Article Text

Abstract
Background: Addition of the long acting β2 agonist salmeterol to inhaled corticosteroids leads to better symptomatic asthma control than increasing the dose of inhaled corticosteroids. However, little is known about the long term effects of adding salmeterol on the asthmatic inflammatory process, control of which is considered important for the long term outcome of asthma.
Methods: After a 4 week fluticasone run-in period, 54 patients with allergic asthma were randomised to receive twice daily treatment with fluticasone 250 μg with or without salmeterol 50 μg for 1 year in a double blind, parallel group design (total daily dose of fluticasone 500 μg in both treatment groups). Primary outcomes were sputum eosinophil numbers and eosinophil cationic protein concentrations. Secondary outcomes were neutrophil associated sputum parameters and a respiratory membrane permeability marker. The effects on allergen induced changes were determined before and at the end of the treatment period.
Results: Adding salmeterol to fluticasone resulted in improved peak expiratory flow, symptom scores, rescue medication usage, and bronchial hyperresponsiveness (p<0.05 for all). There was no sustained effect on sputum cell differential counts and cytokine concentrations during the treatment period or on changes induced by allergen challenge at the end of treatment (p>0.05). However, adding salmeterol significantly reduced sputum ratios of α2-macroglobulin and albumin during the treatment period (p = 0.001).
Conclusions: The addition of salmeterol to fluticasone produces no sustained effect on allergen induced cellular bronchial inflammation but leads to a significant improvement in size selectivity of plasma protein permeation across the respiratory membrane. This may contribute to the improved clinical outcome seen in patients with allergic asthma when a long acting β2 agonist is combined with inhaled corticosteroids.
- ECP, eosinophil cationic protein
- FEV1, forced expiratory volume in 1 second
- IL, interleukin
- MPO, myeloperoxidase
- PC20histamine, concentration of histamine provoking a fall in FEV1 of at least 20%
- RCEs, relative coefficient of excretion in induced sputum
- asthma
- inflammation
- sputum
- bronchodilator agents
- anti-inflammatory agents
Statistics from Altmetric.com
- ECP, eosinophil cationic protein
- FEV1, forced expiratory volume in 1 second
- IL, interleukin
- MPO, myeloperoxidase
- PC20histamine, concentration of histamine provoking a fall in FEV1 of at least 20%
- RCEs, relative coefficient of excretion in induced sputum
Allergic asthma is currently considered primarily a chronic inflammatory disorder and repeated exposure to allergens may be important in the persistence of the disease.1 Other than avoiding exposure to risk factors, the use of inhaled corticosteroids is considered to be the mainstay for the treatment of allergic asthma.1 Regular use of inhaled corticosteroids in asthma is associated with prolonged improvement in exacerbation frequencies, symptom scores and lung function, as well as with a reduction in inflammatory cells in the airways.2,3 By contrast, β2 agonists are principally regarded as bronchodilators and are advised to be used only in combination with anti-inflammatory treatment, except when used intermittently for the mildest form of asthma.1
Several large clinical studies have now shown that adding a long acting β2 agonist to inhaled corticosteroids leads to better symptomatic asthma control and lower exacerbation frequencies than increasing the dose of inhaled steroids.3,4 These findings suggest that adding a long acting β2 agonist to inhaled corticosteroids exerts beneficial effects beyond smooth muscle relaxation. In vitro studies have also indicated a synergistic effect of combining long acting β2 agonists and corticosteroids.5 Some short term clinical studies suggest an anti-inflammatory effect since lower numbers of EG1+ eosinophils and submucosal mast cells were found after adding salmeterol for 12 weeks.6,7 As a consequence, it has been proposed that the addition of a long acting β2 agonist influences the underlying inflammatory process. In contrast, a recent study of