Article Text

Statistics from Altmetric.com
Clinical topics in lung cancer
P1 SYMPTOMS IN LUNG CANCER: DO THEY HELP THE DIAGNOSIS?
S. Bari, D. A. Stock, A. McIver, C. M. Smyth, M. J. Walshaw, M. J. Ledson. Liverpool Lung Cancer Unit, The Cardio Thoracic Centre, Liverpool UK
Background: Many patients with lung cancer present late, limiting the treatment options and their ultimate survival. Although there is no consensus as to whether specific symptoms aid diagnosis, a recent study (
) suggested that encouraging patients to present early with symptoms might expedite management. To investigate the role of symptoms in the diagnosis of lung cancer further, we looked at a cohort of patients undergoing bronchoscopy for suspected lung cancer who had presented to our large lung cancer unit over a five year period.
Methods: Our lung cancer unit diagnoses up to 400 patients per year, and we have kept a database of 3327 patients (1713 (51%) with lung cancer) presenting with paracancer symptoms since 2000. From this, we age and sex matched 616 cancer patients (mean age 74.5 years, 337 male) with 616 (74.2 years, 341 male) who also presented to the unit with suspected lung cancer and underwent bronchoscopy but subsequently had a non-cancer diagnosis. One hundred and thirty one lung cancer patients (21%) and 153 non-lung cancer patients (25%) had chronic obstructive pulmonary disease (COPD). Using χ2 tests, we compared common presenting symptoms which may be associated with lung cancer between the two groups.
Results: Chest pain (χ2 = 94, p<0.001), weight loss (χ2 = 43, p<0.001), breathlessness (χ2 = 4.5, p<0.05), voice change (χ2 = 6.4, p<0.025), stridor (χ2 = 7.3, p<0.001), and loss of appetite (χ2 = 49, p<0.001) were more common in the lung cancer group, whereas haemoptysis (χ2 = 7.5, p<0.01), back pain (χ2 = 19, p<0.001), fever (χ2 = 7.3, p<0.01), and night sweats (χ2 = 8.1, p<0.01) were more common in the non-lung cancer group. Cough, wheeze, and other types of pain were equally common in both groups.
Conclusion: Although several symptoms were more common in the group with a subsequent diagnosis of lung cancer, other than stridor (which was only present in 10 cases) none of these were disease specific and might merely reflect the increased respiratory morbidity expected in an older population of at risk individuals. As all these patients underwent bronchoscopy, the increased frequency of other symptoms suggesting infection in the non-lung cancer patients might explain the otherwise unexpected finding of increased haemoptysis in this group. This study from a large cohort of patients confirms that many patients with lung cancer present with non-specific symptoms. Hence, rapid referral and investigation is important in facilitating the diagnosis.
P2 NO SYMPTOM AWARENESS IN SALFORD LUNG CANCER PATIENTS: THE NEED FOR A PUBLIC HEALTH AWARENESS CAMPAIGN
S. C. O. Taggart, M. Baxendale, K. Peplow, J. Murray. Lung Cancer Unit, Salford Royal NHS Trust, Hope Hospital, Manchester M6 8HD, UK
Background: Many factors affect when and how patients present for diagnosis of their lung cancer (LC) symptoms (Sx)—for example, fear, anxiety, denial, and Sx awareness, etc. These various factors play an important role in the subsequent time intervals between onset of Sx and ultimate cancer diagnosis. This study was performed to establish the Sx awareness of a group of LC patients and determine the interval between Sx onset and presentation to GP and subsequent cancer diagnosis.
Abstract P2 Median time intervals for lung cancer patients
Methods: The study was approved by the local research and ethics committee. Forty seven new LC diagnoses in summer 2004 were invited to participate and 29 (62%) felt well enough to be interviewed at home by a nurse specialist. The GP and hospital records (CT scan + bronchoscopy) were examined to verify whether the subject’s presentation was cancer related (Sx-CR) or not (Sx-incidental).
Results: Participants did not differ from non-participants by age (69.1 v 65.3 years), male sex (62% v 59%) or clinical stage of disease (Stage 1-3A, 24% v 22%; Stages 3B-4, 76% v 78%). None of the 29 subjects were aware of the symptoms of LC. 43% of subjects admitted to extreme fatigue, weight loss, or cough but only 11% to haemoptysis.
Conclusions: Salford LC patients (1) have no awareness of LC symptoms and (2) experience significant time intervals from onset of LC Sx to diagnosis. Approximately two thirds of new LC diagnoses present with active verified cancer symptoms and one third as incidental findings.
Recommendations: (1) A large and concerted effort is required to increase public awareness of LCSx in Salford. The first step will be the introduction of a lung cancer symptom awareness leaflet and an audit trail will track its impact on healthcare provider services. (2) Future studies addressing LC pathway time intervals ought to identify those patients who are presenting with genuine LC symptoms as they experience significantly shorter patient journeys than incidental LC diagnoses.
P3 WORDING OF CHEST X RAY REPORTS CODED AS “POSSIBLE LUNG CANCER”
D. A. Stock, C. McCann, S. Bari, K. Mohan, M. J. Ledson, M. J. Walshaw. Liverpool Lung Cancer Unit, Royal Liverpool University Hospital and The Cardiothoracic Centre, Liverpool UK
Background: We have had a coded chest x ray system as an aid to rapid referral for patients with suspected lung cancer at our lung cancer unit since 2000, and such a system is now recommended by the NICE guidelines for lung cancer care. However, these systems rely upon the accuracy of the reporting radiologist in order to avoid wasting precious secondary care resources. With this in mind, we were interested in assessing the wording used by radiologists as an indication of the likelihood of an ultimate cancer diagnosis.
Methods: In coded x ray reports we looked for correlation(s) between commonly used descriptive terms (shadowing, consolidation, collapse, prominent hilum, opacity, nodule, cavity, [lung] mass, mediastinal widening, pleural thickening, pleural effusion) and the presence of cancer. We also noted those reports where the radiologist had specifically remarked that the appearance was either suggestive of cancer or that cancer could not be excluded.
Results: A total of 413 coded chest x ray reports were reviewed where we had confirmation of the final diagnosis (cancer v non-cancer) on our hospital database. In 259 (62.7%) an ultimate diagnosis of cancer was made. For each descriptive term, the proportion of cases with cancer was as follows: shadowing 33/62 (53.2%), consolidation 31/47 (66.0%), collapse 46/73 (63.0%), prominent hilum 46/82 (56.1%), opacity 28/46 (60.9%), nodule 21/31 (67.7%), cavity 4/5 (80%), [lung] mass 115/142 (81.0%), mediastinal widening 13/16 (81.3%), pleural thickening 3/10 (30.0%), pleural effusion 27/38 (71.0%) (p = 0.0003). Of those reports indicating that the appearance was suggestive of cancer, 128/162 (79.0%) were correct. Where it was commented that cancer could not be excluded, in only 37/97 (38.1%) was cancer ultimately diagnosed (p = <0.0001).
Conclusion: This study shows that some descriptive terms are more powerful indicators of the presence of cancer than others, with “mass” (in the lung) and “mediastinal widening” having the strongest correlation. “Prominent hilum” and “shadowing” are the least discriminatory of the selected terms. Multivariate analysis would help show these differences more accurately. Furthermore, our group of reporting radiologists appears to have good instincts as to the probability of the chest x ray abnormalities being due to cancer. These data can be fed back to the radiology department and may allow the accuracy of future coding to be improved, thereby facilitating more efficient use of lung cancer units’ resources.
P4 VARIATION BETWEEN CHEST PHYSICIANS AND ONCOLOGISTS IN MEASUREMENT OF PERFORMANCE STATUS OF PATIENTS WITH NON-SMALL CELL LUNG CANCER
J. Maguire, V. Kelly, A. Armour, C. Smyth, M. Ledson, M. Walshaw. Liverpool Lung Cancer Unit, Cardiothoracic Centre, Thomas Drive, Liverpool L14 3PE, UK
Performance status (PS) is the most important prognostic factor for patients with non-small cell lung cancer (NSCLC). Accurate assessment of PS is essential to ensure appropriate selection of treatment for patients with this disease.
We have compared assessment of patient PS by chest physicians and oncologists in 107 patients with NSCLC diagnosed in the Liverpool Lung Cancer Unit Rapid Access Service between April 2004 and April 2005. PS was assessed by the chest physician at the patient’s first appointment and by the oncologist after diagnosis either one or two weeks later. Both assessments were made within 14 days in all cases. Fifty three patients were males and 54 female. The median age was 71 years (range 39–89 years).
In 40 cases (39.4%) the chest physician and oncologist agreed on the patient PS. In 38 cases (35.5%) the oncologist assessment of PS was one level higher than that recorded by the chest physician. In 19 cases (17.8%) the oncologist’s PS measurement exceeded that of the chest physician by two, and in two cases the oncologist’s measurement of PS was three higher than that recorded by the chest physician. There were eight cases (7.4%) where the PS recorded by the oncologists was 1 point less than PS documented by the chest physician. In general, chest physicians tended to assess patients’ activity levels more favourably than oncologists.
Regular assessment of PS is part of the routine day to day work of oncology and oncologists are used to using PS to select patients for chemotherapy and radiotherapy. It may be appropriate to consider the potential variation between chest physicians and oncologists in assessment of PS when discussing patient management at multidisciplinary team meetings.
Abstract P4
P5 THE THIRD WAVE: AN UPDATED META-ANALYSIS OF POSTOPERATIVE CHEMOTHERAPY FOR NON-SMALL CELL LUNG CANCER USING CISPLATIN BASED REGIMENS
N. Chaudhuri, M. Field, A. Reddy, A. S. Soorae. Cardiothoracic Centre NHS Trust Liverpool, UK
Objectives: In 1995 the NSCLCCG meta-analysis of randomised control trials (RCT) suggested a small survival benefit with cisplatin based adjuvant chemotherapy regimens post non-small cell lung cancer (NSCLC) resection (
). The results were not widely accepted due to wide confidence intervals and small size of individual RCTs. In the second wave that followed several trials produced conflicting results. In 2004 two landmark studies (JBR10 and CALGB9633) reported significant benefits. We therefore performed an updated meta-analysis of cisplatin based regimens published after the 1995 meta-analysis to define the benefits of adjuvant chemotherapy in a surgical setting for NSCLC.
Methods: RCTs with cisplatin containing regimens reported from 1995 onwards were included and evaluated separately. RCTs were identified by searching MEDLINE, EMBASE, and Cochrane Trials Register, and also searching through reference lists of articles and conference abstracts. The logarithm of the hazard ratio and its standard error were calculated, and a fixed-effect model was used to combine the estimates.
Results: There were 4417 patients enrolled in eight trials included in the analyses. There was relative reduction in mortality associated with postoperative cisplatin regimen (odds ratio 0.81, 95% confidence interval (CI), 0.72–092; p = 0.0008) compared with after surgical resection alone. A Forest Plot (see fig) gives us an idea of CI.

Conclusions: This updated meta-analysis after the “third wave” cisplatin regimen RCTs demonstrates significant survival advantage in the postoperative treatment of NSCLC. However, RCTs are still needed to ascertain the best regimen and alternative drugs (with better survival and safety).
P6 CAVITATING NON-SMALL CELL LUNG CANCER: DOES IT REPRESENT A MORE AGGRESSIVE DISEASE?
G. Horan, T. V. Ajithkumar, T. W. Roques, W. M. C. Martin. Norfolk & Norwich University Hospital, Norwich, UK
Introduction: Cavitating non-small cell lung carcinoma (cNSCLC) is thought to be a distinct entity, with a short presentation, rapid progression, chemotherapy resistant disease, and generally heralding a worse prognosis. We retrospectively analysed the clinicopathology, radiology, treatment intent, and outcome to ascertain this.
Methods: Data from all patients seen with lung cancer from 1/6/96 to 30/6/2005 were analysed. 104 patients were found with cavitating lung lesions out of a total of 1877 patients. Notes were analysed for histology, radiology, tumour site, disease TNM stage, treatment type, intent, and outcome. Outcome for all lung cancer patients treated in the year 1998 was calculated in order to compare survival with cNSCLC patients and to detect any significant differences in the two population groups.
Results: Seventy four of the 104 patients had cNSCLC at initial presentation; the remainder developed the cavitation either post-treatment, at recurrence or development of metastases, with a further 12 patients having other histology types. 74% were male with a median age of 73 years (range 48–93). Squamous histology was found in 90% with adenocarcinoma in the remaining 10%. TNM stage was predominantly stages III–IV (79%). Chest x ray revealed the abnormal cavitation in 18%, CT thorax in 42%, and using both modalities in 40%. The radiological site was mainly the upper lobes (UL) with left UL in 24 (32%), right UL in 26 (35%) and right lower lobe 10 (14%). The remainder were sited in right middle lobe 2 (3%), lingula 3 (4%), left lower lobe 6 (8%), and information unavailable in 3 (4%). This gives an upper; middle; lower lobes distribution of 67%; 7%; 22%. Treatment intent was radical in 13% with 3% receiving induction chemotherapy. 69% were treated using palliative radiotherapy with 13% having received some chemotherapy. 3% received chemotherapy alone. 15% were not offered any active treatment. Median overall survival was 6.8 months (m) divided respectively into stages IB = 25 m, II = 2.7 m, IIIA = 2.4 m, IIIB = 6.3 m, and stage IV = 5.3 m. Survival was not related to sex, however radical patients did significantly better with survival of 22 m compared to 5.3 m for palliative patients (p = 0.0055). The median survival for all lung cancer patients treated in 1998 was 4.9 m with stage III = 5.3 m and stage IV = 2.7 m.
Conclusions: This is the largest series of cNSCLC reported. In our institution it represents 5% of all the lung cancer patients seen since 1996. 79% of cases present with stage III/IV with predominantly squamous histology and the radiological site was mainly the upper lobes. This is similar to non-cavitating lung cancers. Median survival for all lung cancers in 1998 was 4.9 m compared to 6.8 m for cNSCLC. These data would not support the theory that cavitating lung cancer is a distinct clinical entity with a poorer outcome.
P7 HOMOCYSTEINE LEVELS IN NEWLY DIAGNOSED PATIENTS WITH NON-SMALL CELL LUNG CANCER
J. Maguire, A. Armour, V. Kelly, M. Ledson, C. Smyth, M. Walshaw. Clatterbridge Centre for Oncology, Cardiothoracic Centre, Thomas Drive Liverpool L14 3PE, UK
Introduction: Serum levels of homocysteine comprise the most sensitive and accurate marker of subclinical folate deficiency. Increased levels of homocysteine have been associated with a number of pathologies. Patients with lung cancer are frequently elderly and may have insufficient dietary intake of folate. Subclinical folate deficiency may lead to both increased morbidity during chemotherapy and radiotherapy, and possibly reduced response rates to both treatment modalities.
Methods: We measured serum homocysteine levels in 43 newly diagnosed patients with non-small cell lung cancer who were referred to the Liverpool Lung Cancer Unit between October 2004 and April 2005. Twenty six patients were male, 17 female. The median age was 71 years. 23% of patients were PS 0–1, 30.2% PS 2, and 40.9% PS 3. The local laboratory normal reference range for homocysteine is <15 μmol per litre. Twenty six patients (60.5%) had increased blood levels of homocysteine. In 13 cases (30%) the level was ⩾20 μmol/l and in seven cases (14%) homocysteine was ⩾25 μmol/l.
Conclusion: The finding of increased homocysteine levels in 60% of newly diagnosed patients with non-small cell lung cancer is of potentially profound significance, as this implies that there could be a potential therapeutic benefit derived from B12 and folate supplementation before and during treatment for this group of patients with non-small cell lung cancer.
P8 PULMONARY FUNCTION TESTING AS PREDICTORS OF POSTOPERATIVE COMPLICATIONS AND PROLONGED HOSPITALISATION AFTER LUNG RESECTION.
W. W. Y. Tso, D. Wilson, M. Gillion, T. Treasure, B. E. A. Lams. Guy’s & St Thomas’ Hospital, London, U.K
Objectives: To assess the utility of preoperative pulmonary function testing in identifying patients at high risk of complications or prolonged length of stay in hospital after lung resection.
Method: For all patients who had lung cancer resections from September 2002 to June 2005, pulmonary function and the postoperative course were retrieved from the pulmonary function laboratory and cardiothoracic centre database. Complication rates and duration of hospital stay were analysed according to age, extent of surgery (number of bronchopulmonary segments resected) and pulmonary variables (FEV1, transfer factor (TLCO), predicted postoperative (ppo) FEV1, and predicted postoperative (ppo) TLCO).
Results: 221 patients were studied. Lobectomy or sublobar resections were performed in 192 patients and pneumonectomy or extrapleural pneumonectomy in 29. Seven patients died within one month of surgery (mortality rate = 3.2%). In addition, 36 patients had postoperative complications. Nineteen patients who had been classified as high risk according to the British Thoracic Society guidelines (
) had lung resection surgery, of whom three died (mortality rate = 16%) and three patients had postoperative complications. ppoTLCO <40% and number of resected segments 39 were significantly associated with postoperative complication rates (Fisher’s exact test, p = 0.04 and p = 0.01 respectively). The median length of stay (LoS) was 6 days (IQR: 4–8). The extent of surgery, ppoFEV1, TLCO, and ppoTLCO were all significantly related to LoS (p<0.05). Forward multiple regression indicated that ppoTLCO had the most significant relation (p<0.001) with the length of hospital stay. An independent sample t test showed that ppoFEV1 or ppoTLCO <40% predicted were associated with increased LoS. (t = −2.86 and t = −4.08 respectively, p<0.05). Neither age, FVC, nor FEV1 correlated with LoS.
Conclusion: Our data indicate that risk of postoperative complications was significantly increased in patients with a ppoTLCO <40% predicted as well as in those undergoing a pneumonectomy. A ppoFEV1 or ppoTLCO less than 40% of predicted were associated with prolonged hospitalisation.
Airways disease: clinical management
P9 TIDAL BREATHING AT RESIDUAL VOLUME MAY BE ASSOCIATED WITH SEVERE ASTHMA
C. O. Prys-Picard, R. M. Niven. North West Lung Research Centre, South Manchester University Hospital Wythenshawe, Manchester, UK
Introduction: Normal healthy individuals breath at a tidal volume such that they have an expiratory reserve volume (ERV) of 1000–1500 ml. Patients with severe asthma are typically considered to hyperinflate, either passively or dynamically, and have normal or high lung volumes. We are not aware however of data describing the absolute lung volume at which tidal breathing occurs in patients with severe asthma.
Methods: Twenty clinically stable patients with severe persistent asthma were monitored using respiratory inductance plethysmography (LifeShirt Vivometrics Inc, Ventura, CA, USA). Each was asked to perform three forced vital capacity manoeuvres with a 30–60 second period of rest in between. The subsequent uncalibrated respiratory waveforms were examined for evidence of a lack of a discernable ERV in either the rib cage or tidal volume trace in any of the three attempts. The abdominal trace was excluded from the analysis as it has a tendency to paradoxical movement during forced expiratory manoeuvres.
Results: Of the 20 subjects, six were unable to perform a forced expiratory manouevre of sufficient quality and were excluded. Eight patients were able to demonstrate in at least one effort, and at least one trace, a significant ERV (fig 1). Six patients were not able to demonstrate a significant ERV suggesting that their tidal breathing is occurring at the lower limit of their functional lung volume (fig 2).

Tidal breathing.

