Article Text

Statistics from Altmetric.com
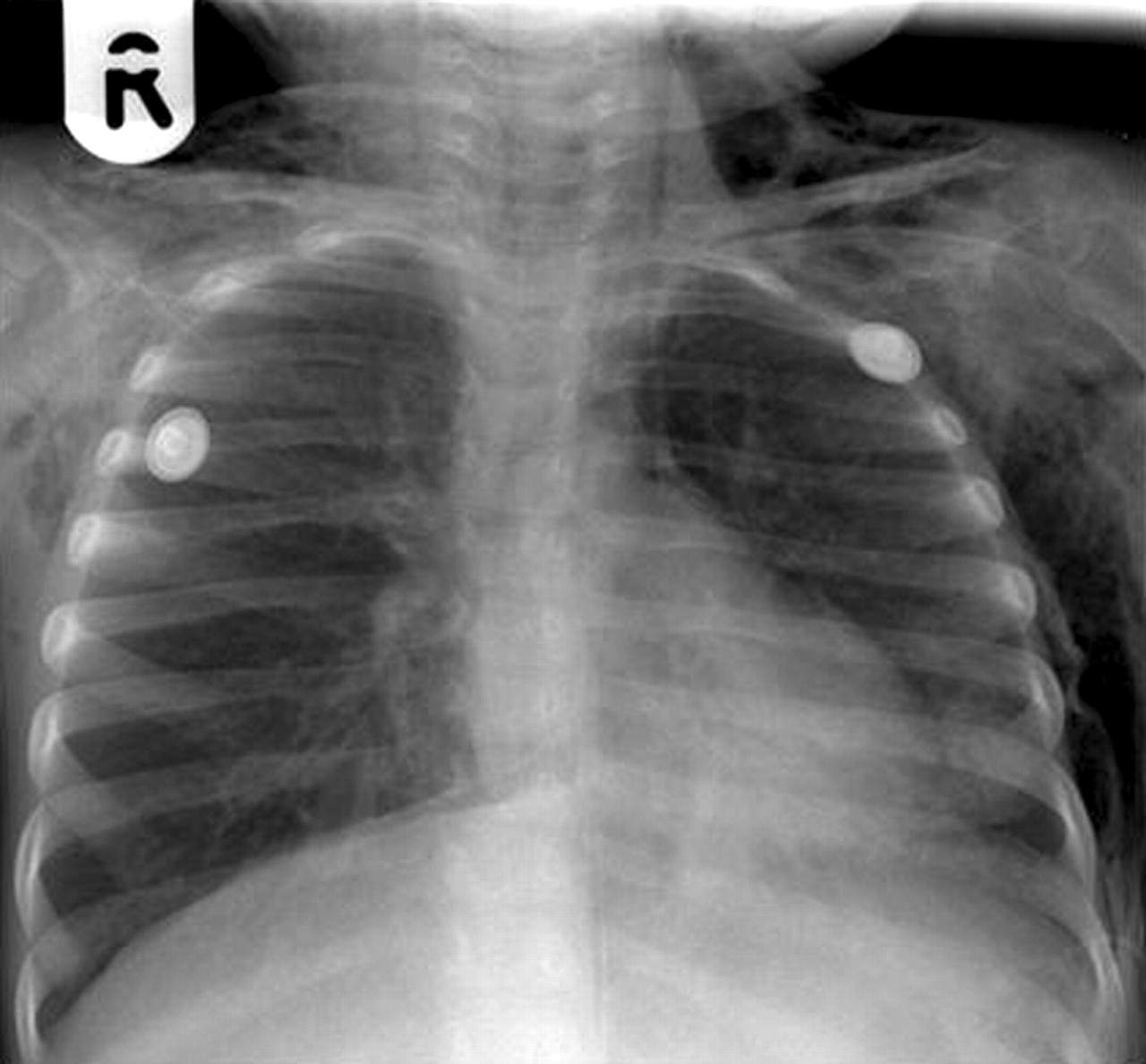
A 2 year old girl undergoing investigation for recurrent respiratory infections and failure to thrive presented acutely with neck and face swelling, tongue protrusion, and extreme difficulty in breathing. Examination showed extensive surgical emphysema over her chest, neck and face confirmed on the chest radiograph, which also revealed a pneumomediastinum (fig 1). While being prepared for emergency intubation the symptoms began to resolve, allowing her to be managed conservatively without ventilation or chest drains. A CT scan (fig 2) showed a moderate anterior pneumomediastinum (thin arrow) without a pneumothorax in addition to some bronchial wall thickening (bold arrow) but no bronchiectasis. Culture of bronchoalveolar lavage fluid was negative (while on broad spectrum antibiotics), but she has since been diagnosed with cystic fibrosis (CF) on the basis of sweat testing and genetic analysis.

Chest radiograph showing extensive surgical emphysema throughout the chest wall and free air within the mediastinal space.

{kind=link}
{kind=link}
CT scan of the chest performed several days after the initial presentation which confirms persistent surgical emphysema and a moderate pneumomediastinum (thin arrow). There is also some bronchial wall thickening (thick arrow) but no evidence of bronchiectasis.
Such air leaks, while not uncommon in advanced CF,1 are extremely rare in young children, the youngest in the literature being aged 4 years.2 The pneumomedistinum in this child was presumably caused by transient peaks in alveolar pressure related to a combination of coughing, airway wall inflammation, and mucus plugging. The avoidance of positive pressure ventilation was probably a contributing factor in her rapid recovery.
Learning points
-
Any cause of severe cough or small airway obstruction may have the potential to cause air leakage.
-
Cystic fibrosis may present acutely with air leakage.
Footnotes
-
Competing interests: none declared.