Article Text

Statistics from Altmetric.com
Asthma has become a major health problem in Asia, with a prevalence in many Asian countries approaching that of developed nations. The regular use of inhaled corticosteroids (ICS) has been shown in cohort and ecological studies to decrease hospital admission rates by up to 80%.1,2 Asthma related mortality has also been shown to decline with ICS use, even at low doses.1,3,4 Conversely, increased use of short acting β2 agonists (SABA) has been associated with increased mortality.5 This study assessed the possible relationship between changes in the use of ICS and SABA and hospital admission and mortality rates for asthma in Singapore.
An ecological population based study was performed from 1994 to 2002 in patients aged 5–64 years. Figures on mortality and hospital admission rates for asthma were obtained from the Ministry of Health, Singapore. The diagnosis codes used were in accordance with the International Classification of Diseases–Clinical Modification, Ninth Revision (ICD-9: 493). Overall and age specific death rates were calculated for the 5–34 and 35–64 year age groups, and overall and age specific hospital admission rates were calculated for children aged 0–14 years and for those aged 15 years and older. Data on the sales of ICS and SABA were obtained from Intercontinental Medical Statistics (Asia) Pte Ltd and presented as canister counts. A Poisson regression analysis using the generalised linear model procedure in S-Plus Version 6 for Windows was carried out to estimate the association between the asthma health outcomes and sales of ICS and SABA.
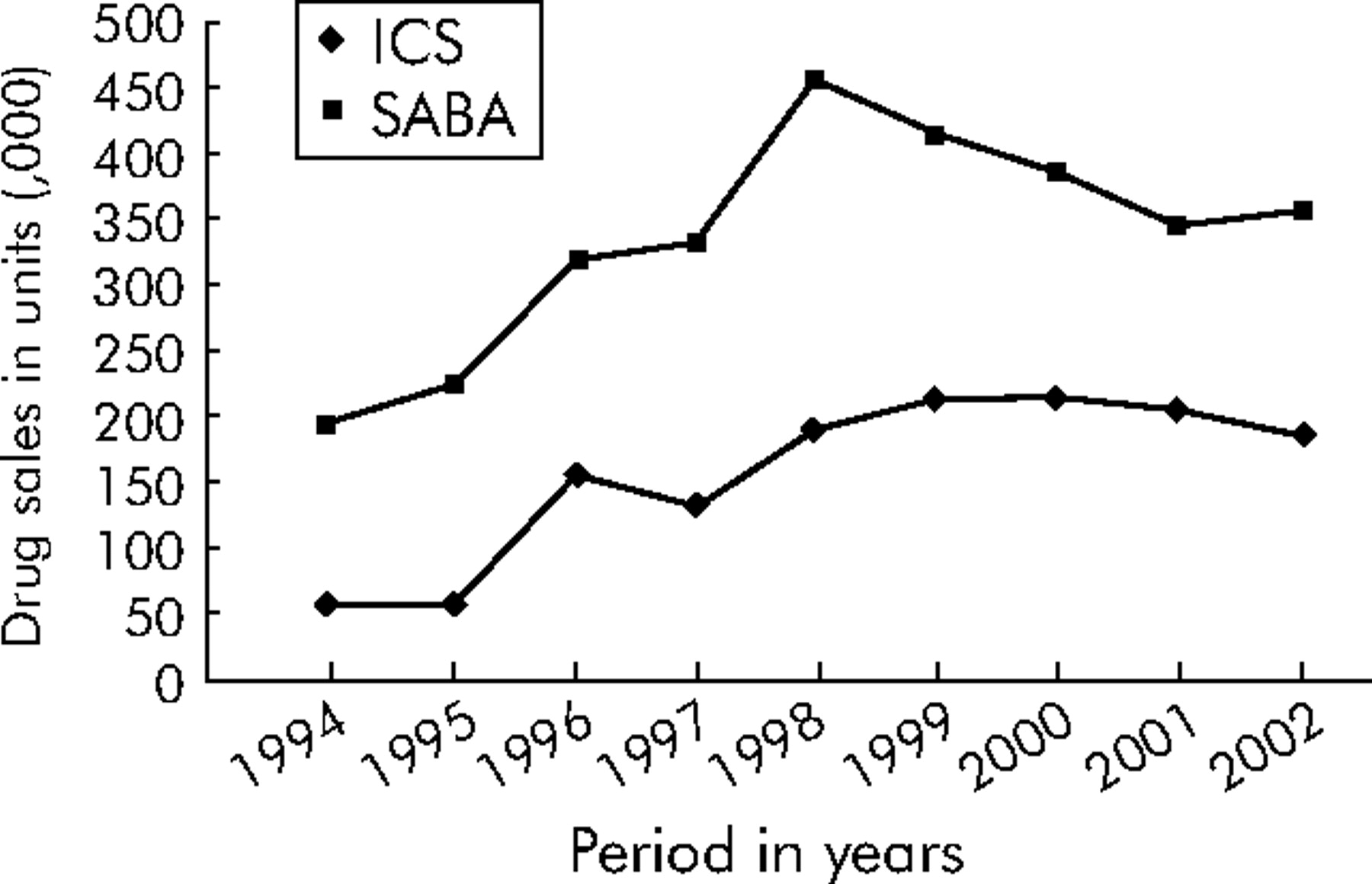
From 1994 to 2002 asthma deaths declined in both age groups (5–34 years and 35–64 years) by 52.5% and 56.7%, respectively. Throughout the study period the hospital admission rates for both age groups declined significantly (trend test: p<0.001 for 0–15 years and p = 0.001 for >15 years; fig 1). Rising trends for sales of ICS and SABA were observed (fig 2).

Age standardised mortality and hospital admission rates for asthma in Singapore from 1994 to 2002.
{kind=link}
{kind=link}