Tidal breathing.
Conclusion: A significant proportion of patients with severe asthma appear to breathe at the lower limit of their functional lung volume. It would be expected that this may make them more prone to atelectasis and sputum retention and may contribute to the wheeze. It is unclear whether this is a primary or secondary phenomenon, but may be a learnt avoidance measure to avoid coughing, which many asthmatics find very unpleasant.
P10 NON-ADHERENCE REMAINS A MAJOR PROBLEM IN DIFFICULT ASTHMA
J. Gamble1, A. Lazenbatt2, L. G. Heaney1. 1Regional Respiratory Centre, Belfast City Hospital, N Ireland; 2Queens University Belfast, N Ireland
Introduction: Approximately 5% of adult asthmatics remain difficult to control despite maximal maintenance therapy being prescribed.1 Corticosteroids are the cornerstone of asthma treatment, however poor adherence with therapeutic regimes is prevalent in all severities of asthma and is a probable cause in some difficult to control cases.1 Management strategies which address this issue within the difficult asthma population need to be studied, however we first need to be understand the extent of the problem.
Aim: Direct measures of adherence such as drug assays are not easily applicable for the quantification of inhaled medication use. Prescription refill rates have been found to be an accurate and practical method of identifying poor adherence.2 Limitations in this method are recognised, however it is likely that non-adherence rates will be underestimated rather than overestimated. Our aim was to determine the number of patients attending a dedicated difficult asthma service who were significantly non-adherent to prescribed inhaled corticosteroids (which we defined as prescription filling of ⩽50% of prescribed).
Methods: In Northern Ireland, all GP surgeries have easily accessible computerised prescription records and patients are only able to obtain prescriptions from a single prescription source (confirmed from the GP and patient). GPs were contacted and produced patient prescription refill data for inhaled corticosteroids for the preceding six months for all subjects attending a Regional Difficult Asthma Clinic. Refill rates were compared with prescribed medication and expressed as a percentage.
Results: 143 subjects were assessed, of those 57 (40%) were non-adherent (seven (5%) no information available). Of those who were non-adherent four (7%) were taking <10% of prescribed inhaled steroids, 10 (17%) were taking 10–20%, 17 (30%) were taking 31–40%, and 26 (46%) were taking 41–50%. Of those taking ⩾50% medication (79 (55%)), 24 (30%) were taking >100%, 36 (46%) were taking 71–100%, and 19 (24%) were taking 51–70%. Many of those who were non-adherent requested multiple beta-agonist inhalers (6 month period, median 8, range 0–88), with many using supplemental nebulised salbutamol, suggesting that symptoms remained prominent and retrieving prescriptions was not the primary problem.
Conclusion: Despite severe symptoms and attendance at a dedicated difficult asthma service with multidisciplinary assessment and support, a significant proportion of patients remain non-adherent to inhaled corticosteroid therapy. These results support the need for the development of strategies to improve adherence in this population. It also suggests that objective review of computerised prescribing records should be a mandatory part of the assessment of difficult asthma.
1
2
P11 PATTERN OF SUPPRESSION OF EXHALED NITRIC OXIDE AFTER INTRAMUSCULAR TRIAMCINALONE IN DIFFICULT PAEDIATRIC ASTHMA
J. R. Panickar, J. Grigg. Institute of Lung health, University of Leicester, UK
Background: In our difficult asthma protocol, children receiving IM-TAM have regular assessment of exhaled nitric oxide (eNO) before and during therapy.
Aim: To prospectively evaluate the temporal pattern of suppression of eNO during intra muscular triamcinolone (IM-TAM) therapy.
Methods: Three children with difficult asthma were treated with IM-TAM (60 mg). eNO, and respiratory symptom score was determined weekly. Data were analysed for the four week period before IM TAM (pretreatment period, weeks 1–4) and for eight weeks after the injection (week 5–12).
Results: The table summaries the eNO response. eNO was suppressed to normal levels following the injection. Suppression of eNO continued for one month, then subsequently increased. In all three children, this increase in eNO preceded the reappearance of significant asthma symptoms by at least two weeks.
Conclusion: eNO is suppressed for up to four weeks following IM-TAM, and the subsequent increase in eNO preceded the reappearance of symptoms. We conclude that eNO may be a useful method to guide the scheduling and dose of subsequent IM injections.
Abstract P11
P12 WITHDRAWN
P13 CATEGORISING THE ASTHMA PHENOTYPE: RESULTS OF A FACTOR ANALYSIS
P. Haldar, R. H. Green, M. A. Berry, A. J. Wardlaw, I. D. Pavord. Institute for Lung Health, Glenfield Hospital, Leicester, UK
Asthma has traditionally been defined on the basis of multiple parameters that typically include variable airflow obstruction, airway inflammation, and symptoms such as wheeze and breathlessness. However, there are a substantial number of additional variables used in the assessment of asthma, in both clinical and research settings. We performed factor analysis—a vector based statistical method of data reduction—to investigate whether our description of asthma on the basis of multiple variables could be effectively reduced into easily identifiable “factors” or domains.
Factor analysis, with orthogonal varimax rotation, was performed on data from 271 patients attending the difficult asthma clinic at Glenfield Hospital using SPSS version 10 for Windows. All patients had refractory asthma according to ATS criteria. Data were recorded in each individual for 26 different variables relating to the assessment of asthma. Factor analysis effectively categorised 17 variables into five identifiable domains: (1) Symptoms (scores on nocturnal symptoms, daytime symptoms, activity limitation, breathlessness and wheeze); (2) Allergy (skin prick tests to common allergens, eczema, and hayfever); (3) Psychosocial (scores attained on validated questionnaires for anxiety and depression); (4) Inflammation (sputum and blood eosinophils); (5) Variable airflow obstruction (bronchodilator reversibility and peak flow variability). Interestingly, serum IgE levels loaded equally on the allergy and inflammation domains. Although exhaled NO loaded on the inflammatory domain, the proportion of its total variance accounted for by this was significantly lower than for the other two variables. The analytical process also generated factor scores that effectively assign a weight to each variable indicating its contribution to the factor. Factor scores for variables within a factor were very similar. This analysis demonstrates that asthma may be defined by several independent factors and heterogeneity of the disease phenotype is likely to be represented by the differing relative contributions of these factors within individuals. Using this method to reduce the multiplicity of gathered data will assist in making complex asthma databases comprehensive and facilitate the interpretation of other statistical analyses.
P14 EVALUATING ASTHMA CONTROL
M. Adams1, A. V. Kamath2, C. F. Ramsey2, B. D. W. Harrison2. 1University of East Anglia, UK; 2Norfolk and Norwich University Hospital, UK
Objective: To evaluate the reliability and validity of a measure of asthma control used at a hospital clinic. The Norwich Asthma Questionnaire (NAQ) incorporates the three questions recommended by the Royal College of Physicians (3Q), assessments of reliever inhaler use by day and by night and daily peak flow records. Preliminary results from 23 patients are reported.
Backround: The concept of asthma control needs to be distinguished from that of asthma severity. One questionnaire for assessing control has been described, the Juniper Asthma Control Questionnaire (ACQ) which incorporates a one-off clinic spirometry assessment together with self-report questions.
Methods: To be included patients will have a diagnosis of asthma with a treatment plan corresponding to British Thoracic Society (BTS) step 2 or above. They will be excluded if they have evidence of another similar illness. Patients are seen on three occasions at three month intervals and asked to complete two measures, the NAQ and the ACQ. The clinician also completes a rating on how control has changed.
Results: For all three measure the internal consistency as assessed by Cronbach’s alpha on the three occasions was acceptable to good (ACQ 0.73 to 0.90; NAQ 0.71 to 0.86; and 3Q 0.76 to 0.82). Test re-test correlations for patients assessed by clinicians as showing no change at time 3 were also acceptable although weakest for the ACQ (ACQ 0.45, NAQ 0.74, and 3Q 0.68). Correlations between the NAQ and 3Q (as measures to be assessed) and ACQ and clinician rating (as the standard) are shown in the table below for the three occasions.
Abstract P14
Correlations between the ACQ and clinician ratings for the three occasions were −0.34, −0.49*, and −0.61** and were thus very similar to those for NAQ and 3Q.
Conclusion: The addition of reliever inhaler use and the use of daily measures of peak flow in the NAQ does not appear to add greatly to the information provided by the very simple 3Q. The ACQ is more complex, both for patients and clinicians and does not seem to add much to the assessment of control. So far, the 3Q seems the simplest measure to use and appears to perform as well as any other.
P15 GLOBAL ASTHMA PHYSICIAN AND PATIENT (GAPP) SURVEY: PATIENT EDUCATION AND PATIENT-PHYSICIAN COMMUNICATIONS—UK FINDINGS
C. Baena-Cagnani1, M. Blaiss2, W. Canonica3, R. Dahl4, M. Kaliner5, E. Valovirta6. President of World Allergy Organization1; Immediate Past President of American College of Allergy, Asthma & Immunology2; Secretary and General of World Allergy Organization3; Board of Directors of World Allergy Organization4; President-Elect of World Allergy Organization5; European Federation of Asthma Honorary Member6; 1–6The GAPP Survey Working Group
Objective: To date, global quantitative research has not been conducted to measure whether there are unmet needs in asthma treatment, specifically the factors that may affect compliance: treatment limitations, patient education, and physician-patient communications. The GAPP survey assessed all of those components with patients and physicians.
Methods: A total of 1700 physicians, 1700 adult asthma patients, 1000 paediatric, physicians, and 1000 parents of pediatric patients were surveyed globally across 16 countries (Australia, Belgium, Brazil, Canada, France, Germany, Ireland, Italy, Japan, the Netherlands, Poland, Spain, Switzerland, South Africa, the United Kingdom, and the United States). In the UK telephone interviewing was conducted with 100 physicians, 100 patients, and in addition 100 asthma nurses.
Results: In the UK, physicians reported they discuss side effects with their patients a majority of the time (local side effects—88%; systemic side effects; 61%) and initiate those conversations 69% of the time. Conversely, of the 49% of asthma patients that discuss side effects with their doctors, more than half state they initiate the discussions. However, patients say they rarely or never (89%) discuss systemic side effects or local side effects (80% rarely or never) with their physician. Many patients are not aware of side effects: short term side effects (39% not aware), long term side effects (49%), decreased production of cortisol in the body (55%). Patients report that many aspects of asthma treatment are not discussed with their physicians—plan for treatment (55% report never discussed), correct inhaler technique (35%), keeping diaries (82%), monitoring peak expiratory flow (33%), and contacting patient organisations (87%). Nearly half (47% answered false or not sure) of patients reported that “asthma attacks can be fatal in patients with mild asthma”.
Conclusions: Physicians may be overestimating patients’ knowledge about asthma and the associated risks. Overall, there appears to be a lack of communications during patient-physician-nurse correspondence. There is an opportunity to improve management of asthma patients and educate patients through better physician-patient communications.
P16 PATTERNS OF AIRFLOW LIMITATION IN PATIENTS WITH A PRIMARY CARE DIAGNOSIS OF ASTHMA AND THEIR RELATION WITH EOSINOPHILIC INFLAMMATION
D. E. Shaw, S. Mellor, M. A. Berry, B. Hargadon, S. McKenna, M. Shelley, H. Pateman, R. H. Green, A. J. Wardlaw, R. McKinley, M. Thomas, I. D. Pavord. Institute for Lung Health, Leicester, UK
Over 80% of asthma is diagnosed and managed solely in primary care. Although defined as an inflammatory disorder of the airways, diagnosis tends to be based on non-specific symptoms, simple lung function testing and the response to treatment trials. Little is known about the pattern of airway dysfunction and airway inflammation in patients seen in primary care. We set out to evaluate the different patterns of airflow limitation and their relationship to eosinophilic inflammation in a population of patients from primary care whom had a diagnosis of asthma and had received one or more prescriptions for inhalers in the last year. Patients were all over 18 years and had a smoking history of less than 10 pack years. 184 (99 female) patients were recruited, 31 at step 1 of the BTS asthma guidelines, 79 at step 2, 25 at step 3, 45 at step 4, and four at step 5. Lung function patterns fell into four groups: (1) no evidence of airflow obstruction, n = 42; (2) asthma: post bronchodilator FEV1/FVC ratio of >70% plus one of a methacholine Pc20 <8 mg/ml, % change in FEV1 post salbutamol >15% or PEF amplitude % mean >20% over 2 weeks, n = 96; (3) mixed asthma/COPD: post bronchodilator FEV1/FVC ratio of <70% and any of the above features of asthma, n = 34; and (4) COPD: post bronchodilator FEV1/FVC ratio of <70% and none of the features of asthma, n = 12. The differential sputum eosinophil count was not significantly different between any of the groups and the proportion of patients with an eosinophil count of >3% was similar in all groups (1, 26%; 2, 33%; 3, 24%; and 4, 25% respectively). The mixed asthma/COPD group tended to be older and the COPD group had received significantly more oral steroid courses in the last year. There was no significant difference in other variables including sex, atopy, hospital admissions ever, BDP equivalent dose, long acting beta agonist use, differential sputum neutrophil count, anxiety, depression and Nijmegen questionnaire score, reflux score, presence of rhinitis, and BMI.
In conclusion patients with a primary care diagnosis of asthma who are receiving treatment have mixed patterns of physiological impairment. A significant number have no evidence of airflow obstruction or airway hyperresponsiveness. The physiological characterisation of airways disease is of little value in predicting eosinophilic airway inflammation, and by implication steroid responsiveness, in this primary care population.
P17 DIFFICULT ASTHMA IN THE UK: A NATIONAL SURVEY OF APPROACHES TO MANAGEMENT AND AVAILABLE SERVICES
N. J. Roberts1, D. Robinson2, M. R. Partridge1. 1Imperial College London, NHLI Divison at Charing Cross Hospital; 2Royal Brompton Hospital, UK
Two UK centres caring for sizable numbers of patients with difficult asthma have published results on the management and outcomes for their patients.1, 2 However little is known in general about services available for these patients nor on approaches to management. A questionnaire survey of 802 consultant respiratory physician members of the BTS was undertaken. The questionnaire consisted of five parts with the first four concerning case histories to elicit how patients were managed, availability of other healthcare professionals, diversity of differential diagnoses, and approaches to management. The fifth section elicited information about the respondent and place of work. 344 questionnaires were returned (response rate 42.9%). When faced with a patient with difficult asthma the majority of doctors would perform lung function testing, bone densitometry and estimation of aspergillus precipitins, and skin prick test reactions to common inhaled allergens/fungi on the majority of patients. Over a third would routinely arrange estimation of α-1 antitrypsin levels and 41.8% of doctors would perform a CT thorax on most patients. Very few would automatically arrange for a liason psychiatric opinion. 193 (65.8%) reported difficulties in accessing liaison psychiatrists and 231 (79.7%) reported that it was difficult to access psychologists. A wide variety of differential diagnoses were reported and diagnoses masquerading as difficult asthma included lung cancer, carcinoid tumours, upper airway obstruction, foreign bodies, psychiatric disease, cystic fibrosis, Churg-Strauss syndrome, tracheobronchial amyloid, and achalasia. Faced with a case of probable vocal cord dysfunction there was a range of reported investigations utilised by respondents and a similarly diverse response as to who would be involved with therapy. 41.6% of respondents stated there was a specific asthma clinic in their hospital and 65 (22.7%) had a specific “difficult” asthma clinic. 21 respondents had a special interest in difficult asthma and those respondents cared for a larger number of patients with this condition and were more likely to use liaison psychiatry, prednisolone assays to check for compliance, measurement of bronchial hyperresponsiveness, and oesphageal pH monitoring.
Difficult asthma does not attract a separate section in the current British asthma guidelines and approaches to the diagnosis and management of these patients varies. Access to appropriate ancillary help is similarly non-uniform.
1
2
P18 GLOBAL ASTHMA PHYSICIAN AND PATIENT (GAPP) SURVEY: TREATMENT LIMITATIONS—UK FINDINGS
C. Baena-Cagnani1, M. Blaiss2, G. W. Canonica3, R. Dahl4, M. Kaliner5, E. Valovirta6. President of World Allergy Organization1; Immediate Past President of American College of Allergy, Asthma & Immunology2; Secretary and General of World Allergy Organization3; Board of Directors of World Allergy Organization4; President-Elect of World Allergy Organization5;European Federation of Asthma Honorary Member6; 1–6The GAPP Survey Working Group
Objective: To date, global quantitative research has not been conducted to measure whether there are unmet needs in asthma treatment, specifically the factors that may affect compliance: treatment limitations, patient education and physician-patient communications. The GAPP Survey assessed all of those components with patients and physicians.
Methods: A total of 1700 physicians, 1700 adult asthma patients, 1000 paediatric physicians, and 1000 parents of pediatric patients were surveyed globally across 16 countries (Australia, Belgium, Brazil, Canada, France, Germany, Ireland, Italy, Japan, the Netherlands, Poland, Spain, Switzerland, South Africa, the United Kingdom, and the United States). In the UK telephone interviewing was conducted with 100 physicians, 100 patients, and in addition 100 asthma nurses.
Results: In the UK virtually all adult physicians (98%) agree that inhaled corticosteroids (ICS) are the “gold standard” of asthma therapies. Many UK patients experience short term side effects (41%) and long term side effects (21%) while taking asthma medication. Due to side effects, patients consider or switch medications (36% v 31%), skip doses of medication (36%), consider stopping their asthma medications (24%), or change their dosage (42%). Physicians report that only 14% of patients comply with their asthma medication as instructed more than 75% of the time. By comparison, 43% of patients state they comply with physician instructions more than 75% of the time. Physicians report that non-compliance causes a greater incidence of negative patient outcomes including more hospitalisations or emergency room visits (92%), increased symptoms (98%), night-time awakenings (98%) and life threatening asthma attacks (87%). Eighty percent of physicians and 77% of UK adult asthma patients believe there are unmet needs in the area of ICS asthma therapy.
Conclusions: Physicians and patients agree that asthma patients are not complying with medications partly due to side effects. There is a significant need for new therapies to improve overall asthma management and lessen the impact that side effects have on compliance.
P19 ADMINISTRATION OF INHALED INSULIN TO PATIENTS WITH TYPE 1 DIABETES IS NOT ASSOCIATED WITH AIRWAY HYPERRESPONSIVENESS
L. Kuitert1, J. Teeter2, S. Pandya3, P. Kon4 for the Exubera Study Group1Barts and the London NHS Trust, London, UK; 2Pfizer, New York, USA; 3Pfizer UK; 4sanofi-aventis Group UK
Objectives: Inhaled insulin (INH, Exubera) is being investigated as an alternative, non-invasive method of insulin delivery. The impact of INH therapy on lung function is an important aspect of its safety profile. This study examined whether differences in lung function emerged within 60 minutes post-INH dosing and if any such changes were associated with insulin antibody levels in patients with type 1 diabetes.
Methods: In a 24 week multicentre study, 226 patients with type 1 diabetes were randomised to receive daily premeal INH or subcutaneous (SC) insulin for 12 weeks (comparative phase), followed by SC insulin for 12 weeks (washout phase). Safety evaluations included airway function (forced expiratory volume in 1 second (FEV1)) and serum insulin antibodies. FEV1, measured prior to and 10 and 60 minutes after insulin dosing at weeks 0, 4, 8, and 12, was used to assess the functional development of airway sensitisation.
Results: Small, non-progressive treatment group differences in decline from baseline FEV1 occurred within two weeks of INH initiation (adjusted difference: −0.043 l), did not worsen over the following 10 weeks, and resolved within two weeks of discontinuation (adjusted difference: +0.041 l). Differences between the treatment groups in the adjusted mean change from baseline in FEV1 10 minute and 60 minute responsiveness were small and not significant at Week 12 (−0.010 l and −0.024 l, respectively). In INH treated patients, insulin antibody levels were low during the first two weeks of therapy, rose to a median of 37.0 μU/ml (mean, 134.3 μU/ml) by week 12, and declined during follow up (median and mean values at week 24: 23.0 μU/ml and 50.3 μU/ml, respectively). Insulin antibody levels in SC insulin-treated patients remained stable throughout the study. Insulin antibody levels were not correlated with FEV1 changes.
Conclusions: INH does not result in acute airway obstruction at the time of inhalation. The treatment group differences in pulmonary function that were observed were small, occurred within the first two weeks of treatment, did not worsen with time, and resolved within two weeks of treatment discontinuation. This study also found that there was no relation between insulin antibody and pulmonary function test responses, suggesting that lung function and immunologic response are caused by different mechanisms.
P20 SECONDARY CARE IMPLEMENTATION OF STEPPING-DOWN INHALED CORTICOSTEROID THERAPY IN STABLE ASTHMA
D. K. C. Lee1, P. S. Borade1, G. P. Currie2, D. A. Promnitz1. 1Department of Respiratory Medicine, Ipswich Hospital, Heath Road, Ipswich IP4 5PD, Suffolk, UK; 2Department of Respiratory Medicine, Aberdeen Royal Infirmary, Foresterhill, Aberdeen AB25 2ZN, UK
Background: Current guidelines advocate stepping-down inhaled corticosteroid (ICS) therapy at three monthly intervals once asthma control has been achieved.
Methods: We assessed asthmatics being followed up in secondary care for a minimum six month period. Patients who had an exacerbation or who were receiving or had received either oral or parenteral corticosteroids, or immunosuppressive therapy within a 12 month period were excluded. A study was performed over the preceding 12 months to evaluate whether ICS therapy had been reduced or not following a prolonged period of stability.
Results: Sixty consecutive asthmatics were assessed in clinic. Recruited patients who fulfilled the strict exclusion criteria and completed the study had mean age of 56 years and FEV1 of 1.97 l (73% predicted). The mean ICS dose was 1267 μg daily and patients had either moderate or severe asthma. Only 17% of patients had step-down in ICS therapy. The remaining 83% of patients continued on the same dose of ICS despite having had stable asthma during the preceding 12 months. There were no significant differences in any outcomes according to whether patients had ICS therapy reduced or not.
Conclusion: Stepping-down ICS therapy in stable asthmatics is poorly implemented. If this is reflective of practices throughout the United Kingdom, many stable asthmatics may be exposed to unnecessary high doses of ICS.
P21 THE ECONOMIC AND HUMAN IMPACT OF POOR CONTROL IN PATIENTS WITH SEVERE PERSISTENT ALLERGIC ASTHMA: RESULTS FROM A MULTINATIONAL STUDY
F. Turk1, S. Kay2, V. Higgins2. 1Novartis Pharma AG, Basel, Switzerland; 2Adelphi Group, Bollington, Cheshire, UK
Introduction: The economic and human impact of asthma is highly skewed towards patients with severe disease. We hypothesised that this disproportionality is driven by patients with uncontrolled, severe persistent allergic asthma.
Methods: Patients with asthma were enrolled in a large, cross sectional observational study and were stratified by disease severity (Global Initiative for Asthma (GINA) treatment and symptoms classifications (GINA 2004)). Patients were recruited in the UK, France, Germany, Italy, and Spain by physicians (1:1 primary care physicians:specialists) who were asked to recruit the next six patients presenting with asthma. Detailed questionnaires were completed by both physicians and matched patients; these covered symptomatology, exacerbations, quality of life, and resource use. Data were weighted to adjust for the overrepresentation in the sample of specialists’ patients and those patients who consult more often. Results are presented for patients with severe (GINA treatment step 4) allergic asthma.
Results: A total of 1306 of the 2802 recruited patients (47%) had allergic asthma, 965 of whom could be classified into GINA symptoms and treatment severity categories. Eighteen per cent (weighted data) of classifiable patients had severe persistent asthma (GINA treatment step 4), of whom 55% were uncontrolled (GINA symptom severity steps 3 and 4). These uncontrolled patients had significantly more acute exacerbations requiring treatment than controlled patients (mean 2.75 v 1.70 events/patients/year; p = 0.011). Resource use was higher in uncontrolled versus controlled patients. Uncontrolled patients had more exacerbations requiring emergency room treatment (0.28 v 0.03 events/patient/year, respectively; p = 0.001) and hospitalisation (0.08 v 0.02 events/patient/year, respectively; p = 0.048), and spent more time in hospital as a result of their symptoms than controlled patients (0.63 v 0.07 days/patient/year, respectively; p = 0.005). In addition, uncontrolled patients had a significantly poorer quality of life than controlled patients (mean EuroQol EQ-5D score 0.85 v 0.94, respectively; p = 0.008). Thirty per cent of uncontrolled patients felt they had to adjust or restrict their lifestyle because of their asthma (scores 4 or 5 on a scale of 1–5, where 5 = yes, greatly, and 1 = no, never), compared with 17% of controlled patients.
Conclusions: Patients with uncontrolled severe persistent allergic asthma have a disproportionately higher use of healthcare resources and poorer quality of life than those with controlled severe persistent allergic asthma. Focusing on improving asthma control in this group of patients has the potential to reduce the economic and human burden of allergic asthma.
P22 COMPUTER ASSISTED LEARNING IS A USEFUL TOOL TO TEACH FINAL YEAR MEDICAL UNDERGRADUATES THE PRINCIPLES OF SPIROMETRY
S. F. Smith, H. Brenton, N. J. Roberts, M. R. Partridge. Imperial College London, NHLI at Charing Cross Campus, St Dunstans Road, London W6 8RP, UK
Previous studies from this department have shown that final year undergraduate medical students have only a limited capacity to interpret spirometry and a poor understanding of its use as a diagnostic tool.1 One hundred and thirty seven final year student volunteers, recruited four months before their final examinations, were randomised into one of three teaching groups, each of which was taught the same factual content which covered the diagnosis and differential diagnosis of lung diseases and interpretation of spirometry. For group 1 (n = 40), this was delivered in the format of an interactive teaching session with an experienced teacher of respiratory medicine. Group 2 (n = 40) received a didactic lecture from the same member of staff. Group 3 (n = 57) were given a limited period of time to study the same material on their own under supervision, but without opportunities for interaction with a staff member, using a purpose created WebCT computer package.
Students completed a series of short answer questions before the teaching session in order to determine their baseline respiratory knowledge and understanding of spirometry. After the teaching, they completed a different set of short answer questions, covering the same content. There was no difference in the baseline capacity to interpret spirometry reports between the three groups (see table).
Abstract P22 Scores for the spirometry questions alone
The group using the computer assisted learning (CAL) package performed significantly better on spirometry than both other groups (see table), despite the fact that, when asked, 82% of students identified an interactive session with an expert teacher as their preferred method of learning. This study emphasises the potential value of CAL in clinical teaching.
This study was funded by the European Respiratory Society.
1
Organisation of lung cancer services
P23 MANAGEMENT OF LUNG CANCER: IS IT AFFECTED BY THE SOURCE OF REFERRAL?
A. Hardy1, C. H. Wong1, A. Cotton1. 1Department of Respiratory Medicine, Pontefract General Infirmary, West Yorkshire, UK
It is recognised that a large proportion of lung cancer patients are diagnosed as hospital inpatients. We wanted to know if the mode of referral to the respiratory department affects a patients management. We audited all patients diagnosed with lung cancer during 2004 at Pontefract General Infirmary and Pinderfields General Hospital in West Yorkshire. During 2004 we diagnosed 221 cases of lung cancer. 81 (37%) were diagnosed as hospital inpatients (IP), 140 (63%) as outpatients (OP). The time to first CT scan, first bronchoscopy, confirmation of diagnosis, and starting treatment were all longer in the patients diagnosed as outpatients. These differences persisted when times were calculated based on day of first being seen by the respiratory consultant, rather than day of referral.
A similar percentage of patients in the groups had a CT (80% IP v 93% OP) and bronchoscopy (52% IP v 80% OP). Three of 81 inpatients (4%) v 18 of 140 outpatients (13%) were referred for a curative resection, suggesting that the outpatient group were diagnosed at an earlier stage, however, we do not have comprehensive data regarding stage at time of diagnosis.
These results suggest that the poorer prognosis seen in patients diagnosed with lung cancer as hospital inpatients is not due to unnecessary delays in their management, but may be due to later presentation of these patients. The aim should be to improve the current outpatient services to reduce waiting times and access is currently being reviewed.
P24 THE EFFECT OF THE LUNG INVESTIGATION DAY ON THE TIME TAKEN TO DIAGNOSE LUNG CANCER
J. R. Ramsay, G. M. Smith, M. F. Muers. Leeds General Infirmary, Great George Street, Leeds, UK
Introduction: Approximately 50% of patients with lung cancer experience delays in diagnosis. 63% attribute this to delays in the healthcare system. Following on from this, 87% of individuals questioned would rather be investigated via a “one stop clinic”. To determine whether the investigation process could be optimised the Lung Investigation Day (LID) was introduced at the Leeds General Infirmary (LGI). This is a one stop clinic for the investigation of patients suspected to be suffering from lung cancer. Patients attend in the morning for their staging CT and lung function. If amenable to CT guided percutaneous biopsy this is performed. If bronchoscopy is required this is performed in the afternoon.
Methods: Three patient groups were identified: those investigated through LID (group 1); non-LID controls, during-LID (group 2); and non-LID controls, before the introduction of LID (group 3). The following data were collected: time from clinic to staging CT, time from clinic to bronchoscopy; and time from clinic to discussion at multidisciplinary meeting (MDT). All patients included in this study had a final diagnosis of lung cancer.
Results: Group 1 sample size = 60. Group 2 sample size = 54. Group 3 sample size = 56. The mean time from outpatient appointment to discussion at MDT for those patients in group 1 was 13.85 (range 4–34, standard deviation 6.57). The mean time from out patient appointment to discussion at MDT for those patients in group 2 was 23.17 (range 9–54, SD 12.28). The mean time from out patient appointment to discussion at MDT for those patients in group 3 was 20.4 (range 4–43, SD 9.91).
Conclusions: The LID considerably reduces the time to investigate patients with lung cancer and has allowed us to meet the BTS recommendation to diagnose lung cancer within two weeks. The introduction of LID does not seem to compromise those patients that do not pass through the LID.
P25 AGE AND STAGE AT PRESENTATION IN LUNG CANCER
J. Ramsay. Leeds General Infirmary, UK
Introduction: Advanced stage of lung cancer at presentation predicts worse survival. The poor prognosis of elderly people could therefore be explained by presenting with late stage disease.
Aim: To study the relation between age and stage at diagnosis for lung cancer.
Methods: Using the Leeds Lung Cancer Database the first set of stage data for each patient was analysed according to age group (⩽65, 66–74, and 75+). Differences in proportions were tested for significance using the χ2 test.
Results: Data from 2530 patients with confirmed lung cancer were examined. 832 were aged ⩽65 years, 800 were aged 66–74 years, and 898 were aged 75+ years. The median age at diagnosis was 71 years (range 28–99). 1028 patients were excluded from the analysis as a diagnosis of small cell lung cancer was made or no staging data were available. Those with complete staging data and proven non-small cell lung cancer (902, 60%) were analysed. Percentages presenting with advanced disease (stages III–IV) were: 74% in those ⩽65; 61.7% in the 66–74 age group; and 64.6% in the 75 and above group (χ2 = 13.4, df = 2, p<0.01). 600 patients with a radiological diagnosis had staging data available. Those presenting with advanced disease (stages III–IV) were: 62.7% in those ⩽65; 70.8% in the 66–74 age group; and 63.6% in the 75 and above group (χ2 = 3.55, df = 2, p<0.1).
Conclusion: This analysis showed no convincing evidence that older patients present with more advanced stage lung cancer. Indeed, it compliments much of the published literature suggesting that elderly people are more likely to be diagnosed with early stage disease.
Abstract P23
P26 GENERAL PRACTICE UTILISATION OF A RAPID ACCESS LUNG CANCER CLINIC IN LIVERPOOL
D. A. Stock, A. McIver, S. Bari, K. Mohan, M. J. Ledson, M. J. Walshaw. Liverpool Lung Cancer Unit, The Royal Liverpool University Hospital and The Cardiothoracic Centre, Liverpool, UK
Background: All lung cancer units have set up rapid access services to cater for urgent GP referrals for patients with suspected lung cancer under the “14 day rule”. Such services are resource intensive, and it is therefore important to ensure that patients are referred appropriately. In Liverpool, we have the highest incidence of lung cancer in England and Wales, and up to 400 cases per year are diagnosed at our lung cancer unit, many under the 14 day wait rule. We were interested to ensure that GPs referring in this way were making best use of available resources.
Methods: We examined all entries in our lung cancer database from its inception in January 2000 through to April 2005 relating to urgent referral under the 14 day wait rule. Each referring general practice (GP) was assigned a code based on the address, and these data were correlated with route of referral and eventual diagnosis (cancer v non-cancer). A separate record of referrals deemed inappropriate by the lung cancer unit clinicians on the basis of a faxed referral proforma was also examined (from January 2001).
Results: Of 3643 entries in our lung cancer database the dataset was complete in 3482. 1974 (56.7%) were referrals from primary care (mean age 70.6 years, 1037 male). “Infrequent referrers” (GP practices that made a mean of one referral or less per year) were excluded. The remaining 75 practices made a total of 1872 referrals (range 6–76, mean 25). In 891 cases a diagnosis of lung cancer was reached (47.6%), with accuracy for individual practices of between 13.0% and 88.9%. There were 136 inappropriate referrals, 121 of which were from the primary care sector. Six from “infrequent referrers” were excluded. The remaining 115 inappropriate referrals spanned 50 of the 75 above practices (mean 1.5, range 0–12; 0%–20.0% of total referrals). Only a single practice sent inappropriate referrals numbering five or more and constituting >10% of their total output.
Conclusions: This study has shown the potential for lung cancer teams to identify practices either underusing the local service or sending an excessive number of inappropriate referrals, thereby facilitating appropriate targeted feedback to ensure the optimal use of resources. To maximise the quality of the data, the raw referral figures need to be adjusted for the size of each practices patient list, and a database created for referrals judged inappropriate following initial assessment at the rapid access clinic. On a local level, these results are reassuring in that there appears to be overall uniformity of referral quality across our catchment area. The data can act as a benchmark for future re-auditing so that any change in referral practice can be identified and addressed accordingly.
P27 IS THE TWO WEEK WAIT GENERIC CANCER REFERRAL FORM OF ANY USE?
J. K. Quint, P. King, A. G. Davison, C. D. Eraut, S. O. Ansari, K. GanesLingam. Southend Associate University Hospital, UK
Introduction: There is no nationally agreed cancer referral form, nor is there any research into what information referral forms should contain. Recently published NICE guidelines advise general practitioners (GPs) to explain to patients why they have been referred using the two week wait referral system, and what to expect from their clinic visit. They also make recommendations about giving hospital clinicians sufficient information on the referral form. Southend Hospital uses a standard generic referral form for all cancers. There is no focus on particular signs or symptoms associated with a given cancer or any indication of information received by patients prior to their visit. We looked at details given by GPs on the referral form, including information indicating the patient was aware of a suspected a diagnosis of lung cancer.
Methods: We collected a copy of all lung cancer two week wait referrals from the beginning of June 2004 to the end of April 2005. Information was collated regarding symptoms, examination findings, investigations done by the GP, other medical history, and whether or not the patient was aware of the referral. A list of all patients diagnosed with lung cancer from June 2004 to the end of June 2005 was compared with the patients on the referral list, to see how many had an actual diagnosis of lung cancer.
Results: 135 patients were referred. 123 copies of referral letters were obtained for analysis. 12 (10%) referral letters were illegible. 114 patients (93%) had a chest x ray done: four were normal, 103 abnormal, seven were requested but results not known by the GP. 94 (76%) patients had symptoms mentioned, 16 (13%) had clinical signs mentioned. Drug history was given in 28 (23%), past medical history in 47 (38%), and smoking history in 49 (40%). It was only clear on three referral forms that the patient (2%) was aware of the reason for referral. One of the three patients who had been expecting a diagnosis of lung cancer had an actual diagnosis of lung cancer made. 46 (37%) patients referred using this system were diagnosed as having lung cancer by the end of June 2005. Of those diagnosed with lung cancer in the last year, only 51 (31%) were referred via the two week wait.
Conclusion: Many initial consultations occur without the physician knowing whether the patient knows that their referral is for possible cancer. This makes these consultations harder to conduct. Some patients are referred having been given an incorrect diagnosis of cancer. In these cases reassurance can be difficult. Although a standard generic referral form is easier for GPs, (fewer forms) with the introduction of computer booking this needs to be re-examined. We hope to introduce cancer specific referral forms to target information given by GPs.
P28 THE VALUE OF LUNG CANCER MULTIDISCIPLINARY TEAM MEETINGS: DID PATIENTS ACTUALLY RECEIVE TREATMENT AS AGREED IN THOSE MEETINGS?
A. Elsheikh, B. Yung, C. Trask, B. Waker, B. Idowu, P. Leonard, C. O’Doherty, J. Prejbisz, D. Mukherjee, J. Samuel. Basildon University Hospitals, Basildon, Essex, UK
Background: It is recommended that all cases of patients with newly diagnosed lung cancer be discussed in the lung cancer multidisciplinary team meetings (MDTMs). The aim is for a provisional treatment plan (PT) to be agreed for each patient. The treatment plan may include surgery with curative intent (CS), radical or palliative radiotherapy (RT), chemotherapy (CT), specialist palliative care (SPC), and active symptom monitoring (AM). Once the PT is agreed, the appropriate members of the team then see the patient and a final treatment plan (FT) is determined. We carried out an audit to determine whether there were any discrepancies between the patient’s PT and FT and to establish the reasons for any discrepancies.
Method: All cases of newly diagnosed lung cancer patients at our hospital between January and May 2005 were identified. All patients’ records containing information on the PT and FT were collected and analysed.
Results: Between January and May 2005, 66 cases (36 male) of patients with primary lung cancer diagnosed at our hospital were discussed in our MDTMs. The mean age of the patients was 71 years (range 46–91). Histological diagnosis was available in 53 patients (80%). 60 patients (91%) had clear PTs following the MDTM. Of the remaining six patients, two required further assessment, two were referred outside our network to be considered for clinical trials, and two died before MDTM. The PTs agreed for the remaining patients were (first treatment listed only)—CS: 7 patients; RT: 9, CT: 20, SPC/AM: 21, others: 3. Only five of the 60 patients (8%) with PTs had FTs that were different (see table).
Abstract P28 Reasons for discrepancies
Conclusion: This audit demonstrates that the majority of lung cancer patients received the treatment proposed in the MDTM. We conclude that the lung cancer MDTM provides an effective forum for individual cases to be discussed fully so appropriate treatment plans can be determined.
P29 INCIDENCE OF LUNG CANCER IN AN EAST LONDON BOROUGH OVER FIVE YEARS SINCE APRIL 2000
T. C. O’Shaughnessy, R. Khajuria. Newham University Hospitals NHS Trust, London, UK
Background: Newham has an ethnically diverse population where over two thirds of the population are under the age of 65 years. We have shown an increase in cases of lung cancer reported in the five years from April 2000. We wished to investigate whether there were any similar trends in the ethnic make up of this cancer population and to whether any trends existed as to the residence of the patients by postcode.
Method: Since 2000 the minimum data set for lung cancer has been collected on all patients diagnosed with lung cancer at Newham General Hospital and stored on the Lung Cancer Management System ((LCMS) Unisoft Computers Ltd). Demographic data on postcode and ethnicity was duly analysed.
Results: See table.
Abstract P29
Conclusion: Although there was an increase in the numbers of cases reported, the proportion of non-white patients did not increase over these five years (see table). The highest proportion of cases come from the areas with the highest deprivation index (that is, Beckton, E6). The low proportion of patients from black and ethnic minorities in the area is probably a reflection of the relatively young age compared with the local white ethnic minority group Further work is required to see if there are any other underlying reasons for this trend.
Use of oxygen in chronic obstructive pulmonary disease
P30 PILOT STUDY COMPARING THREE DIFFERENT METHODS OF FLIGHT ASSESSMENT USING HYPOXAEMIC NORMOBARIC CHALLENGES
S. Bari1, J. A. Smith2, S. Turner3, S. Burbidge3, J. C. G. Simpson3. 1Cardiothoracic Centre, Liverpool; 2Wythenshawe Hospital, Manchester; 3Manchester Royal Infirmary, Manchester, UK
Introduction: Flight assessments using hypoxic normobaric challenges (HNC) have been recommended to assess fitness to fly in patients with respiratory disease. Three different methods have been described; a 40% venturi mask driven by nitrogen (VM), a body box (BB), and a Douglas bag with a 15% oxygen source (DB). There are no data comparing these methods. The aim of this pilot study was to assess the feasibility of a study looking at equivalence of results, patient preference, time taken to perform a test, and the cost of the different methods.
Methods: Ethical committee approval was obtained for a prospective randomised trial. Patients were recruited from the outpatient clinic who had requested a flight assessment. Each patient had the three different types of HNC in random order. A positive HNC was a fall of oxygen saturations to 85% during a 20 minute HNC. Patient comfort was assessed using a visual analogue score (VAS) and HNC preference by ranking (1–3). Data were stored and analysed using Excel and SPSS. Results are presented as median and ranges.
Results: Twelve patients (seven male) with an FEV1 of 0.7 l (range 0.45–1.98) performed 36 HNC. Before the first HNC the pulse was 82 (69–103) and the oxygen saturation 94% (93–96). Eight out of nine patients had a positive test using the DB, three patients were intolerant of this method. All patients performed the VM and BB methods, eight out of 12 had a positive test using the VM and seven out of 12 using the BB. In only six patients did all three methods give a positive result. One patient had a negative result with all three methods. The time taken in seconds to reach a positive test for each of the methods were; DB 187 (143–628), VM 315 (214–1020), and BB 1040 (655–1192). Patient comfort scores for each HNC using the VAS were BB 9 (4–10), VM 8.5 (4–10), and DB 7 (1–10). Ranking in order of preference the BB was most popular seven first ranks, followed by VM eight second ranks, and the finally the DB 11 third ranks. The cost of consumables used in a single HNC for the three methods were BB £0.70, VM £2.20, and DB £14.79.
Conclusions: A comparative study of different HNC methods is feasible. The different methods may give different results. The DB was the quickest method but the least comfortable/preferred and most expensive. The BB is the patient preferred test but is time consuming. The VM may offer the best compromise for time, cost, and patient preference. A larger study is needed to confirm these results.
P31 A NATIONAL AUDIT OF FITNESS TO FLY ASSESSMENTS
S. Bari1, S. Burbidge2, S. Turner2, J. C. G. Simpson2. 1Cardiothoracic Centre, Liverpool; 2Manchester Royal Infirmary, Manchester, UK
Background: Hypoxic normobaric challenges (HNC) are used to simulate conditions when at cruising altitude on commercial airlines. Patients with severe respiratory or cardiac disease, who are at risk of hypoxia while flying, can undergo an HNC to assess their fitness to fly with or without supplemental oxygen. Recommendations have been published by the BTS in 2002 (
). The aim of this audit was to determine the availability of HNC in hospitals in the UK, who performs it, what the preferred method is, and what constitutes a positive HNC.
Methods: An address and label list was provided by the BTS, all the adult respiratory physicians on the list were mailed with a questionnaire. Responses were grouped by hospital, data was stored and analysed in Excel.
Results: 502 physicians in 247 different hospitals were mailed, 320 (64%) from 196 (79%) hospitals replied. 101 (52%) of hospitals did not perform HNC, four of these referred to other hospitals, and 39 hoped to start a service in the future.
In the 95 (48%) hospitals where HNC were performed, this was usually by a clinical physiologist 86 (91%). Doctors or nurses performed the remainder. All assessed patients with chronic obstructive pulmonary disease (COPD), 46% with asthma, 86% with pulmonary fibrosis (PF), and 29% with heart disease.
When performing HNC 68% use 15% oxygen supply and a tight mask, 34% used nitrogen and a Venturi mask, 4% used a body box, and 6% used more than one method. Nine hospitals provided protocols used in their units.
When asked what constituted a positive result 15 gave no answer and five were unintelligible (21% of response from hospitals performing HNC). For the other 75 hospitals; 33 (44%) used arterial blood gases with a positive cut off ranging between 6.5–8.0 kPa, 28 (37%) used oxygen saturations ranging from 80%–90%. Five hospitals used a combination of saturations and arterial blood gases. 13 (17%) stated they used BTS or ATS guidelines. Six others gave a range of response including in one case clinical judgement. The most frequently used levels of hypoxia constituting a positive test during a challenge were 90% saturations, 11 (15%); 85% saturations, 12 (16%); and a PaO2 of 6.6 kPa, 8 (11%).
Conclusions: Fewer than half the hospitals performed HNC, when performed it was usually by a clinical physiologist on patients with COPD or PF. The commonest method used was 15% oxygen supply and a tight mask. There was variation in how to measure the hypoxia and even greater variation in what constituted a positive test. If this is a useful test then there should be wider availability and greater standardisation of testing.
P32 MODELLING THE ANNUAL NEED FOR LONG TERM OXYGEN THERAPY ASSESSMENTS AND AMBULATORY OXYGEN ASSESSMENTS FOR CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATIENTS IN LEEDS
M. Hewson1, P. K. Plant1, V. Walker2, M. T. Henry1. 1Department of Respiratory Medicine, Leeds Teaching Hosiptals NHS Trust; 2East Leeds PCT COPD team, UK
Introduction: Leeds is a city of 747 000 people served by five PCTS and one acute trust. The NICE COPD guidelines (2004) state that all patients with moderate to severe chronic obstructive pulmonary disease (COPD) should have an annual oxygen saturation measurement and those with an SpO2 <92% should have a long term oxygen therapy (LTOT) assessment. Similarly ambulatory patients who desaturate below 90% and by 4% should be considered for ambulatory oxygen. (BTS statement on home oxygen services 2004). From the Wyre valley data we have estimated that there are 6800 patients in Leeds with moderate to severe COPD, but do not know how many require oxygen assessments. 429 patients are currently on concentrators.
Aims: This study aimed to determine the number of LTOT and ambulatory assessments required on an annual basis in Leeds to facilitate service planning.
Methods: A community based pulmonary rehabilitation service has been run in the East Leeds PCT since the end of 2003 for patients referred from either primary or secondary care. The initial assessment includes resting SpO2 and an endurance shuttle walk test with continuous pulse oximetry. The initial SpO2 and minimum SPO2 are recorded. These data are maintained prospectively within a database. We identified the proportion of patients attending pulmonary rehabilitation with an SpO2 <92% and the proportion of patients who desaturated on exercise below 90% and by >4%. These data were used to model the need for oxygen assessments.
Results: 191 patients were identified on the database. 185 had a resting SpO2 recorded and 182 had full exercise data. 38/185, 21% (95% CI 15 to 26%) had a SPO2 <92%. 72/185, 40% (95% CI 32 to 47%) desaturated significantly on exercise. 25/38 patients with an SpO2 <92% also desaturated. Assuming that the PR cohort is typical of the Leeds population of moderate to severe COPD patients and that the 429 concentrator patients do not need a further assessment, 999 patients (95% CI 591 to 1339) require LTOT assessments per year. To be eligible for ambulatory oxygen, the patient must be mobile and leave the home regularly, such patients should undergo pulmonary rehabilitation before oxygen assessment. The Leeds COPD project aims to provide 1000 PR places per year. The need for ambulatory oxygen assessments is therefore 400 (95% CI 320 to 470) per year.
Conclusion: Leeds need to provide 1000 LTOT assessments per year and 400 ambulatory oxygen assessments per year to comply with the NICE and BTS guidance. This will require additional funding.
P33 CURRENT PATTERNS OF REPORTED OXYGEN USE AND ACTIVITY OF PATIENTS USING LONG TERM OXYGEN THERAPY VIA A CONCENTRATOR
C. Walker, C. Ward, M. Stern, L. Restrick. Department of Respiratory Medicine, Whittington Hospital, Highgate Hill, London, UK
Background: From 2006 it will be possible to prescribe ambulatory oxygen for patients on LTOT; Grade I, occasional use for those with low activity, and Grade 2, for those who are active and leave the home on a regular basis. The aim of this study was to assess the current pattern of activity and oxygen use by patients using LTOT to determine the likely number of patients who will need ambulatory oxygen assessment and may want to use ambulatory oxygen.
Methods: A telephone questionnaire was completed for 52/62 (84%) patients who had a concentrator in May 2005 and were known to the Whittington Hospital Respiratory Service. Clinical information was also obtained from the domiciliary oxygen record, if completed when the concentrator was prescribed (n = 31).
Results: The mean age of the 52 patients (33F; 19M) was 70 (range 40–94) years. The underlying diagnosis was COPD in 34/52 (65%); unknown diagnosis (9), obstructive sleep apnoea (4), interstitial lung disease (3), pulmonary hypertension (1), sickle cell anaemia (1). The median (range) MRC dyspnoea score (MRC) was 4 (2–5), with 23 patients MRC 4 and 24 patients MRC 5. 14/52 (27%) had attended, or been referred to, pulmonary rehabilitation (PR). Mean (SD) FEV1 was 0.96 (0.45) l, FVC was 1.48 (0.63) l (n = 27/52), mean (range) SaO2 on air was 83 (75–96) % (n = 31/52) and mean PaO2 on air was 8.1 (1.55) kPa (n = 21/52). 16/52 patients used LTOT continuously. 41/52 (79%) of patients said they go out. Of these, 16/41 (39%) go out every day and 30/41 (75%) go out at least twice a week. A further eight go out once/week. Eleven patients were housebound and three went out 1–2 times per month. The median (range) duration they go out for is 1–2 (0.5–8) hours. 20/41 walk when out; five use public transport, six drive, five are driven, seven are pushed in a wheelchair, and four have powered wheelchairs/buggies. 23/52 (44%) have an oxygen cylinder other than the back-up cylinder; used when going out by 19 patients and at home by three. The median (range) reported cylinder use was 2 (0–6) per month. 37/52 (71%) patients would like to go out more; 25/37 (68%) cited breathlessness and eight (22%) mobility as limiting factors and 19 already have a cylinder.
Conclusion: Of these 52 patients on LTOT, most have severe COPD. However, more than half still go out at least twice a week and more then two thirds would like to go out more but are limited by breathlessness. Very few have had PR. Based on these data a high number (about 73%) of patients on LTOT would need to be assessed for active (Grade 2) ambulatory oxygen and about 6% would be prescribed ambulatory oxygen in a low activity (Grade 1) group. Being able to prescribe ambulatory oxygen offers an opportunity to improve the quality of life of hypoxic, breathless patients particularly if they are also offered PR, which had previously only been offered to a quarter of this group of patients on LTOT.
P34 VALUE OF AN OXYGEN REGISTER IN IDENTIFYING PATIENTS ELIGIBLE TO RECEIVE LONG TERM OXYGEN THERAPY IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE
S. Ambalavanan, D. Moloney, J. F. Miles, D. C. Weir, S. P. Hanley. North Manchester General Hospital, Manchester, UK
Background: Domiciliary long term oxygen therapy (LTOT), is an established treatment in chronic obstructive pulmonary disease (COPD). Early identification of this subset of patients is difficult, patients usually being identified opportunistically in the inpatient (IP) and outpatient (OP) settings. We were interested in exploring alternative methods of identifying potential LTOT candidates.
Methods: In 1997, an oxygen recall register was set up at North Manchester General Hospital for patients with COPD with a PaO2 (on air) between 60–66 mm Hg in the IP or OP setting. Patients were invited for repeat annual capillary blood gas (CBG). If the PaO2 fell to <55 mm Hg or <60 mm Hg, the clinician was notified and prescription of LTOT (<55 mm Hg) or further assessment (<60 mm Hg) advised.
Results: The results of the register are presented for the period 1997 to 2004. Annual CBG was not always achieved on exact expected dates due to problems with staff shortages, exacerbations of COPD, and patients’ requests for deferment.
A total of 194 patients (range of age 50–91, mean 73 years) have thus far been included in the register. The duration of follow up is 0.0–6.6 years. 36 patients have died during the follow up period and 20 patients were removed from the register as follows: (a) repeat PaO2>70, n = −12; (b) patients failed to attend, n = 4; (c) patient moved areas, n = 2; (d) patient’s request, n = 1; (e) unable to attend, n = 1. The table indicates the duration of surveillance for the patients included in the register for the period 0.0–6.6 years. Twenty seven patients (13.9%) were identified to have a level of PaO2<55 mm Hg: all were referred to the clinician for further assessment. Seventy nine (40.7%) patients had a PaO2 of 55–59 mm Hg: these patients were referred to the clinician with advice to look for additional features which might qualify the patient for LTOT—for example, pulmonary hypertension. In total, from both groups 35 (18%) patients were prescribed LTOT.
Abstract P34
Conclusions: In a COPD patient subset identified by a PaO2 of 60–66 mm Hg, 35 (18%) were prescribed LTOT within a period of seven years. If early introduction of LTOT is beneficial to patients, then a recall register based on annual cycle seems an effective method of identifying patients. Community screening using pulse oximetry may offer an effective gateway to the entry on to the register.
P35 THE EFFECT OF AMBULATORY OXYGEN IN PATIENTS DURING PULMONARY REHABILITATION
F. Gray1, A. Smith2, C. Coombs1, M. Britton2, J. Bott1. North Surrey Therapy Services1, Ashford & St Peter’s Hospital NHS Trust2, UK
Introduction: UK Royal College of Physicians Guidelines (RCPG), 1999, suggest criteria for the assessment and provision of ambulatory oxygen (AO2). However, the evidence on oxygen (O2) use during pulmonary rehabilitation (PR) is unclear and, in practice, few centres use it widely in the UK. We have followed the RCPG and report our Endurance Shuttle Walk Test (EWST) and dropout data.
Method: All patients attending PR were assessed for AO2 according to RCPG, using the ESWT. Patients were divided into groups depending on O2 requirements.
Results: n = 149. 57 (38%) were eligible for AO2 assessment. 44 (77%) of these met criteria for prescription. (30% of n = 149). % dropout was 34, 31, 23, and 6 respectively (see table 1). Table 2 shows median change in ESWT for all patients completing PR.
Abstract P35, table 1: Patients and % completed by O2 group
Abstract P35, table 2: Post PR median (range) change in ESWT by O2 group
Conclusion: Dropout was lower in O2 users, who also had the greatest change in ESWT from baseline to post PR.
P36 CLOSING THE LOOP: AN ONGOING AUDIT OF THE PRESCRIPTION AND FOLLOW UP OF PATIENTS RECEIVING LONG TERM OXYGEN THERAPY IN SOUTH DEVON
M. George, H. Chaytor, L. Dobson, J. M. Goldman, D. G. Sinclair. Heart Lung Unit, Torbay Hospital, Torquay TQ2 7AA, UK
The Royal College of Physicians (RCP) publication in 1999, Domiciliary oxygen therapy services: clinical guidelines and advice for prescribers, presented guidelines for the prescription and follow up for patients receiving long term oxygen therapy (LTOT). We have undertaken an audit of the provision of LTOT within our service against these guidelines in 2001 and 2005.
The 2001 audit found 101 adult patients to be receiving LTOT, 53 (52%) of whom were known to the respiratory medicine service and 48 (48%) were not. Audit of those patients known to us largely demonstrated adherence to the RCP guideline. The general practitioner was contacted for those patients not known to our service to determine the reason for the prescription of LTOT. Thirty nine patients had been commenced on LTOT by a hospital service in another part of the country and subsequently moved and were lost to follow up. Nine patients had been prescribed LTOT by their general practitioner with no prior measurement of oxygen requirements. None of these 48 patients were receiving regular follow up or measurement of oxygen and carbon dioxide tensions.
In 2005, having improved our links with the LTOT supplier and undertaken a local programme of education for general practitioners and practice nurses, a second audit was undertaken to determine if the prescription and follow up of LTOT for patients had improved. On this occasion we identified 154 adult patients, an increase of 52%, receiving LTOT. The results of a formal assessment demonstrating the requirement for LTOT, as described in the RCP guideline was available for 145 (94%) patients. Regular follow up, as suggested by the guideline, was also in place for 142 (92%) patients of the 2005 cohort.
From the above we have drawn the following conclusions:
-
The standards laid down by the RCP guideline for the provision of LTOT and subsequent specialist follow up can be met.
-
A community wide programme of education within primary care may increase demand for the provision of LTOT but also leads to a greater recognition of the need for formal assessment before the prescription of LTOT.
-
Close links with the local LTOT supplier are clearly advantageous in maintaining a current database of patients. This is particularly relevant given the current contractual changes being led by the Department of Health for the provision of domiciliary oxygen services.
P37 OXYGEN PRESCRIPTION BY TARGET SATURATION: RESULTS OF A PILOT PROJECT
R. Smith, N. Linaker, R. J. Bright-Thomas, E. Myers, B. R. O’Driscoll, P. M. Turkington. Department of Respiratory Medicine, Hope Hospital, Salford M6 8HD, UK
Introduction: Oxygen is a drug and requires prescription; inappropriate dosage can be dangerous and potentially lethal, especially in COPD patients. It is recognised that oxygen therapy is poorly prescribed by doctors (
). Further work by
) highlighted that an oxygen prescription chart, combined with education, improved the quality of oxygen prescriptions. We introduced an oxygen prescription chart in 2001, but the effect was modest and short lived (see table).
Abstract P37
Methods: In 2005, Salford Royal Hospitals NHS Trust introduced a policy that all oxygen must be prescribed (except for the immediate treatment of life threatening emergencies). A multidisciplinary team was established to ensure that this could be achieved and to develop a new system of prescribing and titrating oxygen.
) a method was developed using desired outcome via target saturations, rather than just mode of delivery and prescription of a fixed percentage. Guidelines and an oxygen prescription sticker for the drug chart were developed and the new system was introduced on two respiratory and two non-respiratory wards. 71 patients were audited over a two week period.
Results: See table.
Conclusions: The insistence that oxygen must be prescribed and the use of a target saturation system of prescribing greatly improved the prescription of oxygen. The vast majority (74%) of patients had oxygen prescribed, were placed within an appropriate target saturation range, and maintained within this range for as long as they received oxygen therapy. This system is now being introduced on all wards in this hospital.
P38 AN AUDIT OF LONG TERM OXYGEN THERAPY IN WOLVERHAMPTON: IMPLICATIONS FOR THE NEW OXYGEN GUIDELINES
J. R. Feary, J. Crutchley, L. J. Dowson. New Cross Hospital, Royal Wolverhampton Hospitals NHS Trust, Wolverhampton WV10 0QP, UK
Introduction: From October 2005, a new modernised domiciliary oxygen service will be introduced in England and Wales. Following this, with the exception of palliative care use, long term oxygen therapy (LTOT) will only be prescribed after respiratory specialist assessment and patients will be required to receive regular follow up. These changes will undoubtedly increase the burden of care for hospital respiratory services especially when the additional requirement for ambulatory oxygen assessment is also considered. The British Thoracic Society has recommended that respiratory physicians review local protocols in order to plan services. Local data have suggested a greater than average use of oxygen concentrators in the Wolverhampton PCT when compared with national data. The aim of this study was to attain more information about our local patient population receiving domiciliary oxygen, in order to plan services for respiratory patients in the future.
Methods: A list of all patients in the Wolverhampton area with domiciliary oxygen concentrators was acquired from the current supplier. Data on medical history, hospital admissions, and outpatient appointments were collated using the New Cross Hospital “patient activity services” system.
Results: 152 patients were identified as having home oxygen concentrators. Of these, 15 (10%) were from paediatric services and were discounted from further calculations. Of the 137 adult patients, 98 (72%) had undergone formal arterial blood gas (ABG) assessment in the lung function department. Of the 39 patients that had not received formal assessment, 18 had been seen in the last year by a respiratory consultant, three were under the care of an oncologist, and two had end stage heart failure. The 16 remaining patients were unknown to either respiratory or palliative care. In the preceding 12 months, 48 (35%) had not been seen in clinic and 86 (63%) patients had not had a hospital admission. A total of 35 (26%) patients had not been seen in an in- or outpatient setting over this time.
Discussion: Significant numbers of patients receiving oxygen therapy via a concentrator in Wolverhampton have not had a formal baseline assessment or regular follow up and as such fall short of the requirements of the new oxygen guidelines. This has significant resource implications for the respiratory service in Wolverhampton.
P39 RECOGNITION OF DIFFERENT OXYGEN DELIVERY SYSTEMS FOR DIFFERENT CLINICAL SCENARIOS BY HEALTHCARE PROFESSIONALS
T. Naresh1, J. A. Annandale1, B. Ramman1, K. E. Lewis1,2. 1Respiratory Unit, Prince Philip Hospital, Llanelli; 2Swansea School of Medicine, Wales, UK
Introduction: Oxygen (O2) should be delivered with different flow rates and systems, according to the clinical situation. Even if prescribed correctly, mistakes may happen in actually applying the correct oxygen delivery system. We wanted to not only test the theoretical knowledge on O2 prescription but also whether health professionals recognised the different types/colours of masks, recommended in our Trust, for different types of O2 prescriptions.
Methods: Cross sectional interview of 22 junior doctors (12 medical, 10 AE) and 62 nurses (24 medical, 38 surgical), of all grades in our Trust.
Abstract P39
All subjects were given three scenarios relating to oxygen saturations (SpO2) on air of:
-
Young adult with acute severe asthma, “Type I respiratory failure” (SpO290%)
-
Elderly, heavy smoker, with borderline “Type 2 respiratory failure” (SpO2 88%)
-
Collapsed young adult with arrhythmia and poor cardiac output (SpO2 unrecordable)
Subjects were asked to choose the most appropriate, initial O2 delivery system from colour photographs of: nasal prongs, rebreathing mask, blue venturi mask (that is, 24% O2), white venturi mask (that is, 28% O2) and a green venturi mask (that is, 60% O2). No subject refused participation.
Results: Table shows that most health professionals chose rebreather mask for asthma but 76% chose the correct mask (24–28% O2) for COPD and 85% correctly chose the rebreather system for initial oxygenation for peri-arrest.
Conclusions: Most doctors and nurses either do not know that 40–60% oxygen is recommended for asthma1 or do not recognise its delivery system. Most knew the recommended dose, and recognised the correct oxygen delivery systems for likely COPD and for peri-arrest.
1
Pulmonary rehabilitation
P40 DOES BODY MASS INDEX INFLUENCE THE OUTCOME OF PULMONARY REHABILITATION IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE?
R. A. Evans, M. E. Hall, M. C. Steiner, M. D. L. Morgan, S. J. Singh. Pulmonary Rehabilitation, Glenfield Hospital, University Hospitals of Leicester NHS Trust, Leicester UK
Introduction: Patients with COPD are a heterogenous population including both obese and cachectic patients. Our pulmonary rehabilitation programme involves predominantly endurance walking exercises, which could be influenced by weight. We investigated whether body mass index (BMI) influenced the Incremental Shuttle Walk Test (ISWT) performance and whether it affected the outcome of pulmonary rehabilitation.
Methods: We retrospectively analysed data from 395 patients; 220 male, mean (SD) age 69.3 years (9.0), FEV1 1.05 (SD 0.48) l, BMI 26.5 (5.8), ISWT 176 (112) m. All patients underwent a seven week course of pulmonary rehabilitation and performed an ISWT before and after.
Results: Complete data were available in 358 patients. Patients were divided into five groups according to BMI shown with the baseline ISWT performance, shown in the table.
There was no significant difference in baseline ISWT distance overall by ANOVA p = 0.126. However, post hoc analysis correcting for multiple comparisons with LSD showed the obese group had a significantly lower ISWT performance than the overweight and normal weight patients −41 m, p = 0.045 and −34 m, p = 0.009 respectively. The mean (95% CI) improvement in ISWT with rehabilitation for each group was Group 1 = 72 (50–94) m, Group 2 = 62 (51–72) m, Group 3 = 57 (49–65) m, Group 4 = 66 (52–81) m, and Group 5 = 45 (17–73) m. There was no statistical difference in the change in ISWT between the groups by ANOVA p = 0.485 or with post hoc analysis. Very obese patients appeared to do less well but this was a small group.
Abstract P40
Conclusion: Over half of this COPD population were overweight. Obese patients seem to have a lower ISWT performance. This does not appear to affect the outcome of pulmonary rehabilitation in terms of exercise capacity.
P41 IS OUTCOME IN PUMONARY REHABILITATION RELATED TO BODY MASS INDEX?
D. J. Ross, K. Darbyshire, R. Johnson, C. Geach, F. Haas, M. Russell, R. Roberts, N. Gohl, A. Barnes. St Richard’s Hospital, Chichester, UK
Pulmonary rehabilitation is an effective treatment in chronic lung disease. It has been observed that patients with low BMI have lost weight and have not gained the same physiological benefits as those with normal or raised BMI (
).
We analysed the data for 53 patients who had attended our pulmonary rehabilitation programme in 2003–04. Patients were classified on the basis of their BMI as low (BMI<21), normal (BMI 21–25), overweight (BMI 26–30), or obese (BMI >30). We compared changes in status before and at the end of a programme. We used the following tools including the Medical Research Council dyspnoea scale (MRC) and the hospital anxiety and depression score (HAD). Statistical analysis was using Wilcoxon paired analysis, except for BMI and shuttle where t test was used. The table shows the change outcomes for each group.
Our low weight patients put on weight, as did our overweight patients (though obese ones lost weight). However, changes in MRC scale, and HAD scores were lower than for others, and obese patients appeared to gain the greatest health status benefit. Interestingly, they appeared to gain as least as much physiological benefit with greater reduction in Borg score. Underweight and obese patients appear to gain different benefits from pulmonary rehabilitation and may have different requirements within pulmonary rehabilitation.
Abstract P41
P42 EVALUATION OF AN ACTIVITY MANAGEMENT (BETTER BREATHING) CLINIC RUN BY OCCUPATIONAL THERAPY FOR PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
C. Elliott, M. Bone. South Tyneside Foundation Healthcare Trust, UK
As part of a structured occupational therapy (OT) intervention in our Acute Respiratory Assessment Service (ARAS), we have been running activity management (Better Breathing) clinics for patients admitted to hospital with acute exacerbations of COPD. Following assessment and provision of individual equipment aids patients were invited to attend an hour long clinic held on the respiratory ward over two successive weeks. Interventions included pacing, breathing exercises, anxiety management, and relaxation techniques. Patients were provided with a tape to practice breathing exercises and reinforce relaxation techniques. Domiciliary follow up visits by the therapist were carried out on individual need. We evaluated the effectiveness of this intervention by means of the Leicester Chronic Respiratory Questionaire-self reported (CRQrq) in a random sample of 50 of the 73 patients who had attended the clinic following its inception. The CRQ-SR is divided into four dimensions: dyspnoea, fatigue, emotional function, and mastery. 32 completed forms were returned. Of the 118 completed scores that could be compared, 99 results showed an increase in performance, while 19 showed a decrease. The latter was predominantly in male patients. These were broken down into Dyspnoea, 1 (of 21); Fatigue, 5 (of 32); Emotional function, 4 (of 32); and Mastery, 8 (out of 33). The collective scores and mean for each area are shown in the table.
Abstract P42
This illustrates an overall marked improvement in coping ability with an efficient use of targeted staff resources. In this selected group of patients with severe COPD and frequent hospital admission, intercurrent exacerbations may have contributed to functional decline seen in some patients. However sociocultural influences may be important, with gender particularly affecting emotional coping with breathlessness and mastery in men, which may have implications for specific therapeutic intervention in the future.
P43 DOES A PHYSIOTHERAPIST LED COMMUNITY BASED DISEASE MANAGEMENT PROGRAMME IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATIENTS AFFECT HOSPITAL ADMISSIONS WITH ACUTE EXACERBATIONS?
S. Pushparajah1, R. McClellan2, A. Henry2, L. M. E. Kuitert1. 1Department of Respiratory Medicine, Royal London Hospital, Barts and the London NHS Trust; 2Department of Physiotherapy, Tower Hamlets Primary Care Trust, London, UK
Background: Management of chronic obstructive pulmonary disease (COPD) in the community is often unsatisfactory and may contribute to morbidity and readmission with acute exacerbations. Use of physiotherapists trained to advise, educate, and review medication, social needs and chronic managment has not been evaluated.
Aim: To determine if a physiotherapist led community based COPD management intervention would reduce hospital admissions, total days hospitalised and/or reduce length of stay (LOS).
Methods: Patients identified during an (index) admission with an exacerbation of COPD were assessed just before discharge and had immediate follow up at home by the physiotherapist. They received up to three sessions which covered education regarding the disease, airways clearance, breathing exercises, exercise tolerance, and a medication/inhaler technique/equipment review. Data were collected on admission frequency, total days hospitalised, and LOS (52 weeks before and after the index admission), FEV1, MRC, and Borg scores, oxygen use, and smoking status.
Results: Between 2000–02, 255 patients were referred. 109 were excluded (not COPD/out of area/deceased during the index admission). 51 did not receive the intervention (discharged before full assessment/inadequate contact details for follow up). 95 patients received the intervention; data were available on 80. Median age was 73 years (46% male), median FEV1 0.86 l (39% predicted), MRC and Borg scores were 4. 54% lived alone; 90% smoked ever; 30% used oxygen; 51% had nebulisers. 21% had COPD as the only significant medical diagnosis and 46% had pre-existing cardiac morbidity. Overall there was no change in LOS for all 80 patients (median 8.0 days) or admission frequency (median 0). However total days hospitalised for COPD fell by 15% from 820 to 697 days. In the more severe patients with previous admissions (n = 27; median FEV1 0.58 l, 30% predicted), admission frequency fell from 2 to 1, total hospitalisation days fell by 33% from 820 to 551 days, and median time interval to next hospitalised exacerbation increased by 23% (from 62 to 76 days). 59% had preventable medication errors (using inhalers and tablets irregularly or not at all) due to poor knowledge and understanding of medications prescribed. Inadequate discharge planning was rectified in 29% of patients who needed further input by other health professionals.
Conclusion: A community based COPD intervention for patients with moderate to severe disease admitted with an exacerbation does not affect LOS. In more severe patients it can reduce frequency of exacerbations requiring hospital admission, total hospitalised days, and increase the time interval to next hospitalised exacerbation.
P44 OCCUPATIONAL THERAPY INTERVENTION IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE
C. Elliott, M. Bone. South Tyneside Foundation Healthcare Trust, UK
Although it is widely recognised that activities of daily living (ADL) are often severely affected in COPD, the role of occupational therapy (OT) has received scant mention. We have recently evaluated an acute assessment and intervention programme run by OT in our local respiratory ward setting. Equipment used included aids for bodily functions, dressing and bathing, settee raisers, bed levers, “Helping Hand”, and perching stools, as well as the obvious mobility aids. Although prescribed, they were not necessarily the predominant therapeutic intervention which included energy conservation (relaxation and pacing), education (for example, intermittent oxygen usage), and coping techniques with goal setting and activity analysis, anxiety management, and breathing techniques. Of 204 patients referred in the first year, 168 were assessed; 14 having died before contact; four having declined contact; and 18 electing for community referral. Of the 168, interventions comprised Activity management (Better Breathing) clinic (73), community intervention (95), equipment (117), bathing aids (40), environmental assessment and intervention (58), Pacing (19), anxiety management (29), and relaxation therapy (27). Qualitative feedback forms were returned in 44 of 50 patients randomly selected as part of an audit project into the effectiveness of the Better Breathing clinic. Results indicated high levels of patient satisfaction.
These results illustrate the effect that a structured OT intervention can play in the care of patients with COPD and support an increasing role for OT in the management of one of the most chronic and debilitating diseases in Britain today.
Abstract P44
P45 IS LONGER BETTER? A COMPARISON OF SIX AND EIGHT WEEK COMMUNITY OUTPATIENT PULMONARY REHABILITATION PROGRAMMES
A. Sarjeant, C. Mackinlay. Great Western Hospital, Swindon & Marlborough NHS Trust, Swindon, UK
Introduction: Pulmonary rehabilitation has an established role in the management of patients with chronic obstructive pulmonary disease and randomised controlled trials have shown lasting improvements in both health status and exercise capacity. Recent evidence has suggested improved outcomes with increased duration of course (Moore et al 2004). Swindon has been running rehab courses for over three years and due to increased demand for places, a six week course has been introduced and outcomes compared with the earlier eight week course.
Methods: The study retrospectively audited the outcome measures of two six and two eight week courses and whether the shorter course provided equal benefits to patients in terms of health status, as measured by the Chronic Respiratory Questionnaire (CRQ), the London Chest Activity of Daily Living (LCADL), and exercise capacity using the standardised incremental shuttle walking test (ISWT).
Results: There were 21 patients in each group. Average age was 69.19 in the six week group and 69.2 in the eight week group. Pre rehab lung function was comparable (FEV1 = 0.96 (6 week) and 1.187 (8 week)). Pre rehab ISWT was 171.14 m in the six week group and 167.14 m in the eight week group. In both groups 85.7% of patients completed the programme allowing their post-rehab data to be collated. Exercise tolerance: an improvement of 50 m or more is considered clinically significant using ISWT. FEV1 did not change significantly.
Abstract P45, table 1
Abstract P45, table 2
Conclusion: Ours is a small retrospective study that has shown improvements in health status and exercise tolerance in both six and eight week pulmonary rehabilitation courses. The shorter programme was as good if not better than the longer programme, adding to the debate in the literature about the optimal length of pulmonary rehabilitation.
P46 FACTORS ASSOCIATED WITH SUCCESS AND FAILURE OF PULMONARY REHABILITATION
R. Garrod1, J. Marshall1, E. Barley2, V. Pomeroy3, P. Jones2. 1School of Physiotherapy, St George’s University of London & Kingston University; 2Respiratory Medicine, St George’s University of London; 3Centre for Rehabilitation and Ageing, St George’s University of London, UK
Aim: The purpose of this study is to identify prognostic features of COPD associated with success or failure in pulmonary rehabilitation. Patients from all grades of the MRC dyspnoea grade were recruited.
Methods: Seventy four patients with stable COPD were entered, mean age (SD) 68 (10 years), 21 MRC Grade 1/2; 29 Grade 3/4, 24 grade 5. Mean (SD) FEV1 1.10 (0.6) l. Patients attended rehabilitation, twice weekly for seven weeks. Assessments were Quadriceps Muscle Strength, 6-Minute Walking Distance (6MWD), Brief Assessment Depression Cards (BASDEC), and St George’s Hospital Respiratory Questionnaire (SGRQ). Relations between variables were tested using Pearson’s r. Predictors of dropout and of response (defined as clinically significant benefit in SGRQ (4 points) or 6MWD (54 m)) were then tested using binary logistic regression. Differences between patients according to MRC Grade were tested using one way ANOVA.
Results: 51 patients completed 10 or more sessions. Thirty nine (77%) patients showed clinically significant benefit in either 6MWD or SGRQ. None of the baseline variables were predictors of response (logistic regression, p>0.05). Significant differences were seen between MRC groups for change in 6MWD and SGRQ total after controlling for baseline 6MWD and SGRQ (GLM main effect p<0.0001, effect of MRC on 6MWD p = 0.003, on SGRQ p = 0.03). Post hoc analyses showed that only the Grade 1/2, and 3/4 patients improved in these outcomes (see table). Three variables showed an association with dropout, less quadriceps strength (p = 0.009), more pack years (p = 0.03), and being more depressed (p = 0.004). Depression was a risk factor for dropout compared with non-depressed (odds ratio 8.7, CI 2.8 to 27.1).
Abstract P46
Conclusions: Baseline variables are poor predictors of response to pulmonary rehabilitation. However, Grade 1, 2, 3, and 4 patients achieve significant benefit while grade 5 patients show smaller magnitudes of improvement. Depression is a risk factor for dropout.
This study is generously funded by the Health Foundation.
P47 THE EFFECT OF ANXIETY AND DEPRESSION ON THE BENEFITS OF PULMONARY REHABILITATION IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE
C. Potter1, H. Broomfield1, L. Restrick2, M. Stern2. 1Department of Physiotherapy, REDS/CRS Team, Whittington Hospital, London, UK; 2Department of Respiratory Medicine, Whittington Hospital, London, UK
Background: There is a high prevalence of anxiety and depression in patients with COPD (Manen et al, 2002), contributing to increased hospital admissions and use of hospital resources (Yohannes et al, 2000). While pulmonary rehabilitation (PR) programmes including psychological interventions may improve these symptoms (de Godoy et al, 2003), most programmes do not include a specific psychological component. Further, anxiety and depression may affect patients’ ability to complete PR. In this study, the effect of anxiety and depression on the outcome of PR and also the effect of PR on levels of anxiety and depression were investigated.
Method: Patients with stable, severe COPD (mean FEV1 0.9 (SEM 0.1) l; n = 52) referred for PR over a 12 month period were studied. Data, including FEV1, MRC Dyspnoea Score (MRCDS), Hospital Anxiety and Depression Scores (HADS, pre, immediately post PR, and 4–12 months later), smoking status, living status, number of hospital admissions, and use of the Chronic Respiratory Support team (CRS), were analysed retrospectively.
Results: 50% of these patients (n = 26) did not complete the PR course. This group had higher levels of anxiety and significantly (p = 0.02) higher levels of depression. Compared to patients who completed PR who had HADS of 7.5 (SEM 0.6) (anxiety) and 6.3 (SEM 0.3) (depression) respectively, the group of patients who did not complete PR had scores of 9.3 (SEM 0.9) and 8.3 (SEM 0.7) respectively. In the latter group, there were also a significantly (p = 0.04) higher number of current smokers (n = 12) compared with the group who completed PR (n = 5) and a higher number who lived alone (n = 10 v n = 4). There was no significant difference in disease severity between the group of patients who completed PR (FEV1 0.8 (SEM 0.1) l, MRCDS 3.8 (SEM 0.2)) and those who did not (FEV1 0.9 (SEM 0.1) l; MRCDS 3.8 (SEM 0.1)). However, the latter group went on to have a significantly higher (p<0.001) number of admissions to hospital in that year (42%, n = 11, had two or more admissions compared with 4%, n = 1 in the group who completed PR) and were more likely (46%, n = 12) to require support from CRS compared to patients who completed PR (15%, n = 4). For those patients who completed PR, HADS scores decreased by 1.4 SEM 0.6) for anxiety and 0.3 (SEM 0.7) for depression by the end of PR, but this small improvement was not sustained. When re-measured 4–12 months following PR, 74% of 23 patients who completed the follow up HADS questionnaire were more anxious and 56% were more depressed than at the end of PR.
Conclusion: These data suggest that specific, targeted psychological intervention should be included both throughout PR as well as part of follow up, including CRS. This strategy may optimise and sustain the beneficial effect of PR on mood disturbance. It may also improve completion rates for PR, facilitate and support smoking cessation, and prevent at least some of the excess hospital admission rates associated with the group of patients who do not complete PR.
P48 AN ANXIETY MANAGEMENT PROGRAMME FOR PATIENTS WITH SEVERE OBSTRUCTIVE AIRWAYS DISEASE
C. Woods, A. Fennerty. Harrogate District Foundation Trust
Anxiety and depression contribute significantly to the disability of many patients with severe obstructive airways disease. We have developed an anxiety management programme run by an occupational therapist with skills in cognitive behavioral therapy and neurolinguistic programming.
Patients are referred to the programme via the weekly respiratory team meeting where difficult cases are discussed. The criteria for referral are that patients should be on optimal bronchodilator therapy, have completed, failed, or were not deemed suitable for a rehabilitation programme, and anxiety is thought to contribute significantly to their disability. Patients are seen in their home and a full assessment is made, identifying any specific functional problems requiring adaptations or equipment, and realistic goals established for the programme. Outcome for the anxiety management is assessed using the Hospital Anxiety Depression scale (HAD).
Forty one patients have been through the programme, 35 with severe COPD and six with asthma. Patients were seen for a mean of four visits (range 2–9) lasting 1–1.5 hours each, the number of sessions depending on individual need.
The mean anxiety HAD score fell by 45%, from 11.4 to 6.8, mean reduction 5.08 (4.19–5.96) (p<0.001). Twenty four (58%) were scored as having moderate or severe anxiety, 12 as mild anxiety, and 12 were in the normal range. Twenty of the 24 patients originally in the moderate or severe range were in the mild or normal range at the end of the programme.
The mean reduction in the depression HAD score was 35% from 9.4 to 5.9, mean reduction 3.25 (2.81–4.12) (p<0.001). Seventeen (42%) of the patients were scored as having moderate or severe depression, 12 as mild depression, and 12 were in the normal range. Sixteen of the 17 patients originally scored in the moderate or severe range were in the mild or normal range at the end of the programme.
While the provision of psychological input into the management of chronic disease is thought to be important access to these services is poor. This work shows that an occupational therapist can acquire skills which can have a demonstrable impact on levels of anxiety and depression in a group of patients with severe airways disease. We do not currently have objective data on how this programme impacts on activities of daily living or quality of life and some ongoing work suggests that the benefits decline with time.
P49 HOSPITAL READMISSION FROM A RESPIRATORY OUTREACH SERVICE AND DISCHARGE CRITERIA
F. Chang, S. Robinson, P. Brammer. Department of Respiratory Medicine, Russells Hall Hospital, Dudley, West Midlands DY1 2HQ, UK
The Dudley Respiratory Assessment Service formed in 2002, provides early discharge from hospital for patients with respiratory conditions. The British Thoracic Society’s Guidelines for the management of patients with chronic obstructive pulmonary disease (1997) have been used as part of the criteria for acceptance of patients on to the service. This audit has been carried out in order to identify if patients are more likely to be readmitted to hospital if they are taken on to the service outside the BTS guidelines. The sample group consisted of 99 patients taken on to the service with a diagnosis of COPD, 61 from December 2003, and 38 from July 2004. Summer and winter months were used to compare if readmission was greater due to seasonal influences. A quantitative analysis of patient data was used to gather statistical information from a non-probability sample, the variables being 13 criteria from the BTS guidelines. Twenty six per cent of the sample group were readmitted within three months. Ten patients were readmitted from the summer group (26.3%) and 16 from the winter group (26.2%). There was no significant difference in readmission rate between summer and winter patients. Of those readmitted, 17 of 26 had at least one measurement outside the criteria. Of those not readmitted, 29 out of 63 had one measure outside the criteria. So, those readmitted were satistically more likely to have one measure outside the criteria χ2 = 5.6 (p<0.05). Those that were more likely to be readmitted were patients with a PcCO2<6.5. Of those readmitted six out of 22 did not fulfil this criteria compared to three out of 63 of those not readmitted, χ2 = 8.7, (p<0.01) and pulse rate <110, where two out of 25 of those readmitted did not fulfil this criteria compared with none of the 73 patients who were not readmitted, χ2 = 5.9, (p = 0.02). For some criteria those being respiratory rate, temperature and pH, only one out of the 99 patients was sent home so no meaningful statistics could be done on these. For other variables (comorbidity, PaO2, new changes on the x ray, social support at home, and the presence of a telephone at home) there was no statistical difference between those readmitted and those not, as far as BTS criteria were concerned.
From our limited data it would appear that those that fulfil all the criteria are less likely to be readmitted than those that do not but some criteria (pulse and CO2) are more useful than others. Therefore we would suggest the importance of the other criteria are examined further as far as the risk of readmission is concerned.
P50 DROPOUTS FROM A PULMONARY REHABILITATION PROGRAMME
R. Carpenter, T. Cadwallader, M. J. Doherty. Department of Respiratory Medicine, Russells Hall Hospital, Dudley, West Midlands, UK
Pulmonary rehabilitation is of proven benefit in patients with chronic lung disease. Guidelines suggest all suitable patients should be offered this beneficial treatment. In our pulmonary rehabilitation programme we have found patients often refuse to participate and even if they initially agree to rehabilitation a large proportion then drop out during the treatment. Eighty five patients started the programme, 52 completed it, 17 dropped out because of illness, that is two consecutive missed visits because of a documented exacerbation, and 16 for “other” reasons, that is failure to turn up twice in a row for other reasons not related to an exacerbation or not giving a reason at all. We compared these three groups in terms of baseline demographics, functional status, and quality of life. Those who dropped out because of illness were younger (63 (9) v 68 (9) years, (p = 0.035)) and had worse baseline exercise tolerance (SWT) 137 (87) v 169 (113) m, (p = 0.026), than those who completed the programme. However, the two groups did not vary in terms of continued smoking, one of 17 versus six of 52, sex, % predicted FEV1 40 (15) v 40 (14), (p>0.2), the hospital anxiety and depression score (HAD) 17 (9) v 15 (7) (p = 0.4) or health status as measured using the Chronic Respiratory Questionnaire (CRQ) 13.8 (4) v 14.8 (4) (p = 0.08).
Although those who dropped out for other reasons had a worse HAD score 18.9 (7) v 15 (7), (p = 0.015), this difference was significant in both domains, anxiety 9.8 (5) v 7.8 (3.9), (p = 0.05) and depression 9.1 (3) v 7.3 (3.8) (p = 0.01). They were also younger (61 (10) v 68 (9) years, (p = 0.008), they were more likely to be current smokers, eight of 16 v six of 52, and had a lower CRQ 13.2 (4) v 14.8 (4), (p = 0.01). They did not differ in terms of sex, % predicted FEV1 40 (13) v 40 (14) (p>0.2) or in terms of exercise tolerance 164.7 (96) v 169.4 (113), (p = 0.4).
In summary, patients who dropped out because of illness were functionally more impaired, whereas psychological and concordance problems seemed more important in those that dropped out for other reasons, suggesting that other treatment approaches might be needed in this subgroup if they can be successfully recognised before starting rehabilitation.
P51 REVIEWING SIX YEARS’ EXPERIENCE OF PULMONARY REHABILITATION AT THE ROYAL VICTORIA INFIRMARY
S. M. Bianchi, E. Yapp, K. Heslop, A. Anderson, L. Whalen, K. E. Stavers, G. P. Burns. Department of Respiratory Medicine, Royal Victoria Infirmary, Newcastle-upon-Tyne, UK
Introduction: Pulmonary rehabilitation has been demonstrated to improve quality of life and exercise tolerance in patients with COPD. Assessing success or failure of pulmonary rehabilitation programmes is problematic due to variation in programme constituents, referral criteria, and heterogeneity in COPD populations. Several standards, such as increase in 6 minute walk distance (6MWD) by 54 m or increases in St George’s Respiratory Questionnaire (SGRQ) scores by more than 4 points, have been suggested as suitable tools for assessing impact of rehabilitation programmes. The Royal Victoria Infirmary Chest Clinic has offered a 10 week pulmonary rehabilitation programme for more than six years, incorporating elements of education, exercise, and psychosocial support.
Methods: To assess outcome of the programme patients had 6MWD, Borg dyspnoea scoring and quality of life (QOL) assessments conducted before and immediately after the 10 week programme. QOL was assessed using a 10 point questionnaire derived from the SGRQ, with a maximum achievable score of 41 points. Admission data for COPD exacerbations were collected for the 12 months before and after the completion of the programme. Baseline data of age, sex, resting heart rate, body mass index, and FEV1 were collected.
Results: Mean 6MWD showed a statistically significant increase from 225.4 (SD 9.7) m to 272.3 (SD 9.91) m over the 10 weeks. Few patients achieved the 54 m improvement suggested by other authors. Review of the histograms of walking distance demonstrates normally distributed pre and post-rehabilitation values, with all groups showing improvements in exercise capacity. We suggest that proportional increases in individual patient’s performance may be a more suitable tool for assessing outcome. Mean percentage increase in walking distance for each patient was 30.9 (SD 4.1) %. Dyspnoea was not increased despite increased exercise tolerance. QOL scores were increased by a mean value of 2.1 (SD 0.8) points (p = 0.01). This improvement correlated with improvements in 6MWD. In patients with FEV1 >1l (mean 1.38 (SD 0.08)) admissions were reduced by half and mean length of stay (LOS) by two thirds. In those with FEV1 <1l admissions and LOS were unchanged despite anticipated deteriorations in health status over the following 12 months.
Conclusions: Our experience suggests that pulmonary rehabilitation maintains or improves performance and health status in patients with COPD, especially in those with moderate disease. We suggest alternative tools, such as proportionate increases in exercise tolerance and a “quick to use” modified QOL questionnaire for assessing success of intervention in this heterogenous group of patients.
P52 THE RESPONSIVENESS OF THE LONDON CHEST ACTIVITY OF DAILY LIVING TO PULMONARY REHABILITATION
R. Carpenter, T. Cadwallader, M. J. Doherty. Department of Respiratory Medicine, Russells Hall Hospital, Dudley, West Midlands, UK
The LCADL (London Chest Activity of Daily Living Scale) is an outcome tool used to measure dyspnoea during daily activities in patients with chronic obstructive pulmonary disease (COPD). It has previously been shown to be reliable and responsive (
). When he used this measure as an assessment tool in our pulmonary rehabilitation programme we had the impression that it did not respond as we had expected it would. We therefore set out to examine this in more detail. Fifty two patients completed a standard eight week rehabilitation programme, mean age 67.5 (SD 9) years, mean % predicted FEV1 40 (SD 14), 70% were male and 90% had COPD. Before the rehabilitation programme the mean LCADL was 34.2 (SD 12) and post rehabilitation it was 33.8 (SD 14), there being no significant difference in this score (Student’s t test, p = 0.8). However, other standard outcome measures used in pulmonary rehabilitation did significantly change, shuttle walk test before rehabilitation was 169 (SD 113) m and 208 (SD 113) m after rehabilitation (p<0.001) and the Chronic Respiratory Questionnaire (CRQ) was 14.8 (SD 4) before rehabilitation and 16.2 (SD 4.2) and post rehabilitation again p<0.001. Neither did any of the individual domains for the LCADL improve with rehabilitation (see table).
Abstract P52
The lack of responsiveness in our patient group to those in the original study could be due to differences in the populations studies, though demographically they look similar, except that nearly 10% of our patients had a diagnosis other than COPD. In particular the prerehabilitation exercise tolerance of our group was almost identical to the group in the prior study by Garrod. We believe our population had difficulty understanding the questions and the appropriate answers, and were particularly confused around the questions in the Domestic Domain and the differences in the meanings between answers 0, 4, and 5.
Outcome of chronic obstructive pulmonary disease: patient factors
P53 IMPROVING EXACERBATION REPORTING BEHAVIOUR IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
T. M. A. Wilkinson, T. A. R. Seemungal, C. Dawson, W. Perera, J. R. Hurst, G. C. Donaldson, J. A. Wedzicha. Academic Unit of Respiratory Medicine, Royal Free Hospital and University College Medical School London, UK
Exacerbations of chronic obstructive pulmonary disease (COPD) adversely affect patients’ health status, contribute to disease progression, and are a major cause of hospitalisation. We have shown that COPD patients often do not seek treatment for a significant proportion of their exacerbations. These patients who fail to seek treatment are at greater risk of hospitalisation and have poorer health status than those with better exacerbation reporting behaviour (Wilkinson, Am J Respir Crit Care Med 2005). We studied whether the specific intervention of regular telephone calls to COPD patients by a nurse specialist could improve reporting exacerbation characteristics in a cohort of patients with COPD.
We studied 116 patients with COPD, mean age 70.5 (SD 24.5) years, FEV1 1.25 (SD 0.55) l, FEV1 % predicted 50.4 (SD 21.8) %. Patients completed daily diary cards of respiratory symptoms and were instructed to report exacerbations to the clinical study team or GP for treatment. Exacerbations were diagnosed using our previously published and well validated symptom based diagnostic criteria. In the first winter of the study (period 1: November 03 to February 04) patients were reviewed three monthly in the study clinic and at reported exacerbations, the cohort was followed through a second winter (period 2: November 04 to February 05) when patients were telephoned at home every two weeks by a respiratory nurse specialist, questioned about symptoms, and encouraged to attend the study clinic if an undiagnosed exacerbation was picked up.
116 COPD patients had 213 exacerbations during periods 1 and 2. The nurse lead intervention during period 2 was associated with an increased reporting rate of 61.7% compared to 45.8% in period 1, p = 0.027. Multivariate analysis showed that reporting rates were higher during exacerbations associated with increased dyspnoea (OR = 3.2, p = 0.009), sputum purulence (OR = 2.24, p = 0.008), increased cough (OR = 2.6, p = 0.002) and period 2 (OR = 2.02, p = 0.024). Over the two periods 31 (26%) patients reported a mean of 0.55 exacerbations more in period 2 (p = 0.002) and patients who reported less exacerbations in period 1 were more likely to have reported more exacerbations in period 2 (p = 0.010).
This study has shown that regular telephone contact with COPD patients can improve exacerbation reporting rates and could therefore potentially improve outcomes and reduce hospitalisation rates. Further studies of novel healthcare interventions are required in COPD.
P54 AUDIT OF NON-INVASIVE VENTILATION IN PATIENTS WITH SEVERE RESPIRATORY ACIDOSIS (PH <7.25): EFFECT OF SETTING
G. South, S. W. Crooks, J. Tague, R. Condliffe, J. W. Hadfield. Chesterfield Royal Hospital NHS Foundation Trust, UK
Introduction: Non-invasive ventilation (NIV) should be considered in all patients admitted to hospital with acute hypercapnic respiratory failure (AHRF). The BTS NIV Guidelines (
) suggest that patients receiving NIV with a presenting arterial pH<7.30 should be managed in a high dependency area (HDU or ITU). This is not always possible in our hospital which has high bed occupancy levels in these areas. By local protocol only those who are candidates for intubation are admitted to HDU, and the others receive NIV on a general Respiratory ward. We report the outcomes in these two settings of patients with AHRF with a pH<7.25 at the start of NIV.
Setting: General respiratory ward (RW) and high dependency unit of a district general hospital.
Method: Prospective audit of all admissions with persistent acute hypercapnic respiratory failure (AHRF) July 2004 to July 2005.
Results: From 66 patient episodes of NIV, there were 35 episodes (in 34 patients) with pH<7.25 before starting NIV. The outcomes in each setting are shown in the table.
No patients from HDU were intubated during the period of the audit. One was intubated before transfer to HDU (not included in table, failed NIV trial in emergency unit).
Conclusion: This audit suggests that NIV in the more severely acidotic patients can be safely delivered outside conventional high dependency areas. Reasons for the apparent differences between the units in outcome are not clear but may include the small size of the audit, greater staff familiarity with the technique on the respiratory ward, differences in case mix/comorbidity, and differences in the availability of junior doctors within each unit. Establishing a high dependency respiratory care area within the respiratory ward and accepting all patients for NIV to a single unit may overcome many of these problems.
Abstract P54
P55 THE TWO YEAR SURVIVAL FOR PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE WHO UNDERGO NON-INVASIVE VENTILATION FOR HYPERCAPNIC RESPIRATORY FAILURE
M. McCloskey, R. Sharkey, S. Gallagher, M. G. Kelly, J. G. Daly. Respiratory Unit, Altnagelvin Area Hospital, Londonderry, N Ireland
The outcome of patients with chronic obstructive pulmonary disease (COPD) who had non-invasive ventilation (NIV) for acute hypercapnic respiratory failure (HRF) was assessed two years after their initial admission. This was a retrospective chart audit and data from all patients who had NIV for HRF to this district hospital from April 2002 to April 2003 was assessed.
54 patients had NIV for HRF over the 12 month period. Data were available on 39 of these patients, 18 males, 21 females, mean age 75 years. 16 patients (41%, five male) died during the acute admission. All of these patients who died acutely had severe COPD and poor quality of life and in all cases decisions not to ventilate invasively had already been taken. Of the remaining 23 patients, three died within two months of discharge, five more died within one year, and three more died within two years, all of these patients died of respiratory illness. Five other patients died of other illnesses the two year follow up period, including cancer and cardiac disease.
Seven patients (18%, four male) are alive two years post discharge; two of these have had frequent admissions and five of them are oxygen dependent.
This study suggests that patients with COPD who require NIV for HRF still have a significant two year mortality.
P56 NINETY DAY OUTCOMES IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATIENTS ADMITTED WITH SEVERE RESPIRATORY ACIDOSIS
G. South, S. W. Crooks, J. Tague, A. Benrajab, J. W. Hadfield. Chesterfield Royal Hospital NHS Foundation Trust, UK
Introduction: The use of non-invasive ventilation (NIV) in patients with chronic obstructive pulmonary disease (COPD) who are admitted with acute hypercapnic respiratory failure (AHRF) is felt to be most successful in those with an arterial pH 7.25–7.35 at presentation (
). Outcomes in those with pH<7.25 are felt to be less good, and early intubation and mechanical ventilation if appropriate is recommended. Audit data from our hospital (
) showed that approximately 2/3 of such patients treated primarily with NIV in our unit survived to discharge. The 90 day outcomes for those with milder and those with more severe acidosis are compared in this prospective audit of COPD patients admitted with AHRF between May 2004 and April 2005.
Setting: General respiratory ward and high dependency unit of a district general hospital.
Method: Prospective audit of all admissions with persistent acute hypercapnic respiratory failure (AHRF) May 2004 and April 2005
Results: In hospital mortality was similar in the two groups with AHRF. However both readmission and death within 90 days of the index episode was much higher in the more severe group.
One patient in the severe group received tracheal intubation and mechanical ventilation after failure of NIV. Median age was 76 years in the severe group (range 58–93) and 73 years in the milder group (57–92).
Conclusion: This audit shows similar in hospital outcome for COPD patients with severe AHRF given NIV as primary treatment compared with those with milder AHRF; however lower pH at presentation was associated with a worse medium term prognosis
Abstract P56
P57 LONGITUDINAL STUDY OF BODY COMPOSITION IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE OVER AN 18 MONTH PERIOD
C. E. Bolton1, A. A. Ionescu1, P. H. Edwards1, S. M. Edwards1, R. J. Pettit2, W. D. Evans2, L. S. Nixon1, D. R. Owens3, D. J. Shale1. 1Respiratory Medicine and 3Diabetes Research Unit, Cardiff University, Llandough Hospital, Cardiff, Wales; 2Medical Physics, UHW, Cardiff, Wales, UK
Introduction: Altered body composition occurs in chronic obstructive pulmonary disease (COPD). We studied changes in body weight, fat free mass (FFM), fat mass (FM), and bone mineral density (BMD) over an 18 month period in patients with COPD.
Methods: Spirometry, body composition (dual energy x ray absorptiometry), circulating IL-6, TNF-α, TNF-α sr I&II, testosterone were determined in patients and healthy subjects (HS) at start and end of study, when clinically stable.
Results: Of 58 patients, 41 (21 male) patients completed the 18 months, mean age 66.3 (95% CI 63.6 to 69.1) years, FEV1% 56.1 (95% CI 49.6 to 62.7) % in addition to 23 (12 male) HS, aged 60.8 (95% CI 57.6 to 64.0) years. At outset, 16/41 patients had a FEV1<50% predicted, 10 a low height squared FFM index –FFMI (<5th percentile for HS). At commencement, BMD was lower in patients at both the lumbar and hip region, p<0.01 and was less in patients with a low FFM than normal FFM, p<0.05. Circulating IL-6, TNF-α sr I&II were greater in patients, p<0.01, and four patients (0 HS) had a low testosterone level. During the study, there was no change in lung function, weight, total FFM, or BMD hip in the patients, but there was a reduction in height, −0.002 (95% CI −0.004 to −0.002) m and a gain in both FM:0.8 (95% CI 0.01 to 1.59) kg, and BMD lumbar occurred: 0.08 (95% CI 0.03 to 0.12) g/cm2. Change in hip BMD was related to change in FFM (r = 0.439, p = 0.004), but lumbar BMD was not (r = 0.003, p = 0.985). The body composition changes were similar in patient subgroups according to lung function severity (< or > FEV1 50% predicted), exacerbation frequency (< or > group median of 1.3/year) and low/normal initial FFM. Weight loss was experienced in 17 patients (12 had normal BMI, normal FFM; three normal BMI, low FFM; two low BMI, low FFM initially), with five patients losing >5% of body weight (−2.7 to −5.9 kg), with FM accounting for the majority of this weight loss. In these five, the weight loss was apparent between two three monthly visits, but with no clear precipitating factor. Those with an initial low FFM, tended to lose FM, while those with a normal FFM initially gained FM. FFM loss occurred in 21 patients (12 who also lost weight). Baseline cytokines were not different between those who lost weight and those who did not.
Conclusions: Weight loss was common, though loss in excess of 5% occurred in 12% and was episodic rather than gradual. Loss of FFM was common but was not concordant with weight loss suggesting a different subset lose FFM. Those starting with a normal FFM tended to gain FM and those with a low FFM lost FM, which suggests that the changes in body composition and weight loss may be affected by different factors.
Supported by the British Lung Foundation, CAPRICORN, and GSK.
P58 COMORBIDITY IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE AND ITS INFLUENCE ON ADMISSION TO HOSPITAL
M. C. P. Apps, R. Ahmed, A. S. Jubber, R. M. Weatherstone, R. W. Fowler. Oldchurch Hospital, Romford, UK
Introduction: Many patients admitted to hospital with exacerbations of chronic obstructive pulmonary disease (COPD) have a large burden of disability from other comorbid conditions, which might predispose them to require frequent admission and complicate their care once admitted. A high level of comorbidity has been reported to be associated with increased morbidity and mortality in patients with respiratory disease (
), and a number of these have been identified as important in combination with or without age (
)
Methods: We have examined the notes of patients attending chest clinics with COPD and analysed them to identify common co morbidities, with similar data being collected on patients admitted to the wards with acute exacerbations of COPD as their primary reason for admission. We have used the co morbidity Charlson index (
) to identify multiple comorbid factors which might affect these patients, which includes chest disease, heart disease, stroke, dementia, diabetes, renal or liver failure, or evidence of any cancer among its items
Results: For 67 outpatients with COPD and 78 patients admitted with COPD the patients admitted with exacerbations tend to be older and frequently have at least one other major comorbidity (82%), and many have several significant medical conditions.
Many of the patients admitted with COPD had significant ischaemic heart disease, and those patients with this as one of their comorbid conditions had 77% more admissions over a two year period than those without heart disease (mean admissions 2.4 SD 1.69 v 1.35 SD 1.55, p<0.001).
Patients with a high Charlson Index tended to have only a slightly higher incidence (22%) of admissions over the same period (1.89 SD 1.5 v 1.89 SD 1.76, NS) which may have been mainly due to the presence of ischaemic heart disease.
Conclusion: Identification of factors which may predispose patients with COPD to require in patients hospital stay by the presence of multiple comorbidities or of heart disease may allow these patients to be targeted by community based programmes of support to reduce the need for admission and allow scarce resources of staff and finance to be used effectively.
Abstract P58
P59 A SIMPLE MULTIDIMENSIONAL STRATIFICATION OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE PREDICTS MORTALITY IN PATIENTS IDENTIFIED IN PRIMARY CARE
N. Keaney1, A. Lawrence1, A. Billett2, T. Hildreth1, S. Haggerty2, C. Waine2, I. Taylor1. 1Sunderland Royal Hospital and 2Sunderland Teaching Primary Care Trust, UK
Chronic obstructive pulmonary disease (COPD) should be regarded as a multidimensional disease characterised: Systemic involvement causing loss of lean body mass and muscle weakness – BMI; Impairment due to Airflow Obstruction – FEV1 %predicted and Disability expressed as perceived breathlessness – MRC Dyspnoea Scale.
) added Exercise to SID for a BODE score that predicted mortality in a group of hospital patients (93% male) with COPD.
In 403 patients with COPD (48% female) identified in primary care we calculated a SID score (BODE without a 6 minute walk test (6MWD)). Mortality (all cause) from 1999–2005 is presented as a Cox-Regression analysis (adjusted for age) for quartiles of SID scores. The overall model is highly significant (p<0.001).
Conclusion: SID is a simple multidimensional index readily applicable in primary care to define the clinical impact of COPD. A 6MWD is not necessary even for a cohort with less severe disease (0.5% with MRC dyspnoea score of 5) than Celli et al studied. This model may be of value for demonstrating which therapeutic interventions can shift the SID score, influence the natural history of COPD, and hence improve prognosis.