bronchial biopsy specimens showed no additional anti-inflammatory effect of adding formeterol to low dose budesonide during 16 weeks of treatment.8 It should be emphasised that the long term clinical studies on adding salmeterol to inhaled corticosteroids were limited to clinical outcomes3,4 and did not evaluate bronchial hyperresponsiveness or surrogate inflammatory biomarkers such as airway eosinophils. These in turn are considered to be the ultimate driving force behind symptoms, the disability of asthma and, most importantly, the long term sequelae such as airway remodelling.9,10 End points such as symptoms and lung function may favour the use of long acting β2 agonists but provide little information about the pathophysiological features of the asthmatic inflammatory process.11 In addition, there are indications that the regular use of short acting β2 agonists has pro-inflammatory effects;12,13 this has led to concerns that adding a long acting β2 agonist could lead to clinical masking of bronchial inflammation.14
A long term randomised clinical trial was performed to investigate whether the improved clinical outcomes resulting from adding salmeterol to fluticasone are accompanied by a prolonged effect on the underlying bronchial inflammatory process in asthma. After a run-in period with fluticasone 250 μg twice daily, 54 patients with mild to moderate persistent allergic asthma were randomised to receive twice daily treatment with either fluticasone (250 μg) or fluticasone/salmeterol (250/50 μg) for 1 year. In addition, bronchial allergen challenges were performed 1 day before randomisation and at the end of the randomised treatment period to investigate the effect on allergen induced bronchial inflammation of maintenance treatment with fluticasone/salmeterol versus fluticasone. Primary outcomes were sputum eosinophil numbers and eosinophil cationic protein (ECP) concentrations. Secondary outcomes were serum levels of interleukin (IL)-5, size selectivity of the respiratory membrane as measured by the ratio of sputum α2-macroglobulin to albumin, sputum neutrophil numbers, IL-8, and myeloperoxidase (MPO). In addition, we measured lung function parameters, peak expiratory flows, symptom scores, and rescue medication usage. The overall differences in outcome parameters over the 1 year treatment period were analysed, as well as differences in allergen induced changes between the two treatment groups.
METHODS
An extended version of the Methods section is available in the online data supplement at http://www.thoraxjnl.com/supplemental.
Study participants
Non-smoking patients with mild to moderate persistent allergic asthma were enrolled. The participating patients were recruited via advertisements and from the Outpatient Department of Pulmonology at the Academic Medical Center (AMC). The study was approved by the institutional ethics and research committees and all subjects gave written informed consent.
Study design
The study was of a double blind, randomised, two armed parallel design (fig 1). After a 2 week steroid washout period, a 4 week run-in period with fluticasone 250 μg twice daily, and a baseline bronchial allergen challenge, eligible patients were randomised to receive twice daily treatment with either fluticasone (250 μg) or fluticasone in a combination inhaler with salmeterol (250/50 μg) for 1 year. Patients were provided with rescue salbutamol 200 μg (GlaxoSmithKline, Zeist, The Netherlands). All drugs were administered via a dry powder inhaler (Diskus).

Study schedule. After a 2 week steroid washout period and a 4 week run-in period with fluticasone 250 μg twice daily, eligible asthma patients were randomised to receive twice daily treatment with fluticasone (250 μg) with or without salmeterol (50 μg) for 1 year. Baseline values were determined at the end of the run-in period. Bronchial allergen challenges were performed the day before randomisation and at the end of the randomised treatment period. Primary and secondary outcomes were measured after washout, before randomisation, at 1, 6, 9, and 12 months of randomisation, as well as 24 hours before and 24 hours after the bronchial allergen challenges (depicted by asterisks).
