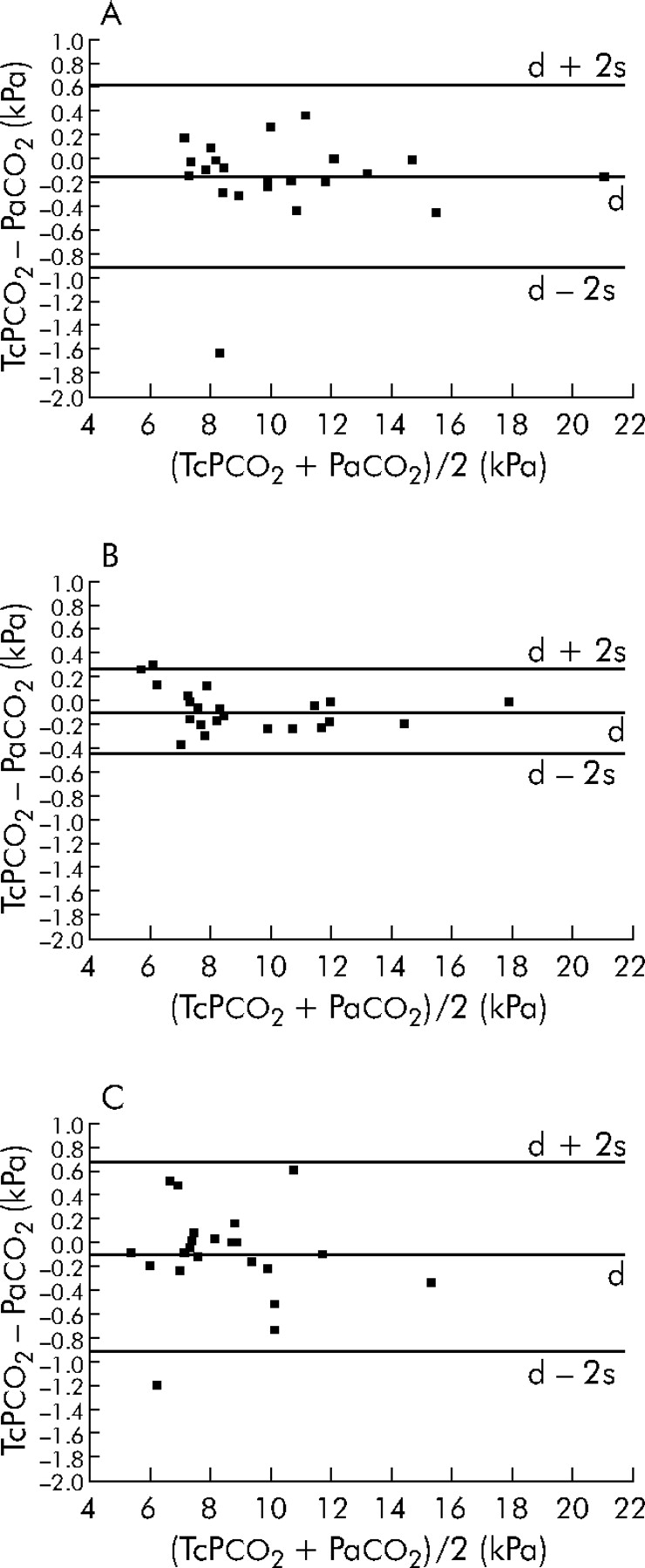
Agreement between transcutaneous and arterial values for CO2 was tested over a range of 5–22 kPa and calculated using Pearson’s coefficient of correlation. Both measurements were highly correlated on arrival in the RSU (r = 0.99, p<0.0001) and 1 hour (r = 0.99, p<0.0001) and 4 hours after commencing NIV (r = 0.98, p<0.0001; fig 1). However, in two of our measurements—interestingly, at a lower Paco2—the agreement was less strong. We also calculated the bias and the limits of agreement between the parameters as described by Bland and Altman;7 95% of the values were within the limits of agreement on arrival in the RSU and 1 and 4 hours after commencing NIV (fig 2). There were no adverse effects from or patient discomfort with the heating electrode.

Correlation between TcPco2 and Paco2 measurements in 22 subjects (A) on arrival in the RSU and (B) 1 hour and (C) 4 hours after commencing non-invasive ventilation for an acute exacerbation of COPD.

{kind=link}
{kind=link}
Bias of TcPco2 compared with Paco2 (d) and SD of bias (s) in 22 subjects (A) on arrival in the RSU and (B) 1 hour and (C) 4 hours after commencing non-invasive ventilation for an acute exacerbation of COPD. Values of (TcPco2 – Paco2) are plotted against the mean values of TcPco2 and Paco2 as described by Bland and Altman.7
These findings suggest that TcPco2 measurements are appropriate for clinical application in estimating the ventilatory response to NIV in patients with hypercapnic ventilatory failure due to AECOPD. However, a larger and more detailed study is needed to confirm these preliminary findings. TcPco2 measurements allow real time estimation of CO2 levels over a prolonged period and therefore facilitate proactive rather than reactive ventilator manipulations. Moreover, TcPco2 measurements may help in deciding the timing of arterial sampling and may therefore considerably reduce the frequency of painful invasive arterial sampling.
Footnotes
-
Competing interests: none declared.