Survival for quartiles of SID scores.
P60 COMPARISON OF PARTICIPANTS AND REFUSERS INVITED TO ENROL IN A CASE MANAGEMENT STUDY FOR PATIENTS WITH MODERATE TO SEVERE CHRONIC OBSTRUCTIVE PULMONARY DISEASE
S. Jones, P. Farrar, M. Poland, M. O’Neill, C. Warburton, P. M. A. Calverley, L. Davies. Aintree Chest Centre, University Hospital Aintree, Liverpool L9 7AL, UK
Acute exacerbations of chronic obstructive pulmonary disease (COPD) present a huge burden to acute medical services with 2/3 of patients readmitting within one year (
). Respiratory case management has been shown to reduce hospital admissions in Canada (
), but as yet there is no evidence to support such a model in the UK.
We are conducting a prospective, randomised controlled trial of a multidisciplinary respiratory case management model for patients with moderate to severe COPD. Patients with one or more COPD hospital admissions in the last 12 months are eligible to enrol in the study. Patients are approached towards the end of their admission and are given a verbal explanation, written information and a minimum of 24 hours to decide whether or not to participate. They are offered an eight week rehabilitation programme, based in hospital and at home, followed by intensive support, including telephone advice, rapid clinic appointments, and home visits for 12 months. The primary outcome measure will be the number of hospital admissions during the 12 month follow up period. We are also interested in whether this method of health care delivery is acceptable to patients in Liverpool. We hypothesised that participation in the case management model would be influenced by disease severity and degree of social support. Over eightmonths, we approached 121 (68 female) eligible COPD patients during a hospital or “hospital at home” admission. Mean age 72.4 (SD 8.3) years, FEV1 0.9 (SD 0.32) l. 54 patients (45%) agreed to participate (“acceptors”) and 67 patients (55%) declined (“refusers”). Compared with acceptors, refusers had worse lung function; refusers v acceptors: mean (SD) FEV1 0.8 (0.25) v 1.0 (0.36); p<0.001, FEV1(%predicted) 36.3% v 42.6%; p = 0.013. Men were significantly more likely to agree to participate (29/53:55%) than women (25/68:37%; χ2<0.05). There were no significant differences between acceptors and refusers with regard to age, home support, current smoking status, Charlson comorbidity score, acidosis on admission arterial blood gas, or number of hospital admissions in the preceding 12 months.
There is currently great political enthusiasm for case management which it is hoped will dramatically reduce the number of hospital admissions in patients with chronic disease. Although our case management programme involved enrolment in a study, which may have influenced patients’ decisions to participate, this was not given as a reason for declining case management by any individual. In our population, females and those with worse pulmonary function were significantly less likely to participate. Should case management prove to be effective, alternative strategies will need to be considered for more than 50% of eligible COPD patients who did not wish to take part.
P61 DO CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATIENTS UNDERSTAND THEIR DISEASE?
J. Greenwood, J. Corless. Arrowe Park Hospital, Wirral, UK
Introduction: Many patients with chronic obstructive pulmonary disease (COPD) seem to be unaware of their exact diagnosis and the underlying cause of their illness. We undertook a survey to define the extent of this problem.
Method: A simple 10 point questionnaire was completed by patients selected randomly in both inpatient and outpatient settings. All patients had obstructive airways disease defined by a forced expiratory volume in one second (FEV1) <80% predicted and a ratio of FEV1: forced vital capacity <70%. All were former or current smokers. Patients completed the questionnaire by themselves unless they were physically unable. To assess their understanding of their diagnosis and causative factors, they were asked to choose responses from a list provided. The patients also were asked whether their chest condition was diagnosed in primary or secondary care.
Results: 50 patients were surveyed. 30 (60%) were male. Their mean age was 68.5 years (range 50–82). 62% knew that their diagnosis was COPD, 40% thought it was bronchitis or emphysema, 13% said they had asthma and 4% did not know what the diagnosis was (more than one response was allowed). 40% of them had never heard of COPD before completing the questionnaire. Of the 28 patients who had their first diagnosis made by a hospital doctor, 22 (79%) knew it was COPD. Of the 22 patients whose chest condition was diagnosed in primary care, 14 (64%) had never heard of COPD. When asked what they thought had caused their chest condition, only 36% thought that cigarette smoking had contributed. Asbestos, dust, and fumes at work were all blamed by the patients, often in combination. Two patients felt their disease was hereditary. Only 46% felt that smoking cessation had made or could make a difference to their chest disease and eight patients (16%) continued to smoke.
Discussion: This survey suggests that many COPD patients have a poor comprehension of the nature and cause of their disease. A discrepancy between patients first diagnosed in primary and secondary care was noted. Many patients used outdated or incorrect terms to describe their illness. Only a minority of patients were aware that their disease was likely to be caused by tobacco smoking, many choosing to blame occupational factors encountered during their life. The dismissal of smoking cessation as a useful intervention by over half of the patients is of particular concern. Although some of our results could be explained by geographical and epidemiological bias, there is a clear need for improved education of COPD patients at the time of diagnosis and during follow up, and the importance of smoking cessation in this group should be emphasised.
P62 THE LAST YEAR OF LIFE OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE: THE CARERS’ PERSPECTIVE
H. Elkington, P. White, J. Addington-Hall. Department of General Practice and Primary Care, Guy’s King’s and St. Thomas’ School of Medicine, King’s College London
Background: Chronic obstructive pulmonary disease (COPD) is a chronic illness which disables patients over years with a gradual deterioration in respiratory function punctuated by acute exacerbations and loss of independence. Without the help of informal carers, often relatives, many patients would be unable to remain in their own home in the latter stages of illness. How much do the carers know about the impact of the illness and its prognosis, and is this enough?
Methods: Questionnaire survey to the relatives of 209 deceased COPD patients in the year after death.1 Questions related to the last year of life. One section asked relatives about their knowledge of the deceased’s illness in the last year of life
Results: 52% response rate. 29% of respondents were the spouse or partner of the deceased, and 52% were the brother or sister. 60% of respondents provided help with personal care and 84% help with household tasks. Over half reported that they were not able to find out all they wanted to know about the deceased’s illness and how it was likely to affect them. 38% did not feel involved in decisions made about the deceased’s care. 79% of these wished to be more involved. 40% were not aware that the deceased might die. 78% of these would definitely or probably liked to have known. Half of the spouses or partners of the deceased and half of the children were aware that the deceased might die.
Conclusion: Relatives play a considerable role in looking after patients with COPD at the end of life. They are not as informed about the deceased’s illness and prognosis as they would like to be. As well as the information needs of patients, those of the carers also need to be addressed at the end of life.
1
P63 PSYCHOLOGICAL IMPACT OF MOODS IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE
S. A. Husain, K. Gaber, F. Paciello, R. Cannings-John, R. Royston, H. Contractor, A. Millar, N. Jarad. Lung Research Unit, Medical School, Southmead Hospital, Bristol & Bristol Royal Infirmary, Bristol, UK
Background: Anxiety and depression has a great big role in hospital admissions for a lot of the elderly chronic obstructive pulmonary disease (COPD) patients. We conducted a study to find out the relation with anxiety and depression levels on hospital stay. Data collection is on going with the aim of collecting data for 150 patients.
Methodology: We used Hospital Anxiety and Depression Scale (HADS) to measure levels of depression and anxiety in elderly COPD patients aged 60 years or above, admitted to the hospital with an acute exacerbation. HADS scores were measured at three time points; the first assessment was done within three days of admission, the second at time of discharge home, and the third in a stable state in the outpatient clinic. The patients themselves completed the majority of the questionnaires. Scores of anxiety and depression ranged between 0 and 21 (no anxiety/depression to high anxiety/depression). The association between length of hospital stay and anxiety and depression scores was analysed using Spearman’s correlation coefficient since length of stay was negatively skewed.
Results: A total of 41 patients moods were assessed of which 17 patients had three mood assessments done completely, as two patients died before the third assessment with a mean age of 76 years (range 60–86 years) and 68% were male. Patients had a median length of hospital stay of 10 days (range 2–51). There was no association noted between anxiety or depression with length of hospital stay from the initial results as perhaps other comorbidities and confounding factors have a role. The median scores for both the anxiety and depression were examined at each time point. Anxiety was slightly higher at admission but decreased at discharge and maintained at outpatients. Depression on the other hand is not as high at admission and decreases slightly at discharge but has increased by the outpatient review.
Abstract P63
Conclusion: Preliminary results show no direct association between anxiety or depression levels and the length of stay in hospital, as there seem to be other confounding factors. There was some indication that anxiety is highest at admission and depression at outpatient visits.
Occupational lung disease
P64 OCCUPATIONAL ASTHMA: OLD AGENTS IN NEW (DIS)GUISES
J. Szram, J. Cannon, A. M. Hole, A. G. F. Brant, P. Cullinan, A. J. Newman Taylor. Department of Occupational and Environmental Medicine, Royal Brompton Hospital, London SW3 6LR, UK
Occupational asthma is a remarkably tenacious disease: because it resides within the workplace, its location and persistence will be dependent on changes within industries. Here we present six cases of asthma induced by classic occupational allergens in novel or near novel settings. Each was seen as a patient at Royal Brompton Hospital. In each case the diagnosis was supported by immunological and/or functional confirmation:
Algorithms promoted to improve the diagnosis of occupational asthma generally refer to high risk occupations. Although these are likely to include most patients with the disease, many widely recognised causative agents are present in an increasing variety of disparate industries. Industry will continue to find new uses and locations for agents, and therefore vigilant history taking—and careful attention to all workplace exposures—remain essential.
-
Two drinks manufacture factory workers presented with work related rhinitis and asthma symptoms. A component of one product was found to be flour; both subjects had positive specific skin prick tests and IgE to flour as well as positive specific bronchial provocation tests to the product in question. Flour is traditionally a major cause of baker’s asthma; these appear to be the first cases where disease has arisen from its use as a drink.
-
A garden furniture maker whose asthma developed from his work with western red cedar. Most previous cases have been in Canadian saw mill workers in the 1970s, although the initial case series was in Australian outdoor furniture makers.
-
A supermarket bread packer with asthma caused by inhalation of polyolefin/polyester fume—a similar process and agent was implicated in US meat wrappers’ asthma in the 1970s.
-
Latex asthma in a printing ink factory worker—first described and characterised in healthcare workers, this condition is likely to occur still among workers whose glove use is not controlled as it is now in UK healthcare.
-
A circuit board manufacturer with asthma from sodium persulphate, used to clean the boards. A similar agent is implicated in hairdresser’s asthma. Exposures to sodium persulphate are increasingly widespread in computer manufacture.
P65 FACTORY EMPLOYMENT RATE AS A MAJOR DETERMINANT OF OCCUPATIONAL ASTHMA
A. Brant, C. Zekfeld, A. J. Newman Taylor, P. Cullinan. Department of Occupational and Environmental Medicine, Royal Brompton Hospital, London SW3 6LR, UK
Introduction: In 1998 we reported, using a cross sectional method, a very large outbreak of occupational asthma in a European detergent factory. We wanted to investigate the timing and determinants of the outbreak, and to examine in particular whether employment patterns had had an important role.
Method: We identified a retrospective cohort of all individuals who had been employed in the factory after 1988 and had worked there for more than four months. We collected health data from routine occupational health records and job histories from the employment records. In addition we collected information on enzyme tonnage usage and static dust and enzyme measurements.
Results: Full information was available for 884 employees (93%). The incidence of chest symptoms varied between 2% and 9%, through the study period with peak incidences in the early and mid 1990s. These occurred at times of expansion in the factory workforce and the use of increasing quantities of detergent enzymes. However the incidence of chest symptoms for new employees—a high risk group—remained constant at around 25% throughout the period; and declined only after a major intervention with substantial reductions in enzyme exposure.
Conclusion: Our findings indicate that the risk of occupational asthma in a workforce is determined by workplace exposures and, importantly, by the rate of employment of new workers.
Supported by BOHRF.
P66 VARIATION IN DIAGNOSTIC METHODS FOR OCCUPATIONAL ASTHMA. A NATIONAL STUDY
S. Naylor, J. Elms, A. D. Curran, L. M. Bradshaw, M. Henson, R. Rawbone, D. Fishwick on behalf of the British Thoracic Society Research Committee. The Centre for Workplace Health, Health and Safety Laboratory, Harpur Hill, Buxton, Derbyshire and the University of Sheffield, UK
Background: The Health and Safety Executive of the UK (HSE) is committed to reducing workplace ill health. Of particular concern to HSE are the individual and societal costs attributable to occupational asthma. This paper presents key findings of a study, jointly funded by the HSE and the British Thoracic Society, investigating clinical approaches employed in UK hospitals for diagnosing occupational asthma.
Methods: 100 hospitals with at least one respiratory consultant in a full time post were randomly selected. Senior respiratory consultants working within respiratory departments were contacted and asked to nominate a consultant who saw occupational respiratory patients on a regular basis to be interviewed for the study. 34 consultants were interviewed. As part of the interview, consultants were provided with a limited amount of background data regarding a real case of baker’s asthma and were then asked to provide a detailed description of the approach they would employ to arrive at a diagnosis.
Results: 88% reported that they would request the patient keep a serial peak flow diary for a period at and away from work. Of those who suggested a PEF diary, 38% suggested two hourly recordings and 46% suggested a duration of four weeks. Only 10% reported that they would carry out non-specific provocation challenge testing, and no one reported that they would carry out specific occupational challenge. Immunological tests were more widely employed, with 50% reporting that they would test for total IgE, 60% for specific IgE to workplace allergens, and 10% for specific IgE to common aero-allergens. 57% reported that they would recommend making changes to day to day work practices in order to reduce workplace exposures, such as using respiratory protective equipment (31%), seeking a change of role within the workplace (26%) or completely changing job (36%). In addition, 21% reported that they would discuss eligibility for industrial injuries benefit and compensation. Of those that did not offer such advice, several reported that they would refer patients to other parties, such as other respiratory consultants (21%) and employee unions (15%).
Conclusions: This study has documented a variable diagnostic approach employed by respiratory consultants when faced with possible occupational asthma. A workable standard of care is required, along with more stringent undergraduate and postgraduate training to ensure greater national consistency.
P67 PREVALENCE OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE AND THE EFFECT OF OCCUPATIONAL EXPOSURES UPON LUNG FUNCTION IN NORTHEAST ENGLAND
A. M. S. Melville1, O. A. Afolabi1, S. C. Stenton2. 1Department of Respiratory Medicine, Northumbria Healthcare NHS Trust and University of Newcastle upon Tyne, UK; 2Royal Victoria Infirmary and University of Newcastle upon Tyne, UK
Background: The prevalence of chronic obstructive pulmonary disease (COPD) in UK adults is estimated at 10 to 12%.1,2 However, few studies have used objective measurements of lung function to derive the estimates, and the effect of occupational exposures on lung function and COPD in the general population is unknown.
Methods: 12 000 randomly selected 45–69 year olds (50% male) in north east England were cross sectionally surveyed in a study of COPD prevalence and causes. Subjects received a postal questionnaire enquiring about occupational exposures, symptoms, respiratory diagnoses and smoking. Spirometric measurements were performed on 845 randomly selected responders. The NICE criteria were used for defining COPD (FEV1<80% predicted and FEV1/FVC<0.7).3
Results: Valid questionnaire responses were obtained from 64%, mean age 58, 47% male. 63% had ever smoked and 55% reported cough, sputum, breathlessness, or wheeze. Logistic regression confirmed associations between symptoms and reporting occupational exposures, smoking, socioeconomic status, and atopy (p for all <0.001). Valid spirometry was performed by 841 subjects with NICE defined COPD present in 10.7%. Regression analysis confirmed that lower FEV1s were mainly obstructive in nature (p<0.001) with decreasing FEV1 associated with smoking (p<0.001), increasing age (p<0.001) and with reporting any occupational exposures (n = 230, p = 0.08).
Conclusions: Although comparisons are hard, our COPD prevalence rate is comparable to the existing UK data and it is likely that occupational exposures contribute significantly to COPD in the northeast of England.
1
2
3
P68 FEV1 DECLINE IN GRAIN EXPOSED WORKERS
V. Moore1, W. Anees1, D. Blainey2, K. Robertson2, P. S. Burge1. 1Occupational Lung Disease Unit, Birmingham Heartlands Hospital, Birmingham, UK; 2Department of Respiratory Medicine, Broomfield Hospital, Chelmsford, UK
Introduction: We have previously studied 129 dockers and grain exposed farmers and found that workers with work related falls in PEF had a lower FEV1/FVC (71%) than those with positive RAST/questionnaire (78%). We have now completed further measurements on these workers over four years to find out whether there is any difference in forced expiratory volume in one second (FEV1) decline between the groups. An extra nine workers who had positive peak flows of inadequate quality have also been included in this study, and only workers >30 years old were included.
Results: The Venn diagram shows the number of workers that were followed up and the mean FEV1 decline in each group, split into four categories. Although the mean decline shows some differences with those that had no symptoms, work related PEFs or positive RAST, this was not significant (p>0.426 for all groups, univariate analysis of variance).
Conclusions: Decline in FEV1 was above predicted values in those with positive IgE to grain or storage mite, those with work related symptoms and those with work related PEF changes. However, none were significantly greater than those without any of these features probably due to small numbers in each group and the wide variance.

P69 EXTRINSIC ALLERGIC ALVIOLITS ASSOCIATED WITH METAL WORKING FLUIDS IN A PRECISION ENGINEERING COMPANY
F. C. Horwood1, H. Pattani1, R. B. Hubbard2, M. J. Ward1. 1Kings Mill Hospital, Sutton in Ashfield, UK; 2Nottingham City Hospital, UK
Background: We report a series of patients with respiratory symptoms related to their work with metal working fluids (MWFs). These patients presented between August 2004 and July 2005. All of these individuals worked at a precision engineering company in North Nottinghamshire at the time of the onset of their symptoms.
MWFs provide cooling and lubrication during the machining and shaping of metals. They may be organic or synthetic fluids. They are otherwise known as coolants, suds, or slurry. The fluid is recycled in the area in which it is used and renewed on a regular basis. This fluid may become contaminated with bacteria or fungi so regular bacterial analysis is performed and a biocide is added to the fluid to prevent overgrowth. It is well known that exposure to MWFs may cause a variety of respiratory conditions including extrinsic allergic alveolitis.
Methods and Results: We identified six individuals who presented with symptoms of increasing dyspnoea, dry cough, flu-like symptoms, and weight loss. Spirometry was very variable. In some cases it was normal but also a purely restrictive pattern or a mixed obstructive/restrictive pattern with reduced transfer factor were seen. High resolution CT scans confirmed the presence of extrinsic allergic alveolitis in the symptomatic individuals. No new cases have presented since a change has been made to the MWF used.
Conclusion: We conclude that these workers developed extrinsic allergic alveolitis to a component of the MWF at their place of work. Previous series of extrinsic allergic alveolitis secondary to microbiological contamination of MWFs have been reported in the UK1,2 with a causative organism found in just one series.2 We have yet to identify a microbiological contaminant as the causative agent but since the change in the MWF has brought an end to new cases this would point towards a contaminant being the cause of the problem in our series.
1
2
P70 POPULATION BASED EPIDEMIOLOGY AND PROGNOSIS OF MESOTHELIOMA IN LEEDS, UK
A. Chapman, S. Mulrennan, B. Ladd, M. Muers. Leeds Teaching Hospital NHS Trust, West Yorkshire, UK
Background: Malignant mesothelioma is a neoplasm with a 6% two year survival. We present a population based audit capturing all patients within a defined geographical area. Epidemiology, presentation and management are described.
Method: Retrospective analysis of all 107 cases diagnosed between 2002 and 2005 from the 750 000 local population. Patient records and coroner’s reports were reviewed.
Results: 84% were male and median age was 76 years (range 36–90). Median survival from diagnosis was 195 days. 69% and 23% had a histological and cytological confirmation during life respectively. 74% reported definite/possible asbestos exposure. 82% had symptomatic pleural effusions at presentation. Twice as many patients were managed with surgical rather than medical pleurodesis and these had a lower recurrence rate (11% v 47%, p = 0.011). 89 patients had VATS/cutting CT biopsies or drains. 55/89 (62%) had radiotherapy to these sites. 32 (42%) were within six weeks. Three (9%) of these had track recurrence and the seeding rate after six weeks was 3/23 (13%). Median seeding time was 174 days. 84% of patients did not receive chemotherapy, despite 60/102 (59%) having a performance status of 0–2. 27% (16/60) of eligible patients refused and 32% (19/60) were deemed unfit by their oncologist.
Conclusion: Survival is worse than in published literature. Median age is higher, performance status worse and many patients are too ill for or refuse chemotherapy. Surgical pleurodesis seems preferable in view of lower recurrence rates. There is tumour seeding even after prompt prophylactic radiotherapy.
P71 SECONDARY CARE DIAGNOSIS OF OCCUPATIONAL LUNG DISEASE: ARE WE DOING ENOUGH?
S. Naylor, J. Elms, A. D. Curran, L. M. Bradshaw, M. Henson, R. Rawbone, D. Fishwick on behalf of the British Thoracic Society Research Committee. The Centre for Workplace Health, Health and Safety Laboratory, Harpur Hill, Buxton, Derbyshire and the University of Sheffield, UK
Background: The accurate and rapid diagnosis of occupational asthma is important not only for the individual worker, but also to allow appropriate workplace intervention to occur before other workers similarly exposed develop respiratory problems. The Health and Safety Executive of the UK (HSE) is committed to reducing the incidence of occupational asthma by 30% by 2010. The adequate provision of appropriate diagnostic resource is essential to delivering this challenging reduction. However, little is currently known about the UK provision of such diagnostic services based in secondary care.
Aim: We report the findings of a national study, jointly funded by HSE and the British Thoracic Society. The study aimed to document the facilities available to assess and diagnose occupational lung disease in a randomly selected group of respiratory medicine departments based in secondary care.
Methods: Using the BTS respiratory directory, a random sample of hospital based respiratory departments were selected for study. The researcher visited all departments, and facilities for assessment were noted according to a study proforma.
Results: 45 respiratory consultants working in 35 hospitals across England, Scotland, and Wales were questioned. Each hospital had a mean of three WTE respiratory consultants, and each consultant served a self reported population of 151 000. All departments bar one employed at least one respiratory nurse specialist, the mean number being five per hospital. Not all respiratory departments had dedicated respiratory physiology technicians, and few had an occupational health physician seeing outpatients in clinic. 58% of the study physicians had previously referred patients with suspected occupational lung disease to a tertiary centre for advice. These tertiary centres were on average 42 miles (range 1–111) from the referring hospital. Although most departments had access to appropriate initial investigations, there was marked variation in access to measures of airway responsiveness, specific allergen challenge, and to complex immunological assessment.
Conclusions: This study has documented variable national provision of diagnostic facilities for patients with suspected occupational lung disease. Access to specialist facilities for investigating these cases needs to be improved nationally.
P72 PILOTING A SURVEILLANCE SCHEME FOR OCCUPATIONAL AIRWAYS DISEASE IN SCOTLAND: SCOTTISHSHIELD
J. G. Ayres1, S. Semple1, A. R. Scaife1, G. D. Henderson1, P. S. Burge2, G. Scadding3. 1University of Aberdeen, UK; 2Birmingham Heartlands Hospital, UK; 3Royal National Throat Nose and Ear Hospital, UK
Background: Occupational asthma (OA) is common but much underrecognised. 3000 cases of OA are recognised each year in the UK leaving a large number of cases either permanently unrecognised or recognised late in the clinical course. Recognition of OA is important not only from the individual’s point of view but also by identifying particular workplaces/occupations, which can then be dealt with and further cases prevented. A successful surveillance scheme for reporting OA has been established and running for 12 years in the West Midlands—SHIELD.1
Aims: To establish a surveillance scheme for occupational airways disease in Scotland and to pilot a surveillance methodology in NE Scotland, Inverness, Orkney, and Shetland (total population approx 750 000), over six months working with respiratory and occupational physicians in the area based on SHIELD methodology used in the West Midlands—ScottishSHIELD.
Methods: When reporting physicians identified patients with OA, a two page questionnaire was completed online (with patient consent) and sent centrally to the Department of Occupational and Environmental Medicine, Aberdeen via email. Data were entered automatically from the internet into an encrypted Access database. After six months, a follow up questionnaire was mailed to consenting patients to establish any beneficial changes to workplace conditions.
Results: In six months 14 cases from Aberdeen and one from Inverness in three months were reported to ScottishSHIELD suggesting underreporting in Inverness. Assuming the “at risk” population covered by the pilot study was 750 000 our results suggest an incidence rate of 4/100 000 per annum. The incidence rate for the UK is around 5/100 000 per annum but may still be well below the true rate. Of the 15 cases in the ScottishSHIELD database (age range 28–58), 13 had classical OA (one also had occupational rhinitis and one also had RADS). Of these 13, 10 had a recognised/likely cause: three, animal proteins in laboratory workers; two, isocyanates; and one each flour, formaldehyde, paper pulp, metabisulphite, and gluteraldehyde. Two had RADS only whose exposure/jobs were zinc fume in welding and possibly strong acid and/or alkali in a knackery worker. Of 10 cases that agreed to follow up, questionnaires have been mailed to eight and returned successfully completed. One case is unemployed, one is off work sick, and six are still in the same job. Of the six in the same job, five have been issued with masks by their employers to wear while working.
Conclusions: The ScottishSHIELD reporting system works but needs to be used by more physicians to develop and overcome underreporting. Consideration needs to be given to rolling the system out to the whole of Scotland.
1
Sleep disordered breathing and obstructive sleep apnoea
P73 CLINICAL UTILITY OF THE HYPNOPTT IN THE ASSESSMENT OF SLEEP APNOEA/HYPOPNOEA SYNDROME
R. L. Riha, E. A. Hill, C. C. Chan, J. Y. Den, H. M. Engleman, N. J. Douglas, T. W. Mackay. Department of Sleep Medicine, Royal Infirmary Edinburgh, UK
Aims: To determine the clinical utility of unsupervised, home based studies for diagnosing the obstructive sleep apnoea/hypopnoeas syndrome (OSAHS) using HypnoPTT (Tyco Healthcare). Comparison was made with in-laboratory, fully supervised polysomnography (PSG).
Methods: A prospective study was conducted on 581 patients from March 2003–March 2005, living within a 50 mile radius of the hospital with at least two of the following: snoring, witnessed apnoeas, and excessive daytime somnolence. After instruction by a sleep technician, all patients underwent a home based sleep study. Data were downloaded and scored manually. Studies were scored blind to previous outcome using standard criteria. A cut off point of ⩾30 apnoea per hour in bed (AH) and Epworth Sleepiness Scale (ESS) ⩾11 was used to diagnose OSAHS on the home based study; a cut off point of AHI 15 and ESS ⩾11 on PSG. Sleepy patients with ⩽30 AH in bed on home study proceeded to PSG within three months.
Results: Mean age was 49 (SD 11) years; 150 (26%) patients were female. Mean body mass index (BMI) was 32 (SD 7) kg/m2. Subjects’ mean ESS was 12 (SD 5)/24. Of the 581 patients, 119 (20%) fulfilled criteria for commencing continuous positive airway pressure (CPAP) therapy. 97 (16%) patients were referred for mandibular repositioning splints (MRS). Additional PSG was performed in 213 patients (37%). There was no significant difference between the PSG and non-PSG groups in age, BMI, sex ratio, or time spent in bed using the HypnoPTT. ESS was significantly higher in the PSG group (14 (SD 4) v 10 (SD 5); p<0.0001). The PSG group also had more sleepy drivers. There was a significant difference in the AHI recorded using the HypnoPTT versus PSG (12 (SD 8) v 24 (SD 20); p<0.0001). A Bland-Altman plot showed systematic bias between the two recording methods. In the PSG group, a further 23 patients proceeded to CPAP therapy and two were referred for MRS. Despite need for additional PSG in 37% patients, costs were calculated to be half that of performing in-lab PSG for all patients.
Conclusions: For diagnostic reliability, a further sleep study is required in 37% patients using the HypnoPTT. Reasons for “negative” home studies may be due to unsupervised application technique, unknown actual sleep time, and recording failure. Clinical bias (based on history and ESS) is a strong determinant of referral of patients for additional PSG. Home based studies continue to be cost efficient.
P74 A COMPARISON OF TWO RESPIRATORY SIGNALS IN THE MEASUREMENT OF SLEEP DISORDERED BREATHING
Y. Turgut, P. Stone, M. Atkins, A. Woodcock. Whythenshawe Hospital, South Manchester University, UK
The accurate diagnosis of the obstructive sleep apnoea/hypopnoea syndrome (OSAHS) is important because of its consequences in relation to both public and individual health. The usual approach to investigate OSAHS is by multichannel respiratory monitoring. There is an increasing number of systems available to use for sleep studies and this study compares the results from two pieces of equipment using different respiratory signals. The Densa DMS 200 uses a measure of respiratory paradox as a marker of upper airway obstruction and respiratory related arousal in conjunct with other respiratory signals while the Resmed Autoset (AS) uses flow limitation alone.
Seventy nine (55 male, 24 female) patients with clinical characteristics of the OSAHS, underwent a supervised, laboratory based overnight sleep study with the Densa and AS diagnostic systems simultaneously.
The mean apnoea/hypopnoea index (AHI) assessed by interactive scoring with the Densa system (AHI-D) was 11.27 compared to AHI-AS of 20.46. In terms of AHI, although correlation was found between the two respiratory signals by Pearson’s correlation test (r = 0.814), by Bland and Altman analysis with mean bias −9.2, no agreement was shown (95% agreement limits were −28.4, +9.97). The phase angle index (PAI-D) as a measure of respiratory paradox by the Densa system and respiratory irregularity index (RII-AS) assessed by AS are used as a measure of arousal. There was no correlation between the two (r value = 0.687, 95% agreement limits 6.94, −46.98).
In conclusion, this study illustrates that different monitoring methods potentially produce different results. All studies should be interpreted by trained individuals who are aware of the limitations of the results. Numbers derived by computer software should be treated with caution and expert technical interaction is important to optimise the results.
P75 A COMPARISON BETWEEN TRANSCUTANEOUS MONITORING (TOSCA 500 SYSTEM) AND ARTERIALISED EAR LOBE BLOOD GAS SAMPLING FOR THE MEASUREMENT OF CARBON DIOXIDE LEVEL DURING THE SET UP PROCEDURE FOR PATIENTS REQUIRING LONG TERM NON-INVASIVE VENTILATION
Y. Turgut, S. C. Johnson, A. Bentley. Ventilatory Support Unit, South Manchester University Hospitals NHS Trust, Wythenshawe Hospital, Manchester, UK
Background: Domiciliary non-invasive ventilation (NIV) is well established in the long term management of conditions assosciated with chronic type II respiratory failure. Continuous transcutaneous CO2 monitoring is a valuable tool in addition to arterialised ear lobe blood gas measurements in the set-up of patients with non-invasive ventilation. The Tosca 500 is the first system to allow the simultaneous non-invasive monitoring of the pCO2, SpO2, and pulse rate through a single ear lobe sensor. The aim of this study was to examine the degree of agreement between the transcutaneous pCO2 (TranspCO2) value measured by the Tosca system and the pCO2 value obtained by arterialised ear lobe blood gas (ELBG) measurements during the set up procedure for stable patients starting on long term NIV.
Methods: Continuous transcutaneous CO2 monitoring was established before the commencement of NIV. The ELBG samples were taken as part of our normal clinical practice and a direct comparison was made with the TranspCO2 values at identical time points. Fifty seven ELBG samples were taken from 27 patients (18 male, 9 female). Twenty six were taken at the beginning of the set up procedure (T0) and 24 samples were taken between hour 1 and hour 2(T>1<2). A further seven samples were recorded at a later time point beyond two hours (T>2) as clinically indicated. Statistical analysis was performed using a paired t test and the 95% limits of agreement.
Results: There was no significant difference in the mean values for TranspCO2 and the ELBG CO2 measurements when all samples were analysed (n = 57) p = 0.26 or at individual time points T0 (n = 26) p = 0.13: T>1<2 (n = 24) p = 0.52: T>2 (n = 7) p = 0.28. The 95% limits of agreement between the two methods are shown in the table.
The 95% limits of agreement would suggest that there may be a clinically relevant difference between the CO2 values obtained by the two methods. The consistency of the results (up to two hours) support our view that this transcutaneous CO2 monitor remains useful in detecting trends in CO2 during the initiation of NIV in stable patients. Ear lobe blood gas measurement remains our gold standard for the estimation of adequate gas exchange
Abstract P75
P76 SYMPTOMS OF SLEEPINESS AND BREATHING PAUSES IN PROFESSIONAL SCOTTISH BUS DRIVERS
H. M. Engleman, E. A. Hill, L. Anderson, T. W. Mackay, M. Vennelle, N. J. Douglas. Department of Sleep Medicine, University of Edinburgh, UK
Background: Previous surveys have shown a high prevalence of obstructive sleep apnoea/hypopnoea syndrome (OSAHS) among professional drivers.
Methods: A survey of sleep, breathing, daytime sleepiness, and accidents was conducted in drivers at local bus garages, with trade union help.
Results: Of 1377 drivers approached, 550 (40%) returned questionnaires, with 533 (18 female) valid responses, from drivers of average age 43 (SD 16) years and body mass index (BMI) 28.5 (SD 7.8) kg/m2. 199/533 drivers (37%) had an Epworth sleepiness score 38, 180/514 (35%) reported snoring 34 nights/week and 67/497 (13%) breathing pauses 3one night/week. A minimal criterion for OSAHS (Epworth sleepiness score 38 and significant snoring or breathing pauses) was met by 17%.
Abstract P76 Prevalence of OSAHS symptoms by response size (n = 550)
“Don’t know” responses varied by item, from none for Epworth score, 116/514 (23%) for snoring and 209/497 (42%) for breathing pauses. Combining “don’t know” responses with those for significant snoring and breathing pauses produced 354/495 (72%) with possible symptoms, of whom 145 (29%) also showed raised Epworth score (38). Epworth scores were weakly correlated with near miss and minor accidents (rho = 0.13, with at work (p<0.01) and with off duty near misses (rho = 0.29, p<<0.001) in the preceding five years.
Conclusions: A symptomatic sleep survey found a high prevalence of bus drivers reporting risk factors for OSAHS, with prevalence on symptomatic criteria estimated conservatively at 17%, with 29% potentially at risk. Daytime sleepiness was weakly linked with more accidents both on and off duty
Funded by: Chief Scientists Office, Scotland.
P77 SERUM ANGIOTENSIN CONVERTING ENZYME IS CORRELATED WITH NOCTURNAL DIASTOLIC BLOOD PRESSURE IN PATIENTS WITH THE SLEEP APNOEA SYNDROME
K. E. Lewis1,2, A. Benjamin1,3, P. Ebden3, I. Bartle1, D. Giffin3. 1Prince Philip Hospital, Llanelli; 2University of Wales Swansea; 3Singleton Hospital, UK
Introduction: Measurements of serum angiotensin converting enzyme (ACE) in the sleep apnoea syndrome (SAS) have shown variable results and its clinical importance in determining blood pressure (BP) and vascular events in SAS is still unknown. Single or even mean 24 hour BP readings may not be sensitive enough to disclose subtle relationships between serum ACE, AHI, and BP (especially at night). We correlated daytime serum ACE and mean nocturnal BP in patients with and without SAS.
Methods: Twenty two consecutive attenders at a sleep disordered breathing clinic had (afternoon) serum ACE and 24 hour BP recorded before sleep studies. Those taking antihypertensives or with granulomatous disease were excluded. 14 patients had SAS (daytime sleepiness and AHI >10 events per hour). Eight patients had daytime sleepiness and an AHI <10 events per hour, but were otherwise similar (see table).
Abstract P77
Results: Pearsons correlation between serum ACE and mean nocturnal diastolic BP in the SAS group: r = +0.51, p = 0.06 and in the non-SAS group: r = −0.24, p = 0.56. Correlations between readings for nocturnal systolic BP and nocturnal mean BP were not statistically significant for either patient group. Median serum ACE in the SAS group was 44 ng/ml compared to 22 ng/ml in the non-SAS Group (p = 0.08). All measures of BP (mean daytime and nocturnal diastolic and systolic) were higher by 2–3 mm Hg in the SAS group but these did not reach statistical significance.
Conclusions: Daytime serum ACE may be an important positive predictor of nocturnal diastoloic BP in patients with SAS. Larger group sizes may detect differences in serum ACE between SAS and controls (with similar Epworth scores/BMI). Measuring nocturnal serum ACE and recording the effects of CPAP on serum ACE in SAS, are ongoing.
P78 INITIAL PATIENT PARAMETERS IN THOSE COMPLIANT WITH CPAP THERAPY FOR OBSTRUCTIVE SLEEP APNOEA SYNDROME AFTER ONE YEAR
P. C. Russell, S. A. Sims, F. Leszkowski, T. C. Stokes, J. R. Webb. Queen Elizabeth Hospital, Stadium Road, Woolwich, London SE18 4QH, UK
Background: Compliance with nocturnal continuous positive airway pressure (CPAP) in patients with the obstructive sleep apnoea syndrome (OSAS) is variable as identified by CPAP clock-time counters (
). Patient compliancy with CPAP after 1, 3, and 6 months has been linked to various patient parameters at the time of diagnosis of OSAS (
;
).
Objective: To retrospectively identify initial patient characteristics in relation to mean daily CPAP compliance 12 months after commencing CPAP therapy in a district general hospital population.
Methods: This study assessed 123 patients diagnosed with OSAS in the Greenwich borough from September 1996 to June 2004 who continued CPAP therapy after 12 months from initiation. Initial patient parameters included age, sex, body mass index (BMI), apnoea hypopnoea index (AHI) >10 events/hour, oxygen desaturation index >4% (ODI) >10/hour, Epworth Sleepiness Scale (ESS), Stradling Sleep Questionaire (SSQ), days from diagnostic sleep study to CPAP titration, and fixed CPAP pressure. Compliance was defined as mean number of hours the CPAP device was switched on per day. CPAP usuage was derived from the built-in hour counter. Patients were unaware of their CPAP monitoring.
Results: A group of 54 (44 male, 10 female; 44%) OSAS patients with low CPAP compliance (⩽4 hour/day) was compared with 69 (58 male, 11 female; 56%) patients with high compliance (>4 hour/day) at 12.3 (SD 2.2) and 12.8 (SD 2.0) months, respectively. Mean values of age (48.3 v 49.7 years), BMI (38.9 v 38.9 kg/m2), positive ESS⩾11/24, (15 v 15) and SSQ⩾21/52 (29 v 29), time from diagnostic study to CPAP trial (54 v 46 days) and CPAP pressure (10.9 v 11.4 cmH20) were not significantly different between low and high CPAP compliancy groups. There was a tendency to a higher initial AHI (40 v 48/hour, p = 0.09) and ODI (39 v 48/hour, p = 0.15) in the more compliant group, but this was not statistically significant. A subgroup analysis of very low (⩽2 hours/day) and very high (>6 hours/day) CPAP compliance also showed no significant differences between these parameters. Of the 123 patients, there was no correlation between compliance and initial ESS, SSQ, ESS+SSQ, age, sex, CPAP pressure, and time between diagnosis of OSAS and CPAP trial. However, a weak, but significant, correlation was found between CPAP compliance and initial AHI (r = 0.19, p<0.05) and initial ODI (r = 0.19, p<0.05).
Conclusions: There appear to be few objective measurements that predict good compliance with CPAP usage after one year. Initial AHI and ODI have a weak, but significant, correlation with compliancy levels after one year of CPAP use. Sleep questionnaires before CPAP therapy, however, are not useful in differentiating long term CPAP compliance in OSAS patients.
P79 AUTOTITRATING CPAP FOR TREATING OBSTRUCTIVE SLEEP APNOEA: A BIMODAL RESPONSE
E. M. Williams, B. Coker, A. Boal and B. V. Prathibha. William Harvey Hospital, Ashford, Kent, UK
Introduction: Obstructive sleep apnoea (OSA) is a widely recognised disorder and the mainstay of treatment is the application of continuous positive airway pressure (CPAP) during sleep. To estimate the optimum pressure required to treat OSA, autotitrating devices can be used. This retrospective study aims to assess the correlation between the optimum pressure required for treatment and the body mass index (BMI) and apnoea-hypopnea index (AHI).
Methods: Forty five patients (mean age 55 (SD 12) years, M34:F11), diagnosed with OSA, underwent the autotitrating CPAP trial (Remstar auto-plus). Statistical regression analysis was performed on the data to find associations between BMI, Epworth score, AHI, and the optimum pressure required to treat the OSA.
Results: Overall the optimum pressure used was 7 (SD 2) cm H2O (n = 45). There was no obvious correlation between optimum pressure and BMI (35 (SD 7) kg/m2, n = 30). However between AHI and optimum pressure there was a bimodal relation when the AHI score was 30 or greater (see fig). In the main group (open circles, AHI <30 and hatched circles AHI ⩾30, n = 36) for every 10 point rise in AHI the optimum pressure increased by 1.6 cm H2O, r2 = 0.66, p<0.001. In some patients (closed circles, n = 9), when the AHI was ⩾30 the optimum pressure was not correlated (r2 = 0.30, p<0.13), with the optimum pressure remaining around 6.5 (SD 0.7) cm H2O across all AHI values.