Outcome measures
Primary outcomes were sputum eosinophil numbers and eosinophil cationic protein concentrations. Secondary outcomes were neutrophil associated sputum parameters and a respiratory membrane permeability marker. In addition, lung function parameters, peak expiratory flows, symptom scores, and rescue medication usage were measured throughout the study. At the start of the washout period a full medical history, physical examination and forced expiratory volume in 1 second (FEV1) were performed. Baseline values of lung function parameters as well as primary and secondary outcomes were measured at the end of the run-in period (time point 0 months). In addition, outcomes were measured after washout and at 1, 3, 6, 9, 11 and 12 months during the randomised treatment period. Furthermore, outcomes were determined 24 hours before and 24 hours after bronchial allergen challenges which were performed at the end of the run-in period (pre-randomisation challenge) and at the end of the randomised treatment period (end of treatment challenge) (fig 1). Two week daily dairy cards, completed before and throughout the randomised treatment period, included peak expiratory flows, symptom scores, and rescue salbutamol usage. Before every visit patients abstained from rescue salbutamol for 8 hours and from the study medication for 12 hours except at 11 months of randomisation (abstaining from study medication for 36 hours).
FEV1 and the concentration of histamine provoking a fall in FEV1 of at least 20% (PC20histamine) were measured according to guidelines.15 Standardised allergen extracts were used for the allergen challenges which were performed as described by Sterk et al15 with modifications. A single dose of allergen was administered containing 100 biological units and was preceded by the inhalation of nebulised salbutamol. Levels of total and specific IgE were determined in the serum.16 Sputum induction and processing of whole sputum samples were performed as described elsewhere.17 Differential cell counts were expressed as number and percentage of cells excluding squamous epithelial cells. Sputum samples containing more than 80% squamous cells on differential cell counting were excluded from analysis. Levels of ECP,18 myeloperoxidase MPO,19 and IL-820 were measured in sputum and levels of IL-5 in serum.21 Size selectivity of the respiratory membrane was analysed by measuring the relative coefficient of excretion in induced sputum (RCEs), which is the ratio of sputum concentrations of α2-macroglobulin to albumin.17,22
Analysis of data
Statistical analyses were performed using SAS Version 8.2 (SAS Institute Inc, Cary, NC, USA). The study was designed to have 80% power to be able to detect a 50% difference in geometric means of the primary outcomes between the groups with a sample size of 54 subjects. Changes over the run-in period were determined using the Wilcoxon signed ranks test or, in cases of normally distributed data, the t test. Differences within and between the treatment groups were determined using mixed model ANOVA adjusted for differences at baseline. Differences in allergen induced changes were determined using ANCOVA and adjusted for baseline allergen induced changes. All p values are two tailed and levels <0.05 were considered significant.
RESULTS
Patients
Sixty patients agreed to participate in the study. Four did not fulfill the inclusion criteria after the run-in period and two withdrew during the run-in period for personal reasons, so 54 were randomised to receive one of the two treatment regimens. Patient characteristics, including age, dose of inhaled corticosteroids prior to the study and lung function parameters, were not significantly different between the treatment groups at baseline (end of run-in) (table 1).
Characteristics of study patients
Four patients in the fluticasone group failed to complete the study. Two of these patients withdrew 1 month after randomisation, one because of worsening of asthma symptoms and one was lost to follow up. The other two patients withdrew after 6 and 9 months of treatment, respectively, because of personal reasons. All patients in the fluticasone/salmeterol group completed the study.
Run-in period
FEV1 and PC20histamine improved significantly over the run-in period which was preceded by a steroid washout period (p<0.001, table 1). Mean peak expiratory flow rates, asthma symptom scores, and short acting β2 agonist usage recorded during the 2 weeks preceding the end of run-in visit (baseline) are shown in table 1. Levels of the inflammatory parameters before and after the run-in period are shown in table 2.
Inflammatory parameters at start and end of the run-in period
Randomised treatment period
Lung function
Morning and evening peak expiratory flows, asthma symptom scores, and short acting β2 agonist usage were significantly improved throughout the randomised treatment period in the fluticasone/salmeterol group compared with the fluticasone group (table 3, fig 2).
Mean differences in clinical and lung function parameters in the fluticasone/salmeterol (FP/S) group compared with the fluticasone (FP) group over the 1 year treatment period

(A) Morning peak expiratory flow rate and (B) short acting β2 agonist usage. Values are mean (SE). There were significant differences in morning peak flow recordings and short acting β2 agonist usage between the two treatment groups (p<0.01).