Annual drug sales in units (×103) in Singapore from 1994 to 2002.
The rates of asthma deaths and hospital admissions were also assessed by comparing the periods 1994–1997 (P1) and 1999–2002 (P2). The mean annual asthma mortality decreased significantly from 2.30 to 1.52 and from 0.66 to 0.44 per 100 000 population for those aged 5–64 years (p = 0.0003) and 5–34 years (p = 0.0348), respectively. Mean annual hospital admission rates also decreased substantially for all ages over the P1 and P2 periods, falling from 175.3 to 122.9 per 100 000 population (p<0.001). In parallel, a corresponding increase was observed in mean annual drug sales for ICS from 100.7 units (×103) in P1 to 204.3 units (×103) in P2 (p = 0.0003). The mean sales of SABA also increased but the change in usage was not statistically significant (p = 0.0507).
Poisson regression analysis confirmed the negative association between the use of ICS and both asthma mortality and hospital admission rates (p<0.05), with and without adjustment for the sales of SABA in all age groups (table 1). The association with the use of SABA was not significant in the same model. The rate ratios of asthma mortality for those aged 5–64 years and hospital admission for all ages were 0.96 (p = 0.0461) and 0.98 (p = 0.0006) for every 10 000 units of ICS sold after adjusting for the sales of SABA (model 2 in table 1).
Poisson regression analysis of asthma mortality and hospitalizations by age group, associated with the sales of ICS and SABA*
Being an ecological study, we recognise that other factors such as improvements in patient education and medical facilities may also have contributed to the observed improvement in morbidity and mortality. Despite this, the data presented here support the current evidence that an overall increase in ICS use has a positive impact on asthma related morbidity and mortality in our population, and highlight the importance of ICS prophylaxis as the most cost effective form of asthma treatment available today.
Footnotes
-
The authors thank Intercontinental Medical Statistics (Asia) Pte Ltd for providing data on sales of asthma medications in Singapore.
-
Competing interests: none declared.