Discussion: This study shows no correlation between BMI and the CPAP required to treat OSA but shows a bimodal response in relation to AHI. This suggests that other factors are involved in addition to the AHI in determining the optimum pressure required to treat OSA.
P80 PREVIOUSLY UNDIAGNOSED OBESITY HYPOVENTILATION SYNDROME: AN INCREASINGLY IMPORTANT CAUSE OF ACUTE ON CHRONIC RESPIRATORY FAILURE IN EMERGENCY ADMISSIONS
J. K. Quint, L. Ward, A. G. Davison. Southend Associate University Hospital NHS Trust
Introduction: Nearly one quarter of all adults in the UK are classified as clinically obese, and the diagnosis of diseases associated with obesity is rapidly increasing.1 Recently, we have noticed an increase in acute admissions in obese individuals with type II respiratory failure of initially unknown cause in whom a diagnosis of obesity hypoventilation syndrome (OHS) was eventually made.
Methods: We have gathered data on 11 patients diagnosed with OHS in the last nine years, looking specifically at the method of presentation for each patient (outpatients or A+E), symptoms, comorbid factors, BMI, diagnosis on admission, blood gases on admission, lung function, sleep studies, and subsequent management.
Results: Seven were male, four female; the mean age was 59 (SD 12) years. Mean BMI 52.7 (SD 16.6) (range 37–102). Two patients were current smokers, one ex-smoker, and eight never smokers. Seven patients were hypertensive, three were known hypothyroid (two on treatment), two had asthma. Only two cases presented prior to 2002, and nine from 2002 to present day. Eight presented to A&E with acute type II respiratory failure of unknown cause, (pH 7.25 (SD 0.15), pCO2 11.6 (SD 4.0), HCO3− 34.9 (SD 4.5)), six of these had decompensated and developed respiratory acidosis (pH <7.35). Three patients presented to respiratory outpatients (pH 7.44 (SD 0.03), pCO2 7.02 (SD 0.78), HCO3− 35.1 (SD 1.4)). At presentation, all had increasing shortness of breath lasting days to months, one had acute bronchitis, another asthma. Sleep studies showed a mean Apnoea/Hypopnea Index score of 33/hour (SD 22), oxygen desaturations per hour mean of 39 (SD 37). The range of the mean nocturnal oxygen saturation was 66% to 89.9%. The mean Epworth sleep score was 15 on presentation (range 5–22). Mean FEV1 was 1.45 (SD 0.54) and FEV1/FVC ratio was 76% (SD 7). Five patients required management with Bipap acutely, three patients required admission to ITU, (two intubated). One patient has required treatment with Bipap long term, eight CPAP. One patient died due to non-compliance with treatment. One has improved with weight loss alone. At follow up the mean EPS was 3 (range 0–10), blood gases on air; pH 7.46 (SD 0.10), pCO2 5.94 (SD 1.15), pO2 8.59 (SD 1.38), HCO3− 28.6 (SD 4.1).
Conclusion: In eight cases (six with decompensated OHS) presenting to A&E, the diagnosis of OHS as the cause of respiratory failure was not appreciated by the admitting team until referral to a chest physician had been made. Decompensated OHS may occur spontaneously or secondary to an added respiratory load—for example, asthma, bronchitis. Decompensated OHS appears to be poorly recognised clinically and has received little attention in the literature.
1
P81 IS THE PRESENCE OF THE METABOLIC SYNDROME A PREDICTOR OF DISEASE SEVERITY IN OBSTRUCTIVE SLEEP APNOEA SYNDROME?
O. Lyons, S. Walsh, A. Kavanagh, S. Zia, J. J. Gilmartin. Regional Respiratory Centre, Merlin Park Regional Hospital, Galway, Ireland
Introduction: There is significant evidence to support an association between obstructive sleep apnoea syndrome (OSAS) and metabolic syndrome (
). While polysomnography remains the gold standard for diagnosis of OSAS it is an expensive and limited resource. Furthermore there is no single screening method available that predicts the probability of a subsequent diagnosis of OSAS in a patient.
Methods: Between January and December 2003, 101 patients referred to a Regional Respiratory Centre for investigation of possible OSAS underwent formal sleep studies. A retrospective analysis of the medical records of these patients was performed. The following parameters were recorded: patient demographics, history of comorbid disease, Epworth Score, BMI, fasting glucose and lipid levels, and blood pressure. Duration of time from initial referral to date of sleep study was also recorded. The diagnosis of OSAS was made by polysomnography. Severity of OSAS was determined by Apnoea-Hypopnoea Index (AHI). Metabolic syndrome was diagnosed according to 2001 National Cholesterol Education Program criteria.
Results: 49 patients were diagnosed with OSAS (mean age 52.9) and 47 had normal studies (mean age 46.8). The mean waiting time from initial referral to sleep study was 141 days in OSAS group compared to 192 days in normal study group.
Of the 49 patients diagnosed with OSAS the metabolic syndrome was present in 21 (42.9%). Of the 23 patients with severe OSAS (AHI >40) 13 had metabolic syndrome (56.5%). In the 47 patients with normal studies the metabolic syndrome was present in only five patients (10.7%).
Conclusion: These data support the known association between OSAS and metabolic syndrome. Indeed it suggests that the presence of metabolic syndrome may predict an increased probability of more severe disease. Given the unacceptably long waiting list and limited resources we propose that the recognition of the metabolic syndrome at presentation may be of use in stratifying patients into high or low clinical suspicion of OSAS thus enabling prioritisation of those deemed at high risk.
P82 THE EFFECT OF MANDIBULAR ADVANCEMENT SPLINTS ON STEERING SIMULATION IN OBSTRUCTIVE SLEEP APNOEA SYNDROME: PRELIMINARY RESULTS
S. E. A. Fairbairn1, J. Richards1, M. Gregory2, M. A. Hack1. 1Gwent Sleep Centre, Newport Chest Clinic, Gwent NHS Trust; 2Maxillofacial Department, Royal Gwent Hospital, Gwent NHS Trust, UK
Introduction: Patients with obstructive sleep apnoea syndrome (OSAS) have been shown to have an increased road traffic accident rate of between twice and seven times that of normal. Untreated OSAS patients show impaired performance on steering simulators compared to normal subjects,1 and show improvement following continuous positive airway pressure (CPAP). Mandibular advancement splints (MAS) are a recognised treatment option for OSAS,2 but little work has been done to show there effect on steering simulator performance.
Methods: Twelve consecutive patients, with diagnosed OSAS (4%dip/hour>10), defined sleepy (ESS>10), with suitable dentition for MAS, were recruited to the study. Patients drove on the steering simulator (Stowood Scientific) before and 6–8 weeks following fitment of the custom made MAS. Primary data analysed were collected in the form of standard deviation (SD) from the centre of the road (theoretical perfect path) and reaction time (RT).
Results: See table. Nine patients completed the study (one withdrew, two intolerant of MAS), (seven men, mean age 50.4 (SD 10) years). Statistical analysis for non-parametric data using Wilcoxon signed rank test. A p value of <0.05 was considered to be significant.
Abstract P82 Median values (5th to 95th centiles)
Conclusions: MAS leads to significant improvement in subjective sleepiness and objective measures of sleep disturbance. OSAS is known to impair driving performance and MAS significantly improves steering ability on the simulator, but not to the baseline level for normal subjects or OSAS patients on CPAP. Reaction time improves but does not reach significance. The acceptability of MAS as an alternative therapy in patients with OSAS who continue to drive needs to be studied further.
1
2
P83 DO HEALTH RELATED QUALITY OF LIFE IMPROVEMENTS OVER A TWO WEEK HOME CONTINUOUS POSITIVE AIRWAY PRESSURE TRIAL FOR OBSTRUCTIVE SLEEP APNOEA PREDICT LONG TERM COMPLIANCE?
A. R. Proctor, C. Billings, C. G. Billings, E. Moloney. Respiratory Function Unit, Royal Hallamshire Hospital, Sheffield Teaching Hospitals NHS Foundation Trust, Glossop Road, Sheffield S10 2JF, UK
Introduction: In short term studies, continuous positive airway pressure (CPAP) has been shown to improve health related quality of life (HRQoL) in obstructive sleep apnoea (OSA) patients. We report a long term follow up of 82 patients treated with CPAP for an average of 18 months. To improve management of patients we have explored the value of HRQoL measures in anticipating compliance issues.
Methods: Hours of use and HRQoL data (Medical Outcomes Questionnaire Short Form 36) were collected pre and post a two week CPAP trial and at annual review of treatment. A retrospective data analysis was performed.
Results: At 18 months the initial improvements seen after the CPAP trial were maintained in QoL domains (p<0.05). A correlation was observed between changes in energy following the CPAP trial and long term use (r = 0.316; p<0.004). There was no correlation between long term compliance and baseline EV scores. Defining an average usage of 4 hours/night over the follow up period as acceptable compliance, significant differences between compliers and non-compliers were found (see table).
Abstract P83
Conclusion: Compliers perceived a greater subjective improvement in energy over the two week CPAP trial. It is the change in energy/vitality (E/V) score over the CPAP trial that best predicts long term compliance (p<0.005). Further research is needed to assess how useful changes in HRQoL scores during a trial of CPAP therapy are in the management of OSA patients.
P84 PROGNOSIS FOLLOWING INITIATION OF NON-INVASIVE VENTILATION IN PATIENTS WITH OBESITY HYPOVENTILATION SYNDROME IN A TERTIARY CENTRE
S. A. Haines, J. I. M. Footitt, M. Khan, A. K. Simonds & M. I. Polkey. Royal Brompton Hospital, London, UK
Introduction: Obesity is increasing in prevalence in developed countries; a minority of such patients develop obesity hypoventilation and are treated with non-invasive ventilation (NIV). Knowledge concerning the long term prognosis of such patients is relevant to planning their clinical care however few such data exist.
Method: The caseload of OHV patients starting NIV at the Brompton between 1995 and 2005 was identified by interrogating a computerised database. 71 patients were identified with a mean follow up of 38 (SD 25) months. The case notes of these patients were reviewed and where necessary additional details were obtained by contacting the patient’s local physician.
Results: The mean age of the patients was 55.9 (SD 11.7) years with a mean BMI 49 (SD 10.2) kg/m2. Comorbidities were COPD/asthma (34%), Type II diabetes (38%) and hypertension or heart disease (49%). 16/71 (23%) patients died; the one year survival was 94%. Survival time (in months) shown in the figure. Cox regression was used to identify factors at presentation suggesting a poorer prognosis: after adjustment for age and BMI only FEV1 and FVC retained significant predictive value when they were included separately into the model. Hazard ratios (CI) were 0.08 (0.01 to 0.54) and 0.19 (0.05 to 0.7) respectively.
Conclusion: After initiation of NIV obese patients have a comparable prognosis to many other patients receiving home mechanical ventilation. Aggressive treatment of such patients is justified.

Molecular mechanisms of lung disease
P85 LONGITUDINAL PROTEOMIC ANALYSIS OF SPONTANEOUS SPUTUM TO ASSESS LUNG INFLAMMATION IN CYSTIC FIBROSIS
R. D. Gray1,2, M. Imrie1,2, A. C. Boyd2, J. A. Innes1, A. P. Greening1. 1Respiratory Medicine Unit, Western General Hospital, Edinburgh, UK; 2Molecular Medicine Centre, University of Edinburgh, UK
Introduction: Cystic fibrosis (CF) lung disease is characterised by cycles of infection and a progressive decline in lung function. Presently available non-invasive measures of lung inflammation in CF are limited due to a lack of sensitivity and specificity. To this end we have sought non-invasive markers from spontaneous sputum in patients with CF. Previous work performed by this group has demonstrated the presence of proteomic markers of CF lung disease, in particular Calgranulin A (CF antigen), in induced and spontaneous sputum using highly sensitive mass spectrometry (SELDI TOF surface enhanced laser desorption ionisation time of flight) in cross sectional studies. We have used SELDI TOF to assess the utility of this technique in monitoring longitudinal change in proteomic markers. Specific ELISA was also performed for Calprotectin (Calgranulin A/B) in sputum.
Methods: 12 adults with CF were recruited when attending the Scottish Adult CF unit with exacerbation requiring antibiotic therapy. Spontaneous sputum was obtained and spirometry performed on presentation and at cessation of antibiotic therapy. Sputum was processed to yield cell pellet for cytological examination and fluid phase for proteomic assessment. Fluid phase sputum was applied to a weak cation exchange SELDI TOF chip surface and mass spectrometry performed. ELISA for Calprotectin was performed in parallel.
Results: Based on previous observations, 15 protein markers were selected on SEDLI TOF for assessment. Four markers significantly reduced from exacerbation to recovery (p<0.05). Of these Calgranulin A and B were identified, the reduction of these markers being demonstrated also by Calprotectin ELISA. FEV1 also changed (improved) significantly during exacerbation (p<0.05). Sputum cytology revealed neutrophil counts generally in excess of 95% in both exacerbation and recovery samples.
Conclusion: We have demonstrated the utility of proteomic techniques in the longitudinal assessment of CF lung disease. Recruitment of patients in this study is on going and this abstract represents pilot data. The most abundant marker was Calgranulin A (CF antigen). In this study we found sputum neutrophil count unhelpful in the monitoring of an exacerbation. Proteomic markers such as Calgranulin A may offer a more specific means of monitoring airways inflammation by sputum analysis.
P86 METHYLATION AND CONSERVATION ANALYSIS OF CPG ISLANDS IN THE ADAM33 GENE
Y. Yang, H. M. Haitchi, S. Puddicombe, R. Hayes, S. T. Holgate, D. E. Davies. Brooke Laboratories, Division of Infection, Inflammation and Repair, School of Medicine, University of Southampton, Southampton, UK
Rationale:ADAM33 is a novel asthma susceptibility gene expressed in lung fibroblasts, but not in epithelial cells (
.
). To study the ADAM33 gene regulatory mechanisms, methylation, and conservation status were analysed at three CpG islands in the promoter and two intragene regions in lung fibroblasts and epithelial cells.
Methods: DNA was extracted from cultured human lung fibroblasts and epithelial cells and then treated by hypohydrogen sodium bisulphite; this converts unmethylated cytosines in genomic DNA to uracil, whereas 5-methylcytosine remains unchanged. The modified DNA was amplified using PCR followed by cloning, sequencing and analysis. The conservation was analysed via http://genome.ucsc.edu.
Results: At the promoter, DNA was unmethylated in ADAM33 expressing fibroblasts, but hypermethylated in ADAM33 repressed epithelial cells. DNA was hypomethylated on one intragene CpG island in fibroblasts, but was hypermethylated in epithelial cells. However, at another intragene CpG island, DNA was hypermethylated in both fibroblasts and epithelial cells with three consistently unmethylated CpGs out of 18 CpGs. The sequence is not very conserved at the promoter CpG island, but a number of conserved sequences appear at both intragene CpG islands.
Conclusion: Methylation of CpG islands in the promoter regulates ADAM33 gene expression. The role of methylation in the conserved intragene CpG islands warrants further investigation.
Supported by The Rayne Foundation, UK.
P87 CODON 178 GENETIC POLYMORPHISM OF THE DNA REPAIR PROTEIN O6-METHYLGUANINE-DNA METHYLTRANSFERASE AND LUNG CANCER
P. A. J. Crosbie1, A. C. Povey2, G. McGown3, M. R. Thorncroft3, R. Agius2, P. V. Barber1, M. F. Santibanez-Koref4, G. P. Margison3. 1North West Lung Centre, Wythenshawe Hospital, Manchester; 2Centre for Occupational and Environmental Health, University of Manchester; 3CR-UK Carcinogenesis Group, Paterson Institute for Cancer Research, Manchester; 4Institute of Human Genetics, University of Newcastle, UK
Introduction: The DNA repair protein O6-methylguanine-DNA methyltransferase (MGMT) removes the highly mutagenic DNA adduct O6-methylguanine and therefore protects against the carcinogenic effects of alkylating agents. We have previously reported that MGMT activity was higher in subjects homozygous for the A-G polymorphism at codon 178 than heterozygous subjects (AG) or subjects with the wildtype (AA).1 As cigarette smokers are exposed to tobacco-specific nitrosamines, which cause cancer in part by the formation of O6-alkylguanine lesions, we have examined whether the MGMT codon 178 polymorphism is associated with lung cancer susceptibility.
Methods: Subjects were recruited from the Bronchoscopy Unit and Chest Clinic in Wythenshawe Hospital. Subjects were over 40 years and white and did not have a previous history of cancer. All subjects were interviewed using a risk factor questionnaire and all provided a blood sample. Cases were defined as those patients with incident lung cancer and controls were cancer free. DNA was separated from whole blood using Qiagen columns. Genotype was determined by restriction digest PCR.
Results: 401 subjects have been recruited and genotyped—151 cases and 250 cancer free controls. Cases were significantly older than controls (69.2 (SD 10.4) years v 65.9 (SD 10.6) years, p = 0.003) but not significantly different in sex, ever smokers, cigarettes smoked per day in current smokers and packyears. The frequency of the codon 178 polymorphism in cases and controls is shown in the table. There was no difference in the allele frequency between cases and controls. 2.9% of controls were GG homozygotes as compared to 0.7% of controls (p = 0.15).
Abstract P87 Codon 178 polymorphism in study population
Discussion: The higher frequency of the GG homozygotes in the control population is consistent with higher MGMT activity in these subjects but further work is required to ascertain whether codon 178 is associated with lung cancer susceptibility.
1
P88 A NOVEL CYCLOOXYGENASE-2 VARIANT, -607T>C, ASSOCIATES WITH SUSCEPTIBILITY TO SARCOIDOSIS IN AFRO-CARIBBEANS
L. Young, G. Chan, A. Papafili, H. Booth, C. Read, R. Marshall, G. Laurent, R. McAnulty, M. Hill. University College London, UK
Background: In normal lung fibroblasts, upregulation of cyclooxygenase (COX)-2 results in the synthesis of antifibrotic prostaglandin E2 (PGE2). Patients with idiopathic pulmonary fibrosis1 and sarcoidosis2 have low levels of lung PGE2 despite the presence of mediators that can stimulate its synthesis. This is thought to be due to a reduced capacity to upregulate COX-2, which may in part result from sequence variants in the regulatory regions of the COX-2 gene. We previously reported a functional promoter variant, −765G>C, in a white study of healthy UK subjects (n = 454) and sarcoidosis patients (n = 194) and shown that carriage of the −765C allele is associated with the risk of developing disease (OR = 1.66 (95% CI 1.16 to 2.39), p = 0.006).3 We have now identified a further variant, −607T>C, that is only found in Afro-Caribbean subjects. These subjects develop progressive lung disease more often than whites with sarcoidosis. We now report on −765G>C and −607T>C in Afro-Caribbeans.
Methods: The −607T>C and −765G>C variants were detected in Afro-Caribbean subjects by direct sequencing of the COX-2 promoter.
Results: In a study comparing UK Afro-Caribbean sarcoidosis patients (n = 93) and healthy controls (n = 233), carriage of −607C is associated with susceptibility to sarcoidosis (OR = 2.24 (95% CI 1.16 to 4.32), p = 0.015). Carriage of the −765C does not appear to associate with sarcoidosis in this ethnic group (OR = 1.19 (95% CI 0.74 to 1.93), p = 0.47). The −607T>C and −765G>C are in weak linkage disequilibrium (D′ = 0.62, p = 0.03).
Conclusions: This is the first report suggesting COX-2 variants associate with susceptibility to sarcoidosis in different ethnic groups. The function of the −607T>C is being investigated. It is possible that functional polymorphisms may interact to modify COX-2 expression, and may help explain the difference in severity of disease seen amongst Afro-Caribbeans compared to whites.
1
2
3
P89 IDENTIFICATION OF PAR1-G PROTEIN SIGNALING PATHWAYS INVOLVED IN THROMBIN INDUCED CCL2 RELEASE
X. L. Deng, P. F. Mercer, G. J. Laurent R. C. Chambers. Centre for Respiratory Research, University College London, UK
Introduction: Activation of the coagulation cascade is a key event in the development of fibroproliferative lung disorders, including acute respiratory distress syndrome (ARDS) and idiopathic pulmonary fibrosis (IPF). In experimental models of lung injury, activation of proteinase-activated receptor-1 (PAR1) by coagulation proteinases is critical in driving both the inflammatory and fibrotic response. PAR1 exerts its pluripotent cellular effects by concomitant activation of Gαi/o, Gαq, and Gα12/13. We have previously shown that protection from lung inflammation and fibrosis in PAR1 deficient (PAR1 KO) mice is accompanied by the reduction in lung levels of the potent thrombin inducible protein CCL2 (MCP-1/JE). The aim of this study was to examine the signaling pathways by which thrombin induces the release of this chemokine by cultured murine lung fibroblasts.
Methods and Results: Wild type (WT) murine lung fibroblasts and corresponding PAR1 KO fibroblasts were exposed to thrombin, TFLLR-NH2 and FTLLR-NH2 (PAR1 peptide agonist and control peptide respectively), in the presence or absence of pertussis toxin (PTX, Gαi/o inhibitor), Ro-318425 (protein kinase C (PKC) inhibitor), Y-27632 and H-1152 (Rho kinase inhibitors). CCL2 protein secretion in cell culture supernatant was assessed by ELISA. Thrombin induced CCL2 release by WT fibroblasts in a time and dose dependent manner, with a maximal response of ninefold at 10 nM thrombin at 24 hours. These effects were mimicked by the PAR1 agonist TFLLR-NH2, whereas the control peptide FTLLR-NH2 had no effect. PAR1 KO fibroblasts similarly failed to respond. WT fibroblasts were preincubated with PTX, Ro-318425, Y-27632,and H-1152 before 10 nM thrombin stimulation for six hours. Measurement of CCL2 protein levels demonstrated that PTX inhibition of Gαi/o had no effect on CCL2 release induced by thrombin, whereas Ro-318425 inhibition of PKC reduced CCL2 release by 49 (SD 6)% (p<0.05 v control). Y-27632 and H-1152 inhibition of Rho kinase inhibited CCL2 release by 44 (SD 5)% and 34 (SD 8)%, respectively (both p<0.05 v control).
Conclusion: Taken together these data show that activation of PAR1 by thrombin induces CCL2 release by murine lung fibroblasts, at least in part, via PKC and Rho kinase signaling pathways. These kinase pathways are likely to be downstream of activation of Gαq and Gα12/13, respectively. Selective inhibition of PAR1 signaling pathways may represent a novel therapeutic approach for a number of respiratory conditions associated with excessive coagulation proteinase signaling.
P90 THE POTENTIAL ROLE OF INTERLEUKIN-17 IN AIRWAY INFLAMMATION AND REMODELLING IN POST-TRANSPLANT OBLITERATIVE BRONCHIOLITIS
D. M. Murphy1, I. A. Forrest1, C. Ward1, P. A. Corris1, G. Pritchard1, D. Jones2, A. J. Fisher1, J. J. Egan3, T. E. Cawston2, J. L. Lordan1. 1The Applied Immunobiology and Transplantation Research Group, The Faculty of Medical Sciences, The University of Newcastle-upon-Tyne, Newcastle-upon-Tyne NE2 4HH, UK; 2The Musculoskeletal Research Group, The Faculty of Medical Sciences, The University of Newcastle-upon-Tyne, Newcastle-upon-Tyne NE2 4HH, UK; 3The Irish Lung Transplant Programme, The Mater Hospital, Eccles Street, Dublin 1, Ireland
Introduction: Obliterative bronchiolitis (OB) is the main cause of premature allograft failure following lung transplantation. It is characterised by airway neutrophilia, epithelial injury and progressive fibroproliferative obliteration of small airways. Airway lymphocytosis is well described in the transplanted lung, particularly during acute rejection episodes. However, potential mechanisms linking this early inflammation to chronic neutrophilic inflammation and airway remodelling are poorly understood. The lymphocyte derived cytokine interleukin (IL)-17 is postulated to play a major role in airway neutrophilic inflammatory conditions.
Aims: To characterise airway expression of IL-17 in lung transplant recipients and assess the effects of IL-17 on the airway epithelium, in particular, its potential effects on neutrophilic inflammation and remodelling.
Methods: Transbronchial biopsies from lung allografts with airway inflammation were stained for IL-17 and the degree of staining in the epithelium and lamina propria quantified. Confluent primary bronchial epithelial cell cultures (PBECs) were established from bronchial brushings of stable lung allografts (n = 10). PBECs were then co-incubated with IL-17 and the resulting levels of IL-8, IL-6, GCSF, GM-CSF, VEGF, MMP-2, and MMP-9 cell supernatant protein measured.
Results: Our data demonstrate variable IL-17 immunostaining of the airway epithelium and mononuclear cell infiltrate of transbronchial biopsies obtained from lung transplant recipients. PBEC stimulation with IL-17 caused significantly raised levels of IL-8, IL-6, GCSF, GM-CSF, and VEGF from baseline. Matrix metalloproteinase (MMP)-2 and -9 protein levels were not affected.
Conclusion: Our results suggest IL-17 as a potential mechanistic link between acute lung allograft rejection, neutrophil recruitment, airway remodelling, and subsequent progression to OB.
P91 THE DIVERGENT EFFECTS OF HEME ON NEUTROPHIL APOPTOSIS
D. D. Melley, G. J. Quinlan, T. W. Evans. Adult Intensive Care Unit, Royal Brompton Hospital & National Heart and Lung Institute, Imperial College, London, UK
Introduction: Neutrophils are sequestered in the alveoli of patients with acute respiratory distress syndrome (ARDS). Neutrophil clearance through apoptosis and subsequent ingestion by macrophages is an essential step in the resolution of inflammation. The cell surface receptor fas is known to activate neutrophil apoptotic mechanisms in an oxidant dependent manner. We have previously shown that heme, which is released from erythrocytes during hemolysis, delays spontaneous neutrophil apoptosis. We now speculate that heme may also lead to dysregulation of fas induced neutrophil apoptosis and thus promote inflammation, through its action as a pro oxidant.
Methods: Neutrophils from healthy volunteers were separated from whole blood by discontinuous Percoll gradient centrifugation. Cells were preincubated at 37°C for eight hours in RPMI medium with or without heme (30 μMol) and then for a further 16 hours following the addition of fas antibody (10, 30, 100 ng/ml). Apoptosis was assessed by flow cytometry following propidium iodide staining.
Results: A significant increase in the percentage of apoptotic cells was noted following incubation with fas antibody at 30 and 100 ng/ml. Moreover preincubation with heme significantly augmented apoptosis at all fas concentrations (see fig).
Conclusion: Heme augments fas induced apoptosis whilst delaying spontaneous apoptosis in isolated neutrophils. Heme induced dysregulation of apoptosis may contribute to the degree of inflammation found in patients with hemolysis.

Heme augments fas antibody induced neutrophil cell death.
P92 HUMAN SQUAMOUS CELL CARCINOMA CELL LINES CONTAIN A SELECTABLE SIDE POPULATION THAT IS CELL CYCLE DEPENDENT BUT IS NOT A CANCER STEM CELL POPULATION
K. Groot1, C. Simpson2, L. Prichard1, D. Davies2, S. Janes1. 1Centre for Respiratory Research, University College London; 2Flow Cytometry Laboratory, London Research Institute, Cancer Research UK
Introduction: A subpopulation of “side population” (SP) cells exist in a number of adult tissues. These cells, named after their characteristic appearance in flow cytometry, have a unique capacity to efflux lipophillic dyes such as Hoechst. In bone marrow and muscle, SP cells have been demonstrated to have stem cell characteristics; being able to self renew and have the capacity to form differentiated cells. The SP cell’s high efflux capacity correlates with the high expression of drug transporter proteins (including ABCG2 and ABCA3). Hence these cells may be intrinsically resistant to a number of cytotoxic drugs explaining tumour resistance and disease relapse. Neuroblastomas contain a SP population and it has been suggested that they are a cancer stem cell population.
Aim: We examined a squamous cell carcinoma cell line (H357) for the presence of an SP cell fraction and proceeded to see if it demonstrated cancer stem cell characteristics.
Methods: Cells were cultured in vitro and passaged at confluence. SP population sorting was performed by incubating 1 million cells/ml with 5 μg/ml Hoechst 33342 at 37°C for 45 minutes. Colony forming assays were performed by sorting single cells into 96 well plates (triplicates). The populations sorted were SP, and cells in G1 and G2 of the cell cycle (both non-SP).
Results: We have noted several novel characteristics of the SP cell fraction. (1) Standardisation of the cell number and Hoechst concentration is critical or the SP fraction varies. (2) The SP fraction is not a strict subpopulation of the cells but in fact Hoechst efflux was dependent on the cell cycle with highly confluent (hence quiescent cells) showing a greatly increased SP fraction. (3) The SP cells can be sorted by FACS leading to a higher SP fraction in subsequent sorts. These sorted and cultured fractions contained both SP positive and negative cells. However the non-SP fractions, once cultured after sorting, were also capable of producing an SP positive fraction (albeit smaller)—hence strongly suggesting that being SP positive is not a feature of stem cells in squamous cell carcinomas. (4) The SP and non-SP cell fractions had no difference in proliferation rate or colony formation.
Conclusion: Squamous cell cancers have an SP population that is selectable. However these cells have no characteristics of cancer stem cells in that they do not have higher differentiation potential, proliferative or colony forming capacity than non-SP cells.
P93 SERUM LIPIDS IN PIGEON FANCIERS’ HYPERSENSITIVITY PNEUMONITIS: A PLACE FOR STATINS?
K. Anderson1, I. Fraser2, N. Sattar3, M. R. Adamson1, S. Bourke4, C. McSharry2. 1Departments of Respiratory Medicine and Pathology, Crosshouse Hospital, Kilmarnock; Departments of 2Immunology, 3Biochemistry, University of Glasgow; 4Newcastle General Hospital, UK
Background: The pathology of hypersensitivity pneumonitis (HP) is best described as a temporally uniform non-specific interstitial lung disease (Katzenstein, 1990) and characterised variously by granulomatous and lymphocytic inflammation, the accumulation of lipid laden (or foamy) macrophages and cholesterol clefts, as well as ultrastructural vascular changes. As a first step in the investigation of these latter, less well recognised, perhaps overlooked phenomena, a study was performed to identify and quantify the serum lipid profile of a volunteer cross sectional group of pigeon breeders attending a pigeon show.
Methods and Results: Blood samples were obtained from 48 pigeon fanciers (24 with symptoms suggestive of HP), and nine healthy control subjects with no avian exposure; all non-smokers. Plasma IgG antibody (μg/ml) to inhaled avian antigen, and C-reactive protein (μg/ml) were measured by enzyme immunoassay and lipid profile by nephelometry (mmol/l), all median and i-q range. The pigeon fanciers with symptoms of HP had higher levels of IgG antibody to avian antigen than asymptomatic or control subjects (39.0 (22.2 to 54.7), 12.0 (2.5 to 46.0), and 1.0 (1.0 to 1.0), p<0.01), and higher CRP levels (2.8 (1.6 to 8.0), 1.7 (1.2 to 6.4), and 1.1 (0.7 to 2.1), p<0.05). The antibody and CRP levels correlated (r = 0.244, p = 0.04). In the whole study group, the plasma lipids levels were: Cholesterol 5.32 (4.68 to 6.10), Triglyceride, 1.74 (1.15 to 2.74) and HDL cholesterol 1.28 (1.04 to 1.55). The triglyceride levels correlated with CRP (r = 0.31, p = 0.008) and IgG antibody (r = 0.32, p = 0.006). The cholesterol level correlated with the IgG antibody titre (r = 0.32, p = 0.006).
Conclusions: In this group of pigeon fanciers, we have demonstrated modest but significant changes in the serum lipid profile associated with inflammation (measured by CRP) and specific antigen sensitisation (measured by IgG antibody). The results suggest that there are aspects of HP which include a systemic inflammatory response, with altered lipids in addition, which could contribute to the pulmonary features of the disease. Although the results are similar in some ways to other illnesses which are statin responsive, the interesting question is whether that treatment would be worthwhile in HP.
Support is acknowledged from the British National Flying Club Medical Team.
Inhaled therapies: new and old
P94 PROBLEMS WITH INHALED THERAPY IN ELDERLY CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATIENTS: TIME FOR RE-EVALUATION?
S. Jarvis, P. W. Ind, R. J. Shiner. Department of Respiratory Medicine, Imperial College School of Medicine, Hammersmith Hospital, London W12 0NN, UK
Introduction: Chronic obstructive pulmonary disease (COPD) prevalence steadily increases with age. However, the effectiveness of inhaled therapy in the elderly COPD population has rarely been evaluated. We studied a group of elderly COPD patients with a range of severity, selected from one general practice register to (1) evaluate their perceptions of their current inhaled therapy and (2) measure the peak inspiratory flow (PIF) with a hand held device while assessing its practical use in general practice.
Methods: We randomly selected a group of 53 elderly COPD patients (36 males) with a mean age of 73.5 years (range 65–87). 21 were classified as mild, 22 moderate, and 10 had severe COPD, with FEV1 mean (litre) values of 2.24 l (SD 0.4), 1.24 l (SD 0.3) and 0.88 l (SD 0.2) respectively. All patients used a metered dose inhaler (pMDI), and 12 of the patients also used a dry powder inhaler (DPI) in addition. None used a nebuliser. Patients completed a questionnaire regarding ease of use, perceived benefit from and specific problems encountered with their inhaler. Three recordings of the PIF were measured at varying inhaled resistances using the “In-Check Dial” (Clement-Clarke, UK).
Results: 46% of our patients reported “moderate difficulty” with the use of their pMDI, in contrast to 12% of DPI users. Problems included handling and coordination difficulties. 76% of the patients had been prescribed a spacer device though 85% of these did not use it regularly. A large percentage of patients (58%), using the pMDI reported good symptom relief but 53% of DPI users “did not know” with regard to perceived symptom relief from their device. There was a progressive decline in PIF with increasing resistance, and only 25% of patients achieved the required PIF recommended for some of the higher resistance DPI inhaler devices currently available. PIF values declined with age and disease severity.
Conclusions: A large percentage of these elderly patients were unhappy with, or unsure of, the effectiveness of their prescribed inhaler device. Many patients even when in a stable clinical condition were unable to generate the PIF values required to gain optimal clinical benefit. The reduction in PIF is most apparent in the most elderly patients with moderate or severe COPD. The role of nebulised inhaled therapy may need to be reassessed in the elderly COPD population.
P95 ASSESSMENT OF INHALER TECHNIQUE AND PATIENT INHALER IDENTIFICATION ON AN ACUTE ADMISSION UNIT
R. M. Jones, P. Lloyd, S. Davies, S. Keeling, G. Arumgakani, N. A. McAndrew. Wrexham Maelor Hospital, Wrexham LL13 7TD, UK
Background: Inhaled medications are important in the management of chronic obstructive pulmonary disease (COPD). Choice of inhaler system and use is in many respects as important as the drug itself. Incorrect inhaler technique is a common and persistent problem in clinical practice.
Objective: To assess whether patients using inhalers were following the correct technique for their prescribed device. In addition, we assessed whether patients correctly identified each type of prescribed device.
Methods: A specialist respiratory nurse and pharmacy technician assessed patients using inhalers, admitted via an acute admissions ward over one month. We used scoring systems in accordance with manufacturers’ guidelines to assess the adequacy of inhaler technique. 42 (27 F, 15 M) patients were identified, of whom 13 were excluded (including five due to previous technical intervention, two too unwell).
Results: Of the 29 patients assessed, mean ages were similar in all inhaler groups. MDIs were the most frequently prescribed 21/40 (52.5%) of all devices. Other devices included Hanidhaler (6), Easibreathe (5), Turbohaler (4), Accuhaler (3), and Diskhaler (1). 13 of the patients using MDIs did so in conjunction with a Volumatic device, 10 (48%) of these on a regular basis. Nine (31%) patients were on more than one type of device—seven (24%) on two and two (7%) on three different types. 20 out of 26 (77%) patients correctly identified their principal “reliever” inhaler. Nine out of 13 (69%) identified their inhaled steroid therapy as a “preventer”. No patients correctly identified their long acting β agonist (0/3) and five of 11 (45%) appropriately identified their combined steroid and long acting β agonist inhaler.
12/17 (70%) patients using MDI devices made two or more mistakes (out of eight steps) in its use. Commonest was poor actuation and inspiration synchrony (65% of cases). Of seven patients using an MDI and Volumatic, six (87%) made two or more mistakes out of eight assessed steps. No patient made over one mistake in the use of the Turbohaler (seven assessed steps), Easibreathe (10 steps), Handihaler (11 steps), or Diskhaler (nine steps). One patient with an Accuhaler (out of three assessed) made two mistakes out of eight steps.