In the fluticasone/salmeterol group there was a trend for a higher FEV1 (table 3). PC20histamine was significantly higher in the fluticasone/salmeterol group over the 1 year treatment period measured on visits after abstaining for 12 hours from the study medication (table 3), but there was no significant difference in PC20histamine at the visit after 11 months of randomisation when patients abstained from the study medication for 36 hours (geometric mean (SE) baseline adjusted PC20histamine 1.6 (1.2) mg/ml in fluticasone group v 1.9 (1.3) mg/ml in fluticasone/salmeterol group, p = 0.53). There were no differences in numbers or severity of exacerbations between the two treatment groups (results not shown).
Sputum eosinophils and ECP
The geometric mean number of eosinophils in the fluticasone/salmeterol group expressed as percentage difference from that in the fluticasone group varied significantly between visits (p = 0.019). After 1 month of randomised treatment the number of sputum eosinophils in the fluticasone/salmeterol group was −71% (95% CI −92 to −1.2) compared with the fluticasone group (p = 0.048, fig 3). However, at other time points there was no significant difference between the groups (6 months: 56% (95% CI −71 to 741); 9 months −0.14% (95% CI −77 to 335), 12 months: 61% (95% CI −43 to 358)). Overall, during the 1 year treatment period there were no significant differences between the two treatment groups in either numbers or percentages of sputum eosinophils (p = 0.72 and p = 0.85, respectively, fig 3). The geometric mean ECP level in the fluticasone/salmeterol group was 5.7% lower than in the fluticasone group (p = 0.88). There were no indications that the difference varied between visits (p = 0.73). The 95% CI of the difference was −57% to +108%, indicating that the true geometric mean ECP concentration in the fluticasone/salmeterol group should have been more than 57% lower than in the fluticasone group to be detected as significant, given the results of the study.
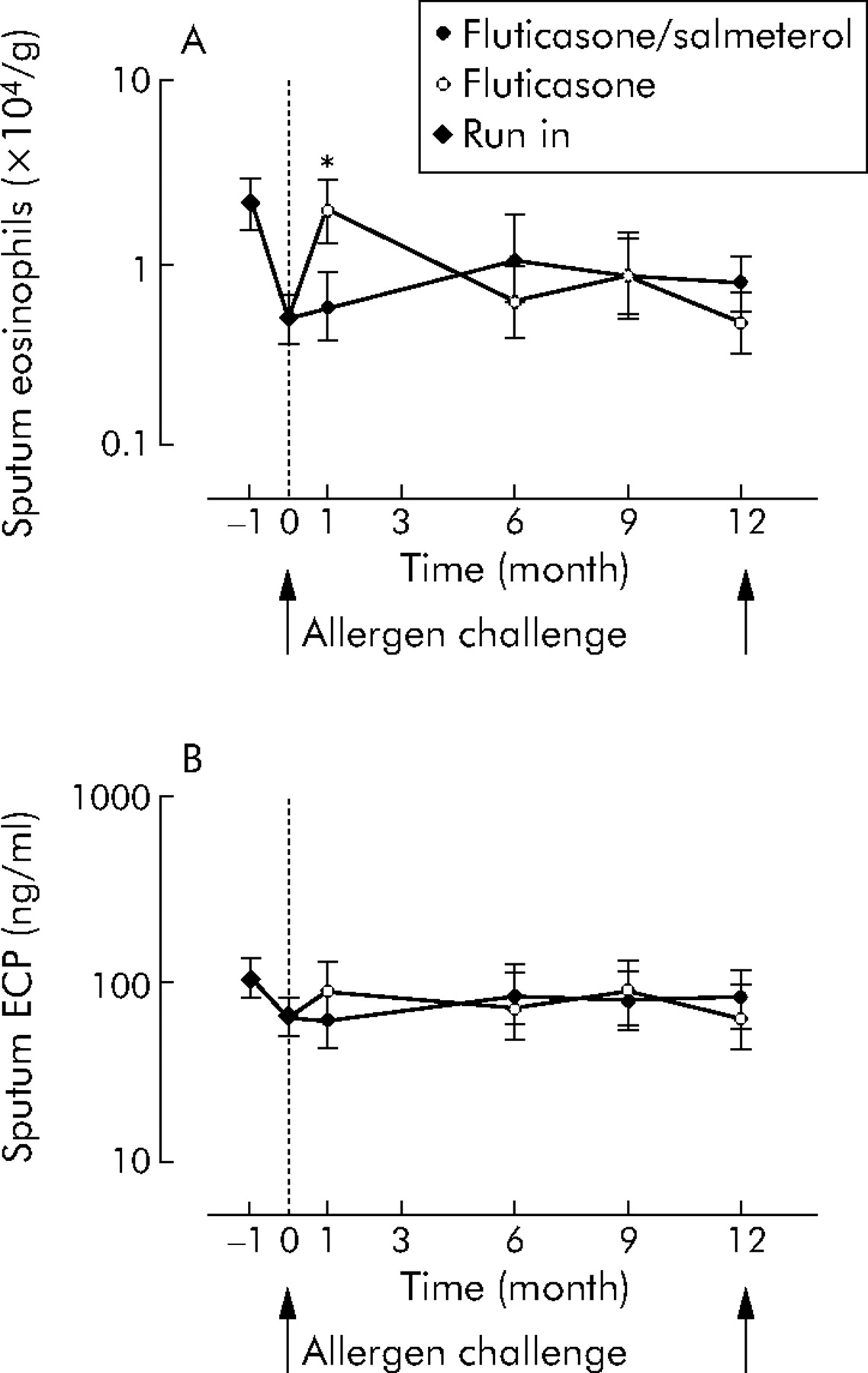
(A) Number of sputum eosinophils and (B) sputum eosinophil cationic protein (ECP) concentration. Baseline adjusted geometric mean (SE) values are shown. Overall, during the 1 year treatment period there were no significant differences between the two treatment groups in the number of sputum eosinophils or in the sputum ECP concentration (p = 0.72 and p = 0.88, respectively).