Inspiratory flow according to age and disease severity.
Conclusion: Mistakes in MDI use, with or without a Volumatic, were more frequent than with other devices. The MDI remains the commonest used device. Of those using MDIs, less than half used them regularly with a Volumatic. The most frequent mistake with MDIs was an error critical to drug deposition. Proportionally more patients made mistakes with an MDI and Volumatic compared to MDIs alone, but Volumatic use minimises the influence of individual errors on drug delivery. Patients identified “reliever” and “preventer” inhalers well but long acting b agonist and combined therapy poorly. Poor technique leads to ineffectual drug therapy thus reducing their proven benefits on disease status and exacerbation frequency.
P96 TWO YEAR EFFICACY AND PULMONARY SAFETY OF INHALED INSULIN IN PATIENTS WITH TYPE 2 DIABETES UNCONTROLLED WITH ORAL AGENTS
L. Kuitert1, A. Barnett2, S. Pandya3, P. Kon4 for the Exubera Study Group1Barts and the London NHS Trust, London, UK; 2University of Birmingham, UK; 3Pfizer UK; 4sanofi-aventis Group UK
Objective: Inhaled insulin (INH, Exubera) offers an alternative to oral antidiabetic agents (OA) or injected insulin in patients with poorly controlled type 2 diabetes. The two year efficacy and pulmonary safety of adjunctive therapy with INH or an additional OA was examined in two studies in patients with type 2 diabetes, poorly controlled by OA monotherapy (HbA1c ⩾8%).
Methods: Patients receiving metformin (Study 1) or a sulphonylurea (Study 2) were randomized to either adjunctive INH (n = 471) or an additional OA (n = 441) for 104 weeks, with pulmonary function tests (PFTs), including FEV1 and DLCO, at 0, 24, 52, and 104 weeks. A washout evaluation of pulmonary function was carried out 12 weeks post-INH discontinuation.
Results: Mean baseline FEV1 was 2.85 l (INH) and 2.83 l (OA), and for DLCO 25.61 ml/min/mm Hg (INH) and 25.53 ml/min/mm Hg (OA). 158 (INH) and 146 (OA) patients were available for comparative analysis of PFTs at week 104. In both groups lung function declined over time. Small treatment group differences in change from baseline FEV1 were greatest at week 24 and less at later visits (see table). Differences in DLCO were small. There was no discernable treatment group difference in either PFT 12 weeks after discontinuing two years of therapy (table).
Abstract P96
Mean baseline HbA1c was 9.6% in both groups, decreasing to 7.7 (SD 1.4)% (INH) and 8.1 (SD 1.3)% (OA) at week 104. The overall rate of hypoglycaemia was lower in the INH group (INH/OA risk ratio = 0.81 (95% CI 0.71 to 0.92)). There were no severe hypoglycaemic events. The most common respiratory adverse event was cough, which was mild and transient.
Conclusions: INH is effective and well tolerated over two years as an adjunctive therapy in patients with poorly controlled type 2 diabetes (⩾8%). Treatment group differences in pulmonary function were small, did not worsen over time, were of questionable clinical relevance, and reversed upon discontinuation of therapy.
P97 INVESTIGATION OF THE EFFECT OF INSULIN ON HUMAN AIRWAY EPITHELIAL ION TRANSPORT IN VIVO
W. T. Owen, A. L. Brennan, D. M. Wood, B. J. Philips, D. L. Baines, E. H. Baker. Glucose and Pulmonary Infection Group, St George’s, University of London, UK
Background: Development of inhaled insulin for diabetes mellitus raises the question as to whether insulin has a direct effect on human airway epithelial ion transport. Insulin increased potential difference and short circuit current across rat alveolar type II cell monolayers and increased amiloride sensitive short circuit current across rat fetal distal lung epithelial cell monolayers (
). We therefore hypothesised that topical insulin would upregulate sodium transport across the human airway epithelium. We determined whether nasal insulin perfusion increased transepithelial sodium transport as measured by nasal potential difference (NPD).
Methods: The effect of insulin and placebo on NPD was compared in six healthy volunteers studied on two occasions using a randomised, double blind, placebo controlled design. Baseline NPD was measured during nasal perfusion with Ringer’s solution, then after 15 minutes of Ringer’s insulin (1 unit/ml) or placebo (Ringer’s solution) perfusion and then after 5 minutes of perfusion with Ringer’s amiloride (10−4M). Changes in maximum and amiloride sensitive NPD after insulin and placebo perfusion were compared. Blood glucose concentration was measured every 5 minutes. The study received local research ethics committee approval and participants gave written informed consent.
Results: Baseline NPD prior to insulin perfusion was −22.0 (−14.8 to −29.8) mV (median (interquartile range) and prior to placebo perfusion was −25.0 (−14.3 to −30.4) mV (p = 0.753). Insulin hyperpolarised the nasal epithelium by 1.2 (−2.4 to 1.5) mV, but this was not significantly greater than placebo (DNPD −0.25 (−2.0 to 0.5) mV, p = 0.463). Amiloride sensitive NPD was 12.8 (8.5 to 21.7) mV following insulin perfusion and 13.7 (9.0 to 18.7) mV following placebo (p = 0.917). Blood glucose fell 0.2 (SD 0.3) mM after insulin perfusion and 0.5 (SD 0.4) mM following placebo (p = 0.058).
Conclusions: Nasal insulin perfusion had no effect on transepithelial ion transport as measured by NPD. Pulmonary insulin receptors have previously been identified on the basolateral membranes of epithelial cells (
.) and lack of effect of topical insulin on nasal epithelial ion transport could be explained if insulin does not cross the nasal epithelium. This is supported by lack of change in blood glucose concentration during the experiments. If these findings are applicable to the lung, inhaled insulin can be used safely without altering pulmonary epithelial ion transport.
P98 EFFECT OF NON-INVASIVE VENTILATION ON BRONCHODILATOR DELIVERY
S. Kaul, I. M. Stell, N. Donaldson, M. J. Pokey, J. Moxham. Department of Respiratory Medicine, Kings College Hospital, London, UK
Introduction: Nebulised bronchodilators are often co-administered with NIV in acute respiratory failure secondary to a COPD exacerbation. Nebulisers are designed to deliver appropriate particles based on patient generated flow rates (8–12 l/min). However it is not known if the much higher flow rates in ventilator systems (60–180 l/min) allow equally effective delivery.
Objective: To compare the effect on lung function and blood gases of administering nebulised bronchodilator during non-invasive ventilation with nebulised bronchodilator alone in stable COPD patients.
Methods: Laboratory crossover study. 18 COPD patients: 1:1 male female ratio; mean FEV1 1.5 (47% pred). There were five main interventions: (1) bronchodilator alone (5 mg salbutamol + 500 μg ipratropium bromide via nebuliser); (2) IPAP 10 EPAP 4 only; (3) IPAP 20 EPAP 4 only; (4) IPAP 10 EPAP 4 plus bronchodilator; (5) IPAP 20 EPAP 4 plus bronchodilator.
Outcome Measures: Spirometry (FEV1, FVC), static lung volumes (TLC, RV, FRC, IC), peak flow, gas transfer (KCO), resistance using body plethysmography (RAW), VA, and earlobe capillary blood gases (PO2, PCO2, pH, bicarbonate, and Spo2) were measured before and 20 minutes after each intervention. The duration of NIV +/− bronchodilators was 30 minutes. The same flow triggered and cycled ventilator and full face mask was used throughout.
Results: Nebulised bronchodilator increased mean FEV1 by 22.5%. Nebulised bronchodilator plus NIV at 10 cm H20 increased mean FEV1 by 15%. Nebulised bronchodilator plus NIV at 20 cm H20 increased mean FEV1 by 13%. There was a significant difference between the bronchodilation produced by bronchodilator alone and IPAP 10 plus bronchodilator (p<0.05). There was a significant difference between the bronchodilation produced by bronchodilator alone and IPAP 20 plus bronchodilator (p<0.05). Parallel changes were seen with FVC, FRC, RV, TLC, and IC.
Conclusion: Nebulised bronchodilator therapy delivered concomitantly during NIV is less effective at delivering bronchodilator than nebuliser alone.
P99 SAFETY AND TOLERABILITY OF TIOTROPIUM ADMINISTRATION TO THE EYES IN HEALTHY MALE VOLUNTEERS, SIMULATING INADVERTENT EXPOSURE FROM AN INHALER
U. Feifel, G. Wallenstein. Boehringer Ingelheim Pharma GmbH & Co KG, Ingelheim, Germany
Background: Inadvertent misuse of active inhalers may lead to the drug being sprayed into the eyes. Resultant concerns include possible systemic and local effects of drugs, such as anticholinergics and β agonists, commonly administered via inhalers (
). Tiotropium is a novel, once-daily inhaled anticholinergic that has its effect through prolonged blockade of the bronchial smooth muscle muscarinic M3 receptor and is being developed as a Respimat Soft Mist Inhaler (SMI) formulation. In various situations of “misuse”—that is, in the worst case directly spraying into an eye, a total of up to 1% of a metered dose from Respimat SMI is likely to enter the eyes (
). Based on this information, this study assessed the safety and tolerability of tiotropium following ocular administration of six dose levels.
Methods: 48 healthy male subjects (mean age 32.0, weight 80.0 kg, height 178.0 cm) were randomised to receive a single dose of 0.02, 0.04, 0.08, 0.16, 0.28, or 0.40 μg tiotropium or placebo, applied as two “eye drops” (volume 50 μl) to one eye. Each group of eight subjects (six on tiotropium, two on placebo) received one of the six dose levels and the same methodology was used in all groups. Pupil diameter, pupillary reflex (via pupillometry), intraocular pressure, and accommodation were measured before and at 1, 4, 8, and 24 hours after dose. In addition, the pupillary reflex was assessed with an eye lamp at 15, 30, and 45 minutes after administration. Local tolerability in the treated eye was monitored up to 24 hours after treatment. Adverse events (AEs) were monitored throughout the study.
Results: In all subjects, both the pupil diameter and the pupillary reflex were not influenced by tiotropium and there were no clinically relevant findings or changes in intraocular pressure. There was no change in accommodation observed in any subject. Swelling, induration, calor, and rubor were not observed in the treated eyes. Twelve subjects (nine on tiotropium and three on placebo) reported mild and transient burning sensation in the treated eye lasting up to 5 minutes and did not require any form of treatment or follow up. This may have been caused by tiotropium and/or benzalkonium chloride (preservative) and/or sodium edetate (stabilising agent), which were present in the aqueous formulations.
Conclusions: Ocular administration of tiotropium, at doses higher (16-fold) than the range that could potentially enter the eyes with inhaler misuse, was safe and well tolerated. Tiotropium inadvertently exposed to the eyes via an inhalation device (such as Respimat SMI) will not cause any changes in pupil diameter, pupillary reflex, intraocular pressure, and accommodation.
P100 TIOTROPIUM: IS IT MORE COST EFFECTIVE THAN NEBULISERS IN AN EVERYDAY SETTING?
D. J. Waine, P. D. J. Handslip. George Eliot Hospital, Nuneaton, UK
Introduction: Tiotropium is a new long acting bronchodilator which has been shown, in randomised controlled trials in patients with chronic obstructive pulmonary disease (COPD), to improve trough FEV1,1 exacerbation rate, breathlessness scores, quality of life scores and need for rescue medication.2 We investigated whether it was effective in the every day setting of a district general outpatient clinic.
Methods: We audited all outpatients who underwent a trial of tiotropium, and would otherwise have been considered for nebulised therapy, over a 12 month period from September 2003.
Results: The patients had COPD of a similar disease severity to those represented in the trials but used more long acting β agonists, oxygen, and oral steroids (see table). Despite this, 50% of those with clear documentation (or 39% of all patients audited) had improved symptoms and 58% had improved spirometry compared to baseline measurements before the trial of tiotropium.
Abstract P100
Tiotropium costs £36.60 per month, compared with £47.03 for combivent (2.5/500 tds), £22.41 for salbutamol (5 mg tds), and £33.75 for ipratropium (500 mcg tds), and the cost of the nebuliser, the consumables, and servicing (totaling approximately £10 per year) need to be considered.
Conclusions: In an every day district general outpatient setting, 50% of patients trying tiotropium experienced symptomatic benefit and 58% had an improvement in FEV1, despite using more long acting β agonists, oral steroids, and nebulisers than those studied in the randomised controlled trials. Nebulisers should only be used if tiotropium has been tried first, since the cost of tiotropium is comparable to the cost of nebulised therapy and it is more convenient to administer and has better evidence for improvements in quality of life and exacerbation rate.
1
2
Infections and inflammatory mechanisms in chronic obstructive pulmonary disease exacerbations
P101 THE EFFECT OF LEVOFLOXACIN ON NEUTROPHILIC AIRWAY INFLAMMATION IN STABLE STATE CHRONIC OBSTRUCTIVE PULMONARY DISEASE: A RANDOMISED, DOUBLE BLIND, PLACEBO CONTROLLED TRIAL
R. Siva, W. Monteiro, D. Parker, M. Shelley, B. Hargadon, S. McKenna, C. E. Brightling, M. Barer, I. D. Pavord. Institute for Lung Health, Glenfield Hospital, Leicester, UK
Neutrophilic airway inflammation is thought to be associated with progression of chronic obstructive pulmonary disease (COPD). There is evidence that bacterial infection is associated with an increase in neutrophilic airway inflammation during exacerbations of COPD but less is known about the association in stable state disease. We have tested the hypothesis that a reduction in bacterial load following Levofloxacin therapy is associated with a reduction in sputum markers of neutrophilic airway inflammation in a placebo controlled double blind study.
We randomised 27 patients with stable state COPD (mean age 66, pack years 49.2,% predicted FEV1 46.0, bacterial load 5.8×106 cfu/ml) to either a course of Levofloxacin 500 mg once daily for seven days (n = 14) or placebo (n = 13). Patients were assessed at baseline and on days 7, 14, and 28. At each visit we measured spirometry, sputum differential inflammatory cell count, and quantitative bacterial load.
Overall there was no reduction in the% neutrophil count with Levofloxacin compared to placebo at day 7 (12.3 v 1.3%; mean difference of 11%; 95% CI −8.8 to 30.7, p = 0.26) or at any other time. There was no correlation between change in % neutrophil count and baseline bacterial load following placebo (r = −0.18, p = 0.55). However following Levofloxacin there was a strong and significant correlation between change in % neutrophil count and baseline bacterial load (r = −0.78, p = 0.003). Levofloxacin achieved a 26.5% (95% CI 0.5 to 52.5, p = 0.046) greater reduction in the % neutrophil count compared to placebo in patients with a baseline bacterial load of >than 106 cfu/ml (n = 12), although this effect was not evident at any other time after day 7. In this group of patients there was a reduction in supernatant IL-8 concentration of 12535 pg/ml following Levofloxacin compared to an increase in supernatant IL-8 concentration of 70658 pg/ml following placebo; mean difference 83192 pg/ml; 95% CI –7540 to 173925, p = 0.07.
In conclusion Levofloxacin reduces neutrophilic airway inflammation in patients with a bacterial load of >106 cfu/ml. This appears to be a short term effect. Further studies are required to investigate whether long term antibiotic use in patients with stable state COPD with high levels of bacterial colonisation influences disease progression.
P102 NEUTROPHIL ADHESION MOLECULES IN AN EXPERIMENTAL MODEL OF RHINOVIRUS INDUCED CHRONIC OBSTRUCTIVE PULMONARY DISEASE EXACERBATION
P. Mallia, S. Message, V. Laza-stanca, M. Contoli, T. Kebadze, S. Johnston. Department of Respiratory Medicine, Imperial College, London, UK
Introduction: Rhinoviruses (RV) are associated with 40–50% of acute exacerbations of chronic obstructive pulmonary disease (COPD) but little is known about mechanisms of RV induced inflammation at exacerbations. Virus infection is associated with neutrophilic inflammation and current treatments such as corticosteroids are ineffective in treating neutrophil driven inflammation. In order to determine the mechanisms of virus induced neutrophilic airway inflammation we carried out RV infection in a group of volunteers with moderate COPD and a group of control smokers without airflow obstruction.
Subjects and Methods: Four subjects with COPD (mean FEV1 70% predicted) and 10 controls (mean FEV1 106% predicted) were infected with rhinovirus. Subjects kept diary cards of upper and lower respiratory tract symptoms (cough, wheeze, breathlessness, sputum volume, and quality). They were inoculated with of RV16 on day 0 and blood sampling and induced sputum carried out on days 5, 9, 12, and 15 then weekly. Adhesion molecule expression on neutrophils was determined by flow cytometry.
Results: All subjects developed a cold according to the Jackson criteria and symptoms of an exacerbation. There was a significant increase in cold scores on days 3–6 and chest scores on days 5–11 compared to baseline. There was a fall in FEV1 and PEF maximal on day 9 although this did not reach statistical significance. There were non-significant increases in the total sputum cell count, percentage neutrophils in sputum and peripheral neutrophil count on day 9 compared to baseline. RV infection was associated with a significant reduced expression of CD11a in blood (p = 0.03) and an increase in CD11a expression on sputum neutrophils (p = 0.026) on day 9. There were similar changes in Mac-1 expression but these were not significant. There was significantly increased expression of CD54 (p<0.05) on sputum neutrophils, and reduced expression of CD62L (p = 0.03) in blood on day 9 compared to baseline.
Conclusions: RV infection in smokers and COPD subjects induces colds and typical symptoms of exacerbation. This is accompanied by a peripheral neutrophilia and increase in sputum neutrophils. The adhesion molecules CD11a, CD54, and CD62L may be involved in neutrophil recruitment to the lung and may represent possible therapeutic targets.
P103 SERUM INTERLEUKIN 6 AT CHRONIC OBSTRUCTIVE PULMONARY DISEASE EXACERBATION AND SUBSEQUENT HOSPITALISATION
W. R. Perera, J. R. Hurst, T. M. A. Wilkinson, G. C. Donaldson, J. A. Wedzicha. Academic Unit of Respiratory Medicine, Royal Free & University College Medical School, London, UK
Introduction: Chronic obstructive pulmonary disease (COPD) exacerbations are a major cause of healthcare use and hospital admissions. Known risk factors for hospitalisation include three or more hospital admissions in the previous year, lower FEV1, and under prescription of oxygen. Exacerbations are associated with increased airway and systemic inflammation. However, no airway or systemic inflammatory marker has been related to subsequent hospitalisation.
Aim: To compare the differences in airway and serum inflammatory markers in patients with COPD exacerbations requiring or not requiring hospital admission.
Methods: Patients were recruited from the East London COPD Cohort in the stable state and followed up prospectively with daily diary cards. They contacted the study team via a dedicated phone line when they noticed any change in their respiratory symptoms. Patients were seen by a physician within 48 hours, the diagnosis of exacerbation was confirmed, sputum and serum samples were taken, and patients were treated according to the clinical severity of the episode. The levels of interleukin (IL)-6 and IL-8 were measured in the sputum and IL-6 was measured in the serum, both in the stable state and at exacerbation.
Results: 73 exacerbations were sampled in 73 patients with a mean age of 69 (SD 8) years, baseline FEV1 1.08 (SD 0.47) l, 44.9 (SD 18.1)% predicted and FEV1/FVC ratio of 47 (SD 14)%. They had a mean smoking history of 48.1 (SD 34.9) pack years and 29.4% were active smokers. Mean baseline pH was 7.41 (SD 0.03), PaCO2 5.74 (SD 0.95) kPa, and PaO2 was 8.86 (SD 1.08) kPa. Nine out of 73 patients were admitted to hospital during their exacerbation, one of them required ITU admission and mechanical ventilation. Patients admitted to hospital had significantly higher levels of serum IL-6 at onset of the exacerbation than those treated in the community, median (SD) IL-6 at onset was 14.4 (11.29 to 108.20) pg/ml in hospitalised patients versus 12.06 (3.6 to 18.05) pg/ml in patients treated in the community, p = 0.012. There were no statistically significant differences in the baseline lung function, baseline sputum IL-6, sputum IL-8, and serum IL-6 between the nine patients admitted to hospital and the 64 patients followed up in the community. The sputum IL-6 and IL-8 at exacerbation were not significantly different in the two groups. The number of patients living alone was similar between the two groups as well.
Conclusion: Patients subsequently admitted to hospital had a higher serum IL-6 at exacerbation than those successfully treated in the community. Baseline airway and systemic inflammatory markers and lung function were similar in the two groups.
P104 VIRAL INFECTION AND CYTOKINE RESPONSES IN EXACERBATIONS OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE
T. E. McManus1,2, A. M. Marley1, F. De Courcey3, N. Baxter1, S. N. Christie2, H. J. O’Neill2, J. S. Elborn3,4, P. V. Coyle2, J. C. Kidney1. 1Department of Respiratory Medicine, Mater Hospital, N Ireland; 2Regional Virus Laboratory, Royal Victoria Hospital, N Ireland; 3Respiratory Research Group, Institute of Clinical Science, N Ireland; 4Department of Respiratory Medicine, Belfast City Hospital, N Ireland
Introduction: In chronic obstructive pulmonary disease (COPD) exacerbations can be triggered by viral and bacterial infections. Real-time PCR allows faster and more accurate detection of respiratory viral infections and assessment of cytokine mRNA responses. We studied patients with COPD when stable and during exacerbations to determine the role of viral infection and airway inflammation.
Methods: Patients were recruited with 24 hours of hospital admission for a COPD exacerbation (AECOPD). Patients with stable COPD who had no change in treatment or symptoms over the previous eight weeks were also recruited (SCOPD). Sputum, nasal and throat swab specimens were obtained and screened for respiratory viruses using nested PCR. Real-time PCR was used to measure mRNA cytokine responses. Ribosomal RNA (18s rRNA) was employed as a housekeeping gene. Supernatant from sputum specimens was analysed for corresponding protein concentrations of cytokines using the BioPlex system. All mRNA levels are adjusted for 18s rRNA and expressed as copies/ml of sputum (c/ml).
Results: One hundred and thirty six patients were recruited during an acute exacerbation and 68 when stable. Mean age of each group was 70 (SD 9) years and 66 (SD 9) years respectively. FEV1 (% predicted) was as follows; AECOPD 0.84 (SD 0.5) (39%), SCOPD 1.00 (SD 0.5) (48%). Smoking history AECOPD 48 (SD 39) and SCOPD 42 (SD 26) pack years. A respiratory virus was detected in 50 (37%) AECOPD and in 8 (12%) SCOPD patients (p<0.001). TNFα mRNA levels were higher in AECOPD (1392 c/ml) than SCOPD (139 c/ml) patients. IL-6 and IL-8 mRNA was also significantly increased during AECOPD (219 c/ml, 38429 c/ml,) in comparison to stable patients (27 c/ml, 4071 c/ml p<0.005). GRO-a and GM-CSF mRNA levels were increased during exacerbations (p<0.005). Expression of growth factors TGFβ1 and TGFβ2 were also increased in AECOPD. Corresponding protein concentrations of IL-6, TNFα, interferon-γ, and IL-4 were raised during exacerbations (p<0.005). TGFβ1 and TNFα mRNA levels were higher during those exacerbations in which a virus was not isolated.
Conclusion: Patients with AECOPD have an increased airway inflammatory response when compared to the stable patients. The expression of some cytokine targets are modulated by respiratory viral infection.
P105 IN VITRO MODEL OF RHINOVIRUS INFECTION OF PRIMARY BRONCHIAL EPITHELIAL CELLS FROM SMOKERS
S. Foo1, P. Wark1, F. Bucchieri1,2, R. Djukanovic1, S. T. Holgate1, D. E. Davies1. 1The Brooke Laboratories, University of Southampton, SO16 6YD, UK; 2Department of Experimental Medicine, Human Anatomy Division, University of Palermo, Palermo 90127, Italy
Introduction: Cigarette smoking increases the risk of contracting bacterial and viral infections and has also been reported to affect the immune system.1 Rhinovirus infection is one of the most common respiratory infections and has the ability to infect the lower respiratory tract.2 A pilot study was conducted to establish an in vitro model of rhinovirus infection and its interaction with the innate immune system of respiratory epithelium from smokers.
Methods: Seven non-atopic current smokers of mean age 56, mean smoking history of 52 pack/years were recruited. Primary bronchial epithelium cells (PBECs) were harvested with brushings at the 2nd to 3rd generation bronchi via flexible fibreoptic bronchoscopies. The PBECs were cultured and then infected with rhinovirus serotype 16 (RV16) for 48 hours. Cytoxicity due to cell necrosis was characterised by lactate dehydrogenase (LDH) release, inflammatory response with interleukin 8 (IL8), and viral titre with 50% tissue culture infectious dose (TCID 50) were studied at varying time points and viral multiplicity of infection (MOI) doses.
Results: An MOI dose as low as 0.01 appeared to cause significant cell necrosis occurring within 48 hours of treatment. Significant IL 8 release was observed in a time and dose dependent manner but reaches a plateau 48 hours post-treatment at higher MOI doses (⩾2). Viral replication plateaus at 24 hours post-treatment with MOIs from 0.5 to 6.
Conclusion: An in vitro model can be established to study the innate immune response of epithelium from the lower respiratory tract of smokers to rhinovirus infection.
This work was by funded by Synairgen Research Ltd.
1
2
P106 HUMAN RHINOVIRUS UPREGULATES ICAM-1 EXPRESSION ON CULTURED NASAL EPITHELIAL CELLS FROM PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
J. R. Hurst, R. Kuchai, L. J. Hammond, R. J. Sapsford, J. A. Wedzicha. Academic Unit of Respiratory Medicine, Royal Free & University College Medical School, Royal Free Hospital, London NW3 2PF, UK
Introduction: Factors underlying exacerbation frequency in chronic obstructive pulmonary disease (COPD) are poorly understood. Frequent exacerbators experience more colds than infrequent exacerbators (Hurst. ERJ 2005), and colds are most commonly due to rhinovirus (RV). COPD is associated with nasal inflammation, which may include upregulation of ICAM-1, the major RV receptor. Frequent exacerbators have greater airway inflammation than infrequent exacerbators (Bhowmik. Thorax 2000). While RV upregulates ICAM-1 in respiratory epithelium, this has not been demonstrated in COPD, and may be one mechanism underlying exacerbation frequency. In this preliminary analysis we aimed to investigate whether RV is capable of upregulating ICAM-1 in primary human nasal epithelial cells (HNECs) from subjects with COPD.
Method: Nasal biopsy was performed in four male subjects with COPD (mean age 67 (SD 6.8) years, FEV1 1.7 (SD 0.40) l or 60 (SD 7.5)% predicted). Confluent cultures of epithelial cells were grown by the explant technique developed in this laboratory (Devalia. Respir Med 1990). Cell surface ICAM-1 expression was assessed using flow cytometry before, and 24 hours after, exposure to RV-16 at a MOI of 0.5 for 90 minutes, or control medium. Results are expressed as the median fluorescence intensity (after subtraction of background staining) and percentage of cells staining positive for ICAM-1.
Results: The results of the median intensity and percentage positive (% +ve) assays are reported in the table. Data are expressed as mean (standard deviation).
Conclusion: RV-16 upregulates its own receptor, ICAM-1, in primary HNECs. Both the median expression per cell and number of cells expressing ICAM were significantly increased compared to control exposure. RV induced ICAM-1 upregulation is a potential mechanism underlying susceptibility to exacerbation in COPD and worthy of further study.
Abstract P106 ICAM-1 expression following RV-16 exposure in HNECs
P107 RELATION BETWEEN RESPIRATORY SYNCYTIAL VIRUS DETECTION AND AIRWAY INFLAMMATION IN PATIENTS WITH STABLE CHRONIC OBSTRUCTIVE PULMONARY DISEASE
T. M. A. Wilkinson, W. Perera, J. R. Hurst, G. C. Donaldson, J. A. Wedzicha. Academic Unit of Respiratory Medicine, Royal Free Hospital and University College Medical School London, UK
Respiratory syncytial virus (RSV) is an established pathogen in acute respiratory illnesses in young children and in adults. It has also been detected in the lower airway of patients with chronic obstructive pulmonary disease (COPD) in the stable state. We have previously reported an association between RSV persistence and accelerated decline in FEV1. We hypothesised that this association was as a result of greater airway inflammation induced by carriage of RSV.
We studied 74 patients with COPD, median (IQR) age 67.4 (62.2 to 71.4) years, FEV1 0.98 (0.77 to 1.37) l, FEV1 % predicted 39.2 (29.6 to 57.8). 241 sputum samples were collected quarterly in the stable state over two years. RSV was detected by PCR and inflammatory cytokines quantified by ELISA.
RSV RNA was detected in 32.8% of stable state sputum samples by PCR. Patients with RSV detected in >50% of samples (“high RSV”, n = 18) showed greater airway inflammation than those with infrequent detection of RSV (⩽50% samples RSV PCR positive, “low RSV”, n = 56), as measured by sputum IL6: high RSV; 253 (244 to 261) pg/ml, low RSV; 182 (178 to 185) pg/ml, difference 71 (63 to 79) pg/ml p<0.001, sputum IL8: high RSV; 3229 (3197 to 3262) pg/ml, low RSV; 2571 (2558 to 2585) pg/ml, difference 658 (629 to 686) pg/ml p<0.001 and sputum Myeloperoxidase: high RSV; 23.0 (16.7 to 29.3) ng/ml, low RSV; 10.3 (7.5 to 13.2) ng/ml, difference 12.7 (7.5 to 18.2) ng/ml p<0.001. Similarly frequent RSV detection was associated with higher airway bacterial loads (108.12(0.48) log cfu/ml) compared to infrequent RSV detection (107.76 (0.58) log cfu/ml, p = 0.024).
RSV is not only detectible in the lower airway of patients with stable COPD but is associated with heightened levels of airway inflammation. Whether this is a direct effect of the virus or via modulation of inflammatory responses to other stimuli such as bacterial infection remains uncertain. Further studies into the mechanisms and consequences of RSV persistence in the lung may provide novel opportunities to modulate disease progression in patients with COPD.
P108 STUDIES OF INTERLEUKIN-1β AND ITS RECEPTOR IL-1 RECEPTOR 2 AND ANTAGONIST IL-1 RECEPTOR ANTAGONIST IN STABLE CHRONIC OBSTRUCTIVE PULMONARY DISEASE
E. Sapey1, D. Bayley1, D. Griffiths1, P. Newbold2, R. A. Stockley1. 1University of Birmingham, Birmingham, UK; 2Astrazenaca, UK
It is widely accepted that inflammation is fundamental to the pathogenesis and progression of chronic obstructive pulmonary disease (COPD). However, there is controversy concerning whether pulmonary inflammation causes increased systemic inflammation, which could account for the enhanced comorbidity seen with this condition. IL-1β has been identified as a prominent proinflammatory mediator in COPD with significantly higher sputum concentrations compared to healthy controls and this increases further during exacerbations. However, the relation between sputum and plasma IL-1β and the IL-1β antagonists IL-1RII and IL-1RA has not been clarified in COPD.
18 patients with GOLD stage 3 disease, a significant smoking history (mean pack year 41.8, range 19–89) and with chronic sputum production were studied. Sputum and plasma were collected on 11 occasions over a four week period. Sputum was processed to obtain cell differential counts and supernatant for analysis of IL-1b and plasma was obtained to measure IL-1β, IL-1RII, and IL-1RA.
Sputum IL-1b correlated positively with sputum neutrophil counts (Spearman’s correlation coefficient (SCC) 0.94, p<0.001). Sputum IL-1β was significantly higher than plasma IL-1β (p<0.001) but there was no correlation between this mediator in the two compartments. Serum IL-1RII correlated positively with IL-1RA (SCC 0.5, p<0.001). Plasma IL-1RII and IL-1RA correlated positively with plasma neutrophil counts (SCC 0.3, 0.2 p = 0.003, 0.005). However both antagonists correlated negatively with sputum neutrophil count (IL-1RII SCC −0.3, p = 0.002: IL-1RA SCC −0.5, p<0.001) and sputum IL-1β (IL-1RII SCC −0.3, p = 0.01; IL-1RA SCC −0.4, p<0.001).
IL-1 has two naturally occurring antagonists, IL-1RII, which binds preferentially to IL-1β, blocking its physiological activity; and IL-1RA, which binds to IL-1 receptor one preventing free IL-1 from binding to the receptor. It has been suggested that IL-1 causes increased secretion of the two antagonists as part of a negative feedback loop. If pulmonary inflammation led to a simple overspill into the systemic compartment one would expect a positive correlation between these proteins. These results suggest that this relation is more complex. It may be that there is an “overspill” of free IL-1β from the lung into plasma, but this free IL-1b is bound by the receptor antagonists thereby abrogating specific antibody binding to the soluble receptors and antagonist. Further work is required to clarify this observation.
P109 ESTABLISHING PRIMARY CULTURES OF NASAL EPITHELIAL CELLS FROM NASAL BRUSHINGS
C. M. McDougall, G. M. Walsh. School of Medicine, University of Aberdeen, UK
The airway epithelium plays a pivotal role in controlling many airway functions. Cell cultures permit the study of the role of the epithelium in the aetiology of airway diseases, mechanisms of airway inflammation and the effects of drugs. The nose is a particularly attractive source of airway epithelial cells because of the greater ease of access compared to the tracheobronchial epithelium and the potential for repeated isolation from the same individual. We have developed a simple method for establishing primary cultures of nasal epithelial cells using the minimally invasive technique of nasal brushing.
Epithelial cells were collected from the medial aspect of the inferior turbinate using a cytology brush and were dislodged by agitation in bronchial epithelial growth medium (BEGM; Cambrex BioScience, Wokingham, UK). The cell suspension was seeded in a 4 cm culture plate, precoated with rat tail collagen at 5 μg/cm2, with a final volume of 3 ml. Cells were maintained at 37°C in an atmosphere of 95% air/5%CO2. The cells were subcultured by trypsinisation at 70–90% confluence and after first passage attached and grew on uncoated plasticware.
We have obtained nasal brushings from 29 subjects (19 male, median age 32 years, range 24–59 years). The procedure was well tolerated by all subjects, with no complications noted. Successful cultures, with the culture reaching 70–90% confluence and being successfully subcultured, were established in 20 samples (69%). Six cultures succumbed to infection (5 bacterial, 1 fungal). In the other three, no obvious reason for the failure could be identified. In all successful cultures, there was evidence of cell attachment within 24 hours of seeding. The median time to 70–90% confluence was nine days (range 5–22 days). The mean cell number recovered at passage one was 2.05×105 (range 0.08–8.85×105) and mean cell viability, assessed by trypan blue exclusion, was 96.3% (SD 1.74%). These monolayer cultures demonstrated the typical “cobblestone” morphology of epithelial cells. Their epithelial nature was confirmed by positive immunostaining for the epithelium-specific protein cytokeratin 19 (n = 3). The presence of contaminating fibroblasts or endothelial cells was excluded by negative immunostaining with antifibroblast and anti-von Willebrand factor antibodies. The cultured cells have been used for experiments to determine the pattern of cytokine release and to assess drug toxicity, demonstrating the feasibility of performing functional studies on these cultures. Cells grew rapidly for several weeks but underwent growth arrest and detachment after 5–7 weeks (corresponding to passage 3–5 depending on rate of growth) (n = 4). Cells from five cultures were cryopreserved at −80°C and successfully recovered.
We conclude that an in vitro model of respiratory epithelium, suitable for functional studies, can be established from nasal brushings.
P110 MECHANISMS UNDERLYING ASSOCIATION BETWEEN HYPERGLYCAEMIA AND AIRWAY INFECTION IN PATIENTS WITH ACUTE EXACERBATIONS OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE
D. M. Wood, C. H. Janaway, S. Ong, T. Harries, A. L. Brennan, D. L. Baines, B. J. Philips, E. H. Baker. Glucose and Pulmonary Infection Group, St George’s, University of London, UK
Background: People with acute exacerbations of chronic obstructive pulmonary disease (AECOPD) and blood glucose (BG) >8 mM are more likely to have at least one or multiple respiratory pathogens isolated from sputum than people with BG ⩽8 mM (
). Gram negative bacteria were isolated more commonly in sputum from people with AECOPD and diabetes mellitus (DM) than those without, and blood glucose >11 mM predicted infectious complications of non-invasive ventilation for AECOPD. We have previously shown in healthy volunteers that glucose is undetectable in nasal secretions until blood glucose exceeds 8 mM (
). Furthermore elevated airway glucose concentrations predicted airway infection in people intubated on intensive care (
). We therefore determined the effect of hyperglycaemia on airway glucose concentrations in people with AECOPD.
Methods: 10 people with AECOPD without DM were recruited within 24 hours of admission. Participants underwent 48 hour continuous blood glucose monitoring (Minimed). Paired blood (BG), nasal (NG), and sputum (SG) glucose concentrations were measured hourly during waking hours. The study was approved by the local research ethics committee and participants gave written informed consent.
Results: Glucose was detected in 74/104 nasal and 40/87 sputum samples. Glucose was more often detected in nasal and sputum samples when BG>8 mM (NG 82.5%; SG 57.1%) than when BG⩽8 mM (no NG 57.4%, p = 0.005; no SG 35.6%, p = 0.035). NG and SG concentrations were higher when BG>8 mM (mean NG 1.5 (SD 1.1) mM; SG 0.5 (0.0–1.5 mM), median (interquartile range)) than when BG⩽8 mM (NG 0.6 (SD 0.7) mM, p<0.0001; SG 0.0 (0.0–1.0) mM, p = 0.041). Participants had BG>8 mM on 48 hour blood glucose monitoring for 36.3 (SD 23.8) % of the day.
Conclusions: Glucose is present more often and at higher concentrations in airway secretions when BG>8 mM than when BG⩽8 mM. Glucose in airway secretions could increase infection by promoting bacterial growth or impairing host immunity and could contribute to the increased respiratory infection seen in people with AECOPD and hyperglycaemia.
P111 REPEATABILITY OF INDUCED SPUTUM CHARCTERISTICS, SYMPTOMS, AND HEALTH STATUS IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE
S. K. Saha, S. McKenna, D. Parker, W. Monteiro, P. Bradding, I. D. Pavord, C. E. Brightling. Institute for Lung Health, Glenfield Hospital, Groby Road, Leicester LE3 9QP, UK
Background: There is a need for repeatable and responsive outcome measures in chronic obstructive pulmonary disease (COPD). Possible measures include markers of lower airway inflammation in induced sputum, assessment of symptoms, and health status. We have previously examined the repeatability of these measures over two weeks, but their repeatability over longer periods is uncertain.
Methods: In 60 subjects with moderate and severe COPD who participated in a randomised controlled crossover study of mometasone or placebo for six weeks we assessed the within-subject repeatability of sputum indices, health status using the chronic respiratory disease questionnaire (CRQ), and symptom visual analogue scores (VAS) for dyspnoea, cough, wheeze, and sputum production (0–100 mm; total score 0–400 mm) before and after placebo treatment.
Results: 41 subjects produced adequate paired induced sputum samples. The reproducibility of measurements was calculated by the intraclass correlation coefficient (ICC) and standard deviation of the difference (SD) between the two visits. The ICC was relatively high for the eosinophil and neutrophil differential cell counts, for the total and individual symptom VAS and for the total and each CRQ domain (0.4–0.88). The repeatability of the total sputum cell count (TCC) was poor questioning the repeatability of absolute cell counts over a six week period.
Conclusion: In conclusion, sputum indices of granulocytic inflammation, symptom VAS and the CRQ are reproducible outcome measures in COPD over a six week period.
Supported by: Schering-Plough.
Abstract P111 Repeatability of COPD outcome measures over a six week period
P112 DETERMINATION OF THE PREVALENCE OF ELEVATED SERUM TROPONIN T LEVELS IN SEVERE EXACERBATIONS OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE REQUIRING NON-INVASIVE VENTILATION AND ITS USE AS A PROGNOSTIC MARKER
R. P. Narayanan, M. A. I. Khan, P. M. Turkington. Department of Respiratory Medicine, Hope Hospital, Salford M6 8HD, UK
Background: Cardiac troponin T (cTnT) elevation can occur in myocardial necrosis due to any cause, and raised levels have been found in patients who have not had a classic acute coronary syndrome. It would not be surprising if cTnT was raised in acute severe exacerbations of COPD due to consequent right and/or left ventricular dysfunction (
). Known predictors of outcome in chronic obstructive pulmonary disease (COPD) include hypercapnoea and respiratory acidosis (
). However no relation between any rise in cTnT and severe exacerbation of COPD or inpatient mortality has yet been established.
Methods: 20 consecutive patients admitted in the Medical High Dependency Unit with an acidotic exacerbation of COPD requiring non-invasive ventilation (NIV), who gave informed consent were included in the study. Patients with renal failure, evidence of acute coronary syndrome, or features suggestive of pulmonary embolism were excluded from the study. A blood sample was sent for cTnT estimation between 12 and 24 hours of COPD exacerbation, and patients followed up to discharge from hospital or death.
Results: The mean age of the patients was 66 (SD 10.25) years. 45% were male and 22.2% had previous history of hypercapnoeic respiratory failure. All patients remained acidotic and hypercapnic after initial treatment and controlled oxygen therapy and therefore all received non-invasive ventilatory support. Eleven of the 20 patients (55.6%) had cTnT levels > = 0.01 between 12 and 24 hours of exacerbation. Mean level of cTnT was 0.13 (SD 0.19) with a range of 0.01 to 0.70. Mean length of hospital stay that admission in those with raised cTnT was 17.78 (SD 10.55) with a mean period of NIV ventilation of 3.12 (SD 1.9) days. Corresponding figures for the normal cTnT level group were a mean length of inpatient stay of 14.62 (SD 17.2) with an average of three days of NIV. There were two mortalities, both from the raised cTnT group.
Conclusions: Cardiac troponin T appears to be increased in a signficant percentage of patients with acidotic exacerbations of COPD. However further data are required to establish whether a rise in cTnT during an acidotic exacerbation of COPD has any bearing on mortality or morbitity.
P113 HYPERGLYCAEMIA IS ASSOCIATED WITH POOR OUTCOMES IN PEOPLE ADMITTED TO HOSPITAL WITH ACUTE EXACERBATIONS OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE
E. H. Baker, C. H. Janaway, B. J. Philips, A. L. Brennan, D. L. Baines, D. M. Wood, P. W. Jones. Glucose and Pulmonary Infection Group, St George’s, University of London, UK
Background: Hyperglycaemia is detrimental for many patients admitted with acute illness, but the effect of blood glucose on outcomes from acute exacerbations of chronic obstructive pulmonary disease (AECOPD) has not been elucidated. Recent UK guidelines do not comment on measurement or control of blood glucose in AECOPD. We therefore determined the relation between blood glucose concentrations, length of stay, and mortality in people admitted with AECOPD.
Methods: Patients admitted with “acute exacerbations of COPD with lower respiratory tract infection” in 2001 and 2002 were identified retrospectively and data retrieved from electronic records. Patients were divided by blood glucose quartile (Group 1, <6 mmol/l (n = 69); Group 2, 6.0–6.9 mmol/l (n = 69); Group 3, 7.0–8.9 mmol/l (n = 75); and Group 4, >9.0 mmol/l (n = 71).
Results: Relative risk of death or long inpatient stay was significantly increased in Group 3 (relative risk 1.46 (95% CI 1.05 to 2.02) (p = 0.02) and Group 4 (relative risk 1.97 (95% CI 1.33 to 2.92) (p<0.0001), compared to Group 1. For each 1 mmol/l increase in blood glucose the risk of adverse outcomes increased by 14% (95% CI 4 to 25%) (p = 0.005). In those with spirometry, blood glucose quartile (p = 0.014) predicted adverse outcomes independently of age (p = 0.025), sex (p = 0.014), and COPD severity (p = 0.332). Isolation of multiple pathogens (p = 0.034), Staphylococcus aureus (p = 0.005), and yeasts (p = 0.052) from sputum also increased with increasing blood glucose concentrations.
Conclusion: Hyperglycaemia is associated with poor outcomes in patients with AECOPD. Mechanisms are unclear, although increased respiratory infection may play a role. Blood glucose control to a mean of 130.7 mg/dl (about 7.2 mmol/l) in a heterogeneous population of critically ill adult patients, reduced hospital mortality by 29.3% and ICU length of stay by 10.8% (
). If tight control of blood glucose has similar benefits for patients admitted with AECOPD to those seen in patients on intensive care, it could significantly reduce inpatient stay and mortality with benefits both to the individual and to the NHS.
P114 CHRONIC OBSTRUCTIVE PULMONARY DISEASE AND A FASTER DECLINE IN FEV1 ARE STRONGLY ASSOCIATED WITH HIGH SENSITIVITY C-REACTIVE PROTEIN: A MULTICENTRE EPIDEMIOLOGICAL STUDY
I. S. Olafsdottir1, T. Gislason1, B. Thjodleifsson2, I. Olafsson3, D. Gislason1, R. Jõgi4, C. Janson5. 1Department of Allergy, Respiratory Medicine and Sleep, Landspitali University Hospital, 108 Reykjavik, Iceland; 2Department of Gastroenterology, Landspitali University Hospital, 101 Reykjavik, Iceland; 3Department of Clinical Biochemistry, Landspitali University Hospital, 108 Reykjavík, Iceland; 4Lung Clinic, Tartu University Clinics, Estonia; 5Department of Medical Sciences: Respiratory Medince & Allergology, Uppsala University, Sweden
Background: Chronic obstructive pulmonary disease (COPD) is characterised by an accelerated decline in lung function and progressive airway inflammation. Only a few of the key pathogenic players are presently known. High sensitivity C-reactive protein (HsCRP) is an inflammatory marker known to be related to smoking, obesity, and cardiovascular disease.
Objective: To study whether HsCRP is related to COPD and lung function.
Methods: This study is based on 1237 randomly selected subjects from three centres in European Community Respiratory Health Survey: Reykjavik, Uppsala, and Tartu. The HsCRP values ranged from <0.01–70.0 mg/l and were divided into four equally large groups (⩽0.45, 0.46–0.96, 0.97–2.21, and >2.21 mg/l).
Results: Ninety two subjects fulfilled the spirometry criteria for COPD (FEV1/FVC <70%). COPD was significantly more often in the 3rd or 4th HsCRP quartile with an OR (95% CI) 2.17 (1.05 to 4.48) and 2.73 (1.30 to 5.72) after a statistical adjustment for age, sex, body weight, and smoking. The rate of decline in FEV1 between ECRSH I and II was 44 ml/year in males and 31 ml/year in females. The decline in FEV1 was significantly larger in men with high HsCRP levels (16 (5 to 27) ml) while no significant association between FEV1 decline and HsCRP levels was found in women.
Conclusions: Higher HsCRP values in an epidemiological cohort are significantly associated with COPD and lower lung function in men and women. In men higher HsCRP values was related to a more a rapid decline in FEV1 during the study period.
Pulmonary vascular disease: clinical
P115 HAEMOLYTIC DISORDERS COMPLICATED BY PULMONARY HYPERTENSION
C. A. Elliot1, J. Wright2, K. Ryan3, M. Woodhead4, I. J. Armstrong1, T. S. Saba1, D. G. Kiely1. 1Sheffield Pulmonary Vascular Disease Unit; 2Haematology Department, Royal Hallamshire Hospital, Sheffield, UK; 3Haematology; 4Respiratory Medicine, Manchester Royal Infirmary, Manchester, UK
Pulmonary arterial hypertension (PAH) is increasingly recognised as a complication of sickle cell disease, with a significant impact on survival. Decreased levels of nitric oxide have been suggested as a mechanism for this, due to its uptake by free haemoglobin released as a consequence of haemolysis.
Over the last three years, at our centre, we have diagnosed 10 patients with haemolytic disease as having pulmonary hypertension according to standard criteria.
Haematology diagnoses include sickle cell disease (n = 5), thalassaemia intermedia (n = 1), pyruvate kinase deficiency (n = 2), hereditary spherocytosis (n = 2). The mean age for the group was 43 years and only the patients with sickle cell disease had not undergone surgical splenectomy.
The group have significant pulmonary hypertension demonstrated at cardiac catheterisation with mean right atrial pressure 11 (SD 7) mm Hg, mean pulmonary artery pressure 41 (SD 14) mm Hg, and pulmonary vascular resistance 308 (SD 194) dynes with well maintained cardiac index of 4.4 (SD 1.1) l/min/m2. Interestingly none of these patients were shown to have a positive vasodilator response to inhaled nitric oxide.
Patients with haemolysis but no splenectomy were found to have PAH. However, all those with previous splenectomy had evidence of CTEPH (usually distal disease) as well as PAH.
We conclude that haemolysis (not only in the setting of sickle cell disease) increases the risk of developing PAH. In addition splenectomy appears to be a risk factor for the development of distal CTEPH. As such, in patients with haemolytic disorders we would recommend a low threshold for the investigation of breathlessness and a high index of suspicion for the presence of pulmonary vascular disease.
P116 A SURVEY OF THE NEEDS AND IMPACT OF PULMONARY HYPERTENSION IN 2004 AND 2005 OF PATIENTS IN THE UK
I. Armstrong, T. Siddons, S. Waller, K. Yeowart. Pulmonary Hypertension Association UK
Introduction: The aim of this study was to obtain a greater understanding of the patient and their families perception of the impact of PH on their daily lives. These findings could then help inform, focus, and identify ways of significantly improving the care and support of PH patients and their families.
Method: All (patient) members of the Pulmonary Hypertension Association UK (PHA UK) were questioned in 2004/05, through a postal questionnaire. Over 200 responses were returned. These members were questioned about four main areas of their experiences: (1) the disease and its implications for them, (2) the reason for seeking medical help in the first instance and their subsequent experience of the referral pathway, (3) their experiences of treatment and what are/were their own treatment goals, and (4) their experience in acquiring sufficient information about the disease to satisfy their needs.
Results: The initial phase and analysis (which is still ongoing) identified major issues relating to employment, personal and family relationship, childcare, and future planning. There was also concern identified concerning a lack of general PH awareness in four key areas: (1) primary care centres, (2) secondary and non-specialised care settings, (3) non-immediate family members, and (4) the work and school environment. The next phase of this ongoing study will aim to quantify these apparent deficiencies in support and awareness. This would then help influence future strategies for the PHA UK.
This Study was supported, in part, by a grant from the Department of Health for England and Wales.
P117 ABNORMAL POST-EXERCISE SYSTOLIC BLOOD PRESSURE RESPONSE TO EXERCISE IS COMMON IN PATIENTS WITH SUSPECTED PULMONARY HYPERTENSION
C. G. Billings1, C. A. Elliot2, I. J. Armstrong2, T. S. Saba2, D. G. Kiely2. 1Respiratory Function Unit; 2Sheffield Pulmonary Vascular Disease Unit, Royal Hallamshire Hospital, Sheffield, UK
Background: Incremental Shuttle Walking Test (ISWT) distance correlates with cardiac output and cardiac index and predicts prognosis in patients with pulmonary hypertension (PH) treated with targeted pulmonary vascular therapy. Post-exercise systolic blood pressure (SBP) response (3 minute SBP/peak exercise SBP) has been shown to be a useful parameter in the evaluation of patents with coronary artery disease and chronic heart failure with a ratio of >0.90 considered abnormal. This study explores the potential use of post-exercise systolic blood pressure response to exercise in the assessment of patients with suspected PH.
Methods: The systemic blood pressure of patients attending for ISWT with known or suspected PH was measured. Blood pressure was measured in triplicate whilst sitting at rest (Omron 705IT) prior to the ISWT (pre-exercise SBP). Immediately on terminating the ISWT the patient was seated and blood pressure taken in duplicate (peak SBP). Blood pressure was again measured at three minutes post-exercise (3 minute SBP). The ratio of the 3 minute SBP to the peak SBP was used as the response ratio and an upper limit of 0.90 was set as normal. Here we review the results of 444 consecutive studies comparing those with normal (Group 1) to those with an abnormal SBP response (Group 2).
Results: See table. No difference in pre-exercise or 3 minute SBP was found between the two groups, however a significant difference in the distance walked between the two groups was found 313 (SD 202) m versus 206 (SD 135) m, 95% CI 73 to141.
Abstract P117
Conclusions: In patients with suspected PH an abnormal exercise SBP response is associated with a significantly reduced exercise capacity. In addition to absolute ISWT distance this measurement may help to identify patients with a low walking distance due primarily to abnormalities in cardiovascular function.
P118 HISTOLOGY OF ARTERIOLAR WALL REMODELLING IN A LUNG VOLUME REDUCTION SURGERY PATIENT COHORT
G. Sirico1, K. Pinnion1, P. Vaughan1,2, D. A. Waller2, M. L. Foster1. 1Department of Pathology, AstraZeneca(R&D) Charnwood; 2Department of Thoracic Surgery, Glenfield Hospital, Leicester LE3 9QP, UK
Objective: Non-hypertensive changes in lung vessel morphology in severe chronic obstructive pulmonary disease (COPD) remains a problematic area. Research is complicated by a lack of studies in well characterised patient groups. In this study we report preliminary data on changes in arteriolar wall histology in a lung volume reduction surgery (LVRS) surgical cohort with strict inclusion criteria.
Methods: Samples from 16 patients undergoing LVRS were compared with samples from three patients undergoing surgery for malignancy. Patients were well characterised clinically and subject to standard inclusion criteria. Patients with pulmonary hypertension were excluded. In all, 52 vessels were studied in the LVRS group and 20 in the lobectomy group. Sections were assessed by H&E histology and then further stratified using Miller’s elastic stain and picrosirius red. Phenotype of vessel wall cells was further studied using CD31, desmin, and vimentin immunohistochemistry.
Results: Arteriolar walls from the LVRS group showed intimal hypertrophy with a medial hyperplasia in the majority of samples. Sporadic medial hypoplasia was also seen which was usually associated with severe inflammation. Severely affected vessels displayed marked sclerosis. Interestingly, the LVRS vessels were characterised by a re-orientation of collagen fibres (adopting a radial alignment), which expanded into the intima. Positive desmin and vimentin staining, and negative CD31 staining suggested a mesenchymal origin for this intimal lesion. Apoptosis of medial smooth muscle cells was observed in all grades of lesions. The intima, media, and overall severity scores for were all significantly higher for LVRS (p = 0.001, p = 0.01, and p<0.001 respectively) when compared with the lobectomy group.
Conclusion: The pulmonary arteriolar remodelling seen in patients undergoing LVRS differs significantly from lobectomy samples and appears to involve medial insult followed by proliferation. This is distinctive from the intimal proliferation seen in pulmonary hypertension.
P119 LONG TERM EXPERIENCE WITH BOSENTAN FOR THE TREATMENT OF IDIOPATHIC PULMONARY ARTERIAL HYPERTENSION UNDER ROUTINE CONDITIONS
D. G. Kiely1, J. Carlsen2, M. Humbert3, C. van Lierop4, M. M. Hoeper5. 1Royal Hallamshire Hospital, Sheffield, UK; 2Rigshospitalet, Kopenhagen, Denmark; 3Hopital Antoine Beclere, Clamart, France; 4Actelion Pharmaceuticals, Allschwil, Switzerland; 5Medical School, Hannover, Germany
In agreement with the European Agency for the Evaluation of Medicinal Products (EMEA), a non-interventional, prospective, web based post-marketing surveillance programme (called TRAX PMS) was run to monitor the safety of the dual endothelin ETA/ETB receptor antagonist bosentan (Tracleer) for the treatment of pulmonary arterial hypertension (PAH).
We report data collected from May 2002 until Nov 2004 on 1583 patients with idiopathic PAH (63.3% females; 72.0% in NYHA class III, and 12.1% in class IV). Concomitant medications at baseline included anticoagulants in 82.1% and prostanoids in 19.6%. Mean exposure to bosentan was 43.8 (SD 35.9) weeks; 576 patients (36.4%) were treated with bosentan for at least one year; 130 (8.2%) for at least two years. Potential safety signals included adverse events with focus on elevations of liver function tests (ALT/AST). Potential safety signals were recorded in 36.7% of patients. Elevated ALT and/or AST values after bosentan initiation were recorded in 8.4% (see fig).

Median time to onset of first ALT/AST elevation was 92 days. No cases of fatal or permanent liver injury were associated with bosentan. The safety of long term bosentan treatment was confirmed, as ALT/AST elevation rates and the frequency and severity of potential safety signals were consistent with the data in clinical trials.
P120 BOSENTAN FOR THE TREATMENT OF DISTAL CHRONIC THROMBOEMBOLIC PULMONARY HYPERTENSION: OUTCOMES AT ONE YEAR
R. Hughes, X. Jais, J. Suntharalingam, D. Hodgkins, G. Simmoneau, J. Pepke-Zaba. Pulmonary Vascular Diseases Unit, Papworth Hospital, Cambridge, UK; Service de Pneumologie, Hopital Antoine Beclere, Clamart, France
Background: Chronic thromboembolic pulmonary hypertension (CTEPH) is an uncommon but devastating complication of acute pulmonary embolic disease that results in progressive right ventricular dysfunction. Pulmonary endartectomy offers patients a potential surgical cure, but is only suitable for those with large vessel disease distribution. There is limited evidence supporting the use of medical therapy in those patients with inoperable “distal” disease. The purpose of this study was to evaluate the efficacy of open label Bosentan, a dual receptor endothelin antagonist, in a cohort of patients with distal CTEPH at two large international specialist centres.
Methods: 27 patients with radiologically confirmed distal CTEPH were started on Bosentan prior to July 2004. Comparison were made of right heart catheter study measurements, NYHA classification and 6 minute walking distance (6MWD) at 4 and 12 months after commencing Bosentan.
Results: During the 12 months of follow up, three patients discontinued Bosentan and were transitioned to an alternative therapy. One patient subsequently died after seven months despite commencing nebulised Iloprost. The remaining 24 patients completed at least 12 months Bosentan therapy. Results at baseline and twelve months are shown in the table.
Conclusions: Despite having poor prognostic characteristics at baseline, patients with inoperable distal CTEPH commenced on Bosentan therapy derive significant benefits both in terms of walking distance and haemodynamic parameters after four months of therapy. This benefit is sustained for at least 12 months after commencing Bosentan and represents a significant clinical response in this otherwise untreatable, rapidly progressive condition.
Abstract P120
P121 TREATMENT OF PULMONARY ARTERIAL HYPERTENSION IN ASSOCIATION WITH SYSTEMIC TO PULMONARY SHUNTS: A RETROSPECTIVE REVIEW
S. Anwar1, C. A. Elliot1, K. English2, G. Williams2, N. Brooks3, L. O’Toole1, I. J. Armstrong1, N. Hamilton1, T. S. Saba1, D. G. Kiely1. 1Sheffield Pulmonary Vascular Disease Unit, Royal Hallamshire Hospital, Sheffield; 2Leeds General Infirmary, Leeds, UK; 3Wythenshawe Hospital, Manchester, UK
Pulmonary arterial hypertension is frequently seen in association with systemic to pulmonary shunts due to a variety of different causes. Recently a number of therapies have been shown to improve exercise capacity in patients with PAH (pulmonary arterial hypertension) although there are few data in patients with systemic to pulmonary shunts.
We have retrospectively identified patients with congenital systemic to pulmonary shunts managed at our unit between 1997 and 2005.
We identified 67 patients with PAH associated with a systemic to pulmonary shunt. Of these 30 had atrial septal defects (ASD), 12 ventricular septal defects (VSD), three patent ductus arteriosus (PDA), 22 other (complex or combined).
Mean age at presentation to our unit was 41 (SD 15) years. Pulmonary hypertension was confirmed either at right heart catheterisation (RHC) or at echocardiography. Of these 67 patients, three have been referred for ASD closure. 52 patients were treated with targeted pulmonary vascular therapy; Bosentan = 37, Treprostinil = 6, iv iloprost = 6, nebulised iloprost = 3, as initial therapy). Of the patients receiving targeted therapies there was a significant improvement in the distance walked on the incremental shuttle walk test (ISWT) compared to baseline at 3–6 months after initiation of therapy from 165 (SD 109) m to 209 (SD 127) m, p = 0.003.
This retrospective audit has demonstrated an improvement in walking distance in patients receiving targeted therapy. Prospective multicentre studies are required to further evaluate the potential role of these therapies in patients with PAH in association with systemic to pulmonary shunts.
P122 DIAGNOSTIC UTILITY OF NYCOCARD D-DIMER ASSAY IN PULMONARY EMBOLISM
P. K. Sarkar1, S. Kaneri2, M. Farrugia2, G. E. Wilson1. 1Department of Medicine; 2Department of Radiology, Newham University Hospital NHS Trust, Glen Road, Plaistow, London E13 8SL, UK
Introduction: In recent years, CT pulmonary angiography (CTPA) has become the radiological investigation of choice. High costs and radiation exposure mandate an effective screening strategy to choose patients who need CTPA. D-dimer assay is now established as the best initial screening test. A recent study using a diagnostic algorithm including D-dimer showed that up to one third of CTPA studies could be avoided. Our hospital uses the NycoCard D-dimer assay, a rapid semiquantitative immunoassay, at a cut off value of 0.5 mg/l (95th percentile of samples from normal people). Medicines and Healthcare products Regulatory Agency (MHRA) report showed that at the manufacturer recommended cut off value of 0.3 mg/l, the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) are 90%, 44.8%, 29%, and 94.7% respectively. In patients with low clinical score, the sensitivity improves to 96.1% and NPV to 97.2%.The British Thoracic Society (BTS) guidelines recommend that each hospital should provide information on sensitivity and specificity of its D-dimer test and use D-dimer in conjunction with clinical probability assessment. We aimed to analyse the diagnostic utility of NycoCard D-dimer assay.
Methods: We analysed the data from case notes of 45 patients who were investigated for suspected PE with NycoCard D-dimer assay and CTPA. Patients were assigned to low, intermediate, or high clinical probability categories, following the BTS guidelines. We calculated the sensitivity, specificity, PPV, and NPV at a cut off value of 0.5 mg/l. We also analysed the data at manufacturer recommended cut off value of 0.3 mg/l and the performance of the assay in patients with intermediate or low clinical probability.
Results: At a cut off value of 0.5 mg/l, 25 patients had positive and 20 patients had negative D-dimer results. Seven of the 25 patients with positive D-dimer and one of the 20 patients with negative D-dimer were demonstrated to have PE on CTPA. The sensitivity, specificity, PPV, and NPV of the assay were 87.5%, 51.3%, 28%, and 95% respectively. Further analysis showed that at the cut off level of 0.3 mg/l, all patients with PE on CTPA had positive D-dimer and none of the patients with negative D-dimer showed evidence of PE. All patients with low/intermediate clinical probability and positive CTPA scan for PE had D-dimer >0.5 mg/l whereas none of the patients, who had a low/intermediate clinical probability and a D-dimer level ⩽0.5 mg/l, had PE on CTPA.
Conclusion: We conclude that using the NycoCard D-dimer assay and clinical probability assessment, it is possible to effectively select the patients who need further imaging studies.
P123 COMPUTED TOMOGRAPHY PULMONARY ANGIOGRAM REQUESTS FOR THE INVESTIGATION OF ACUTE PULMONARY EMBOLI. HOW APPROPRIATE ARE THEY?
A. L. Goodman1, G. V. Robinson1, C. W. H. Davies1, E. Elson2. 1Department of Respiratory Medicine; 2Department of Radiology, Royal Berkshire Hospital NHS Trust, Reading RG1 5AN, UK
Introduction: Patients with suspected pulmonary embolism are often admitted on the general medical take. Local guidelines for the investigation of possible PE are based on the BTS guidelines (
) and are available on the intranet. All patients should have a pre-test clinical probability score (PTP) and those with low or intermediate PTP should have a D-dimer. Both computed tomography pulmonary angiograms (CTPAs) and ventilation-perfusion scintigraphy (V/Q) scans are available in our hospital. CTPAs are recommended only for those with an abnormal CXR, patients with an intermediate V/Q scan result or pregnant women. Our radiologists do not screen these imaging requests. This study assessed the appropriateness of requesting of CTPAs after concern was raised by the radiology department that many CTPA requests were inappropriate.
Methods: Using our hospital electronic PACS system we identified all patients who had a CTPA or V/Q scan for the investigation of acute pulmonary embolism during the month of June 2005. The notes were reviewed to assess indication for CTPA, evidence of documentation of PTP, CXR findings, D-dimer, and result of CTPA. If PTP was not recorded it was calculated retrospectively using information from the notes and on the request cards.
Results: 52 patients had a V/Q and/or CTPA in this month. Data were available for 49 patients, 24 of whom had a CTPA. Of the total only 3/49 (6%) had a PTP recorded in the notes. Only 14/21 (67%) patients with low or intermediate PTP score had a D-dimer test before CTPA. All those with a high PTP had a D-dimer performed. One patient with a negative D-dimer and low PTP had a CTPA. CXRs were performed in 46/49 (94%) of cases and results were recorded in the notes in 43/46 (93%). Of those with an abnormal CXR 14/21 (67%) had a CTPA rather than a V/Q. Of those with a normal CXR who were not pregnant 5/23 (22%) had a CTPA rather than a V/Q. Only one of these five had a positive CTPA. Two patients had intermediate V/Q scans but only one had a subsequent CTPA (negative for pulmonary embolism). CTPAs were positive in only 4/24 (17%) patients. CTPAs provided useful alternative diagnostic information in 10/20 (50%) when negative, but not in any with a normal CXR. In 2/4 (50%) with a positive CTPA, pathology additional to pulmonary embolism was shown on the CT (lymphangitis and collapsed left lower lobe).
Conclusions: Despite concerns from the radiology department about inappropriate CTPA requests, we found that in fact CTPAs were not requested frequently enough in patients with abnormal CXR with possible pulmonary embolism. Most patients with a normal CXR who had CTPA rather than V/Q as suggested in BTS guidelines did not have a pulmonary embolism.
P124 LACK OF CLINICAL PROBABILITY ASSESSMENT IN PATIENTS INVESTIGATED FOR PULMONARY EMBOLISM
L. Power, N. J. Withers. Department of Medicine, Royal Devon & Exeter Hospital, Exeter, UK
BTS Guidelines state that assessment of clinical probability is essential in all cases of suspected pulmonary thromboembolism (PTE) (
). We have conducted a survey of all patients undergoing investigation for suspected PTE (VQ scan and/or CT pulmomary angiogram (CTPA)) at our Trust over a one month period. Case notes were reviewed and in cases where no probability score was available, a retrospective risk score was applied.
Sixty nine patients (27 female) were included. Forty two patients underwent CTPA, 15 underwent VQ scan and three had a VQ followed by a CTPA. The majority of scans (42, 75%) were performed on medical (including elderly care/oncology) admissions.
Abstract P124
Only two patients (3%) had a documented probability score in their notes. Retrospective scoring showed 27 (39%) with a low probability score, 33 (47%) with a moderate/high score and nine (13%) in whom a score could not be calculated. Major risk factors on retrospective scoring were immobility (29 cases), tachycardia (19), and lack of alternative diagnosis (12). Measurement of D-dimer levels was undertaken in 41 (68%) of patients of whom 39 (95%) had a raised level.
Thirteen CTPAs were positive, one VQ scan showed high probability, seven indeterminate probability, and 10 low probability. The relation between retrospective clinical probability score, D-dimer result and scan result is shown in the table (indeterminate VQ graded as positive).
This survey shows that clinicians are not adhering to published guidelines on assessment and investigation of suspected PTE, and that assessment of clinical probability of PTE is not being undertaken. The high percentage of positive D-dimer measurements in this group might suggest that this is driving requests for CTPAs and VQ scans rather than assessment of clinical probability.
Local guidelines for assessment and investigation of PTE are being introduced and adherence to them will be audited.
P125 PULMONARY EMBOLIC DISEASE: A PROTOCOL WITH THE APPROPRIATE USE OF CLINICAL PROBABILITY AND D-DIMER IS FEASABLE AND SAFE IN THE INVESTIGATION OF SUSPECTED PULMONARY ENBOLUS, IN THE SETTING OF A DISTRICT GENERAL HOSPITAL
G. S. J. van Rensburg. Yeovil District Hospital, UK
Background: Computerised tomographic pulmonary angiography (CTPA), is increasingly the investigation of choice in the diagnosis of pulmonary emboli. This is putting an extra burden on already stretched radiology resources. A negative D-dimer combined with a low clinical probability has been shown to be effective in excluding pulmonary emboli,1 without using valuable radiological resources.
Aim: The aim of this audit was to examine if a protocol with the appropriate use of D-dimer and clinical probability, in the investigation of suspected pulmonary emboli is safe and feasible at our hospital, and if it would reduce the need for CTPA.
Methods: The clinical probability for having pulmonary emboli was determined retrospectively, in 100 patients, who underwent CTPA. 50 patients had a definite diagnosis of PE and 50 had a negative CTPA. Clinical probability was determined according to national guidelines,2 using a set protocol (fig 1). Most patients had a D-dimer assay (the Medical Devices Agency (MDA) latex test). A D-dimer value >0.4 mgFEU/ml was regarded as positive.

Protocol to determine clinical probability.
Results: Although a low (12%) and intermediate (42%) clinical probability for pulmonary emboli was determined in the pulmonary emboli positive group, D-dimer was positive in all of the cases where it was requested (fig 2). This provides a definite safety mechanism.

Clinical probability and D-dimer in the pulmonary emboli group.
A majority of patients had a low (40%) and intermediate (50%) clinical probability in the CTPA negative group. Although a large proportion had a positive D-dimer,
CTPA could have been avoided in a definite 5 (10%) cases where a negative D-dimer with a low and intermediate clinical probability would have excluded in a potential further nine (18%) cases, CTPA could have been avoided if D-dimer was done with a negative result (fig 3).