Sputum neutrophils, IL-8, MPO and serum IL-5
Sputum neutrophil numbers, sputum IL-8, sputum MPO, and serum IL-5 were not significantly different between the two treatment groups throughout the randomised treatment period (p = 0.16, 0.87, 0.70 and 0.23 respectively, data not shown).
Size selectivity of the respiratory membrane: relative coefficient of excretion (RCEs)
Overall, during the 1 year treatment period the RCEs was significantly lower in the fluticasone/salmeterol group than in the fluticasone group (p = 0.001, fig 4).

Relative coefficient of excretion (RCEs) during the run-in and the randomised treatment period. Baseline adjusted geometric mean (SE) values are shown. During the run-in period there was a significant decrease in the RCEs (p = 0.006). Overall, during the 1 year treatment period, the RCEs was significantly lower in the fluticasone/salmeterol group than in the fluticasone group (p = 0.001). The relative coefficient of excretion is the ratio of α2-macroglobulin to albumin in induced sputum.
Effect of adding salmeterol on allergen induced changes in bronchial inflammation
There were no significant differences between the treatment groups in the change in FEV1 after the allergen challenges, which were preceded by the inhalation of salbutamol (p = 0.81).
Sputum eosinophils and ECP
Sputum eosinophils (fig 5) and ECP concentrations increased significantly after the pre-randomisation allergen challenge as well as after the end of treatment allergen challenge (table 4).
Allergen induced increase in inflammatory parameters

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Numbers of sputum eosinophils before and after bronchial allergen challenges (A) before randomisation and (B) at the end of treatment. Geometric mean numbers of sputum eosinophils increased significantly after both the pre-randomisation and the end of treatment allergen challenge. There was no significant difference between the two treatment groups between the increases in sputum eosinophils after the end of treatment allergen challenge (p = 0.33).