Clinical probability and D-dimer (pulmonary emboli negative).
Conclusion: D-dimer and clinical probability is safe and feasible to exclude pulmonary emboli in the clinical setting of a district general hospital. This screening method may also reduce the need for CTPA.
1
2
Cystic fibrosis
P126 PREVALENCE OF ANXIETY AND DEPRESSION IN ADULTS WITH CYSTIC FIBROSIS
A. B. Palamarthy1, C. E. Bolton1,2, D. E. Stableforth1, I. A. Campbell1, C. A. Davies1, J. E. Jenkins1, D. J. Shale1,2. 1Cystic Fibrosis Centre, Llandough Hospital, Penarth, Wales, UK; 2Department of Respiratory Medicine, Cardiff University, Llandough Hospital, Penarth, Wales, UK
Introduction: In patients with cystic fibrosis (CF), anxiety and depression affects both quality of life and adherence to therapy.1–3 Validated questionnaires formulated for use in a non-psychiatric setting can detect the presence and severity of anxiety and depression, which is often overlooked in routine assessment.
Method: The hospital anxiety and depression questionnaire (HAD) was completed by consecutive, consenting adults when clinically stable: either at the end of a two week iv course of antibiotics or in the outpatient clinic. A score ⩾8 is deemed clinically significant.
Results: Of the 69 patients (38 male), median (range) age 27 (18–45) years, 34 had FEV1<50% predicted, 14 had low BMI (<20 kg/m2), with no sex difference for these measures. Chronic P aeruginosa infection was present in 68, of whom six had B cepacia, four MRSA, and one all three. In the preceding year, the median number of hospital admissions was: 2 (0–9), total inpatient days: 18 (0–213) and total courses of iv antibiotics: 3 (0–10). Anxiety was found in 33 (48%) patients (13 male), while 10 (15%) patients (six male) had depression scores, with nine of these 10 also with anxiety. More females had anxiety scores than males, √2, p = 0.012. Only 12 patients had previously received antidepressants: six with current depression scores, 10 with current anxiety scores. FEV1% predicted and BMI were not different between those with high or normal anxiety or depression scores. No transplant (heart, liver or lung) recipients, n = 6, had depression scores, while two had anxiety scores. The number of iv antibiotic courses and hospital admissions in the last year were greater in those with either high anxiety or high depressive scores compared with those with normal scores, but the number of days in hospital was similar. The number of hospital admissions was related to both anxiety (r = 0.281, p = 0.019) and depression scores (r = 0.462, p<0.01), and inversely to FEV1% predicted (r = −0.473, p<0.01). Logistic regression, with anxiety score as the dependent variable, revealed sex as the only predictive variable with an odds ratio (OR) for male sex: 0.286 (0.106 to 0.774). For a depression score, only the number of admissions was predictive: OR 1.7 (1.2 to 2.4). Other variables assessed were sex, previous transplant, age, lung function, BMI, and presence of Bcepacia or MRSA.
Conclusions: There was high prevalence of anxiety and depression scores in adults with CF. Assessment of the psychological status using the HADS questionnaire is simple and may indicate patients requiring psychological support. This review was carried out when patients were clinically stable and may not reflect the impact of periods of illness and medical deterioration, decision making (for example, transplant), and bereavement.
1
2
3
P127 UTILITY OF IMPULSE OSCILLOMETRY IN PREDICTING GAS TRAPPING IN CYSTIC FIBROSIS
E. Toon1, D. Bilton1, M. D. Goldman2, C. Haworth1, K. E. Oates1. 1Papworth Hospital, Cambridge, UK; 2University of California, Los Angeles, California, USA
Cystic fibrosis (CF) is characterised by progressively worsening airways obstruction routinely assessed by spirometry. Small airways obstruction is monitored using measures of flow at low lung volumes (FEF75) and gas trapping (RV/TLC%). Although impulse oscillometry (IOS) is not used routinely in patients with CF, its sensitivity to small airways function and requirement for only passive patient cooperation makes it an attractive alternative to traditional lung function measurements. We compared spirometry, static lung volumes and IOS indices in 40 stable adult CF outpatients (17 female, mean FEV1 65% predicted (range 22–106%), mean age 24 (SD 12) years) at routine annual review.
R5 (total respiratory resistance) and X5 (peripheral airways capacitative property) showed non-linear relations with FEV1 (r = 0.75, p<0.0001; r = 0.87, p<0.0001 respectively) in which the IOS parameters showed relatively greater deterioration per unit change in FEV1 at lower FEV1 values. A similar relation was found when X5 was plotted against FEF75 (r = 0.66, p<0.0001), with X5 showing higher sensitivity when FEF75 suggested increased disease severity.
FEF75 and RV/TLC% showed good correlation (r = 0.82, p<0.0001), however the relationship between these two parameters was non-linear and FEF75 proved to be a poor discriminator of disease severity when RV/TLC% >40. Conversely, X5 plotted against RV/TLC% showed a strong linear relationship (r = 0.81, p<0.0001), with X5 able to reflect the degree of gas trapping even in severe disease.
It is suggested that X5 is a more sensitive indicator of gas trapping than FEF75 in severe disease.
P128 ROUTINE PLANER SCINIGRAPHY TO DETERMINE THE MOST APPROPRIATE NEBULISER FOR CYSTIC FIBROSIS PATIENTS
C. Waudby1, G. Wright2, J. Seymour1, S. Mulrennan3, A. Morice3. 1Department of CASS-Medicine, The University of Hull, UK; 2The Nuclear Medicine Department, Castle Hill Hospital, UK; 3Academic Department of Medicine, Castle Hill Hospital, UK
Introduction: Nebulisers are used for the administration of antibiotics and DNase in cystic fibrosis (CF). The percentage of aerosol delivered to the lungs via a nebuliser varies greatly depending on respiratory function, nebuliser technique and individual preference. We developed a protocol for the routine assessment of the pulmonary aerosol deposition within an individual; tested inter- and intraoperator consistency and nebuliser pulmonary deposition repeatability.
Method: Using lung ventilation scintigraphy we assessed the percentage of aerosol delivered to the lungs of 10 CF patients, via Pari LC Plus using Turbo-boy compressor and the Prodose (AAD) nebuliser. The nebulisers delivered 5 mg Salbutamol followed by approximately 20MBq of Tc99m-DTPA. FEV1 measurements were taken before and after nebulisation. Each patient visited the department on three occasions allowing one of the nebulisers to be used twice. Anterior and posterior images of the lungs, nebuliser chamber, and mouthpiece were taken immediately following nebulisation. Two operators processed the scintigraphic images; this was repeated twice to assess inter- and intraoperator consistency.
Results: The Pari delivered less activity to the lungs than the Prodose 1.47% (SD 0.46%) versus 2.58% (SD 0.86%), p⩽0.002. The mean FEV1 increase following Salbutamol nebulisation was 3.20% (SD 2.9%) (Pari) versus 3.6% (SD 4.06%) (Prodose) percent predicted. The mean activity remaining in the nebuliser chamber was 65.45% (SD 14.21%) (Pari) versus 83.61% (SD 12.22%) (Prodose). The intra and inter operator reproducibility was 0.13% (SD 0.1%) versus 0.025% (SD 0.07%). The mean aerosol lung deposition difference between repeated visits for the same patient using the same nebuliser was 0.26% (SD 0.3%) (Pari) versus 0.25% (SD 0.38%) (Prodose).
Conclusion: The routine use of gamma scintigraphy for the assessment of nebuliser aerosol pulmonary deposition in CF patients allows the clinician to make an informed choice as to which nebuliser best suits an individual based on the percentage of medication they receive. This technique may help optimise nebuliser treatment and improve patient care.
P129 TOBROMYCIN NEBULISER SOLUTION IN THE TREATMENT OF CYSTIC FIBROSIS PULMONARY EXACERBATIONS: EFFECT ON SPUTUM PSEUDOMONAS AERUGINOSA DENSITY
M. Al-Aloul, H. Miller, M. J. Ledson, M. J. Walshaw. Adult CF Unit, The iothoracic Centre, Liverpool, UK
The best method of delivering antibiotics in the treatment of cystic fibrosis (CF) pulmonary exacerbations is debatable. Pa in the “conductive lung zone” is better targeted with aerosolised antibiotics whereas the distal “respiratory zone” is less accessible to this route compared with systemic antibiotics administration, which achieves higher alveolar drug levels. We hypothesised that the combination of nebulised and IV antibiotics may be a more effective “double hit” approach than IV antibiotics alone. To investigate this further, using a randomised crossover design we compared the effects of nebulised vs IV tobramycin on Pa sputum density in 13 CF patients (mean age 22 years (SD 7), FEV1% predicted 65 (SD 22), BMI 20.2 (SD 3.5), seven males), chronically infected with the Liverpool epidemic Pa strain, who were admitted with pulmonary exacerbations. Sputum isolates were sensitive in vitro to both colomycin and tobramycin.
Patients were randomised to receiving 14 days of either nebulised tobramycin (TOBI, 300 mg bd, Pari LC Plus nebuliser) or IV tobramycin (mean daily dose of 8.2 mg/kg (SD 1.5) in 2–3 divided doses). At the second exacerbation, the alternative form of tobramycin was given. Therapeutic serum concentrations (trough of <2.0 mg/l and peak of 6–10 mg/l) were maintained throughout the IV antibiotics courses. At every exacerbation all patients also received IV colistimethate sodium (Colomycin) 2 megaunits tid. The mean interval between admissions was 7.8 months (SD 5.5). Allowing for age change, baseline patient characteristics and the remainder of their therapy was otherwise identical in the two inpatient episodes.
Sputa before and after each treatment were examined; sample quality in two prevented further analysis. In the remaining 11 patients, there was a trend for baseline Pa sputum density to be higher before TOBI treatment (6.34 log10 cfu/ml (2.1) v 4.91 (1.3), p = 0.078). Within-group analysis showed that TOBI but not IV tobramycin resulted in a significant reduction in sputum Pa density (−1.16 log10 cfu/mi (0.93), p<0.001 v −0.48 (1.4), p = 0.066). However, the observed difference in the mean reduction in Pa density was not significant (0.68 log cfu/ml, 95% CI −0.26 to 1.62, p = 0.18).
We have previously shown that high dose nebulised TOBI, combined with a second appropriate IV antipseudomonal antibiotic, is as effective in treating acute CF pulmonary exacerbations as IV tobramycin, with the added advantage of nephro-protection (BTS winter meeting 2004). A superior effect on sputum Pa density adds further weight to the notion that this novel therapeutic approach targeted to the site of infection may be superior to conventional IV therapy in managing CF exacerbations, a subject that merits further research.
P130 IMPACT OF RESPIRATORY VIRUSES IN CYSTIC FIBROSIS
D. Wat1, C. M. Gelder1, S. Hibbitts1, F. Cafferty2, I. J. M. Doull3. 1University of Wales College of Medicine, Cardiff; 2Papworth Hospital NHS trust, Cambridge; 3University Hospital of Wales, Cardiff, UK
Background: Cystic fibrosis (CF) is a common autosomal recessive disease caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR), with progressive obstructive lung disease being the major cause of morbidity and mortality. Bacteria are the major respiratory pathogens in the initiation of pulmonary exacerbations in CF but the role of respiratory viruses could have been underestimated in the past due to insensitive laboratory detection methods.
Objective: To evaluate the frequency of respiratory viral infection in a group of paediatric CF patients.
Methods: Between December 2002 and May 2004, pernasal swabs were obtained from 71 CF patients below the age of 18 years whenever they developed upper respiratory tract symptoms and when they attended their routine hospital appointments. Viral nucleic acids were extracted by silica slurry1 and were subsequently amplified in “real time” by nucleic acid sequence based amplification (NASBA) using molecular beacons. This is a method which has been proved to be more sensitive than traditional methods such as cell culture and immunofluorescence and it also provides a rapid turnaround of results within 120 minutes, hence allowing diagnostic virology to have an impact on patient management.2 Respiratory viruses being sought in this study included influenza A, influenza B, parainfluenza types 1 to 4, respiratory syncytial virus, rhinoviruses, and coronavirus.
Results: Of the 138 symptomatic pernasal samples and 136 asymptomatic ones which were studied, the viral detection rate was 46% and 16.9%, respectively. There were significant differences in influenza A (p<0.05), influenza B (p<0.05), and rhinoviruses (p<0.05) detection between the two sample types. When all types of respiratory viruses were considered, there were significantly more viruses detected in the symptomatic samples (p<0.05).
Conclusion: Our results provided evidence that viruses were more likely to be isolated from CF patients during respiratory exacerbations. In particular, influenza A, influenza B, and rhinoviruses were more likely to be involved in the exacerbations of CF.
1
2
P131 PROINFLAMMATORY CYTOKINES IN ADULT CYSTIC FIBROSIS PATIENT IN A STABLE STATE AND DURING PULMONARY EXCAERBATIONS
S. Sarfaraz1, F. S. Wong2, N. A. Jarad1. 1Adult CF Centre, Bristol Royal Infirmary, Bristol BS2 8HW, UK; 2Department of Cellular and Molecular Medicine, School of Medical Sciences, University of Bristol, Bristol BS8 1TD, UK
Background: Cystic fibrosis is characterised by a self-perpetuating cycle of airway obstruction, chronic bacterial infection, and vigorous inflammation resulting in structural damage. The inflammatory markers used clinically to assess pulmonary exacerbations are often not helpful.
Aims: This study aims at assessing the level of circulating proinflammatory cytokines in CF patients with and without pulmonary exacerbations and to compare them with an age matched control subjects.
Patients and Methods: Exacerbation was defined as a change in more than two respiratory symptoms and/or lung function tests deemed to require an oral or intravenous course of antibiotics. Blood samples were taken from 21 patients in a stable state, at presentation of pulmonary exacerbation and two weeks after treatment. Sera were also taken from 14 age-matched healthy controls. The following cytokines were measured in sera: IL-6, IL-8, IL-1β, IL-10, IL-12p70, and TNFα using a cytokine multiplex bead assay and flow cytometry.
Results: All the proinflammatory cytokines measured in sera, with the exception of TNFα (unmeasurable) showed higher values in stable cystic fibrosis patients as compared to healthy controls. The values of IL-12p70 reduced at the start of exacerbations and further decreased two weeks after treatment. Serum IL-6 increased at the start of exacerbation, but returned to baseline values at the end of exacerbations.
Conclusion: The systemic proinflammatory cytokines measured were increased in cystic fibrosis patients as compared to controls, indicating chronic low level inflammation, even when clinically well. The changes in IL-6 and IL-12p70 may provide useful markers of inflammation in exacerbation. Functional studies may indicate how these changes during exacerbations reflect variable behaviour of the cells secreting the cytokines.
Funded by MMO2 and E-San LTD.
P132 DETECTION OF INCREASED GLUCOSE CONCENTRATIONS IN LOWER AIRWAY SECRETIONS FROM PEOPLE WITH CYSTIC FIBROSIS
A. L. Brennan1,2, K. M. Gyi2, N. Clark1, D. A. Fisher3, D. M. Wood1, D. L. Baines1, B. J. Philips1, D. M. Geddes2, M. E. Hodson2, E. H. Baker1. 1Glucose and Pulmonary Infection Group, St George’s, University of London; 2Royal Brompton Hospital; 3University of Surrey, Roehampton, London, UK
Background: Glucose concentrations are low in normal human airway secretions, but rise when blood glucose is increased or the airway epithelium is inflamed (
). Glucose in airway secretions was associated with increased isolation of respiratory pathogens in sputum from patients intubated on intensive care (Philips. Thorax 2005 (in press)). Glucose in airway secretions could contribute to accelerated pulmonary decline in people with cystic fibrosis (CF) who develop hyperglycaemia by promoting airway infection or inflammation. The aim of the present study was therefore to determine whether glucose concentrations were elevated in lower airway secretions from people with CF with and without hyperglycaemia.
Methods: Paired blood glucose (BG) measurements and 15 minute exhaled breath condensate collections for determination of airway surface liquid (ASL) glucose concentrations (
) were made in 23 healthy volunteers (HV), 10 people with CF and normal glucose tolerance (CF-NGT), 17 people with diabetes mellitus without CF (DM), and 10 people with CF related diabetes (CFRD). ASL glucose concentrations were compared between groups at BG concentrations ⩽7.0 mM, 7.1–11.0 mM, and >11.0 mM. Participants gave informed consent and the study was approved by the Local Research Ethics Committee.
Results: In people with BG ⩽7.0 mM, ASL glucose was: HV, 0.4 (SD 0.2) mM; CF-NGT, 2.0 (SD 2.0) mM; CFRD, 3.1 (SD 1.5) mM; p<0.0001 (analysis of variance). In people with BG 7.1–11.0 mM, ASL glucose was: CF-NGT, 2.0 (SD 0.5) mM; DM, 1.4 (SD 0.6) mM; CFRD, 5.2 (SD 2.8) mM; p = 0.026. In people with BG >11.0 mM, ASL glucose was: CF-NGT, 3.5 (SD 1.2) mM; DM, 1.2 (SD 0.7) mM; CFRD, 6.1 (SD 1.8) mM; p<0.0001.
Conclusions: At given blood glucose concentrations ASL glucose was HV<DM<CF-NGT<CFRD. This suggests that airway glucose concentrations are increased by hyperglycaemia (DM) and airway inflammation (CF-NGT), but most when hyperglycaemia and airway inflammation co-exist (CFRD). Increased airway glucose concentrations in people with CF could increase bacterial load by stimulating bacterial growth or impairing host immunity.
P133 CD14+CD16+ BLOOD MONOCYTES IN CYSTIC FIBROSIS
S. Rao, A. K. A. Wright, S. Range, L. Ziegler-Heitbrock, J. Grigg. Department of Infection, Immunity and Inflammation, University of Leicester, Leicester, UK
Background: Cystic fibrosis (CF) is characterized by recurrent airway infection and inflammation and the monocytes/macrophages may contribute to this. We hypothesized that patients with CF would exhibit an increase in the circulating pool of pro-inflammatory CD14+CD16+ monocytes. In this study, we compared blood CD14+CD16+ concentrations in a group CF patient with healthy controls.
Method: Whole blood was obtained from 11 cystic fibrosis patients (mean age 21 years, range 11–34 years) and six healthy volunteers (mean age 26 years, range 22–35 years). Four CF patients had an active exacerbation. Ten CF patients were on steroid therapy of which one was receiving oral prednisolone and rest on inhaled steroid. For each subject, 100 μl of whole blood was stained with fluorescent-labeled anti-CD14, anti-CD16 and anti-HLA DR antibodies. Flow cytometry was performed after lysis of red blood cells. 100 μl of flow count beads were added to each sample to determine absolute cell counts.
Results: The absolute number of CD14+CD16+ monocytes was significantly higher in CF compared with healthy controls (mean (range) cell count per μl blood: 37 (8–97) and 18 (9–26) respectively, p = 0.035, 95% CI 1.62 to 36.77). There is also a trend for an increase in the CD14++ monocyte concentrations in CF (mean cell count per μl blood: 417 and 271, p = 0.08, 95% CI −20.3 to 311.2). One of the four CF patients sampled during an exacerbation had a very low CD14+CD16+ concentration (8 cells/microlitre blood).
Conclusion: The circulating pool of CD14+CD16+ monocytes is increased in CF, compatible with a role for these proinflammatory cells in maintaining chronic pulmonary inflammation in this condition. Further study of the clinical and therapeutic correlates associated with increased number of CD14+CD16+ monocytes will allow us to understand their role better in CF.
P134 CONTROL OF METHICILLIN RESISTANT STAPHYLOCOCCUS AUREUS AT A LARGE CYSTIC FIBROSIS CENTRE
A. D. McSorley, M. E. Dodd, B. Isalska, A. K. Webb, A. M. Jones. Manchester Adult Cystic Fibrosis Centre
Introduction: The spread of methicillin resistant Staphylococcus aureus (MRSA) both in hospitals and the community is causing concern. At our centre inpatients have single rooms and there is a dedicated building for the treatment of patients with cystic fibrosis (CF). Patients infected with Burkholderia cepacia complex (BCC) are nursed in single rooms on general medical wards. Clinics are segregated according to sputum microbiology. Sputum is sent for culture at every admission and clinic visit. The policy at the centre is to isolate any MRSA positive patients and eradicate the infection with antibiotics. We report the outcome of this policy at our centre for the past 10 years.
Methods: All isolates of MRSA in sputum samples from CF patients were identified in our microbiology database from 1996–2005. Casenotes were reviewed and details recorded of the eradication regimen used and its success rate. Clearance of MRSA was defined as a minimum of three negative screens with at least six months between the first and last negative screen. A screen for MRSA included nose and groin swabs and sputum cultures.
Results: From 1996 to 2005 the numbers of patients at the adult CF centre increased from 192 to 260. 13 patients (4 male, 9 female) have had sputum positive MRSA infection. A further two patients were found to have nasal carriage of MRSA at time of transfer from paediatric centres; both were treated with mupirocin ointment and cleared the infection. Baseline demographics for the 13 sputum positive cases were mean (SD) age 26.1 (5.0) years, % predicted FEV1 62.0 (26.7) %, %predicted FVC 77.5 (23.3) %, BMI 21.6 (4.4). Five patients were MRSA positive at transfer from another centre. Four patients with MRSA infection had BCC infection and received inpatient care on general medical wards. 12/13 cases had eradication antibiotic treatment; in one case treatment was withheld as the patient was pregnant. 11/13 cases eventually cleared the infection and the other two are currently MRSA negative but awaiting further swabs to fulfil our definition of clearance. In 8/13 cases sputum became negative for MRSA within four weeks. Four of 13 cases needed repeated treatment (1× twice, 3× three times) with one case finally clearing MRSA 32 months after initial infection; one case had a close family member with MRSA infection and one worked as a nurse on a ward where there were frequent MRSA positive cases. A total of 17 antibiotic treatment regimens were used. Regimens chosen were determined by tolerability, allergy, availability, sensitivity of the organism, and previous use by the patient.
Conclusions: Strict isolation of positive cases and aggressive and if necessary repeated antibiotic treatment can control MRSA infection at CF centres. All CF centres should have a policy for management of MRSA infection.
P135 THE FUNCTION AND FATE OF NEUTROPHILS IN CYSTIC FIBROSIS
D. J. McKeon1, K. A. Cadwallader1, A. M. Condliffe1, D. Bilton2, E. R. Chilvers1. 1Respiratory Division, Department of Medicine, University of Cambridge; 2Adult CF Center, Chest Medical Unit, Papworth Hospital, UK
Introduction: The inflammatory response in cystic fibrosis (CF) is neutrophil dominated. The pathogenic capacity of these cells is determined in large part by their secretory capacity and tissue residency. Previous reports have demonstrated excessive reactive oxygen species (ROS) secretion by CF neutrophils, which has been postulated to be due the absence of CF transmembrane regulator (CFTR) protein expression in these cells.
Aims: This study sought to examine NADPH oxidase function and neutrophil longevity in patients with CF and to determine whether CFTR mRNA is present and CFTR protein expressed in human neutrophils.
Methods: Twelve clinically stable DF508 homozygote subjects were studied. Neutrophils were purified from peripheral blood using discontinuous plasma/Percoll gradients with age matched healthy control cells isolated in parallel. Superoxide anion production was measured using both cytochrome C reduction and chemiluminesence (CL) using the probes lucigenin or luminol under the following conditions; GM-CSF (100 ng/ml, 30 minutes), GM-CSF followed by fMLP (100 nM), fMLP alone, or PMA (1 ng/ml). Neutrophil apoptosis was examined by taking freshly harvested neutrophils suspended at 5×106/ml in Iscove’s MDM with 10% autologous serum and cultured at 37°C in flat bottom 96-well plates. Apoptosis was assessed morphologically. The presence of CFTR mRNA was examined in extracts from “ultrapure” neutrophils (residual mononuclear cells removed by negative magnetic selection-CD36/CD2/CD3/CD19/CD56/glycophorin A) and PCR amplification performed using primer sets specific for CFTR. CFTR Western blotting was performed using whole cell lysates and CFTR immunopreciptates.
Results: The cytochrome C signal and lucigenin and luminol median integral (AUC) and peak height (PH) CL signals were identical in all conditions for CF and control cells except the PH following PMA (controls 1.26 relative light units (RLU), CF 1.94 RLU, p<0.05). Investigation of apoptosis revealed no difference in percentage survival at 6 hours (CF 3.6 (SD 0.8) %, control 6.5 (SD 1.3) %, n = 12, p = 0.07) but increased serum dependent survival in CF neutrophils at 20 hours (CF 43 (SD 5) %, control 56 (SD 3) %, p = 0.0046). RT-PCR demonstrated low abundance CFTR mRNA (45 cycles) with an absence of CFTR expression on Western blots.
Conclusion: These data suggest that there is no intrinsic abnormality of NADPH structure/function in CF neutrophils but enhanced survival; the lack of expression of CFTR even in non-CF neutrophils and the serum dependency of the survival effect suggests that this may be related to the influence of a circulating factor(s).
P136 NATIONAL UNITED KINGDOM SURVEY OF CYSTIC FIBROSIS PULMONARY EXACERBATION: MANAGEMENT VARIATION AMONGST PAEDIATRIC AND ADULT PHYSICIANS
S. Higgs, N. A. Jarad. The Adult CF Centre, Bristol Royal Infirmary, Bristol BS2 8HW, UK
Background: Variation between clinicians on the definition of pulmonary exacerbation requiring intravenous or oral antibiotics in cystic fibrosis (CF) patients has been previously documented. Interobserver agreement on patients with mild symptoms and signs has not been investigated on a wider scale. This study aimed to investigate the agreement between CF physicians on scenarios in which antibiotics would be given for what the physicians considered to be pulmonary exacerbations.
Methods: We distributed questionnaires outlining seven scenarios to all CF adult physicians and CF paediatricians in the UK. We sought additional information on whether the clinic cared predominantly for adult or paediatric patients and on whether the clinic cared for a small number of patients (less than 50 patients) or a large number of patients (50 patients or more). In the scenarios the age, sex, and disease severity of the patient was the same. Factors varied included increase in symptoms, decline in lung function, increase in one symptom, change in microbiology, preholiday management, and pressure of a parent. In addition we asked an addendum question on the percentage of patients receiving regular elective antibiotics as a practice.
Results: Response was received from 166 of 229 (72.5%). They were 124 (75.1%) pediatricians and 41 (24.9%) adult physicians. Responses came from 65 (39.4%) clinics caring for 50 patients or more, and 100 (60.6%) clinics caring for fewer than 50 patients. Significant variation existed between all physicians and particularly between adult and paediatric physicians in several areas. Interobserver disagreement ranged from (18.8% to 60%). Significant variation existed if the clinic cared for adult or paediatric patients. CF physicians were, in general, more prone to providing intensive treatment if they cared for less than 50 patients. Paediatric physicians, particularly those working in smaller clinics, practiced regular “elective” antibiotics more frequently than adult CF physicians.
Conclusions: Wide differences exist in defining pulmonary exacerbations requiring intervention among adult and paediatric CF physicians in the UK. Type of specialty and number of patients cared for by physicians explain some of the differences. Significant difference in attitude still exists towards regular elective intravenous antibiotics between adult physicians and paediatricians. More objective methods of diagnosing and managing exacerbation are needed.
P137 AIR POLLUTANTS, SEASONAL VARIATION, AND PULMONARY EXACERBATIONS IN A COHORT OF ADULT CYSTIC FIBROSIS PATIENTS
N. A. Jarad1, T. Powell1, J. De Jaeger1, J. Burt1, W. Bird2. 1Department of Respiratory Medicne, Bristol Royal Infirmary, Bristol BS2 8HW, UK; 2Health Forecasting, Met Office, Exeter EX1 3PB, UK
Background: There has been limited study into the impact of noxious air pollutants on cystic fibrosis (CF). Exposure to particulate air pollution has been reported to be linked with an increased risk of exacerbation and decline in lung function in CF.1 We investigated the impact of ozone (O3), sulphur dioxide (SO2), nitrous oxide (NOX), and particulate matter with a diameter of less than 10 μm (PM10) levels, and rate of exacerbations in CF patients who attended the adult CF centre in the Bristol area.
Method: Number of exacerbations (requiring oral or IV antibiotics) for CF patients in Bristol was calculated from January 1999 to December 2003. Daily maximum recordings of O3, SO2, NOX, and PM10, measured in Bristol by the Meteorological Office, were also obtained for this period. These were then averaged for each week in the study period to give the weekly average maximum value for each pollutant. We correlated these weekly max values with the total number of exacerbations for each week during the study period. Total number of exacerbations for each month of the year during the study period was also calculated to assess for seasonal variation. We considered the cold season to be from October to March and the warm season to be from April to September.
Results: We recruited into the study 39 CF patients (27M, 12F), mean age 25.5 years (range 18–40) mean FEV1% pred 70.8% (range 22–157). Patients experienced 355 exacerbations during the study period that was converted into 262 weeks, see below. During the warm season there was 165 exacerbations (57 req orals: 108 req IVs) and 190 exacerbations (68 req orals: 122).
Conclusion: There was no significant correlation between ambient pollutants and exacerbations rate in CF. No significant seasonal variation in exacerbations rates between warm and cold months.
1
Abstract P137
Organisation of chronic obstructive pulmonary disease services: what is worthwhile?
P138 UPTAKE OF BRITISH THORACIC SOCIETY GUIDELINES IN HOSPITALS IN THE EASTERN REGION
M. Ali, A. G. Davison on behalf of the Eastern Region Thoracic Society (ERTS)Southend Associate University Hospital, UK
Background: The British Thoracic Society (BTS) has published various respiratory guidelines and these contain recommendations graded from A to D, depending on the level of evidence. In November 2004 the ERTS agreed to pool all local guidelines so that respiratory departments could have access to these to produce local guidelines.
Methods: Fifteen of the 16 trusts in ERTS submitted guidelines. At this time there were 23 BTS guidelines published since 1997. The uptake of A and B recommendations and the incorporation of algorithms from the BTS into local guidelines were studied.
Results: There were a total of 126 respiratory guidelines across the trusts with a variable number of guidelines per hospital ranging from 2–19. Most commonly produced local guidelines were for the management of community acquired pneumonia and acute asthma (10 out of 15 had guidelines for each). There were no local guidelines for seven topics covered by BTS guidelines. There were 57 local guidelines across the hospitals for 16 topics covered by BTS guidelines and the total possible number of grade A and B recommendation for these were 223 and 560 respectively. Uptake of these grade A and B recommendations, by trusts that had these guidelines, were 114 (51.1%) and 241 (43%), respectively. Nine BTS algorithms for various guidelines were available and total uptake of these by trusts, who had these particular guidelines, was 23 out of 52 (44.2%). 45 out of 57 (78.9%) local guidelines were dated by the trusts. Reference to BTS or other guidelines was given in 22 out of 57 (38.59%). Two of the 57 guidelines were the full BTS guidelines.
Conclusion: Hospitals almost universally adapt BTS guidelines for local use by shortening them. There is a need to improve the uptake of respiratory guidelines by hospitals and the incorporation of A and B recommendations. Local guidelines should be dated and referenced so that updates can be undertaken. Uptake of BTS guidelines may be improved if they included a shortened model version for local use.
P139 IMPACT OF PRIMARY CARE TRUST BASED CHRONIC OBSTRUCTIVE PULMONARY DISEASE TEAMS AT REDUCING HOSPITAL ADMISSIONS IN LEEDS IN 2003 AND 2004
M. Hewson1, P. K. Plant1, V. Walker2. 1Department of Respiratory Medicine, St James’s University Hospital, Leeds; 2East Leeds PCT COPD team, UK
Introduction: Leeds is a city of 747 000 people served by five primary care trusts and one acute trust. A cross city project has developed a model of PCT based chronic obstructive pulmonary disease (COPD) teams of nurses and physiotherapists. These teams provide diagnostic support to GP practices (DIAG), help with chronic disease management (CDM), community based pulmonary rehabilitation (PR), and early discharge (ED) (after 24 hours in hospital). A key focus is the prevention of future exacerbations.
Aim: This analysis aimed to determine whether the implementation of PCT based COPD teams reduces the need for hospital admission.
Methods: We compared the admissions per practice per 1000 registered population over 35 years for the periods April to December 2003 and April to December 2004 for each PCT. The services provided by each PCT in this time varied. In 2003 and 2004 two PCTs (North East and North West) had no teams and act as a control group. In 2003 South and West had no team and in 2004 South provided DIAG and CDM and West PR. These teams represent partial implementation. In 2003 East undertook DIAG and in 2004 provided DIAG/CDM/PR and ED—that is, full implementation.
Results: See table.
Abstract P139 Mean admission rate per 1000 registered age >35 years per practice per primary care trust
Full implementation in East Leeds led to a 29% fall in admission rate compared with 2003. There was a significant change in admission rate of 1.91/ 1000 aged >35 years per practice compared to the control group (95% CI 0.25 to 3.6, p<0.01). There was a non-significant trend to reduction in the partial implementation group.
Conclusion: Community based COPD teams offering diagnostic support, chronic disease management, pulmonary rehabilitation, and early discharge can reduce future admission rates, without needing to intervene at the point of admission.
P140 CONFIDENCE AND UNDERSTANDING AMONG GENERAL PRACTITIONERS AND PRACTICE NURSES ABOUT DIAGNOSIS AND MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE
D. M. G. Halpin1, S. Connellan2 on behalf of BTS COPD Consortium.
Telephone interviews were conducted with 61 practice nurses (PNs) and 39 general practitioners (GPs) to determine confidence about diagnosing and treating chronic obstructive pulmonary disease (COPD).
80% of GPs described themselves as confident/very confident. This has increased markedly from 52% in 2001. PNs were less confident, with only 55% citing confidence as high (57% in 2001). When differentiating between asthma and COPD, 79% of GPs (45% in 2001) and 70% of PNs said they were confident/very confident. Smoking history was seen as the main factor which differentiates COPD from asthma. More GPs thought cough was a decisive factor than PNs. Spirometry was deemed the most important investigation by both groups but more PNs thought a chest x ray was helpful. Half the GPs and PNs still thought reversibility testing was essential to diagnose COPD. 95% had access to a spirometry service either on-site or elsewhere. GPs were much more confident in interpreting spirometry results and, slightly worryingly there was a tendency for those PNs claiming to have had spirometry training (n = 16) to express lower confidence. Overall GPs and PNs are more confident in the use of spirometry than in 2001: 42% of GPs and 43% of PNs claimed to be confident in 2001 compared with 71% of GPs and 54% of PNs in 2005.
More respondents had heard of pulmonary rehabilitation than in 2001 (90% v 77%) and more had a programme in their area (76% v 49%). Only 54% GPs and 25% PNs were confident about who to refer for long term oxygen assessment but overall 35% had oximeters in their practices. 90% of respondents were aware of national guidelines. 44% were aware of the NICE guidelines, 22% of the BTS guidelines, and 17% of GOLD guidelines. 80% of those aware of guidelines stated that they had used them to audit current diagnosis/management of COPD and 24% to educate other healthcare professionals and patients.
A series of case histories were presented to the GPs, to evaluate consistency of diagnosis and treatment pathways. These showed that GPs were not as consistent in their diagnosis as they report and when asked what investigations would be carried out—of those citing COPD as a diagnosis only between 13% and 36% suggested spirometry.
These data suggest that confidence about the diagnosis and treatment of COPD has risen significantly since 2001. But awareness of specific guidelines remains low and there is some disparity between perceptions and reality especially in the area of investigations.
P141 THE DEVELOPMENT OF A TIER 2 CHRONIC OBSTRUCTIVE PULMONARY DISEASE SERVICE IN STOCKPORT
S. Gaduzo, K. Fern, D. O’Hara, S. Parry, J. Bootes, T. Emery. Stockport Primary Care Trust, UK
Background: Tier 2 developments are designed to relieve pressures on secondary care outpatient services. Several chronic diseases, including chronic obstructive pulmonary disease (COPD) have been the focus of Tier 2 developments and here we describe our experiences of setting up such a service for COPD patients in Stockport. The service is based around developing a multidisciplinary team consisting of a general practitioner with special interest (GPwSI), COPD specialist nurses, respiratory physiotherapist, spirometry measurement technician (MT03), and respiratory pharmacist. The aim was to triage general practitioner referrals to secondary care chest clinic for suspected COPD cases, to assess suitability for the Tier 2 service. At the same time treatment guidelines were condensed into a simple flow chart and a COPD pack was circulated to all local GPs.
Methods: Patients were accepted if they were >40 years old, smokers (or ex-smokers), diagnostic uncertainty, established COPD with management difficulties. Excluded were patients whose symptoms and signs suggested lung cancer (weight loss, haemoptysis, abnormal CXR), diagnosis of asthma, or other respiratory illness (for example, pulmonary fibrosis).
Results: From April to July 2004, 77 patients were triaged by the service. 25 were felt to be suitable for Tier 2 review (32%). 19 were assessed at the Tier 2 clinic, six failed to attend (they have all been sent another appointment). Of the 19 seen, 13 patients (68%) were seen only once and discharged back to their GP with management advice and treatment plan. Three (16%) had simple investigations at the Tier 2 clinic and were reviewed once before being discharged as above. Two (11%) were referred to secondary care chest clinic (suspected bronchiectasis). One (5%) was referred to secondary care cardiology clinic (aortic valve disease).
Conclusions: We have demonstrated that a primary care based Tier 2 service for COPD can effectively assess at least a third of secondary care referrals.
Future plans: Health economic data comparing Tier 2 versus secondary care management of COPD will determine the long term viability of the service.
P142 MANAGEMENT OF ACUTE EXACERBATIONS OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE BEFORE ADMISSION: FAILINGS IN PRIMARY CARE
C. Hayle1, D. Bowen1, M. J. Walshaw2, J. Hadcroft1. 1Royal Liverpool University Hospital, Liverpool; 2Cardiothoracic Centre, Liverpool, UK
Chronic obstructive pulmonary disease (COPD) is a common problem and its prevalence is particularly high in Liverpool. The Royal Liverpool University Hospital (RLUH) is a 963 bedded city centre teaching hospital serving a population of 350 000. During the period 1 April 2004 to 31 March 2005 there were 1227 admissions with COPD, with an average length of stay (LOS) of 10.6 days. Despite the heavy burden of COPD on this trust, support available to patients with COPD is limited. Prompt treatment of an exacerbation can shorten its length so should influence the requirement for hospital admission or LOS. We studied 44 consecutive patients (22 male, mean age 70.8 years) admitted to the respiratory wards at the RLUH with an acute exacerbation of COPD (AECOPD) to determine what action had been taken prior to admission and what, if any, treatment had been received. 29/44 had been admitted at least once during the preceding 12 month period with mean number of admissions being 2.52, range 0–17. Of the 44, only 16 (36.4%) were referred in by their GP with 28 (63.6%) self presenting to the AED, reflecting the heavy dependence of patients in Liverpool on secondary care. 38 (86.4%) reported shortness of breath as their reason precipitating hospital admission. The mean time between becoming unwell and attending hospital was 9.27 days (range 0–61). Only seven (15.9%) of this group had been given advice about recognising or treating an exacerbation, although 21 (47.7%) had contacted their GP early in their exacerbation to request a clinic appointment or home visit. Six (13.7%) increased their own treatment without seeking advice and nine (20.0%) neither increased their medication nor sought medical help. Of the 21 patients who contacted their GP, seven (33.3%) were prescribed antibiotics plus oral steroids, five (23.8%) received antibiotics alone, one received oral steroids alone (4.8%), and seven (33.3%) were not given any extra treatment. When asked for suggestions as to how their admissions could have been avoided, 13 cited medical reasons, four social reasons, and 22 did not feel that their admission could have been avoided, with one patient admitting he felt more secure in hospital.
This study suggests that there is a paucity of support for patients with COPD in our catchment area, which is reflected in the high proportion of patients who are unaware of how to recognise and treat an exacerbation. When patients contact their GPs, who provide the only support currently available, few receive appropriate treatment. Despite plans to the contrary by local PCTs, the patients still rely heavily on secondary care for the management of their exacerbations and frequently attend hospital for treatment. The lack of support in the community may in part explain the high rates of admission and readmission. Plans are afoot to begin a case management type service and this will hopefully address some of the issues highlighted here.
P143 A PROTOCOL DRIVEN NURSE LED CLINIC LEADS TO COST SAVINGS AND SHORTER WAITING TIMES FOR ROUTINE RESPIRATORY REFERERALS
L. Chandler, M. E. J. Callister, S. E. Williams, S. P. L. Meghjee. Pinderfields Hospital, Midyorkshire Trust, Aberford Road, Wakefield, West Yorkshire WF1 4TU, UK
Introduction: Increasing outpatient workloads together with new targets for waiting times, especially for lung cancer, has lead to increased pressure on respiratory outpatient services. Nurse led care has been proposed as a cost effective alternative to consultant led care in clearly defined clinical scenarios in other medical specialties such as cardiology (
), although other studies have not confirmed cost savings (
). However, less had been published regarding nurse led clinics in respiratory medicine. Internal audit within our respiratory department have recently identified an annual excess of 150 referrals over current capacity. Many routine referrals were for management of stable air flow limitation, and were considered suitable for initial assessment by a specialist respiratory nurse.
Methods: A highly protocolised nurse led clinic was established, and prospective audit data was collected for the first 100 patients seen. Staffing cost and waiting times were compared for nurse led and consultant led care. Case mix and outcome data were also collected. Time was allocated in a consultant clinic running concurrently with the nurse led clinic in which to discuss cases. Costs were calculated according to numbers seen in clinics and staff costs for H-grade nurse and a newly appointed consultant.
Results: 100 patients were seen in the nurse-led clinic between January and September 2004. Mean age was 63 years and 50% were female. 76 patients were new referrals from primary care, and 24 were follow ups from a COPD early discharge scheme. Eventual diagnosis were COPD (54 cases), asthma (19 cases), anxiety/hyperventilation (4 cases), and other diagnoses (23 cases including ischaemic heart disease, gastro-oesphageal reflux, benign pleural disease). Median time from referral to appointment was six weeks, compared to a 12 week wait for a routine appointment in a consultant clinic at the time of the study. The staff cost of seeing a new referral in a nurse led clinic was £11.00 (£8.92 for nurse time and £2.08 for time allocated for discussion with the consultant) compared with £22.30 for a new patient referral to a consultant clinic. The respective costs per review patient were £5.48 (£4.46 nurse time, £1.02 consultant discussion) compared with £11.16 in a consultant clinic. This represented just over a 50% cost saving for both groups of patients. The annual saving of three nurse led clinics per week would be £9746.
Conclusion: Highly protocolised nurse led clinics lead to more rapid assessment of patients, and result in a moderate cost saving. This study made the untested assumption that costs of investigations and support staff would not differ between nurse and consultant assessment. Furthermore this study did not systematically assess the safety of nurse led clinics, although no adverse management decisions were identified in this cohort.
P144 MULTIDISCIPLINARY WORKING IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE: IS IT WORTH IT?
J. Limond, C. Bell, D. Sieves1, C. Downie, C. Sugden1, L. McAlpine, D. Raeside. Monklands District General Hospital; 1St Andrews Hospice, Airdrie, UK
Introduction: Chronic obstructive pulmonary disease (COPD) is a major public health problem with a very variable clinical course. Consequently many patients have prolonged survival with very disabling symptoms and poor quality of life. (NHLBI 2000) Many healthcare providers and patients take a nihilistic view of the therapy of COPD, thus The Global Initiative for Chronic Obstructive Lung Disease (GOLD) has stated its aim to increase awareness and decrease morbidity and mortality from the disease. (
). In the chest clinic at Monklands Hospital we set out to assess the effectiveness of adopting a multidisciplinary approach to COPD as recommended by the British Thoracic Society guidelines. (
).
Methods: A pilot Multidisciplinary COPD clinic was set up in December 2003 with a core staff of a respiratory nurse specialist, a respiratory physiotherapist, a senior clinical physiologist, a palliative care physician, and a chest physician. Other professionals (including dietetics, occupational therapy, citizen’s advice, and carer’s representatives) have facilitated slots as required. Clinic slots last two hours when any relevant issues are discussed and a structured assessment tool is completed. Patients also completed the HAD and St George’s Hospital Respiratory Questionnaires.
Results: 46 appointments constituted 35 new attendances in 18 months. 16 male and 19 females, mean age 65 years (range 30–81) were included. Subjects had severe airflow obstruction (mean FEV10.8L (38% predicted)) and a high level of symptoms (mean MRC score 4.4) and had high scores in the St George’s Respiratory Questionnaire (SGRQ) for disease impact. A subgroup of patients had much higher FEV1 values (mean FEV1 1.2 l (56% predicted)) but this group also scored highly in the SGRQ for disease impact. Mean SGRQ total scores for patients with severe airflow obstruction was 69% and for those with milder airflow obstruction 71%.
Patients scored highly for anxiety and depression (HAD anxiety >11, 40% depression >11 34%) This had often been previously unrecognised. Abnormal body mass index (BMI) was noted in 46% of patients. Group mean exacerbation rates requiring admission pre clinic were 1.6 and post clinic 0.9 (p = 0.04), while exacerbations managed in primary care were 3.5 pre-clinic and 2.5 post-clinic (p = 0.3). Group mean HAD scores for anxiety were 10 pre and 10.5 post-clinic (p = 0.8) and for depression were 11.1 pre-clinic and 10.7 post-clinic (p = 0.5). Group mean SGRQ scores were 73.6% pre clinic and 66.3% post-clinic (p = 0.2).
Conclusion: This clinic has been well received by patients and GPs but is expensive to run in terms of staff time and thus far has been accessed by a small number of patients. The data presented above suggest that despite high apparent satisfaction rates within the MD team and an intuitive feeling that the clinic has succeeded, we have not been able to demonstrate definite, worthwhile benefit from this clinic.
P145 CHARACTERISTIS OF PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE WHO REPEATEDLY ATTEND THE ACCIDENT AND EMERGENCY DEPARTMENT DESPITE A CHRONIC RESPIRATORY SUPPORT SERVICE
H. Broomfield1, R. Singh2, M. Stern2, L. Restrick2. 1REDS/CRS Team, Whittington Hospital, London, UK; 2Department of Respiratory Medicine, Whittington Hospital, London, UK
Background: Despite chronic respiratory support (CRS) for patients with chronic obstructive pulmonary disease (COPD), including pulmonary rehabilitation, some patients still repeatedly attend accident and emergency (A&E). The aim of this study was to characterise this group to determine whether attendance reflects disease severity or other factors that might be amenable to intervention.
Method: Notes were retrospectively reviewed of the 75 patients coded with ⩾two A&E attendances in a year with COPD at the Whittington Hospital from January 2004. Data, including FEV1, comorbidities and use of hospital resources including CRS was analysed.
Results: 65/75 patients (87%) were correctly coded with COPD. The mean age of the 65 patients (31M; 34F) was 74 (range 43–97) years. Mean (SD) FEV1 was 0.74 (0.35) l and FVC 1.57 (0.66) l; n = 59/65). They had a total of 263 attendances to A&E, of which 69% (182), resulted in admission and accounted for 2472 bed-days. Alcohol excess was identified as a contributing factor for six patients (9%) who accounted for 52 attendances (20%), 30 admissions (16%), and 137 bed-days (6%). Although 41 (63%) patients were known to the CRS team, 27% of these (11) had had follow up discontinued due to comorbidity (5 patients; 4 with heart failure) or not willing to work with CRS (6 patients). These 11 patients had a high attendance (median 3; range 2–19/year) and accounted for a large number of bed days (median 38; range 2–161). Of 24 patients not known to CRS, 11 died before assessment, eight did not meet the CRS criteria, and five patients did, but had not been referred. Overall CRS was only started and continued in 27/46 patients assessed (59%). There were 24/65 deaths in 15 months from January 2004—that is, a 37% death rate. Mean (SD) FEV1 in the patients who died was 0.70 (0.30) l; FVC 1.48 (0.74) l; n = 19/24. Comorbidity was identified from the hospital notes (n = 20); ischaemic heart disease (9), congestive cardiac failure (6), hypertension (6), alcohol related problems (3). Cause of death on the death certificate (n = 14) was directly due to COPD in only half; bronchopneumonia (6), COPD (1), other sepsis (2), carcinomatosis (2), pulmonary embolus (1), coronary artery disease (1), heart failure (1). 13/24 (54%) deaths were known to CRS and five had had CRS withdrawn.
Conclusion: Patients with COPD who have ⩾two A&E attendances/year have a high mortality and are high users of hospital resources (including bed days) despite a comprehensive CRS service. Severity of disease, extensive comorbidity, particularly cardiac disease and alcohol excess, are important contributing factors. Thus, a broader approach, taking these factors into account, will be needed alongside the provision of CRS in order to reduce repeated A&E attendances.
P146 DEFINING CHRONIC OBSTRUCTIVE PULMONARY DISEASE BY A NEW COMMUNITY SPIROMETRY SERVICE IN LIVERPOOL
J. Hadcroft1, D. Russell2, M. McGee2, L. M. Lukehurst2, S. Callaghan3, M. J. Walshaw2. 1Royal Liverpool University Hospital, Liverpoo1; 2Central Liverpool PCT, Liverpool; 3Cardiothoracic Centre, Liverpool, UK
Chronic obstructive pulmonary disease (COPD) is a common problem but its true extent has never been known with any degree of certainty. The recent General Medical Services (GMS) contract encourages GPs to confirm the diagnosis of COPD with spirometry and reversibility and to compile a register of patients with COPD. For the first time it may become possible to determine the prevalence of COPD in England and Wales.
In order to provide our two feeder primary care trusts (PCTs) with a reliable and accurate measurement of lung function, the pulmonary function department of the Cardiothoracic Centre (CTC) in Liverpool provides a community spirometry service. Four sessions per week are conducted in the community and the fifth in the chest laboratory at the CTC. Patients select their preferred venue. We report our experience during the first 12 months.
There are 191 230 adults aged 35 years and over in the two PCTs. The only referral criterion for community spirometry was a clinical suspicion of COPD. In the first year, 3901 spirometries were carried out on 2490 patients. Of these 1238 (52%) were confirmed to have COPD; the majority have mild disease (936), 265 moderate, and 55 severe COPD according to NICE’s classification of severity. Of the 48% without COPD, 809 (32% of total) were normal, 256 (10%) restrictive, and 148 (6%) had asthma. The most popular venue was the CTC (33% of tests).
This service was set up to confirm the diagnosis of COPD in patients in whom there is a high clinical suspicion of COPD, yet only 52% of the group tested actually have this disease on spirometric grounds. 32% of the tests performed were normal, although this does not exclude a diagnosis of asthma. This suggests that the number of patients with COPD may actually be lower than previously suspected, with 0.67% of the over 35 population of our two PCTs having COPD confirmed by our spirometry service in the first year. However, there is still a large number of patients who have not yet been tested or have had spirometry elsewhere so this figure underestimates the extent of the disease. In the future the service should include asymptomatic smokers in whom intervention (smoking cessation) may prevent symptoms from developing.
A commonly held belief is that patients prefer to access services locally, but the emergence of the CTC as the most popular venue suggests that this may not be the case. This information should help in the development of future services. Community spirometry enables large numbers of patients to access pulmonary function, providing invaluable information about diagnosis and management. The provision of such a service by an established pulmonary function department ensures that PCTs are provided with accurate and high quality data.
P147 USE OF COMPLEMENTARY AND ALTERNATIVE THERAPIES BY PATIENTS ATTENDING A CHEST CLINIC
N. Cheng-Kai-On1, E. Mills2, T. Sarkodie3, S. J. Quantrill3. 1Canadian College of Naturopathic Medicine, Canada; 2Canadian College of Naturopathic Medicine-Division of Clinical Epidemiology, Canada; 3Whipps Cross University Hospital, UK
Background: The use of complementary and alternative medicine (CAM) by patients with general and chronic health complaints is high. National estimates in the UK suggest a population usage of 20% and a higher national usage in the United States of 62%. To date, no published studies have determined the prevalence of use of CAM within patients with respiratory illness. We aimed to determine the prevalence of use, therapies accessed, and sources of information among a cohort of respiratory illness patients attending a London outpatient chest clinic.
Methods: During the period of June to August 2004, we invited patients at the Whipps Cross University Hospital Chest Clinic to complete a structured questionnaire consisting of 12 questions assessing: use of CAM; conditions for which CAM was used; sources of information regarding CAM; satisfaction with CAM use; perceptions of safety of CAM and CAM products; and discussion with physicians about their CAM use. The study was approved by the local research ethics committee.
Results: Of 385 patients approached to participate, we received 295 completed questionnaires (response rate 77%). The median age was 58 (interquartile range 39–69). Respondents were primarily male and white (63%). Eighty seven patients reported a history of CAM use (29.5%). The most common forms of CAM reported were high dosage supplements and vitamins (13%); herbal medicines (12%); and exercise therapies (8%). Patients reported accessing a professional for information from a variety of sources, including: their GP (9%); homeopath (3%); and herbalist (2%). A further 21% chose not to discuss their CAM use with their physicians. Patients perceived the therapies and products to be largely safe, but some had safety concerns with: herbal medicine (18%); Oriental medicine (15%); high dose supplements (13%); homeopathy (9%); and acupuncture (9%). The most common reasons for using CAM in this population were: recommended by a friend or relative (29%); perceived improved health (20%); dissatisfaction with conventional medication (17%); used as a last resort (16%); concerns over adverse events related to prescription medications (10%); and read about it in a magazine article (10%).
Conclusions: The use of CAM within this population is above the national average. Considering the out of pocket expenses related to CAM use, the potential for adverse events and drug interactions with natural products, and supporting patient values, we recommend initiating discussion with patients regarding their CAM use in an open and non-judgmental manner.
P148 HEALTHCARE NEEDS ASSESSMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE SERVICES IN TRAFFORD
A. Verma1, G. Mates2, C. Franco3, L. Davies3, R. F. Heller1, B. Leahy2. 1Evidence for Population Health Unit, University of Manchester, M13 9PT; 2Trafford Healthcare NHS Trust, Moorside Road, Manchester M41 5SL; 3Trafford PCTs, Oakland House, Old Trafford, Manchester M16 0PQ, UK
Introduction: The introduction of intermediate care (Tier 2) in most primary care trusts (PCTs) will facilitate patients with COPD to be managed in primary care. The BTS/NICE guidelines on the management of COPD were published in 2004. Before setting up the intermediate care service, it was felt that a healthcare needs assessment would identify current and future gaps that could be filled by the Tier 2 team.
Methods: An audit of the admissions, practice based computer records and prescribing was undertaken by Trafford North and South PCTs. A questionnaire was also sent to 23 GP practices to determine needs in primary care.
Results: The audit of admissions and readmissions to Trafford Healthcare Trust between 1 January 2004 and 31 May 2004, showed that 50% of patients who were admitted with COPD were not under the care of a respiratory physician. There were 136 admissions with a primary diagnosis of COPD of which 17 were patients admitted twice, one patient ×4 and one patient ×6. The median (range) age on admission was 73.6 years (range 57.8–87.1) with an average length of stay of 11.1 days per admission. An audit of referrals to a respiratory outpatient department for COPD showed that 109 referrals out of 187 patients did not have COPD. A similar audit of the respiratory specialist nurses referrals revealed 20 out of 200 patients were inappropriately referred. The audit of computer based records at five GP practices, showed that severity, admissions, and spirometry results were not recorded routinely. The postal questionnaire to 23 GP practices had a 78% response rate (18/23 practices). 16/18 (88.9%) had a COPD register and all practices had a noted smoking status and offered smoking cessation support. Only 9/18 (50%) of nurses had received any training in COPD. 15/18 (83.3%) were trained in spirometry though only 10/18 (55.6%) used it to confirm diagnosis. Comments received included more training on COPD and spirometry.
Conclusions: 50% of patients admitted with COPD are not under the care of a respiratory physician who have a high outpatient workload. Primary care colleagues are excellent at smoking cessation but would like more training and support in diagnosis and management of patients with COPD.
Recommendations: To provide a Tier 2 service that has an assessment and diagnostic arm to improve patient satisfaction and convenience while reducing outpatient/inpatient stay through early diagnosis and appropriate management based on the BTS/NICE guidance. This service will need to be evaluated once established.
P149 USING POPULATION IMPACT MEASURES IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE FOR PRIORITISATION OF RESOURCES IN TRAFFORD
A. Verma1, I. Gemmell1, L. Davies2, R. F. Heller1. 1Evidence for Population Health Unit, University of Manchester, M13 9PT; 2Trafford PCTs, Oakland House, Old Trafford, Manchester M16 0PQ, UK
Introduction: There are several population impact measures (PIMs) which allow evidence based estimates of risk to be modelled using local data. This can help in decision and policy making. We previously estimated the number of admissions prevented by increasing the uptake of influenza and pneumococcal vaccination in the Trafford over 65s population.
Methods: Population size and incidence were gained from local data from the Office of National Statistics and Trafford PCTs data. A detailed review of the literature showed relative risk reductions of 0.33 and 0.48 for influenza vaccine and pneumoccocal vaccine respectively. The formula is:
N * Pe * [Pd *] BR * RRR
where N = population size, Pe = proportion of the population eligible, here the difference between current immunisation rates and “best practice” rates, Pd = proportion of the population with the disease (we do not need this as we are not intervening in a diseased population because all are eligible), BR = baseline risk of the outcome under investigation, RRR = relative risk reduction. The current immunisation rate for influenza and the assumed pneumococcal in the over 65 year group is 72%; we would aim to increase this to 90% and determine the number of events prevented by this change.
Results: The population size for Trafford is 225 000, the population aged 65+ is 45 000, and the proportion of population with the disease eligible for the vaccination is 90%–72% the BR is 4.3 hospitalisations per 1000 for COPD in this age group. The number of hospitalisations prevented in a year among this population is 11.5 admissions per year for influenza vaccine and 16.7 admissions per year for pneumococcal vaccine. This resulted in a potential saving of £38,000 and £56,000 per annum for influenzae and pneumococcal vaccine respectively.
Conclusions: The utility of PIMs is to help prioritise and implement national guidelines based on recent evidence and local data by comparing the different cost savings afforded by reducing the number of admission prevented.
Tuberculosis: epidemiology and contact tracing
P150 SHOULD MEDIASTINOSCOPY BE PERFORMED ROUTINELY FOR MEDIASTINAL NYMPH NODES WHEN TUBERCULOSIS IS SUSPECTED?
L. P. Ormerod, S. Khalid, J. Blaikey. Chest Clinic, Blackburn Royal Infirmary, Blackburn, Lancs BB2 3LR, UK
Although studies in the 1980s (before routine CT scan availability) suggested that mediastinoscopy was seldom necessary,1 and in the 2000’s that treatment with the standard regimen of 2RHZE/4RH gave excellent results clinically when no cultures were available,2 some colleagues have become anxious about the management of suspected tuberculosis (TB) mediastinal glands without either a tissue diagnosis or material for culture. TB mediastinal glands have been reported to show a definite reduction in size by two months with a pyrazinamide containing regimen.3
We analysed a cohort of patients treated for presumed mediastinal gland TB in the years 1999–2004 inclusive, with particular reference to modalities of investigation and treatment given. All patients coded as having TB mediastinal glands, with or without other sites were analysed. 63 patients, all of Indian Subcontinent group were assessed. 27 were male and 33 female. 16 (25/%) were seen as contacts of household cases, half (8) of sputum microscopy positive cases, and six (9%) from new immigrant screening. The remainder presented symptomatically. 28 had TB at another site: lymph node 14; pleural effusion and pulmonary four each, abdominal, two; bone, skin, testis, and retina, one each. Only 12 had a CT thorax performed. Most cases were supported by TB at another site and or the setting of immigrant or contact screening supported by a positive tuberculin test. Some of the CTs were done to confirm borderline hilar enlargement or distinguish it from vascular shadowing. Two patients only had mediastinoscopy. One young female who had TB cervical glands on histology, but a grade 1 Heaf test, and another case with medisatinal nodes and a positive Heaf 3, but splenomegaly on CT. Both had the diagnosis of TB confirmed at mediastinoscopy.
Virtually all patients showed a definite reduction in mediastinal node volume after two months of RHZE initial phase. This confirms the pre-CT finding that mediastinoscopy does not need to be done routinely, but only in those who have atypical features, or in whom there is not x ray improvement after two months of chemotherapy.
1
2
3
P151 IMPORTANCE OF ACCURATE CLASSIFICATION OF DEATHS IN PATIENTS WITH TUBERCULOSIS
N. Boparai, R. Miller, A. Goodburn, G. Scott, H. Booth. TB Clinic, Middlesex Hospital, University College Hospitals, London W1T 8AA, UK
Background: The London Tuberculosis Register (LTBR) gives four outcomes for patients with TB who die: TB cause, TB contributed [Contrib], TB incidental, TB influence unknown (TBIU). Completed treatment calculations (target >90%) permit exclusion of cases whose TB was incidental to cause of death.
Aims: To review causes of death in patients notified with TB between January 2002 and December 2004 inclusive in order to assess the impact of death classification on the calculation of performance targets.
Abstract P151
Methods: Retrospective case note review of 17 cases of TB who died.
Results: The final LTBR outcome was modified in 12 (71%) cases after case note review. Death rates from TB: initially = 4%, after note review = 2%.
Conclusion: This study shows the importance of review of death in cases of TB who die in order to give an accurate final outcome on the LTBR. This process may be difficult and time consuming as these complex cases are often under the care of several specialties and die out of hospital/in other hospitals; information from necropsy is pivotal.
P152 HOW IS PERIPHERAL LYMPH NODE TUBERCULOSIS MANAGED IN CLINICAL PRACTICE?
J. Blaikey, S. Khalid, L. P. Ormerod. Chest Clinic, Blackburn Royal Infirmary, Blackburn, Lancs BB2 3LR, UK
The British Thoracic Society’s third lymph node study confirmed that a six month short course chemotherapy was effective for peripheral lymph node tuberculosis, but as in the earlier studies showed that node enlargement, new node development and sinus formation were not uncommon both during1 and after treatment.2 During treatment new nodes developed in 16–22%, and sinus formation in 8%. 23–41% had residual nodes at the end of treatment. 5% had new nodes or enlargement of residual nodes after treatment but there were no culture confirmed relapses.
We describe a cohort of patients treated between 1999–2004 inclusive for lymph node tuberculosis, with emphasis on diagnostic procedures, the need for interventions and/or corticosteroid treatment during TB treatment, and events after the completion of TB treatment.
46 patients were identified 42 (91%) were of Indian Subcontinent ethnic origin and four (9%) were of white ethnic origin. 10 (22%) were diagnosed by positive histology and culture, 18 (39%) by positive culture only (aspiration), 13 (28%) by histology only, and only five (11%) by clinical diagnosis. Seven (15%) had mediastinal gland TB and 3/28 of those with positive cultures had isoniazid resistance. 2RHZE/4RH was given as standard treatment, unless there was pyrazinamide intolerance (2RHE/7RH) or proven isoniazid resistance (2RZE/7RE).
After commencement of TB treatment as above, recurrent aspiration of nodes was required in 13 (28%), new nodes developed in four (9%) and corticosteroids were needed in five (11%). 10 (22%) had residual nodes at cessation of treatment. Five (11%) were referred back after treatment because of new events. Three of these were immunological, but two patients had culture positive disease.
Peripheral lymph node tuberculosis continues to challenge clinicians because of the range of events than can occur during and after treatment. Similar proportions of clinical events occur in clinical practice as in the controlled trials.
1
2
P153 IS IMMIGRANT SCREENING FOR TUBERCULOSIS WORTHWHILE?
S. Grundy, J. Barclay. Chest Clinic, Royal Oldham Hospital, Greater Manchester, UK
The incidence of tuberculosis is high among the immigrant population. Screening of this population for tuberculosis, on arrival in this country, aims to detect those with clinical tuberculosis and uninfected people who may benefit from BCG vaccination. However, a recent review suggests that screening for active tuberculosis has little impact on public health and is not cost effective.1
Our experience of working in a district general hospital serving 260 000 patients, of which 10% are immigrants, was that the attendance rate was very low. It is known that the process for identifying those who require screening through the Port of Arrival system is inefficient.2 Between 1984 and 1998 no case of clinical tuberculosis was detected by our screening service. It was decided to stop inviting new immigrants notified from the Port Health Authority for screening. All local GPs were informed of this change, reminded of the symptoms of tuberculosis and invited to refer appropriate new immigrants for BCG vaccination.
We reviewed the incidence of tuberculosis in our population over the period 1993 to 2004. Comparison of the incidence of tuberculosis revealed no difference between the period when we provided full screening with the period when we did not. The average incidence of pulmonary tuberculosis before 1998 was 10.9 cases per 100 000 population compared with 10.6 cases per 100 000 population after 1998. The average incidence of all cases of tuberculosis notified was 16.1 cases per 100 000 population before 1998 and 17.1 cases per 100 000 population after 1998. This small increase in cases is consistent with a small increase in national figures for incidence of tuberculosis over this time period (11.2 cases per 100 000 population prior to 1998, 12.4 cases per 100 000 population after 19983) (see fig).

Cases of tuberculosis notified per year.
The cessation of screening of new immigrants did not affect the incidence of tuberculosis in our population. We suggest that further similar, larger studies are carried out to confirm our findings.
1
2
3
P154 OFFERING HIV TESTS IN THE TUBERCULOSIS CLINIC: IMPROVING CLINICAL PRACTICE USING A CONTINUOUS QUALITY IMPROVEMENT PROGRAMME
H. Booth, M. Noursadeghi, N. Boparai, A. Goodburn, G. Scott, R. Miller. TB Clinic, University College Hospital, London W1T 8AA, UK
Background: In 2001 the London Tuberculosis Group published a consensus document which stated that HIV testing should be routinely offered to every adult diagnosed with tuberculosis (TB) in London.
Methods: An audit (i) was undertaken to assess our dedicated TB clinic’s performance. As a result of this audit local guidelines were developed which recommended that HIV testing should be offered to all patients with TB at two months of treatment unless clinically indicated to offer it earlier. A re-audit was performed (ii) resulting in further training and production of guidelines on the content of HIV pre-test discussion. From 1 January 2005 a continuous quality improvement (CQI) programme was introduced. After every TB clinic information is collated in a simple Access database regarding the HIV status of the patient and the doctor that the patient saw. Individual performance compared to that of anonymised colleagues is fed back to the attending doctors.
Abstract P154
Results: See table.
Abstract P156
Conclusions: Producing guidelines and training did improve compliance with the London-wide recommendations. However, the most dramatic change has been with the introduction of CQI. As data are collected contemporaneously it is more accurate, complete, and easier to collect than retrospective audit. Feedback is more timely and individualised. This is important for training of junior staff that move frequently. Individual patients also benefit as, unlike conventional audit, they are identified as having “missed” testing early so that this can be addressed at a subsequent visit. It is envisaged that with CQI we will achieve the 100% target by the time patients’ have completed their TB treatment course.
P155 ONLY TELEPHONE REMINDERS IMPROVE ATTENDENCE AT A TUBERCULOSIS CONTACT TRACING CLINIC
A. L. Kerry1, C. Cale2, S. M. Menzies3, M. R. Hetzel2. 1Wonford Hospital, Exeter, UK; 2Bristol Royal Infirmary, Bristol, UK; 3Churchill Hospital, Oxford, UK
Introduction: Contact tracing for tuberculosis (TB) remains an important method of detecting undiagnosed infection. “Did not attend” (DNA) rates at such clinics are high. TB is more common in ethnic minorities and language barriers could therefore contribute to the DNA rates. We previously reported no apparent benefit from an explanatory letter translated into several languages over a standard appointment letter.1 However, other studies have suggested that automated telephone reminders improve returns after tuberculin skin tests2 and in TB care.3 In this further study we therefore compared the effectiveness of these two methods on attendance at a TB contact tracing clinic in a large inner city hospital serving a multiracial population.
Method: During the 12 month period 2001/02, patients were sent a standard appointment letter. During the second 12 month period 2002/03, patients were sent a standard appointment letter plus a translated letter that explained why the appointment was necessary.1 During the third 12 month period 2003/04, patients received a standard appointment letter only plus a telephone call two weeks before their appointment. The attendance rates for the three groups were compared using a χ2 test.
Results: Translated letters were sent to 363 individuals, 253 of whom attended.1 Of the 297 individuals contacted by telephone, 257 attended. Attendance rates were significantly higher among those who received a telephone call (86.5%) than those who received a translated letter (69.7%, p<0.001). During the study period 2003/04 154 individuals could not be contacted by telephone because no telephone number was available. Of these individuals 73 (47.4%) did not attend the clinic. The DNA rate among these individuals was significantly greater than that seen in historical controls that only received a standard appointment letter (DNA rates 28.4 v 30.3% v 47.4% for years 2001, 2002, and 2004 respectively p<0.001).
Conclusion: A telephone reminder two weeks prior to a clinic appointment results in increased attendance rates at a TB contact tracing clinic when compared to a standard appointment letter alone or a translated explanatory letter. Language barriers did not prevent communication. If all contacts gave a telephone number, attendance could be improved further.
1
2
3
P156 ELISPOT TEST IN DIAGNOSIS OF LATENT TUBERCULOSIS
A. E. Boyd, A. Ashcroft, G. H. Bothamley. Homerton University Hospital NHS Foundation Trust, UK
Introduction: Tuberculin (TST) is currently used in the diagnosis of tuberculosis (TB) but has a poor specificity. An elispot test based on secretion of interferon-γ by T cells in response to peptides of ESAT-6 and CFP-10 hold the promise of greater specificity. The National Institute of Clinical Excellence (NICE) in draft proposals recommend a two-step approach, using this type of test to confirm the significance of a positive TST. We examined one of these tests (T SPOT-TB, Oxford Immunotec) in parallel with the TST.
Methods: We conducted a single blind prospective case control study July 04–July 05 of 55 adult patients with suspected latent TB. The T SPOT-TB test was performed in addition to TST and chest radiography.
Results: See table—the numbers in brackets refer to specimens that were not processed according to protocol (stored overnight or frozen before testing).
All four of the TST positive and elispot negative patients had been BCG vaccinated. The four TST negative and elispot positive patients were also all HIV negative, one patient was in the first trimester of pregnancy but there were no other immunocompromising conditions; they were aged 25, 29, 35, and 38 years and all had been BCG vaccinated.
The use of elispot to “confirm” a positive TST would have excluded 4/21 (19%; 95% confidence intervals (CI) 7.8% to 40.3%) of our patients from chemoprophylaxis or follow up radiography. The two-step approach, however, would have prevented 4/18 (22%; 95% CI 9.1% to 45.5%) patients who were elispot positive from being offered chemoprophylaxis.
Conclusions: The proposed recommendations by NICE may reduce chemoprophylaxis by 7.8%–40.3%.
P157 AUDIT IN THE ROLE OF URINE IN THE DIAGNOSIS OF TUBERCULOSIS
E. Nour1, F. Karim2, B. Cherian2, S. J. Quantrill2. 1Ealing Hospital; 2Whipps Cross University Hospital, UK
Background: Early morning urine (EMU) samples appear to be sent in large numbers from patients suspected of having tuberculosis (TB), despite previous evidence that the yield is very low. The purpose of the audit was to assess the usefulness of urine analysis in the diagnosis of TB in order to improve the quality and efficiency of medical care.
Methods: This was a retrospective study, conducted between January 2000 and June 2004. All patients with positive urine cultures for Mycobacterium tuberculosis (MTB) were identified from microbiology records.
Results: During this period 9109 samples were submitted for acid-fast bacilli (AFB) testing from 3800 patients: 4984 sputum, 1122 urine (1025 sputum samples were sent for the same patients) and 3003 others—for example, ascitic, pleural fluid, bronchial, lymph node aspirate, pus, wound swab blood culture, etc.
Of all urine samples submitted for analysis, only 15 urine samples (1.3%) obtained from 10 patients were positive for TB. In these early morning urine (EMU) smear positive in seven out of 33 samples processed. Only three out of 10 patients had sterile pyuria. Of the 10 patients with positive urine for MTB, five patients presented with pulmonary TB, one patient presented with genitourinary symptoms and EMU culture was positive. The remaining patients had pleuroperitoneal, lymph node, and miliary TB.
The patient who presented with genitourinary symptoms had normal IVU and EMU culture positive for MTB responded to six months of antituberculous therapy. The rest of the patients had other source of specimens positive for MTB at the same time as positive EMU culture and hence the management was not changed by the result. Blood culture was positive in patients with HIV.
The cost of the diagnostic procedure in our study was calculated using Welcan schedule of time based unit values for quantitation of pathology workload, one urine sample cost £8.10 and 1122 samples incurred cost of about £9088.20 excluding nursing time and transport of specimens to the laboratory.
Mortier et al found that of 7200 EMUs analysed only 65 (0.9%) urine samples obtained from 33 patients (1.2%) were positive cultures for MTB.1 We have found that of 1122 EMUs analysed only 15 urine samples (1.3%) obtained from 10 patients were positive for MTB and this had changed the management in only one patient with renal TB and persistent sterile pyuria. These data suggest that submission of urine specimens to the microbiology laboratory for identification of MTB is rarely useful in the diagnosis TB.
Conclusions: We recommend EMUs for the diagnosis of TB in patients with persistent sterile pyuria, absence of other source of specimens especially in patients with HIV, miliary TB, and patients with suspected genitourinary TB.
1
P158 SHORT TERM BLEACH DIGESTION OF SPUTUM IN THE DIAGNOSIS OF PULMONARY TUBERCULOSIS IN PATIENTS CO-INFECTED WITH HIV
L. Lawson1,3, M. A. Yassin3, A. Ramsay2, E. N. Emenyonu1, T. D. Thacher4, P. D. O. Davies5, S. B. Squire2, L. E. Cuevas3. 1Zankli Medical Centre, Plot 1021, B5 Shehu Yar’adua Way, Abuja, Nigeria; 2EQUI-TB Knowledge Programme at; 3Liverpool School of Tropical Medicine, Pembroke Place, Liverpool L3 5QA, UK; 4Department of Family Medicine, Jos University Teaching Hospital, Jos, Nigeria; 5Tuberculosis Research & Resource Centre, Cardiothoracic Centre, Liverpool L14 3PE, UK
The short term bleach digestion of sputum has been reported to improve the yield of smear microscopy. At last year’s BTS winter meeting we presented evidence that in HIV negative patients a single bleached ZN smear produces the same diagnostic yield as three standard ZN smears. (
)
This has not been validated in areas with high HIV prevalence. We undertook a study to assess the performance of bleach digested smears to diagnose pulmonary tuberculosis (PTB) among patients with and without HIV.
756 PTB suspects were asked to submit three sputum samples and were offered HIV tests. Direct smears were prepared from each sputum specimen. One specimen was selected to prepare a digested smear, and one was cultured. 458 (61%) patients had PTB diagnosed by culture positivity, and 230 (56%) of the 413 patients screened for HIV were positive. 116 (50%) of the 225 HIV positive and 113 (62%) of the 181 HIV-negative patients with PTB were direct smear positive (p = 0.03). In comparison, one digested smear identified 111 (49%) of the 225 HIV positive and 108 (60%) of the 181 HIV negative patients with PTB (p = 0.04). Three direct smears identified 235 (51%) and one digested smear identified 229 (50%) of the 458 patients with PTB, but both methods were less sensitive in HIV positive than in HIV negative patients.
Conclusions: HIV positive patients were less likely to be smear positive, than HIV negative patients. One digested smear could improve the efficiency of PTB diagnosis independently of the prevalence of HIV.
P159 ADMINISTRATION OF BCG VACCINATION: SURVEY OF UK PRACTICE
M. E. Roberts, J. T. Macfarlane, A. Anderton, U. Leivers. TB Service, Clinical Respiratory Medicine, Nottingham City Hospital, UK
Aims: To discover current practice in areas of uncertainty in BCG vaccination.
Methods: Postal questionnaire sent to tuberculosis (TB) unit in 251 UK respiratory centres examining current practice in relation to: (Q1) the administration of BCG at sites other than to the upper arm, (Q2) revaccination in the absence of BCG scar in children, (Q3) assessment of HIV status prior to vaccination, (Q4) evaluation of risks for anaphylaxis prior to vaccination and (Q5) documented episodes of anaphylaxis in the last year, (Q6) availability of resuscitation equipment in location vaccine administered, (Q7) formal training in paediatric resuscitation techniques, (8) treatment of BCG ulcer.
Results: 148 questionnaires returned (59%). Of these: (Q1) 31% offered BCG at sites other than the upper arm, including upper thigh (91%), ankle (4%), back, buttock, and sole of foot. Only 17% of centres routinely ask patient about location preference prior to BCG. 24% would only administer vaccinations at non-standard site for clinical reasons, while 76% accept patient preference (for example, cosmetic). Doctors administer non-standard vaccinations in 43% of centres; both doctors and nurses in 8%, and nurses only in the remainder. (Q2) 64% of responders did not perform check heaf tests on children without scars from prior BCG, or offer repeat BCG. Of the 36% who did, 79% revaccinated children with a negative test. (Q3) 49% of centres routinely assess for HIV risk before BCG vaccination, with 72% assessing all patients and 24% immigrants and asylum seekers only. (Q4/5) 81% enquire about atopy before administering BCG, but only 4% (three cases) had encountered an allergic reaction requiring acute therapy. (Q6/7) 91% had resuscitation equipment available, but only 43% of staff administering BCG had been trained in paediatric resuscitation techniques. (Q8) Discharging, non-healing BCG ulcers were treated conservatively in 45% of centres, with antibiotics in 25%, and a combination of the two in 25%. The most popular antibiotic choices were isoniazid (46%) or a macrolide (36%). Duration of therapy varied widely from three to 90 days (median 28 days).
Conclusions: Results from this large survey show BCG practice varied widely. Only a third of centres offer alternative sites for BCG administration (the Department of Health Green Book suggests the thigh). Over a quarter revaccinate heaf-negative children in spite of prior vaccination, in accordance with the Green Book, but contrary to the new NICE guideline. Assessment of HIV status varied widely prior to BCG. The new NICE guideline advises HIV risk assessment in all patients. Allergic reactions are very rare. Most centres have resuscitation equipment available, but less than half are trained in paediatric resuscitation. The Green Book states that personnel should be trained in the treatment of anaphylaxis. Management of BCG ulcers was very variable—antibiotics being used in about half of centres. The NICE guideline offers no specific advice. Units should assess their practice in the light of new evidence based guidelines being produced by NICE.
P160 IS CONTACT TRACING OF ANY VALUE FOR FARMERS AND FARM WORKERS WHO HAVE BEEN IN CONTACT WITH BOVINE TUBERCULOSIS?
S. E. A. Dodds, C. D. Sheldon. Royal Devon & Exeter Hospital NHS Foundation Trust, Exeter, UK
Background: Bovine tuberculosis (BTB) is one of Britain’s biggest animal health issues and cost over £88 million in 2003.1 The incidence of BTB in Devon is the highest in England with 644 herds affected in 2004 and 4228 cattle slaughtered. Current British Thoracic Society (BTS) Guidelines for the Control and Prevention of TB2 suggest screening of all people who have been in close contact with open cases of BTB with pulmonary or udder lesions and those who have drunk unpasteurised milk. The high incidence of BTB in our region provides an opportunity to establish whether the prevalence of mycobacterium bovis is reflected in the human population.
Method: 72 farmers and farm workers from 25 herds within Mid and East Devon were referred to the Chest Clinic in 2004. 88.9% attended with reasons for non-attendance including timing of appointments around market days, harvest times and morning and evening milking. Data obtained on screening included health interviews, numbers of cattle affected, and whether herds were dairy or beef. Patients then had either a Heaf test or an x ray according to the BTS Guidelines (2000).
Results: No cases of mycobacterium bovis infection were identified. There was one abnormal chest x ray indicating exposure to pulmonary TB with no active disease seen. The numbers of cattle affected per herd varied from 1 to 35 with several herds having BTB continuously.
Conclusion: Outcomes from this analysis indicate that there is little value in contact tracing in this population. As a result of our findings in early 2005 the local Health Protection Agency changed their guidance and now send letters of information to both farmers and their general practitioners when they have been exposed to open cases of BTB. If these findings are replicated across the rest of the country this could support a national change in screening policy.
1
2
P161 CONTACT TRACING IN PULMONARY TUBERCULOSIS: A SURVEY OF CURRENT PRACTICE, 2004
S. R. Anderson1, J. M. Watson2, I. Campbell3. 1UCL Centre for Infectious Disease Epidemiology & HPA Centre for Infections, UK; 2HPA Centre for Infections, UK; 3Llandough Hospital, Cardiff, UK
Ten per cent of UK tuberculosis (TB) cases are found through contact tracing. The British Thoracic Society made recommendations on contact tracing in their 2000 code of practice (Joint Tuberculosis Committee. Control and prevention of tuberculosis in the United Kingdom: code of practice 2000.
). There is however variation in the application of these guidelines.
This national survey aimed to evaluate contact tracing procedures and contribute to the development of new guidance, including consideration by the National Institute of Health and Clinical Excellence (NICE). Questionnaires to assess contact tracing were sent to all health professionals who trace contacts.
192 questionnaires were sent and 141 responses received (response rate 73%). Over 90% of contact tracing is undertaken by nurses, 2% by respiratory physicians and 6.4% by health protection teams. Although 91% of TB services say they follow the BTS guidance, there is considerable variation in the use of:
-
an age cut off to determine contact investigation: 40% do not use this;
-
BCG status to determine investigation: 36% do not use this;
-
tuberculin skin tests: only 54% restrict these to contacts without BCG;
-
chest x rays: 70% offer to ALL contacts with a positive skin test;
-
chemoprophylaxis: 35% do not follow the guidelines.
Possible ways to improve contact tracing, while making best use of limited resources, include:
(a) contact tracing in prisons
(b) contact tracing in asylum seekers
(c) contact tracing in HIV positive contacts
The authors are supported by the Joint Tuberculosis Committee of the BTS.
-
Adding to future guidelines.
-
Develop clearer definitions of close and casual contacts.
-
Review of chemoprophylaxis regimes.
-
Review new tests for infection and their role in contact tracing.
-
Develop a new, standardised, evidence based protocol for contact tracing.
P162 RISE IN TUBERCULOSIS NOTIFICATIONS IN HEALTHCARE WORKERS IN AN INDUSTRIAL WESTERN EUROPEAN CITY
S. J. Jamieson, C. D. S. Williams, M. P. Jones, P. D. O. Davies. TB Research and Resource Unit Liverpool CTC, UK
In Liverpool between January 2000 and December 2002 (36 months) 3.5% of tuberculosis (TB) notifications were in healthcare workers (HCW). Of these seven cases, one had been born in the UK and one had been in the UK for 35 years. In the following two years, January 2003–December 2004, 20 HCWs were notified 4% and 16% respectively of total notifications. All cases were non-UK born and all but one had entered the country in the previous five years.
29% of the 2000–02 group were smear positive disease, 35% of the 2003–04 group fell into this category. Of the 27 cases all but three were from Africa or the Indian subcontinent.
HCWs with little or no contact to patients, such as pharmacists and microbiologists, were not included in the study. Over half were hospital (52%) or care home (11%) nurses with multiple and/or prolonged contact with vulnerable patients. A further 22% were hospital doctors.
Contact tracing for smear positive cases was extensive given the number of vulnerable contacts to HCWs. An average of 87 contacts per index case was identified. In some cases, incident meetings were called involving public health, microbiologists, clinicians, nurses, and managers. Patients and their GPs and/or consultants were contacted, press statements prepared, a helpline set up, and screening implemented and evaluated. None of this revealed any evidence of transmission in this country; strongly positive tuberculin reactors were always of the same ethnic group and likely to have acquired latent TB infection in their country of origin.
The rise in TB in HCWs is almost entirely connected with ethnicity and shows how increasingly dependant we are upon overseas workers in the health service. It also highlights the need for vigilance in TB screening and awareness in those entering the country from Africa and the Indian subcontinent, not only upon commencement of employment, but also in the first five years of residence.
P163 INTESTINAL PARASITES AND TUBERCULOSIS IN SOUTHEAST LONDON
T. Jalil, C. Corrigan, N. Price, H. J. Milburn. Departments of Respiratory Medicine and Infection, Guy’s and St Thomas’ Foundation Trust, London, UK
Background: Intestinal parasites (IPs) are common in areas of the world with high tuberculosis (TB) prevalence. Aswell as causing chronic debilitating illness, IPs induce pronounced T-helper (Th-) 2 responses, causing greatly increased production of IgE. The acquired cellular immune response to TB, however, involves a Th1 profile of cytokines in containing infection and the presence of Th2 cytokines is associated with severe disease. Studies have shown down regulation of Th1 cytokines and impaired Th1 responses in helminth infected subjects. These data suggest that infection with IPs may predispose to active TB infection.
Aim: of this study was to determine the prevalence of IP infection in patients with active TB in southeast London and whether IgE levels and eosinophilia are good markers for these infections in TB patients and their contacts.
Patients and Methods: IgE levels were measured in 30 and eosinophil counts in 45 patients with active TB, three with treated TB and 11 contacts. Serology for strongyloides, filaria, schistoma, and toxocara was performed in all with IgE levels >100 KU/l (NR 0–81) or eosinophil counts >0.4×109. All patients were offered HIV testing and most agreed. None was positive.
Results: IgE levels were raised in 19/30 patients with TB (63%) (mean 578; median 156; range 7–3557 KU/l), in 2/3 with treated TB (498; 166; 7–1320) and 6/11 contacts (55%) (744; 282; 18–4509). Eosinophilia was present in 6/45 (13%) TB patients, 1/3 treated TB, and 2/11 (18%) contacts. To date, serology has been completed in 14. 6/8 TB patients were positive (strongyloides 5, filaria 1, 1 toxocara, 1 taenia (from stool)) (one patient had evidence of three parasites); 1/3 treated TB patients (schistosoma), and 1/3 contacts (strongyloides). All those with positive serology originated overseas (3 from Pakistan, 1 from Bangladesh, 4 from sub-Saharan Africa) although all had lived in the UK for >3 years and one for 12 and another for 15 years.
Conclusions: IgE levels were surprisingly high in many patients with TB and also a significant number of contacts while eosinophilia was relatively rare. All those with positive serology had raised IgE levels while only 4/8 had an eosinophilia. IPs were common in patients with TB who had originated overseas. By their skewing of the immune system to a Th2 respose, intestinal parasites may increase susceptibility to active TB infection.
P164 EFFECT OF THE INTRODUCTION OF LIQUID CULTURE METHODS ON THE SPEED AND SENSITIVITY OF ISOLATION ON M TUBERCULOSIS: EAST LANCASHIRE 2002–05
R. Stephenson, M. Dunham, P. Maynard, I. Byrom, L. P. Ormerod. Departments of Respiratory Medicine and Bacteriology, Blackburn Royal Infirmary, Blackburn, Lancs BB2 3LR, UK
The tuberculosis culture method used in Blackburn was switched from the solid culture (LJ) method to automated liquid culture, by Becton Dickenson MGIT 960 machine, in May 2004. The effect of this change on the speed of isolation, and the proportion of cases culture confirmed, were assessed as follows. The time from receipt of the culture sample to first positive isolate was analysed, for all isolates of M tuberculosis for Blackburn patients by LJ slope from January 2002 to April 2004 inclusive, and for Blackburn patients May 2004–October 2004, and all East Lancashire patients (Blackburn + Burnley) November 2004–April 2005 inclusive by MGIT system. The sensitivity, or proportion of cases with a positive culture, was calculated for Blackburn patients only because of full clinical ascertainment of the numbers of cases with samples sent for TB culture at the Blackburn site.
Results: See table.
Abstract P164
The reductions in median time for isolation of M tuberculosis of 16.5 days for smear positive respiratory samples, 17.5 days for smear negative respiratory samples, and 10.5 days for non-respiratory samples, were all significant by the Mann-Whitney U test (p<0.0001; p = 0.0018; and p = 0.0007 respectively).
All microscopy positive sputum samples were culture confirmed by either LJ slope or MGIT. The proportion of TB patients with samples sent for TB culture culture confirmed was 12/26 (46%) of smear negative pulmonary cases by L-J slope and 6/8 (75%) by MGIT. The proportion of non-respiratory patients with samples sent for TB culture confirmed was 38/61 (62%) by L-J slope, and 18/25 (72%) by MGIT. The trend to increased sensitivity is not yet statistically significant due to small sample sizes.
The data show a highly significant statistical improvement in time to obtaining positive cultures. The sensitivity is also higher but not yet statistically significant. It is planned to widen the availability of TB liquid culture to other areas of Lancashire and South Cumbria following these results.
Thoracic surgery and pleural procedures
P165 CONTEMPORARY USE OF A PROSPECTIVE COMPUTERISED DATABASE IN THORACIC SURGERY: PATIENT AND PRACTICE MANAGEMENT ASPECTS
N. Chaudhuri, J. McShane, R. Grainger, A. D. Grayson, N. K. Mediratta, M. Carr, A. S. Soorae, R. D. Page. The Cardiothoracic Centre NHS Trust, Liverpool, UK
Objectives: The scientific value of a computerised database for collection of data is obvious. It is more difficult to establish the intangible management benefits. We decided to examine the patient and practice management aspects of our database.
Methods: In our institution a computerised database of patients undergoing thoracic surgery has been established for the purpose of prospective collection of data as part of clinical practice. As with any management information system the three characteristics of useful information—time, form, and content—were examined.
Results: 3786 patients underwent thoracic surgery between October 2001 and January 2005. The commonest use of our database is the generation of tabulated monthly practice and summary data for audit. A significant use of the database is the generation of statistical process control (SPC) charts to analyse postoperative mortality (fig 1), morbidity, length of stay, and intensive care requirements. The database allows audit of thoracic training. Data mining and evaluation using statistical techniques such as propensity scores enable us to compare alternative and novel practices to provide better patient care. We have also synchronised our database with the UK National Strategic Tracing Service to establish mid and long term survival in patients who undergo resection for lung cancer (fig 2).

SPC chart for mortality following lung resection.

Survival data following lung cancer resection.
Conclusions: A computerised database provides information useful in patient and surgical practice management. Linking patient data to national survival data allows live update of patient survival and could help us in producing risk stratification tools in future.
P166 HALF DECADE OF BIRMINGHAM’S EXPERIENCE IN LOOKING AT SURGICAL RESECTIONS ON PATIENTS WITH STAGE 111 NON-SMALL CELL LUNG CANCER FOLLOWING NEOADJUVANT THERAPY
P. S. Krishna Moorthy, R. Khan, J. F. Marzouk, P. B. Rajesh, F. J. Collin, R. Steyn, R. Vaughan. Department of Thoracic Surgery, Birmingham Heartlands Hospital, UK
Background: The role of surgery after neoadjuvant chemotherapy in patients with stage III especially 111B remain unclear and a tough task. However more clinical trials were performed all over the world showing some reasonable outcome for patients who were classified inoperable at some point of time. Therefore we are of sharing some of our experience at our unit in encountering this group of patients.
Methods: A retrospective study of 39 consecutive patients (20 patients (51%) in stage 111A and 19 patients (49%) in stage 111B) who were initially thought marginally resectable or inoperable of having a neoadjuvant chemotherapy/radiotherapy followed by surgery in Birmingham Heartlands Hospital (BHH) from January 2000 to June 2005.The demography, diagnosis, neoadjuvant therapy, and operative procedures were all documented. The endpoints were downstaging, complete resectability, 30 days mortality, complication, and survival.
Results: All 39 patients had neoadjuvant therapy (18 patients had at least one cycle of chemotherapy; one had radiotherapy only; 10 patients had both). 10 patients (26%) with complete, 28 (72%) with partial response, and one (2%) with stable disease, underwent surgery with no 30 days mortality. A radical resection was possible in 32 (82%) cases (9 lobetomies, 7 bilobectomies, 15 pneumonectomies, and 1 bronchoplastic resections were performed). Complications occurred in nine patients (23%). 30 patients who underwent surgery (77%) showed a pathologic downstaging. A complete pathologic response was obtained in seven (18%) cases. During the mean follow up of 22.6 months, local recurrence occurred in 5 (13%) and late deaths of 13 patients (33%). Nine (23%) patients died from cancer (both progression of non-resected cases and recurrence) and four (10%) from unrelated cause. Overall five year survival (Kaplan Meier) was 47%. Stage 111A has 54% survival but only 39% reaches in 111B (p = 0.222, log rank). Resected versus non-resected showed a significant difference: 58% versus 0% (p = 0.0009, log rank).
Conclusions: The trimodal approach for stage 111 NSCLC appears safe and effective. It provides good therapeutic results with acceptable morbidity in surgically resected cases.
P167 PREDICTORS OF EARLY DEATH FOLLOWING EXTRAPLEURAL PNEUMONECTOMY FOR MALIGNANT MESOTHELIOMA
J. G. Edwards, D. J. Stewart, A. E. Martin-Ucar, D. A. Waller. Glenfield Hospital, Groby Road, Leicester, UK
Aims: To evaluate the causes and predictors of non-tumour related death within four months of extrapleural pneumonectomy (EPP) for malignant mesothelioma (MM).
Methods: Prospectively collected data were analysed from 101 consecutive patients undergoing EPP. Variables retrieved included demographics, prognostic factors, pathological data, postoperative complications, and the causes of death. Binary logistic regression and χ2 analysis were used to identify predictors of 120 day mortality.
Results: Referrals were received from 28 cancer centres nationwide. EPP was performed in 101 patients. Six patients died in the surgical centre, four within 30 days. A further patient died following transfer to the referring hospital, before discharge (inhospital mortality 7%). Among those discharged home, at time points of one, two, three, and four months postoperatively, a further 3, 1, 3, and 4 had died. There were a total of 19 early deaths and a further 42 have died later than four months. At re-operation or postmortem, early disease recurrence was apparent in five (2.6) patients.
Predictors (with incidence among all patients) of early death included postoperative ITU admission (n = 19, p = 0.006), pneumonia (n = 11, p = 0.04), postoperative infection (n = 19, p = 0.04), cardiovascular complications (n = 30, p = 0.03), symptomatic mediastinal shift (n = 12, p = 0.04), and N1,2 disease (n = 45, p = 0.02). There was no association with operative experience (p = 0.76).
Conclusions: Early post-discharge care is the responsibility of the non-operating team. The potential remains for postoperative complications in this period. Patients, particularly those who right ventricular or respiratory failure, should be monitored closely in the community.
P168 CORRELATION OF RADIOLOGICAL AND PLEUROSCOPIC FINDINGS IN PATIENTS WITH HISTOLOGICALLY PROVEN MESOTHELIOMA
M. Ali, A. K. M. Cassim, M. S. Jakeways, A. G. Davison, D. Eraut, S. Ansari, K. Ganes Lingam. Southend Associate University Hospital, UK
Background: Diagnosis of malignant mesothelioma can sometimes be difficult. A negative percutaneous pleural biopsy and cytological results do not exclude mesothelioma. In our hospital surgical pleuroscopy is the next diagnostic procedure. In patients with a confirmed diagnosis of malignant mesothelioma surgical pleurodesis is also undertaken. Our aim was to look at the correlation between computed tomographic (CT) and pleuroscopic appearances in patients with malignant mesothelioma.
Methods: Over the last five years 49 pleuroscopic procedures were done. 13 out of 49 (26.5%) were diagnosed to have malignant epithelioid mesothelioma on surgical biopsy at pleuroscopy and case notes of these were reviewed. 77% were male and the mean age was 73.5 years. Data were collected for history of asbestos exposure, results of cytological examination of pleural fluid, blind percutaneous pleural biopsies, CT scan, and pleuroscopic and histopathological findings.
Results: Twelve patients had a CT scan of the thorax and all had pleural effusion. Pleural plaques were reported in one (8.3%), pleural thickening in three (25%), and pleural masses in two (16.6%). One (7.6%) had diagnosis confirmed on initial pleural fluid cytological examination. 10 had blind percutaneous pleural biopsy and results for these were suggestive (not diagnostic) of malignancy in three (30%). Macroscopically at pleuroscopy tumour deposits were seen in seven (53.8%), pleural thickening in two (15.3%), pleural plaques in one (7.6%), pleural thickening and tumour in one (7.6%), pleural plaque and tumour in one (7.6%), and pleural plaques and thickening in one (7.6%). Of nine with tumour deposits on pleuroscopy, six (66.6%) did not have any pleural change on CT scan other than pleural effusion.
Conclusion: These data show that both the macroscopic appearances of pleuroscopy and CT scan are not reliable in diagnosing mesothelioma. 61.5% of CT scans in patients with a final histological diagnosis of mesothelioma showed no pleural change other than an effusion. Of these in only 62.5% were there definite macroscopic appearances of tumour at pleuroscopy. This study highlights the importance of pleuroscopic biopsy when a diagnosis of mesothelioma is suspected.
P169 APPROPRIATENESS OF VIDEO ASSISTED THORACOSCOPIC SURGERY VERSUS BEDSIDE TALC SLURRY PLEURODESIS IN PATIENTS DYING OF CANCER: JUDGEMENTS OF AN EXPERT PANEL PROCESS
C. Tan1, T. Treasure1, J. Browne2, M. Utley3, C. W. H. Davies4, H. Hemingway3. 1Guy’s Hospital, London; 2Royal College of Surgeons of England, London; 3University College London, London; 4Royal Berkshire and Battle Hospitals, Reading, UK
Objectives: The UK Thoracic Surgery Register records over 1000 video assisted thoracoscopic (VATS) talc pleurodeses annually for malignant effusions. We have evidence of effectiveness from our systematic review of randomised trials and a recently reported Cochrane review, but some patients derive no benefit and are exposed to the risk of an unavailing invasive procedure. A consensus on appropriateness seemed to be timely.
Methods: The RAND/UCLA Appropriateness Method (RAM) exemplified in the UK study of coronary interventions (
) was developed in the 1980s to assess over or underuse of procedures. Our panel, chaired by a RAM expert, comprised three respiratory physicians, three thoracic surgeons, and two oncologists. Factors considered include: anticipated survival, known/unknown tissue diagnosis, dyspnoea score, response to trial aspiration, evidence of trapped lung, and radiological evidence of pleural thickening. This yields 300 permutations. To test each set by randomised trials would be impossible. The panel was asked to rate the appropriateness of both VATS talc pleurodesis and bedside talc slurry for each permutation.
Results: The longer the expected survival the more appropriate was either intervention. When the tissue diagnosis was unknown VATS was rated appropriate in 58% of scenarios, uncertain in 24%, and inappropriate in 18% compared with bedside talc slurry where it was never rated appropriate, uncertain in 7%, and inappropriate in 93%. Even where there was a good response to trial aspiration, pleurodesis by VATS was only judged appropriate by VATS in 50% of cases and by bedside slurry in 26%. Paradoxically pleurodesis was rated to be increasingly appropriate with less breathlessness.
Conclusions: Although some of the conclusions had face validity, there were serious incongruities. For instance the worse the dyspnoea the less likely the physicians were to recommend VATS, while the surgeons judged severe breathlessness to be an indication to intervene. While the outcome was sometimes flawed, the process was revealing in exploring and making explicit the preconceptions, thought processes, and value judgments that we see employed in the lung cancer MDT.
P170 THE IMPACT OF A SPECIALISED PLEURAL PROCEDURES LIST ON DIAGNOSTIC RATES OF BLIND PERCUTANEOUS PLEURAL BIOPSIES: THE END OF THE ABRAMS NEEDLE?
N. Khalil, S. Ambalavanan, J. F. Miles. North Manchester General Hospital, UK
Introduction and Objective: Blind percutaneous pleural biopsies have a limited role in the investigation of unilateral pleural effusions due to its low diagnostic yield compared to CT or thoracoscopic methods, with the possible exception of tuberculosis (TB).1–3 In North Manchester General Hospital (NMGH), a specialised pleural biopsy service was set up, which allowed all biopsies to be done in the day services unit, by experienced operators, using ultrasound guidance to identify fluid. We have audited the yield of this service to see whether the specialised pleural service has improved the quality of pleural specimens obtained and the diagnostic biopsy rate.
Methods: A retrospective analysis was carried out of all patients who had undergone blind percutaneous biopsies (Abrams) between 18/02/04 and 18/02/05 (one year). In total, 32 blind pleural biopsies were performed during this period. Data were collected using the NMGH lung cancer database, histology reports, x ray reports, and clinic letters.
Results: The inadequacy rate for blind percutaneous pleural biopsies received by the lab was only 12% (in comparison to 23% in an audit in NMGH looking at sample adequacy). Diagnosis was confirmed in 47% of patients (13% mesothelioma, 59% metastatic carcinoma, 7% TB, 21% chronic inflammation). Diagnosis was suspected, but needed substantiation by further procedure in 16% (60% mesolthelioma, 40% metastatic carcinoma) of patients. No diagnosis was made based on pleural biopsies alone in 37% (eventual diagnosis: 25% mesothelioma, 17% metastatic carcinoma, 17% inflammatory effusion, 8% sarcoidosis, and 33% had no diagnosis made) of patients.
Conclusion: A dedicated specialist pleural service has improved the quality of pleural specimens obtained. However, diagnostic rates with Abrams remain low and the persistence in the use of non-CT guided or non-thoracoscopic methods cannot be justified further unless a diagnosis of TB is suspected.
1
2
3
P171 MANAGEMENT OF PRIMARY AND SECONDARY SPONTANEOUS PNEUMOTHORAX
P. S. Borade, C. I. D. Ludwig, D. K. C. Lee, D. A. Promnitz. Department of Respiratory Medicine, Ipswich Hospital, Heath Road, Ipswich IP4 5PD, UK
Background: There is paucity of data with regards to the management of primary and secondary spontaneous pneumothorax.
Methods: A study was conducted to evaluate whether patients with either primary or secondary spontaneous pneumothorax were managed according to current British Thoracic Society guidelines.
Results: 56 consecutive patients with spontaneous pneumothorax were assessed over a 12 month period. In patients with primary spontaneous pneumothorax, 84% were inappropriately managed with intercostal drain insertion. 79% of these patients merely required simple aspiration and 5% warranted observation alone. For patients with secondary spontaneous pneumothorax, 50% were incorrectly managed with simple aspiration when intercostal drain insertion was required. Complications occurred in 32% of patients who had intercostal drain insertion. 77% and 85% of patients with primary and secondary spontaneous pneumothorax respectively were referred to a chest physician regardless of outcome. The mean hospital stay for patients with primary and secondary spontaneous pneumothorax was 4 and 22 days respectively.
Conclusion: The vast majority of patients with primary spontaneous pneumothorax were needlessly exposed to intercostal drain insertion. Implementation of the British Thoracic Society guidelines is crucial in order to avoid unnecessary patient discomfort and procedure related complications. It should also reduce the number of inappropriate referrals to a chest physician.
P172 MANAGEMENT WITH CHEST DRAIN: A REGIONAL SURVEY
F. Akbar1, A. J. Leonard2. 1Southampton University Hospitals, Southampton; 2Great Western Hospital Swindon, UK
Background: Chest drains may be urgently required when managing patients with pneumothorax and pleural infections. Available guidelines are not always followed.1
Objective: We sought to determine the familiarity of Accident & Emergency (A&E) and general medical registrars with the knowledge base underlying the use of chest drains in acute situations.
Methodology: A questionnaire was posted to all registrars involved in emergency medical admissions in Wessex and Southwest regions. It contained two clinical scenarios; that of a pneumothorax in a breathless chronic obstructive pulmonary disease (COPD) patient with lung deflated halfway between chest wall and hilum, and a patient with a parapneumonic effusion of pH 7.1. The ideal answer to each question could be determined from current BTS guidelines. The results were analysed according to specialty (respiratory, R v non-respiratory, NR). NR registrars were further subdivided according to experience in placing intercostal drains (>20 v <20 drains inserted).
Results: The response rate was 47.9% (139/290). Gastroenterology and endocrine registrars (30%) were underrepresented compared to those in all other specialties.
75% (21/28) of R but only 45% (50/110) NR would insert a drain as initial management of the pneumothorax (p = 0.005). 89% of all respondents chose for this case a small bore drain (£ 12 Fr) with no difference according to specialty or experience. 82% R and 63% NR (excluding A&E) would remove the drain when bubbling had ceased but was still swinging; 17% (14% R v 18% NR) would wait until swinging had stopped too, and 13% NR would remove the drain even if bubbling providing the chest x ray showed an inflated lung. For the empyema, all R but only 70% NR would insert a drain as initial treatment (p = 0.003). There was greater reluctance to use small bore drains in this case compared to the pneumothorax; R selected ⩽12 Fr drains more frequently than NR (67% v 40 %, p = 0.014). NR who had an experience of >20 chest drains chose to insert a drain more frequently in both cases than their less experienced counterparts, who frequently replied that they would wait for a respiratory opinion. 75% of all respondents had learnt the procedure under supervision and only 55% had had formal teaching in chest drains.
Conclusion: Standard practice varies between R and NR registrars, but even the former did not apply current guidelines uniformly well. Learning programmes should be introduced more actively in the initial part of SpR training. Guidelines need more vigorous dissemination among non-respiratory specialties.
1
P173 PNEUMOTHORAX AND THE VALUE OF POST THORACOCENTHESIS RADIOGRAPHY IN A WARD SETTING
J. Singh, K. S. Srinivasan, H. Moudgil. Respiratory Medical Unit, Princess Royal Hospital, Apley Castle, Telford TF1 6TF, UK
Background: Although the possibility of iatrogenic pneumothorax remains a complication following thoracocenthesis, the need for routine post-procedure chest radiology is often being questioned and even more so as the subsequent intervention rates are also small. Data quoting rates of between 3% to 20% (
) are, however, more specific to image guided techniques for differing indications with little on morbidity associated with more commonly based ward procedures. We have presently audited our practices.
Methods: Over a one year period to end 2004, 131 procedures were undertaken on 121 patients (10 repeated samples); of these, 105 underwent pleural aspiration and 16 were combined with closed pleural biopsy. Two procedures were guided by CT and one using ultrasound. All images were reviewed on the hospital picture archive (PACS) systems.
Results: Follow up radiology was undertaken after 109 (83%) of procedures; after 93 (71%) this was within 24 hours but thereafter after 24 hours (n = 12), 48 hours (n = 1), or beyond 72 hours (n = 3). Where known from follow up films, 11/109 (10%) patients had a radiologically detectable pneumothorax; two of these were among the 17 patients who required chest drain insertion for therapeutic drainage. Of those who underwent closed pleural biopsy only one had a pneumothorax but in a further three no subsequent chest radiograph was undertaken. Overall length of stay was at mean 9.15 days (range 0–82) with as anticipated, longer stay for patients requiring chest drains than those who underwent aspiration alone (mean 13.9 v 8.4 days).
Conclusions: This audit (1) describes the distribution of ward based pleural investigation, (2) reports the heterogeneity in post procedure attitude to chest radiology to exclude complicating pneumothorax, (3) documents an absolute pneumothorax complication rate of at least 10%, and (4) identifies significant morbidity with both prolonged hospital stay and requirement for chest drain insertion.
P174 THE ROLE OF “BLIND” TRUCUT PLEURAL BIOPSY IN THE INVESTIGATION OF AN EXUDATIVE PLEURAL EFFUSION
H. Singh, J. Blaikley, L. P. Ormerod. Chest Clinic, Department of Medicine, Blackburn Royal Infirmary, Infirmary Road, Blackburn, UK
Background: The role of blind pleural biopsy has been under question in recent times with excellent results being shown for radiologically guided procedures which are resource limited. Traditionally blind biopsies are peformed by Abrams needles and the yield as reported in a randomised control trial was 8 out of 17 patients. (
) The same trial showed that the yield of CT guided cutting needle pleural biopsy was 13/15 patients.
Abstract P174
Methods: We present the results of 27 consecutive procedures in patients with an exudative pleural effusion, performed over 12 months. These were done by using 16–18 G trucut needle in a standard way as used by the radiologists, but without any radiological guidance, except a chest radiograph and pleural aspiration before the procedure to confirm the presence of fluid. Three to five passes were made with the needle and patients had a pleural drain was put in at the end of procedure if needed.
Results: Out of 27 patients, pleural tissue was obtained in 22 (81%). The fluid cytology and microbiology did make a final diagnosis in seven (25%) out of 27 but the pleural biopsy histology helped to make a final diagnosis in 22 (81%) out of 27 patients. It was deemed to be inadequate in five out of 22 cases. There were no complications.
Conclusions: “Blind” trucut pleural biopsy is a safe and effective procedure and its yield is comparable to the abram’s needle. It is a relatively easier and less traumatic procedure than the latter in our experience.
P175 IS THE INITIAL FEASIBILITY OF LOBAR LUNG VOLUME REDUCTION SURGERY IN STAGE I NON-SMALL CELL LUNG CANCER JUSTIFIED BY LONG TERM SURVIVAL?
A. E. Martin-Ucar, K. R. Fareed, A. Nakas, J. E. Pilling, J. G. Edwards, K. J. West, D. A. Waller. Department of Thoracic Surgery, Glenfield Hospital, Leicester, UK
Background: Previous published work in our unit confirmed the feasibility of performing lobar lung volume reduction surgery (lobar LVRS): a standard lobectomy in patients with lung carcinoma and severe emphysema of apical distribution whose respiratory reserve is outside operability guidelines. We aim to determine whether this approach is justified by long term survival.
Methods: Since April 1997 to March 2005 a single surgeon performed upper lobectomy for stage I non-small cell lung cancer (NSCLC) on 118 patients. Perioperative course and survival of the 27 cases (23%) with severe heterogeneous emphysema of apical distribution and a predicted postoperative FEV1 (PpoFEV1) of less than 40% were compared to the remaining 91 cases (77%) with a PpoFEV1 greater than 40%.
Results: Hospital mortality and stay were similar between the two groups. Survival after lobar LVRS in stage I NSCLC was worse than in the group without concomitant severe emphysema, although rates of tumour recurrence were similar.
Discussion: Survival after lobar LVRS for stage I lung cancer is affected by death without evidence of cancer recurrence. However, outcomes are still better than reported after any other modality of treatment. The long term results justify earlier reports of the feasibility of this aggressive approach in these high risk cases.
Abstract P175
P176 LUNG VOLUME REDUCTION SURGERY FOR EMPHYSEMA: LESSONS LEARNT FROM THE FIRST 100 CASES IN A SINGLE INSTITUTION
P. Vaughan, I. F. Oey, M. D. L. Morgan, T. J. Spyt, D. A. Waller. Glenfield Hospital, UK
Objectives: It is 10 years since the introduction of lung volume reduction surgery (LVRS) in our unit. We have performed over 100 procedures, and therefore sought to evaluate our practice.
Methods: Data expressed as median (range). Since 1995, prospective data have been collected on 106 consecutive procedures. Sex distribution was 62% male; age 59 (39–73) years. 10% of patients were α-1-antitrypsin deficient. 8% had lower lobe surgery. Two surgeons performed all procedures using buttressed stapled lung resection either via sternotomy or video assisted thoracoscopic surgery (VATS) following a period of pulmonary rehabilitation. Five patients underwent staged bilateral LVRS. Changes in physiological and nutritional parameters have been calculated.
Results: Surgery has been performed on 27% of referrals. Preoperative demographics and physiological parameters have not altered significantly with experience. LVRS was performed by VATS in 80% of patients and was unilateral in 76%. Our 30 day mortality is 4%; 90 day mortality is 8%. Patients remain in hospital for 15 (5–111) days with median air leak duration of 10 (1–71) days. Postoperatively, maximum improvement in FEV1 of 25% occurs at three months with a significant increase for up to 12 months (p<0.05). RV:TLC ratio was maximally reduced by 9% at 3 months and BMI maximally improved by 1.1 kg/m2 at two years. Both remain significantly improved for two years (p<0.01 respectively). When split into four cohorts according to operation date, there has been a significant reduction in operating time to 75 (40–150) minutes (p = 0.001), the number of bilateral operations performed (p<0.001), and number of patients admitted to ITU of 8% (p<0.001).
Conclusions: LVRS can be performed in selected patients with acceptable mortality and morbidity, which is subject to a learning curve effect. We now favour staged unilateral VATS. The physiological outcome however is not uniform and further refinement of selection is required.
P177 MEDIUM TERM FOLLOW UP AFTER DEPLOYMENT OF ULTRAFLEX EXPANDABLE METALLIC STENTS TO MANAGE ENDOBRONCHIAL PATHOLOGY
J. E. S. Park, A. Sheth, B. P. Madden. Department of Cardiothoracic Medicine, St George’s Hospital, London, UK
Between March 1997 and March 2004 we deployed 80 Ultraflex metallic expandable stents (Boston Scientific, Waterson, MA, USA) in 69 patients under direct vision using rigid bronchoscopy. To date 15 patients have been followed for more than one year (median 41 months, range 12–83 months). Indications for stenting in these patients were neoplasia (5), stricture (5), airway malacia (1) iatrogenic tracheal tear (1) and compression from an aortic aneurysm (1), a right interrupted aortic arch (1), and a right brachiocephalic artery aneurysm with tracheo-malacia (1) (see table). Ten tracheal stents (9 covered, 1 uncovered) and 10 bronchial stents (8 uncovered, 2 covered) were inserted and five patients received two stents.
Abstract P177 Number of patients stented at more than one year follow up by diagnostic category and specific diagnosis
Complications included troublesome halitosis (5) which was difficult to treat despite of various antibiotic regimes; granulation tissue formation above and below the stent which was successfully treated with low power Nd Yag laser (7), and metal fatigue (1). We did not encounter stent migration.
We conclude that ultraflex expandable metallic stents have an important role in the management of selected patients with diverse endobronchial pathologies and are well tolerated in the long term. Although associated granulation tissue can be successfully treated with Nd Yag laser, halitosis can be a difficult problem to address.
Cough
P178 PREDICTORS OF IDIOPATHIC COUGH: OUTCOME OF A RETROSPECTIVE ANALYSIS
L. Polley1, C. Cardwell2, R. Costello3, L. P. A. McGarvey1. 1Regional Respiratory Centre, Belfast City Hospital, N Ireland; 2Department of Epidemiology and Public Health, Queen’s University of Belfast; 3Department of Medicine, RCSI, Beaumont Hospital, Dublin
Background: Protocols for evaluating cough at specialist centres are well established and the majority of patients benefit from the process.1 However, there is a subgroup of patients in which no cause for cough can be identified. These idiopathic coughers (IC) represent a difficult clinical challenge and factors predictive of the condition would be helpful. It has previously been suggested that this group often consists of perimenopausal females2 and patients who more frequently report preceding upper respiratory tract infections (URTI).3
Methods: We undertook a retrospective analysis of the hospital notes of 241 sequential referrals (71.4% female, median age 58 years, median cough duration 36 months) to Belfast City Hospital’s specialist cough clinic over eight years. Subjects were identified as either IC or successfully treated cough (TC). Independent samples t tests, χ2 tests, and logistic regression analysis were used to compare characteristics of IC and TC patients.
Results: Forty three (17.8%) patients were excluded from the analysis as diagnostic evaluation was ongoing. TC was confirmed in 170 (70.5%) patients. Diagnostic categories were as follows; gastro-oesophageal reflux disease (32.4%), asthma (25.3%), post-nasal drip syndromes (17.8%), eosinophilic bronchitis (6.2%), post-viral cough (8.8%), and other (13.3%). IC was diagnosed in 28 (11.6%) patients. Females were significantly more likely to have IC (OR 3.57 (1.03 to 12.3), p = 0.05). The odds of IC was significantly increased in patients with cough duration >4 years compared to those <4 years, (OR 7.0 (2.3 to 21.1). No significant relationship was found between IC and age, height, weight, BMI, referral source, or preceding URTI. Subjects with IC had higher scores in the physical domain of the Leicester Cough Questionnaire (p = 0.009), with no difference in other quality of life measurements. Patients with both raised immunoglobulin E and positive RAST (n = 12) all improved, independent of corticosteroid therapy (p = 0.009, Fisher’s exact test)
Conclusion: Female gender and cough duration at presentation are significantly associated with increasing likelihood of having idiopathic cough. However we have found no such association with age or preceding URTI.
1
2
3
P179 OPIATE THERAPY IN CHRONIC INTRACTABLE COUGH
J. Jackson, C. Wright, M. Menon, A. H. Morice. Academic Division of Respiratory Medicine, University of Hull, UK
Introduction: Despite frequent recommendations of benefit (
,
) there is no randomised control trial describing the effect of opiates in chronic cough (CC).
Aim: We tested the hypothesis that opiates in the form of slow release morphine (MST) 5 mg bd produce a reduction in cough frequency and severity in patients with CC resistant to diagnosis and treatment.
Method: 27 patients (18 female) with CC resistant to treatment, with mean age 58.3 (SD 10.6) were randomised into a double blind, placebo controlled, crossover study. Treatment period of four weeks was compared with the four week matched placebo. Objective and subjective measures of cough reflex sensitivity were captured. Patients were required to complete a daily diary record of cough score, using a visual analogue scale of 0–9 to indicate the severity and frequency of their cough. The change in cough score was the primary end point for the study. In addition, study visit assessments included the citric acid, concentration response cough challenge using the Mefar dosimeter and the Leicester Quality of Life Questionnaire (QOL).
Results: Using the paired t test, diary data analysis showed a highly significant (p<0.0001) reduction in cough score during the treatment phase mean 3.44 (SD 1.75) compared with placebo 4.97 (SD 1.68). A significant (p<0.002) improvement in the QOL score was also observed when compared with placebo 4.57 (SD 0.84) with MST treatment 5.22 (SD 0.89). However, there was no significant difference between C2 (concentration of citric acid eliciting and average of two coughs/inhalation) for placebo geometric mean 63.09 (SD 3.75) compared with that of the treatment period 81.21 (SD 4.14).
Discussion: The two subjective assessments demonstrate a change in the severity and frequency of cough. Low dose morphine MST is a clinically effective suppressant of cough. The failure to demonstrate a significant difference in C2 calls into question the use of cough challenge in assessment of clinical response.
P180 DETERMINING THE OPTIMUM DOSE OF SLOW RELEASE MORPHINE TO TREAT CHRONIC INTRACTABLE COUGH: OBSERVATIONAL STUDY
C. E. Wright, J. Jackson, M. Menon, A. H. Morice. University of Hull, Academic Department of Medicine, Castle Hill Hospital, Cottingham HU16 5JQ, UK
Introduction: We have previously shown that a one month treatment with 5 mg slow release morphine (MST) significantly improved subjective measures of cough symptoms in patients with intractable cough.
Aim: To determine whether extended MST treatment continues to be effective in relieving symptoms of cough.
Method: Following a core crossover study of 5 mg MST versus placebo in the treatment of intractable cough 18 subjects (female (8), mean age 56 (SD 10) years) out of 27 continued taking MST for a further three months. During this three month period patients were given the choice to double the dose of MST to 10 mg if they felt their cough symptoms were not under control. Cough symptoms were scored in a daily diary record.
Results: Of the 18 subjects initially taking part 33% increased dose of MST to 10 mg in the first month thus at end of the core study, a further 11% increased to 10 mg in month 2 and at month 3 a further 22% increased to 10 mg making a total of 66% of the patient population taking 10 mg MST by the end of the extension study. Those patients increasing dose to 10 mg at the beginning of this extension study had a mean reduction in cough severity in the core study of 0.75 (SD 1.0) as compared to 2.4 (SD 1.5) in those continuing at 5 mg. By three months the cough symptom scores were similar for both 5 mg and 10 mg groups of 2.09 (SD 1.1) and 2.92 (SD 2.0) respectively. Side effect profile was similar for both 5 mg and 10 mg MST however in the 10 mg group there was a double the incidence of drowsiness.
Conclusion: Treatment with 5 mg MST seems to be suboptimal in 66% of patients studied. 10 mg MST was the optimum treatment with a side effect profile similar to that of 5 mg MST. Continuous administration of opiates can result in intolerance, however in this study cough intensity appeared to play the major role in dose escalation.
P181 ANALYSIS OF COUGH REFLEX SENSITIVITY DATA
B. Prudon, D. D. Vara, I. D. Pavord, S. S. Birring. Institute for Lung Health, Department of Respiratory Medicine, Glenfield Hospital, Leicester, UK
Assessment of cough reflex sensitivity is widely performed in the research setting. Inhaled capsaicin is the most widely used tussive agent that is usually administered in doubling dose increments. Cough sensitivity is commonly expressed as C2 and C5; the concentration of capsaicin that causes 2 and 5 coughs respectively. There is no consensus on the best method to calculate C2 and C5. We compared two commonly used methods to express C2 and C5 in 134 healthy subjects and 36 patients with isolated chronic cough who underwent cough reflex testing using a Koko Digidoser with an inspiratory flow regulator valve. C2 and C5 were determined by the first administered concentration that resulted in 32 and 35 coughs respectively and by interpolation of log transformed data. 15 healthy subjects and 15 patients with chronic cough also had repeat capsaicin cough reflex sensitivity measurement after two weeks. Both C2 and C5 were higher when expressed as the first administered concentration compared to interpolated values (geometric mean C2 (mmol/l): 13.8 and 10.9 respectively; mean difference 0.3 doubling doses; p<0.001; C5: 46.8 and 40.8 mmol/l; mean difference 0.2 dd; p<0.001.) There were similar differences between first administered concentration and interpolated C2 and C5 when the data for healthy subjects and patients with chronic cough were analysed separately. Both methods for determining C2 and C5 correlated highly (C2: r = 0.97; C5: r = 0.99, p<0.001) and were highly repeatable (intraclass correlation coefficients >0.9). We have shown there are minor differences in C2 and C5 when expressed as first administered concentrations or when calculated by interpolation. Interpolated concentrations are closer to the real C2/5 but they offer no particular advantage over first administered concentration. Standardisation of cough reflex testing and expression of data are required similar to other challenge tests such as methacholine bronchoprovocation.
P182 AMBULATORY PH MONITORING IS IMPORTANT IN THE DIAGNOSIS AND TREATMENT OF DRY COUGH DUE TO GASTRO-OESOPHAGEAL REFLUX DISEASE
D. McIntosh, A. Stanton, N. Rajoriya, C. McKenzie, S. Thomson, S. McLaren, J. F. MacKenzie, C. E. Bucknall. Department of Respiratory Medicine, Stobhill Hospital and Departments of Respiratory Medicine, Clinical Effectiveness & Gastroenterology, Glasgow Royal Infirmary, Glasgow, UK
Gastro-oesophageal reflux disease (GORD) is recognised as an important cause of dry cough and investigation algorithms commonly include either an empirical trail of treatment or pH study to assess this. We have included this in our investigation protocol for some time and report preliminary results, which will be complete for a larger cohort by the time of the Winter meeting.
Patients with dry cough, who have normal chest examination, CXR, and PFTs, commonly undergo ENT examination, histamine challenge for PC20 assessment, and pH study as part of a standard investigation protocol; they receive an empirical trail of therapy during the period of investigation, if there is a reasonable clinical suspicion of the main cause of their cough (nasal or inhaled corticosteroids or standard doses of PPI).
14 patients have been investigated with pH studies so far. Average age of these patients is 56 (SD 17) years, range 27–82 years; nine females. The results of these patients’ investigations are as follows:
-
five patients with positive studies, and improved cough with abolition of reflux—three patients on 20 mg PPI, two patients on 40 mg PPI
-
three patients with positive studies and incomplete abolition of reflux—one declines further study and on empirical Rx, one lost to follow up, one on 40 mg BD
-
six patients with negative studies, one of whom reports ongoing heartburn, in whom non-acid reflux may be occurring
Eight of 14 (57%) of patients investigated have GORD documented. Of the six patients with initially abnormal and repeat pH study data, three have required more than standard doses of PPI to reduce (n = 1) or abolish (n = 2) abnormal oesophageal acid exposure. These preliminary data suggest that diagnostic and therapeutic monitoring pH studies are essential in the management of dry cough, since lack of response to an empirical trial of therapy is difficult to interprete. If all 14 of these patients had been managed empirically, only three could have been expected to have a response, but five would have had GORD wrongly discarded as a diagnosis and six would have had an unnecessary trial of therapy.
P183 DEXBROMPHENIRAMINE MALEATE INHIBITS CAPSAICIN AND RESINIFERATOXIN ACTIVATION OF TRPV1
L. R. Sadofsky, S. J. Compton, A. H. Morice. Respiratory Medicine, Division of Academic Medicine, The Postgraduate Medical Institute in Association with the Hull York Medical School, University of Hull, UK
There is growing evidence to suggest that the capsaicin receptor, TRPV1 is one of the primary sensory receptors for cough. This cation channel responds to stimulation by capsaicin, resiniferatoxin, and protons, by causing sensory nerve depolarisation. In cough variant asthma and eosinophilic bronchitis, histamine levels are increased, and we therefore sought to determine whether histamine activates TRPV1 and whether antihistamines could antagonise TRPV1 responses to capsaicin and resiniferatoxin.
Rat TRPV1 (rTPRV1) was cloned from rat dorsal root ganglia cDNA and human TRPV1 (hTRPV1) was cloned from MRC5 cDNA. Both were permanently expressed in human embryonic kidney cells (HEK293, rTRPV1-HEK, and hTRPV1-HEK). To assess the activation of TRPV1 by capsaicin and resiniferatoxin, the cells were loaded with the fluorescent calcium binding probe, fluo-3, and increases in intracellular calcium levels were measured using a Photon Technology Quantamaster Fluorospectrophotometer.
rTRPV1-HEK was activated by capsaicin and resiniferatoxin in a concentration dependent manner with EC50 values of 424 nM and 0.1 nM respectively. hTRPV1-HEK also responded to capsaicin and resiniferatoxin in a concentration dependent manner with EC50 values of 5.5 nM and 0.8 nM respectively. Following preincubation with the antihistamine dexbrompheniramine maleate (100 μM and 1 mM), both the capsaicin and resiniferatoxin concentration effect curves for rTRPV1 and hTRPV1 displayed a rightward shift and reduction in maximum response. Preincubation of rTRPV1-HEK, with dexbrompheniramine maleate (100 mM), right shifted the concentration effect curves for capsaicin and resiniferatoxin with EC50 values rising to 762 nM and 2.5 nM respectively. For hTRPV1-HEK in the presence of dexbrompheniramine maleate (100 μM & 1 mM) the EC50 values for the capsaicin concentration effect curves rose to 13.8 nM and 12.9 nM respectively. Preincubation of hTRPV1-HEK with another antihistamine, diphenhydramine hydrochloride (100 μM and 1 mM) also caused a reduction in the maximum response to capsaicin and an increase in EC50 values to 3.1 nM and 1.8 nM respectively. hTRPV1-HEK and pcDNA3-HEK both responded similarly to histamine in a concentration dependent manner. Finally no additive effect was observed between histamine (30 mM) and capsaicin.
Conclusion: Preincubation of hTRPV1-HEK and rTRPV1-HEK cells with dexbrompheniramine maleate inhibits capsaicin and resiniferatoxin activation of TRPV1 in our cell system.
Investigations
P184 THE IMPACT OF PICTURE ARCHIVING AND COMMUNICATION SYSTEMS UPON THE REVIEW AND REPORTING OF CHEST RADIOGRAPHS ON INTENSIVE CARE UNITS IN ENGLAND AND WALES
B. Esdaile1, A. Pillai1,2, C. Mehta1, T. Evans2, N. Soni1, S. Singh1. 1Chelsea & Westminster Hospital, London SW10 9NH, UK; 2The Royal Brompton Hospital, Sydney Street, London SW3 6NP, UK
Objective: In light of the proposed implementation of the national programme for information technology (NPfIT) within the NHS, this study was designed to assess (1) the prevalence of PACS (Picture Archiving and Communication System) on intensive care units (ICU) in England and Wales, and (2) the impact of PACS on (a) the speed of image availability and (b) the frequency of on-unit reporting by radiologists. We also audited two ICUs, one with and the other without PACS, to determine chest radiograph (x ray) request-to-review times.
Design and Methods: (1) A prospective telephone survey of Adult ICUs in England and Wales. Senior staff at 226 ICUs were questioned on PACS availability, the prevalence of usage of hard copy x rays, how often on-unit radiology reporting took place, and on the times between x ray request and acquisition. (2) An audit of x ray request-to-review times, in one ICU (No PACS) over a six month period, and another ICU with PACS over three months.
Results: 34% (77/226) of ICUs had PACS. Of these, 87% (67/77) had their x ray images available within an hour of request. 55% (42/77) of ICUs with PACS did not have hardcopy x rays. Only 12% (9/77) of ICUs with PACS had on-unit radiology reporting compared with 23% (35/149) of ICUs without PACS. An 89 day audit of an ICU without PACS revealed a mean Request-to-review time by the ICU team of 4 hours 39 minutes. On 48 out of 89 occasions, the x rays were reported directly in the Radiology department jointly with ICU. In the 58 day audit of an ICU with PACS, the Request-to-review time was 1 hour 47 minutes, always jointly reported on-site.
Conclusions: PACS is already present in about one third of ICUs in England and Wales. It reduces radiograph hardcopies on ICUs and shortens the x ray request-to-availability time to <1 hour in most cases. PACS reduces x ray request-to-review times 2.5-fold. This may prevent delays in x ray guided decisions of clinical management. The presence of PACS is associated with less on-site ICU radiologist reporting. This may save time for radiologists and intensive care clinicians, but potentially reduce a multidisciplinary approach to x ray assessment on the ICU.
P185 UTILITY OF ROUTINE CHEST X RAY AFTER UNCOMPLICATED TRANSBRONCHIAL LUNG BIOPSY IN DIAGNOSIS OF PNEUMOTHORAX IN CASES OF DIFFUSE PARENCHYMAL LUNG DISEASE
T. S. Jordan, R. K. Kedia, M. Winson, K. V. Alexander, A. Kumarswami. Mid Cheshire Hospitals NHS Trust, Leighton Hospital, Middlewich Road, Crewe, Cheshire CW1 4QJ, UK
Introduction: Transbronchial lung biopsy (TBLB) under fluoroscopy guidance improves the diagnostic yield and reduces the risk of pneumothorax in cases of diffuse parenchymal (DPLD) and solitary pulmonary nodules (
). The incidence of pneumothorax following TBLB is estimated to be <4%. In previous retrospective studies of clinical notes, routine post-procedure chest x rays was of limited clinical value in diagnosis of pneumothorax. We undertook a prospective study to evaluate the utility of routine post-procedure chest x ray following TBLB.
Method: Patients with suspected DPLD had TBLB under fluoroscopy. On average, four biopsies were taken from the affected lobe. Patients were asked to report any pleuritic chest pain or shortness of breath during or immediately after the procedure. Patients were lying in a supine position with the head elevated by six inches. The bronchoscope was passed through either the mouth or transnasally with the operator standing in front of the patient. At the end of the procedure, fluoroscopic screening for pneumothorax on the side the of the biopsy was performed. All patients underwent a chest x ray (PA view, expiratory) 90 minutes after the procedure to rule out pneumothorax.
Results: Of the 36 patients (male:16) in the study, none of them reported any pleuritic chest pain or shortness of breath during or immediately after TBLB. None of these patients was found to have a pneumothorax on either fluoroscopy immediately after the procedure or on expiratory chest x ray 90 minutes following TBLB.
Conclusion: Patients that are asymptomatic during and immediately after TBLB and who, on fluoroscopic screening immediately after the procedure are not found to have a pneumothorax, do not require a routine post procedure chest x ray and can be discharged home directly from the bronchoscopy suite.
P186 SHOULD BRONCHOSCOPY BE THE INITIAL INVESTIGATION IN PATIENTS PRESENTING WITH HAEMOPTYSIS AND AN ABNORMAL CHEST X RAY?
R. A. Heinink, S. Ashenford, J. Singh, H. Moudgil, K. S. Srinivasan. Department of Respiratory Medicine, Princess Royal Hospital, Telford, UK
Background: It has been suggested that performing computed tomography (CT) as the initial investigation in patients with haemoptysis can avoid unnecessary fibreoptic bronchoscopy (FOB). Several studies have shown this to be true in patients with normal chest x ray (CXR), but it is not as clear as to whether this is also true for patient’s with abnormal CXR.
Aim: To assess whether FOB should be the initial investigation in patients presenting with haemoptysis and an abnormal CXR.
Method: A retrospective study of 70 patients who had FOB for investigation of haemoptysis with an abnormal CXR was performed. CT scan results, FOB findings, FOB sampling results, and final diagnosis were recorded.
Results: Mean age of patients was 62 (range 20–84); males 44 (63%). If the “probable cancer” and “possible cancer” groups are combined as a positive result, then the sensitivity in our study of CT selecting those patients with cancer is 100%, with a specificity of 87%.
Conclusion: Our study suggests that thoracic CT imaging performed as an initial investigation in patients with haemoptysis and an abnormal CXR has a high sensitivity and specificity in selecting those patients with cancer. It may avoid unnecessary FOB and also gives specific diagnosis of benign conditions as a cause for haemoptysis in those without cancer. This is in keeping with published NICE guidelines.
P187 SHOULD COMPUTERISED TOMOGRAPHY PRECEDE FIBREOPTIC BRONCHOSCOPY IN A DISTRICT GENERAL HOSPITAL SETTING?
R. A. Heinink, A. Fiddler, E. Stretton, A. Afridi, H. Moudgil, K. S. Srinivasan. Department of Respiratory Medicine, Princess Royal Hospital, Telford, UK
Background: NICE guidelines on the diagnosis and treatment of lung cancer recommend that computed tomography (CT) is performed before undertaking fibreoptic bronchoscopy (FOB) in the investigation of lung cancer. The reasons for this are twofold: firstly, thoracic CT can identify whether FOB or CT guided biopsy is most appropriate in order to obtain a tissue diagnosis. Secondly, it is postulated that sensitivity of FOB is higher if CT is performed prior to FOB. The latter reason is based on two studies by Laroche et al and Bungay et al (although only one of these studies reached statistical significance). Both of these studies were undertaken at major centres for the diagnosis and treatment of lung cancer, so we aimed to determine whether this explanation for the guideline was applicable in our district general hospital (DGH).
Methods: A retrospective study of the 360 FOBs performed in 2003 was undertaken. The number of FOBs leading to histocytological diagnosis and whether or not the CT scan was available at the time of FOB was recorded. The number of cancers diagnosed in the two groups of patients (CT available at time of FOB, and CT not available at time of FOB) were statistically compared using the χ2 test.
Abstract P187, table 1
Abstract P187, table 2
Abstract P187, table 3
Results: The results are summarised in the table, with the sensitivity of FOB to achieve a tissue diagnosis in the last row. The differences between these two groups of patients was not statistically significant (p = 0.54). We also performed the above analysis excluding patients with no central lesion on their CXR, and once again found no significant difference in sensitivities of FOB when CT was available compared to when CT was not available at time of FOB (53.6% v 59.5% p = 0.7).
Conclusion: To perform thoracic CT before FOB would both delay time to potential histocytological diagnosis and require an increase in radiological services, although may potentially lead to the avoidance of unnecessary FOBs. These results imply that CT scans performed before FOB do not necessarily increase the sensitivity of FOB significantly in a DGH setting.
P188 LOCAL ANAESTHESIA FOR FIBREOPTIC BRONCHOSCOPY: TRANSCRICOID INJECTION OR NEBULISATION VIA THE BRONCHOSCOPE?
N. J. Burrows, H. Pattani, N. J. Ali, G. M. Cox. Kings Mill Centre, Sutton in Ashfield, Nottinghamshire, UK
Introduction: Vocal cord anaesthesia is important during fibreoptic bronchoscopy to increase patient comfort and allow successful intubation. Previous studies have shown a transcricoid injection of local anaesthesia to be the preferred method, however, it is contra indicated in the investigation of haemoptysis, coagulopathies and HIV positive patients.1 In this study we compare a novel method of anaesthetising the vocal cords with directly nebulised anaesthesia (ENK nebuliser) versus a transcricoid injection.
Method: Consecutive patients referred for bronchoscopy were randomised to receive either local anaesthetic via the ENK nebuliser (ENK group) or by transcricoid injection (TC group). Both methods were assessed by cough counting, length of procedure and the use of extra sedation or local anaesthetic. After the procedure both patient and bronchoscopist completed visual analogue scores to rate their experiences.
Results: 64 patients were randomised (30 to the TC group and 34 to ENK group) with a predominance of males in both groups. There was a trend towards more coughs per procedure in the ENK group, however, this was not statistically significant (p = 0.09). The time it took to complete the procedure before and after passing the vocal cords was similar in both groups. More extra local anaesthetic was used in the ENK group compared to the TC group (p = 0.012). There were significant differences in the bronchoscopist visual analogue scores for ease of intubation and overall procedure experience in favour of the transcricoid method. The patient visual analogue scores were similar in both groups.
Discussion: The ENK nebuliser was found to be no better than transcricoid injection at anaesthetising the vocal cords and is probably worse. More extra local anaesthetic was needed and the bronchoscopist visual analogue scores were worse however the patient experiences were similar. The ENK nebuliser is an alternative method for anaesthetising of the vocal cords if the transcricoid method is contraindicated.
1
P189 LOCAL ANAESTHESIA TO THE ANTERIOR NARES BEFORE BRONCHOSCOPY: IMPROVED TOLERABILITY OF LIDOCAINE 5% W/V COMPARED TO XYLOCAINE
A. Kochhar, H. L. Mogford, H. Bhojal, B. E. A. Lams. Department of Respiratory Medicine, Guy’s and St Thomas’ NHS Trust
A previous audit performed in our department had determined that local anaesthetic spray to the anterior nares with xylocaine (lidocaine (10 mg/spray), ethanol, menthol, macrogel, essence of bananas, natural saccharin (Astra Zeneca)) was the part of the procedure least tolerated by patients. On the basis of this, one of two bronchoscopy lists changed to the use of lidocaine hydrochloride 5% w/v and phenylephrine hydrochloride 0.5% w/v topical solution (Aurum Pharmaceuticals), a formulation that, unlike xylocaine, does not contain menthol and ethanol. A repeat audit allowed us to gain information on whether this change led to increased tolerability.
Methods: Patients requiring a bronchoscopy received a questionnaire in which they were asked to give a score from 1–5 on the tolerability of the nasal anaesthetic spray. 1 represented “not bad”, 5 “extremely unpleasant”. Data on 100 consecutive completed questionnaires were analysed. Those who could not remember (n = 7 for xylocaine, n = 5 for lignocaine) were excluded.
Results: The use of lignocaine spray was associated with a significantly better tolerability score than the use of xylocaine spray (1 (1–5) versus 2 (1–5) respectively, data expressed as median (range), p = 0.017, see fig).
Conclusion: We suggest that operators currently using xylocaine spray as local anaesthesia to the anterior nares should consider switching to lidocaine. We postulate that the xylocaine spray’s poor tolerability may be related to its formulation which includes ethanol and menthol, both of which may cause painful irritation of the nasal mucosa.
P190 RECOLLECTION OF INFORMATION GIVEN DURING CONSENT FOR BRONCHOSCOPY: IS CONSENT STILL VALID?
S. Bari, D. A. Stock, L. Nolan, C. M. Smyth, M. J. Walshaw, M. J. Ledson. Liverpool Lung Cancer Unit, The Cardiothoracic Centre, Liverpool, UK
Background: Informed consent for any patient-related procedure is mandatory, and in 2001 the DOH published guidelines on good practice in consent taking. However, it is also important that patients maintain their understanding of the information given and hence their consent up to the time of the procedure. To look at this further, immediately prior to bronchoscopy we tested patient’s recollection of the information given to them at the preceding consenting process.
Method: In our one stop lung cancer clinic patients are consented for bronchoscopy by a senior doctor at the morning consultation, prior to bronchoscopy 2–6 hours later. The consenting process includes the use of a dedicated proforma which conveys information regarding types of local airway anesthesia (local spray (LS) and cricothyroid injection (C)), sedation (S), biopsies (B), and potential complications (shortness of breath (SOB), haemoptysis (H)), discomfort (D)). Patients are also given bronchoscopy information sheets. Subsequently, on entering the bronchoscopy suite but prior to sedation, 66 consecutive patients were asked to recall the above data, and whether they remembered it spontaneously (SP), after prompting (NP), or had no recollection (NR) was recorded.
Results: After excluding three patients (two known short term memory loss, one language problems), 63 were audited (mean age 67 years (range 28 to 93), 37 male). All remembered the procedure to which they had consented. Recollection results (as mean %) are shown in the table. Average spontaneous recall for all categories was 37%, and this was inversely related to age (<50 years 57%, 50–70 years 46%, >70 years 28% respectively).
Conclusion: Thus, although all patients could recall being informed about the procedure, after 2–6 hours only about one third of the information given could be reproduced spontaneously, and recall for the common complications of the procedure was most affected. Recall also worsened with increasing age. This study raises the issue of whether preconsenting for operations ensures that the consent is still valid up until the procedure, and highlights the special problems encountered with more elderly people, who inevitably make up the majority of patients requiring bronchoscopy.