There was a trend for a smaller increase in the percentage of sputum eosinophils in the fluticasone/salmeterol group after the end of treatment allergen challenge (p = 0.09), but there were no significant differences between the two treatment groups after the end of treatment allergen challenge in the changes in numbers of sputum eosinophils and ECP concentrations (table 4).
Sputum neutrophils, IL-8, MPO and serum IL-5
The number of sputum neutrophils, sputum IL-8, sputum MPO, and serum IL-5 increased after the pre-randomisation allergen challenge (p<0.001, 0.001, 0.005 and <0.001, respectively) as well as after the end of treatment allergen challenge (p = 0.02, 0.06, 0.02, and 0.02, respectively, data not shown). There were no significant differences between the two treatment groups in the changes in these parameters after the end of treatment allergen challenge (p = 0.92, 0.85, 0.93 and 0.89, respectively, data not shown).
Size selectivity of the respiratory membrane: relative coefficient of excretion (RCEs)
There was no significant difference between the two treatment groups in the changes in the RCEs after the end of treatment allergen challenge (p = 0.15, table 4). Likewise, there were no significant differences between the two treatment groups in the changes in sputum α2-macroglobulin or albumin after the end of treatment allergen challenge (table 4).
DISCUSSION
This is the first randomised clinical trial to investigate over a 1 year treatment period whether the improved clinical outcomes resulting from adding salmeterol to fluticasone are accompanied by an additional effect on bronchial inflammation. In agreement with earlier studies, peak expiratory flows, symptom scores, rescue medication usage, and bronchial hyperresponsiveness were significantly improved in the fluticasone/salmeterol group relative to the fluticasone group. Similar levels of sputum eosinophils, sputum ECP, sputum IL-8, sputum MPO, and serum IL-5 were found in both groups throughout the treatment period as well as after the bronchial allergen challenges. However, we did find significantly reduced ratios of sputum α2-macroglobulin and albumin in the fluticasone/salmeterol group relative to the fluticasone group. This secondary outcome, the relative coefficient of excretion (RCEs), was chosen as a marker of size selectivity of plasma protein permeation across the respiratory membrane.
The lack of a sustained effect of adding salmeterol on cellular bronchial inflammation, as found in induced sputum, is in agreement with a recent study by Overbeek et al8 who failed to show an additional anti-inflammatory effect in bronchial biopsy specimens of adding formeterol to low doses of budesonide during 16 weeks of treatment. Earlier in vitro23,24 and short term in vivo studies6,7 did report an initial anti-inflammatory effect which may be in line with our observation of a transient decrease in the number of sputum eosinophils 1 month after randomisation in the fluticasone/salmeterol group. This difference in sputum eosinophils at 1 month after the pre-randomisation allergen challenge may be explained by a slower recovery from the allergen induced increase in bronchial inflammation in the fluticasone group. Bronchial allergen challenge increases levels of inflammatory markers,25 which may increase the sensitivity to detect differences in levels of inflammatory markers between the treatment groups. On the other hand, it should be noted that the medium to high daily dose of fluticasone resulted in relatively low baseline levels of the inflammatory parameters. This may have obscured a modest long term anti-inflammatory effect on cellular bronchial inflammation of adding salmeterol. The study was powered to detect a 50% difference in primary outcomes (sputum eosinophils and ECP) between the groups, since such a difference was considered to be clinically relevant. Therefore, adding salmeterol to an inhaled corticosteroid under the conditions chosen neither causes a clinically relevant deleterious or masking long term effect on cellular bronchial inflammation nor significantly improves it. It should be emphasised that this finding may be unique to the administration of the combination product of salmeterol and fluticasone as patients may be tempted to leave off the latter when using both medications separately. It was reported previously that reducing the dose of inhaled corticosteroids in patients on salmeterol can mask increasing inflammation and delay awareness of worsening asthma.14
With respect to the effects on allergen induced bronchial inflammation, it should be stressed that patients abstained from the study medication for 12 hours before every visit, including the allergen challenge visits. This may have obscured an acute effect of adding salmeterol to fluticasone, but the aim of the study was to investigate the long term rather than the acute effects of fluticasone/salmeterol versus fluticasone on allergen induced bronchial inflammation. We, like others, have found indications in vivo for an acute short term anti-inflammatory effect of the addition of salmeterol to inhaled corticosteroids in a bronchial allergen challenge model.26
A concomitant characteristic of the bronchial cellular inflammatory process is the presence of increased permeability of the respiratory membrane.27 In healthy subjects the permeation of large plasma proteins is restricted, but during inflammation there is an apparent loss of size selectivity of the respiratory membrane.22 This will affect the sputum concentration of large plasma proteins more than of smaller proteins. The ratio of sputum levels of a large plasma protein (α2-macroglobulin) to levels of a smaller plasma protein (albumin) is considered a marker of size selectivity of the barrier between the blood and the airway lumen.13 We particularly chose this ratio since it is not influenced by variable dilution of sputum samples. Over the run-in period, when all patients received fluticasone 250 μg twice daily, we found a significant decrease in the RCEs. This finding is in keeping with an earlier study.13 Moreover, we found a continued decrease in the RCEs in the fluticasone/salmeterol group throughout the randomised treatment period, whereas the RCEs stabilised in the fluticasone group. This finding may point to increased size selectivity of the respiratory membrane caused by adding salmeterol. This is in keeping with earlier studies showing anti-exudative short term effects of long acting β2 agonists in animal28,29 as well as in human models.30 Such an anti-exudative effect may be desirable in the treatment of asthma, since the extravasated plasma contains potent adhesive and leucocyte activating proteins (such as fibrinogen and fibronectin) and inflammatory peptides including bradykinins and complement factors.31 However, analysis of the sputum concentrations of the individual serum proteins suggested an increase in albumin rather than a decrease in α2-macroglobulin in the fluticasone/salmeterol arm throughout the randomised treatment period. This might be explained by increased water clearance by salmeterol, which has been shown in animal models,32,33 in addition to increased size selectivity. An alternative explanation for the decrease in RCEs may be provided by the occurrence of selective transport of serum albumin to the airway lumen. In vitro, active transport of albumin across the ferret trachea has been reported which was increased by the short acting β2 agonist salbutamol.34 Moreover, specific serum albumin binding proteins have been identified.35 The role of albumin in the airway secretions is at present unclear. There is evidence that albumin may bind various mediators such as leukotrienes36 and may therefore render potentially active luminal agents less effective. Albumin may also act as a luminal antioxidant, preventing the formation of oxygen free radicals.37 In this respect, increased levels of albumin in sputum may have physiological advantages.
In summary, we have shown that improved clinical outcomes resulting from adding a long acting β2 agonist to maintenance treatment with inhaled corticosteroids are accompanied by similar levels of markers of chronic as well as allergen induced cellular bronchial inflammation. However, size selectivity of plasma protein permeation across the respiratory membrane appeared to be significantly improved by adding salmeterol to fluticasone, and this may contribute to the improved clinical outcomes seen.
Acknowledgments
The authors thank Barbara Smids-Dierdorp, Tamara Dekker, and Marianne van de Pol for their work on the inflammatory parameters in this study.
REFERENCES
Supplementary materials
Files in this Data Supplement:
- view PDF - Online Data Supplement.
Footnotes
-
Published Online First 31 January 2006
-
This study was supported by a grant from GlaxoSmithKline.
-
The Department of Pulmonology and Laboratory of Experimental Immunology, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands receive research grants from GlaxoSmithKline, Numico and AstraZeneca for performing trials. The author and co-authors of this manuscript have no financial relationship with a commercial entity that has an interest in the subject of this manuscript.