Tolerability scores for xylocaine (median = 2, range 1–5) versus lignocaine (median = 1, range 1–5) as local anaesthetic spray to the anterior nares (p = 0.017).
P191 WHAT IS THE OPTIMUM NUMBER OF TRANSBRONCHIAL BIOPSIES?
R. Agarwal, A. K. Banerjee, J. Gonzalez, N. Donaldson, R. D. Barker. Department of Respiratory Medicine, King’s College Hospital, London, UK
Introduction: Transbronchial biopsy is indicated for the diagnosis of localised and diffuse interstitial lung disease (including sarcoidosis), pulmonary malignancy (including lymphangitis carcinomatosa), and miliary tuberculosis. The British Thoracic Society (BTS) guidelines on diagnostic flexible bronchoscopy suggest that 4–6 biopsies should be taken per patient. Depending on the underlying diagnosis, a diagnostic rate of between 25% and 75% can be achieved. Pneumothorax is a major risk factor and occurred in 5–11% of patients in previous studies.
Objectives: Evaluate the practice of transbronchial biopsy in our institution including the diagnostic efficacy and the risk of pneumothorax.
Methods: A retrospective audit of all transbronchial biopsies performed between 2001 and 2005.
Results: Data from 69 patients were analysed—21 inpatients (30%) and 48 outpatients (70%). A mean of 2.3 biopsies per patient were taken from inpatients, and a mean of 3.5 biopsies per patient from outpatients. 10% of the inpatients and 33% of the outpatients had five or more biopsies taken. The clinical indications for transbronchial biopsy were suspected malignancy in 15 patients, sarcoidosis (29 patients), tuberculosis (10 patients), other infections (including PCP) in 10 patients and interstitial lung disease (5 patients). The biopsies were diagnostic in 85% of the patients, and inconclusive in the remainder. The mean number of biopsies taken per patient was similar for those with diagnostic (3.1 per patient) and inconclusive (3.2 per patient) histology results and there was no statistically significant difference (p = 0.69). The rate of pneumothorax was 7% (5 patients). Patients who developed a pneumothorax had more biopsies taken (mean of 4.4 per patient) than those without a pneumothorax (mean of 3.1 per patient). This difference tended to but did not reach statistical significance (p = 0.08).
Conclusions: More biopsies were taken from outpatients than inpatients, which may reflect the poorer health status of the inpatients. The diagnostic efficacy of transbronchial biopsy was satisfactory at 85%, and was achieved using a lower number of biopsies than is currently recommended. There was no association between the number of biopsies taken and the likelihood of making a firm diagnosis. The pneumothorax rate was slightly high and pneumothorax was associated with a greater number of biopsies. We suggest that, in contrast to the guidelines, three good transbronchial biopsies might be sufficient for diagnosis, while minimising the risk of pneumothorax.
Abstract P191
P192 UK NATIONAL SURVEY ON ROLE OF TRANSBRONCHIAL LUNG BIOPSY AND BRONCHOALVEOLAR LAVAGE IN THE MANAGEMENT OF DIFFUSE PARENCHYMAL LUNG DISEASE
R. K. Kedia, S. Bari, T. Jordan, V. Kumar, T. Sellor M. D. Winson. Midcheshire Hospital NHS Trust, Leighton Hospital, Crewe, Cheshire CW1 4QJ, UK
Background: Diffuse parenchymal lung disease (DPLD), a generic term used to encompass large group of disorders that primarily affect the lung parenchyma and alveolar filling space in a diffuse manner and account for 15% of patients in respiratory practise. Previous studies in UK found wide variation in the management of DPLD among respiratory physicians (
). British Thoracic Society (BTS) standards of care committee issued a guidelines for the diagnosis, assessment, and treatment of DPLD in adults in 1999. BTS recommends that BAL, TBLB, and OLB should be readily available to all respiratory physicians assessing a patients with suspected DPLD. We undertook a national survey of respiratory physician in UK on their practise of BAL, TBLB, and OLB in suspected DPLD.
Methods: All respiratory physicians on BTS register were sent a detailed 12 points questionnaire to assess their current practice in management of DPLD with main focus on TBLB, BAL, and OLB. The questionnaire for survey was approved by BTS for educational purpose. All return data were collected by audit department and stored on computer for analysis.
Results: A total of 457 out of 810 (56%) respiratory physicians replied to the survey sent between August to October 2004. 415 (51%) were suitable for analysis. 64% and 35% of responders were from DGH and teaching hospitals respectively. 92% of responders reported seeing five new cases/month of DPLD. 80% of responders perform HRCT routinely prior to contemplating TBLB. 66% and 87% of responder reported performing TBLB under fluoroscopy and post procedure chest x ray (CXR) to rule out pneumothorax respectively. Only 62% of responder had facility to perform and analyse BAL. 71% of responder admitted sending less than 25% of cases of DPLD for OLB.
Conclusion: Despite BTS guideline, current UK national survey highlights the wide variation in practice of TBLB, BAL, and OLB among respiratory physicians in UK for management of DPLD. We recommend that new BTS guideline, currently under review should reassess the utility of these diagnostic procedures in the management of DPLD.
P193 PERCUTANEOUS TRANSTHORACIC LUNG BIOPSY: THE EXPERIENCE OF A DISTRICT GENERAL HOSPITAL
F. C. Gilchrist, S. S. Lok, A. Lynn, R. G. Dent. Queen Elizabeth II Hospital, Welwyn Garden City, UK
Background: Percutaneous transthoracic lung biopsy (PTLB) is a procedure used widely in the investigation of lung masses. It has a key role in the diagnosis of lung cancer. The most common indication for PTLB is a lung mass not amenable to bronchoscopic biopsy. We have audited all PTLBs carried out in the East and North Herts NHS trust over a period of two years to (1) measure local complication and diagnostic rates; (2) assess compliance with British Thoracic Society guidelines (
); (3) to see if improvements could be made in the way PTLB is carried out in our Trust.
Methods: Clinical coding identified patients who had a lung biopsy between 12/2001 and 12/2003. Case notes were checked for details of the procedure. Further information was obtained from the radiology database, private patient notes and records of multidisciplinary team (MDT) meetings kept by the lung cancer specialist nurse.
Results: During the two year period a total of 56 procedures were performed on 55 patients; 36 men and 19 women, mean age 69.14 years. 45/55 (82%) patients were discussed by the MDT but only 37 of these discussions took place before biopsy. Lung function was recorded in 44/55 (80%) patients. 38/56 procedures (69%) were diagnostic. Nine patients went on to surgery where a diagnosis was made. No diagnosis was obtained in eight patients including one individual who underwent two biopsies. In 43 patients the final diagnosis was of malignancy. Of these 34 were identified by PTLB. Therefore the cancer pick up rate was 79%. For cancerous lesions greater than 2 cm in diameter, pick up rate was 84.9% (BTS target 85–90%). Pneumothorax occurred in 11/56 or 19.6%. Of these, four required intervention, two chest drains (3.6%), and two aspiration (3.6%). Of 35 outpatients who underwent PTLB, two required admission following the procedure giving an admission rate of 5.7%.
Conclusions: Diagnostic and complication rates associated with PTLB as it is performed in our trust are within, or very close to, the values recommended by the BTS. Discussion of patients by the MDT and recording of lung function did not take place in all casesew details were available of the biopsy procedure itself. We hope that the development of a lung biopsy form covering the complete patient pathway from decision to undertake lung biopsy, to diagnosis, on which all details of the procedure can be recorded by clinic doctor, radiologist, and admitting doctor will help compliance with guidelines and aid future audit.
P194 RANDOMISED CONTROLLED TRIAL COMPARING THE ENK DEVICE WITH CONVENTIONAL ADMINISTRATION OF TOPICAL LIGNOCAINE DURING FLEXIBLE BRONCHOSCOPY
M. J. Corless, J. Deane, J. Mills, G. Pendleton, M. Munavvar. Lancashire Teaching Hospitals, Preston, UK
Background: Adequate local anaesthesia in bronchoscopy is crucial to improve comfort and tolerance during the procedure. It is also essential for good diagnostic yield. The ENK device has been shown to be highly effective in Anaesthetics during fibreoptic intubation of conscious patients with difficult airways. It nebulises small doses of local anaesthesia and oxygen through the working channel of the bronchoscope.
Objective: To compare patient tolerability and cough during bronchoscopy according to the technique of administration of local anaesthesia.
Methods: 35 patients undergoing bronchoscopy were randomly assigned to anaesthesia via the ENK device or via standard administration via syringe. One experienced bronchoscopist, one of two endoscopy nurses, and the patient completed visual analogue scores to indicate ease of the procedure, extent of coughing, patient tolerance and anxiety. Prolonged interventional procedures were excluded as these may affect the tolerability. Duration of procedure, samples taken, amount of sedation, and amount of local anaesthesia were also recorded.
Results: In each category, a higher number signifies a more favourable response.
Abstract P194
There is no significant difference in tolerability or patient cough between the two techniques. However, there was increased ease of procedure using the ENK device as judged by the bronchoscopist. For longer procedures (greater than 15 minutes in duration and often involving multiple sampling) there was a trend towards reduced cough when using the ENK device. This was not statistically significant, but this may be a reflection of the small sample size.
Conclusion: The findings suggest that this device may be useful for administration of anaesthesia in bronchoscopies which are expected to be of longer duration (for example, multiple sampling or therapeutic procedures) or in those patients who have been previously intolerant of bronchoscopy.
P195 ARTERIALISED EARLOBE BLOOD GAS SAMPLING IN THE UK: STILL AN UNDERUSED TECHNIQUE
F-JThompson1, R. H. Harvey1, M. Shaha2, E. Manderson1, D. Lai1, P. L. Shah1, S. Singh1. 1Chelsea & Westminster Hospital, London, UK; 2University of Applied Health Sciences, Switzerland
Background: Arterialised earlobe blood gas (AzEBG) sampling has been used since 1965 as an alternate for arterial blood gases (ABG).1 Despite evidence of its equivalence with ABG accuracy, it has previously been an underused technique.2
Methods: A descriptive survey was conducted to determine the provision of AzEBG sampling in the UK. A postal questionnaire was sent to 255 respiratory centres identified from the 2004 UK Directory of Asthma & Respiratory Care. Quantitative and qualitative data analysis was undertaken.
Results: The response rate was 57% (n = 110) which increased to 74% (n = 189) after a postal recall. Sixty six per cent (n = 125) were district general hospitals, 25% (n = 48) teaching hospitals, 5% (n = 9) specialist respiratory centres. The majority of respondents were nurses (93%: n = 215). Thirty seven per cent (n = 69) of respiratory centres undertook the procedure and used various equipment to collect AzEBG. AzEBG were most frequently undertaken in the lung function unit (n = 40) and ward areas (n = 27). Practitioners undertaking the procedure were nurses (n = 39), respiratory clinical nurse specialists (n = 38), and lung function scientists (n = 36). The most frequent reasons why most centres (63%, n = 120) did not conduct AzEBG included; lack of financial resource, unavailability of equipment, no training in its use (n = 47), perception of higher accuracy with ABG (n = 29), ABG technique quicker (n = 16), unaware of technique (n = 9), unsuitable patient case mix (n = 2), and patient or operator safety (n = 2).
Conclusions: In spite of the increasing provision of AzEBG over the last decade, the technique remains underused with only one third of centres adopting it. Further studies to re-establish accuracy, patient comfort and cost effectiveness are desirable. If identified as reliable and accurate, versus ABG, AzEBG can simplify blood gas procedures and monitoring of respiratory patients, and could be performed by a variety of hospital staff.
1
2
P196 THE VALUE OF A NEW CAPNOGRAPHIC DEVICE IN THE ASSESSMENT OF ASTHMA AND CHRONIC OBSTRUCTIVE PULMONARY DISEASE
M. R. Partridge1, A. Lindsell2, M. Varney2, D. Williams2. 1Imperial College London, NHLI Division at Charing Cross Hospital, London; 2Asthma Alert Ltd, Coopers Lane, Engelfield Green, Surrey TW20 0JZ, UK
Aim: The purpose of this study was to determine the degree of correlation between a traditional assessment of asthma and chronic obstructive pulmonary disease (COPD) and a novel capnographic measurement.
Background: Capnography measures the rate of change of concentration of carbon dioxide against time in exhaled breath. The shape of the capnogram is modified by obstruction of the airways. A normal capnogram has a square wave pattern arising from homogeneity of gas distribution and alveolar ventilation. Airway obstruction modifies the shape of the capnogram in predictable ways.
Methods: We have used a new, inexpensive, hand held instrument to perform capnography on 80 adult patients with a variety of respiratory diseases attending the outpatient clinics and lung function laboratory at Charing Cross Hospital. Of these, 57 patients had asthma or COPD and the patients undertook spirometry followed by capnography. Each patient completed a run of one minute duration carrying out relaxed tidal breathing. A number of sequential capnograms were analysed and a single capnographic index generated for each patient. The analysis was based on the Q-angle measurement as described by You et al. Capnographic results were compared with spirometric measurements.
Results: All patients found the technique easy to perform and capnogram shape reproducibility was high. Data for 57 patients comparing capnographic Q-angle with FEV1 %predicted showed a significant correlation (r = 0.8) and the majority of the data fell within one standard deviation of the logarithmic relation expressed by You et al.
Summary: These initials results have demonstrated a good correlation between capnographic index Q-angle and traditional spirometric parameters of airway narrowing. The technique has potential in the long term monitoring of those with airway disease. Because the method involves normal (tidal) breathing rather than forced expiratory techniques, it is easy for patients to perform.
1
P197 THE REVISED WYTHENSHAWE AMBULATORY OXYGEN PROTOCOL - 2005
A. Duck, E. Barnett, J. Vestbo. South Manchester University Hospital Trust, UK
Introduction: We have described our ambulatory oxygen protocol developed to titrate ambulatory oxygen levels for patients with interstitial lung disease and other severe lung diseases awaiting lung transplantation. In the light of the forthcoming changes in the domiciliary oxygen services we have refined our protocol to meet the new standards suggested by the British Thoracic Society (BTS 2004).
Method: Patients who describe breathlessness have pulse oximetry measurement. If pulse oximetry is <94% at rest a long term oxygen assessment (LTOT) and incremental shuttle walk test (SWT) are performed with pulse oximetry to determine level of oxygen at rest and oxygen desaturation during exercise. If pulse oximetry is >94% at rest, only a SWT with oximetry will be performed. If there is evidence of oxygen desaturation <85% on SWT and patient can achieve level 3 (70–120 metres) on SWT, an ambulatory oxygen titration test will be performed. Patients are also asked to complete an ambulatory oxygen questionnaire to evaluate the out of home activity level and likely oxygen requirements.
The ambulatory oxygen titration test will commence on the oxygen level necessary to maintain oxygen levels (PO2>8.0) at rest. The patient is asked to walk for a maximum of six minutes at a pace that is comfortable and usual for them, and to stop when they would normally stop. They must transport their oxygen and are given a choice of methods. Distance walked, Borg scale, and oxygen saturations (SpO2) pre and lowest post walk test are measured. If oxygen saturations drop <90% during walk test the oxygen level is increased from air to 2, 3, 4, and 6 l/min until SpO2 is maintained at >90% at patient’s current walk speed. Patients who maintain SpO2 at >90% on up to 2 l/min will have the walk test repeated with an oxygen conserving device attached to check for similar results.
Results: 131 patients have been tested: COPD/emphysema/α-1-antitrypsin, 48; ILD, 60; PPH, 14; bronchiectasis, 6; and 3 with miscellaneous respiratory conditions. Of the 48 patients with COPD, only 22 (46%) required supplemental oxygen to ambulate, only 15 increased their walking distance, all by 10%. 19 patients were able to maintain their SpO2>90% with supplemental oxygen and 11 perceived less breathlessness.
Conclusion: Severe breathlessness in COPD is not only related to hypoxia and patients should be able to demonstrate a reasonable walking distance ability before being prescribed supplemental oxygen for ambulation. A minimum 10% increase in walking distance should be considered in COPD, before prescribing supplemental oxygen for walking, if patients are to perceive a benefit motivated enough to use it.
P198 EVALUATION OF A TRANSCUTANEOUS CARBON DIOXIDE MONITOR (“TOSCA”) IN ADULT PATIENTS IN ROUTINE RESPIRATORY PRACTICE
S. M. Parker, N. Bhala, G. J. Gibson. Department of Respiratory Medicine, Freeman Hospital, Newcastle upon Tyne NE7 7DN, UK
Background: Although non-invasive measurement of oxygenation is routine in clinical practice, transcutaneous monitoring of PCO2 (PtcCO2) is much less used due to technical difficulties with earlier transcutaneous electrodes.
Objective: Our aim was to determine the reliability of estimating arterial PCO2 (PaCO2) using a recently introduced combined SaO2/PtcCO2 monitor (“TOSCA”, Linde Medical Systems) in adult patients in routine clinical respiratory practice.
Methods: Ethical approval was granted for the measurement of PtcCO2 in patients requiring arterial blood gases for clinical reasons. 10 minutes after the probe had been attached to an earlobe PtcCO2 was recorded, immediately before arterial blood sampling. The PCO2 values obtained were compared by Bland-Altman analysis.
Results: Samples were taken from 48 patients with varied pathology and there were no technical problems. Mean age was 51 years (range 20–86 years). The mean difference between PaCO2 and PtcCO2 was −0.04 kPa (SD 0.67) kPa. Bland-Altman analysis showed generally good agreement between the two measurements (see fig). Four of 48 measurements showed a PCO2 difference >1 kPa with no technical or clinical explanations apparent.

Conclusions: Overall the accuracy of estimation of PaCO2 by the TOSCA transcutaneous electrode was good and the device appears promising for use in routine respiratory practice.
Distal lung inflammation
P199 EFFECT OF CHANGES IN BLOOD GLUCOSE CONCENTRATION ON GLUCOSE CONCENTRATIONS OF LOWER AIRWAY SECRETIONS SAMPLED BY EXHALED BREATH CONDENSATE
N. Clark1, D. M. Wood1, D. A. Fisher2, T. Ruffles1, A. L. Brennan1, B. J. Philips1, D. L. Baines1, E. H. Baker1. 1Glucose and Pulmonary Infection Group, St George’s, University of London; 2Roehampton University, London, UK
Background: We have shown that glucose is undetectable in normal nasal secretions (lower limit of detection 0.5 mM), but nasal glucose concentrations are elevated when blood glucose exceeds 6.7–9.7 mM, the airway glucose “threshold” (
). We have recently developed non-invasive techniques to measure glucose concentrations in lower airway secretions collected as exhaled breath condensate (
). In this study we determined whether a blood glucose threshold for the detection of glucose in lower airway secretions could be detected.
Methods: Hyperglycaemic clamping was used to change blood glucose (BG) of healthy volunteers (1) rapidly from baseline to >12 mM then back to baseline (n = 6) and (2) slowly from baseline to 12 mM in 1 mM increments (n = 6). Glucose was measured in airway surface liquid (ASLG) from lower airways sampled as exhaled breath condensate collected for 10 minutes after 10 minutes at each BG concentration.
Results: (1) At baseline BG was 5.4 (SD 0.9) mM and ASLG was 0.36 (SD 0.27) mM. BG was increased to 14.6 (SD 1.6) mM and ASLG rose significantly to 0.75 (SD 0.39) mM (p = 0.045). When the clamp was removed BG fell to 5.3 (SD 0.8) mM and ASLG to 0.38 (SD 0.27) (p = 0.07). (2) At baseline BG was 5.7 (SD 0.5) mM and ASLG was 0.30 (SD 0.28) mM. BG was increased in 1 mM steps. ASLG was significantly increased above baseline at and above blood glucose 9.4 (SD 0.5) mM (p = 0.046).
Conclusions: Glucose was increased in lower airway secretions when blood glucose was raised and was cleared from airway secretions when blood glucose fell. An apparent lower airway glucose threshold of 9.4 (SD 0.5) mM was identified which was similar to the nasal glucose threshold. Taken together these findings imply that glucose is cleared actively from airway secretions by a saturable glucose transporter such as the sodium-glucose cotransporter.
P200 DEVELOPMENT OF AN IN VIVO MODEL OF GLUCOSE CLEARANCE FROM HUMAN AIRWAY SURFACE LIQUID
T. Ruffles1, N. Clark1, D. A. Fisher2, D. M. Wood1, A. L. Brennan1, D. L. Baines1, B. J. Philips1, E. H. Baker1. 1Glucose and Pulmonary Infection Group, St George’s, University of London, UK; 2University of Surrey, Roehampton, UK
Introduction: Glucose concentrations in human airway surface liquid (ASL) are increased during hyperglycaemia (
). Increased glucose concentrations in ASL from lower airways of patients intubated in intensive care was associated with increased airway infection (Philips. Thorax 2005 (in press)). Clearance of glucose from airway secretions could reduce the risk of pulmonary infection in susceptible individuals. However, the physiology of glucose clearance from human airways is poorly understood. We have previously demonstrated that glucose concentrations can be measured in ASL collected as exhaled breath condensate (EBC) (
). The aim of the present study was to develop an in vivo model of glucose clearance from ASL using this technique.
Methods: 10 minute EBC collections were made from six healthy volunteers before (one collection) and after (three consecutive collections) a five minute inhalation of nebulised glucose solution (5 mM glucose, 150 mM NaCl). Control experiments were performed on two further occasions with (a) no nebuliser and (b) nebulised 150 mM NaCl. EBC samples were lyophilised to remove NH4+ and resuspended in deionised water. Samples were analysed for conductivity to estimate total cation concentration and dilution factor of ASL droplets in EBC. EBC glucose concentration was measured by high performance anion exchange chromatography with pulsed amperometric detection and corrected for dilution to estimate ASL glucose concentration. Participants gave informed consent and the study was approved by the local research ethics committee.
Result: Baseline ASL glucose concentration was 0.63 (0.28–0.92) mM (median (interquartile range)). The glucose nebuliser significantly increased ASL glucose concentration by 2.21 (1.34–5.01) mM (p = 0.046). ASL glucose had fallen to 0.52 (0.14–1.62) mM and 0.31 (0.20–0.84) mM at the 2nd and 3rd collection following the nebuliser respectively (p = 0.042). Neither repeat EBC collections nor saline nebulisation significantly altered dilution factor or ASL glucose concentrations. No adverse effects of the technique was reported by the volunteers.
Conclusion: ASL glucose concentrations can be raised by nebulisation of glucose and glucose is cleared rapidly from airway secretions. Repeat measurements and nebulisation of saline as a vehicle for glucose did not alter cation concentration or dilution factor and hence did not interfere with measurement of ASL glucose concentrations by this technique. Further studies are required to elucidate mechanisms underlying glucose clearance from human airways.
P201 THE EFFECT OF A PDE4 INHIBITOR (CILOMILAST) ON THE RELEASE OF INFLAMMATORY CYTOKINES FROM AIRWAY EPITHELIAL CELLS
K. J. C. Byrne1, G. Skibinski1, L. McGarvey1,2, L. G. Heaney1. 1Respiratory Research Group, Queens University Belfast, N Ireland; 2Regional Respiratory Centre, Belfast City Hospital, N Ireland
Exacerbations are an important clinical feature of chronic obstructive pulmonary disease (COPD) and reduction of the proinflammatory response induced by infective agents is an important therapeutic strategy. A new generation of selective phoshodiesterase-4 (PDE4) inhibitors such as Cilomilast, have been proposed for the treatment of COPD, however their effects on the inflammatory response of airway epithelial cells are not fully established.
Abstract P201 The effect of Cilomilast on cell lines stimulated with lipopolysaccharide (100 μg/ml)
We used the airway epithelial cell lines, A549 and BEAS-2B, to investigate the effect of Cilomilast on the lipopolysaccharide (LPS) stimulated release of proinflammatory cytokines. Cells were stimulated with LPS from Pseudomonas aeruginosa in the presence or absence of various concentrations of Cilomilast. Interleukin-6 (IL-6) and IL-8 were measured in cell culture supernatants.
Preliminary data in primary bronchial epithelial cells, obtained from smokers with and without COPD suggest this effect is also observed in primary cells.
These data suggest that Cilomilast may be useful in reducing the proinflammatory response to bacterial products in airway epithelial cells. This may potentially reduce the severity of clinical exacerbations in COPD patients.
Funding for this PhD (KJCB) is supplied by a DEL-CAST studentship, Industrial Partner GlaxoSmithKline.
P202 IMPROVING SURVIVAL FROM HIV ASSOCIATED PNEUMOCYSTIS JIROVECII PNEUMONIA ADMITTED TO THE INTENSIVE CARE UNIT
R. F. Miller1, M. Singer2, S. G. Edwards3. 1Centre for Sexual Health and HIV Research, 2Bloomsbury Institute of Intensive Care RFUCMS, University College London, London, UK; 3Camden PCT, Mortimer Market Centre, London, UK
Background: Patients with severe HIV associated Pneumocystis jirovecii pneumonia (PCP) may require admission to the intensive care unit; it is perceived that these patients have a poor prognosis. The aim of this study was to identify prognostic factors associated with survival in HIV infected patients with PCP admitted to ICU.
Methods: Between 1 June 1990 and 31 May 2005 there were 366 episodes of HIV associated PCP at an inner London specialist HIV/AIDS treatment centre: of these 50 (13.6%) were transferred to the intensive care unit. For each patient, by case note review, details of year of presentation (before mid 1996 (when highly active antiretroviral therapy (HAART) became available), or later), patient’s knowledge of their HIV serostatus on admission to the intensive care unit, episode of PCP, age, disease severity at presentation (Pa02, breathing room air), presence of comorbidity (cryptococcal or histoplasma infection, endocrine, cardiac, or neuropsychiatric disease), identification of bacteria or cytomegalovirus as co-pathogens in bronchoalveolar lavage (BAL) fluid, need for mechanical ventilation, development of pneumothorax, and survival were recorded.
Results: Of the 50 patients 45 were men. Overall mortality was 56%; mortality before mid 1996 was 20/27 (74%) and after this time was 8/23 (35%). In 30 patients PCP was the first presentation of HIV infection, the remainder were known to be HIV infected before admission to the intensive care unit with PCP. As a group patients were profoundly immunosuppressed, median (range) CD4 count = 30 (0–320) cells/μl and were hypoxaemic, median (interquartile range) Pa02 = 7.7 (6.7–8.6) kPa: 46 patients received adjunctive methylprednisolone and 29 required mechanical ventilation. Pneumothorax occurred in 11 patients (nine of whom were mechanically ventilated). In univariate analysis factors associated with a poor outcome (odds ratio) were: admission to ICU before mid 1996 (5.36), presence of comorbidity (3.33), pneumothorax (1.43), and increasing patient age (1.1).
Conclusions: These data demonstrate an overall survival rate of 44% for severe HIV associated PCP requiring admission to the intensive care unit and further suggest that younger patients, diagnosed since 1996, and who have no comorbidity have a better outcome. Of note patients with co-pathology in BAL fluid (cytomegalovirus or bacterial infection) or those presenting with previously undiagnosed HIV infection and low CD4 counts do not appear to have a worse prognosis than those patients without BAL co-pathology or those known to be HIV infected (and accessing health care) before admission to the intensive care unit with severe PCP.
P203 GENOTYPIC VARIATION IN PNEUMOCYSTIS JIROVECII ISOLATES IN BRITAIN
R. F. Miller1, A. R. Lindley2, A. Copas1, H. E. Ambrose2, R. J. O. Davies3, A. E. Wakefield2. 1Centre for Sexual Health and HIV Research, RFUMS, University College London, UK; 2Molecular Infectious Diseases Group, Department of Paediatrics, Weatherall Institute of Molecular Medicine, University of Oxford, Oxford, UK; 3Oxford Centre for Respiratory Medicine, Churchill Hospital, Oxford, UK
Background:Pneumocystis jirovecii is the cause of Pneumocystis pneumonia (PCP) in immunosuppressed humans. Asymptomatic colonisation with P jirovecii may occur in patients with minor immunosuppression or chronic lung disease. P jirovecii has been identified in air in rural and hospital environments. The aim of this study was to describe the molecular epidemiology of P jirovecii in Britain over a 12.5 year period.
Methods: Between January 1989 and July 2001 161 samples of P jirovecii were obtained from 116 patients (115 adults) with bronchoscopy confirmed PCP (n = 119), patients colonised by P jirovecii (n = 35), and from air spora (n = 6). Three patients with PCP underwent repeat bronchoscopy (interval = 17–23 days) because of failure to respond to therapy. Genotypes P jirovecii were discriminated by identifying polymorphisms at positions 85 and 248 of the mitochondrial large subunit rRNA (mt LSU rRNA).
Results: Genotype 1 (38%) was the most frequently identified genotype: genotype 2 (26.6%), genotype 3 (20.3%), and genotype 4 (5%) were less common. Mixed infection (more than one genotype) was identified in 10% of samples. Whereas genotype 1 was the most frequently detected type in both patients with PCP and those colonised by P jirovecii (38% and 42% respectively) these groups differed in the relatively lower rate of detection of genotype 4 (2% v 17%) and the higher detection of mixed infection in those with PCP (13% v 3%). In patients with PCP there was no association between year of diagnosis and specific genotypes. Detection of specific genotypes of P jirovecii was associated with patient’s place of residence; p = 0.02. There was no association between specific genotypes and clinical severity of PCP, as measured by Pa02; p = 0.3. In the three patients with PCP who had repeat bronchoscopy the genotype of P jirovecii was the same in the first and second lavage sample.
Conclusions: The finding of similar genotypes in isolates of P jirovecii from patients with PCP, those colonised and in samples of air spora, together with evidence of clustering of specific genotypes with patient’s postcode of residence is consistent with the hypothesis of person-to person transmission of P jirovecii, via the airborne route. The lack of association between specific mt LSU rRNA genotypes and severity of PCP suggests that this locus is not implicated in virulence of the organism. The lack of change of genotype in those who had repeat bronchoscopy suggests that P jirovecii does not mutate in the human host during an episode of PCP.
P204 COLONISATION OF THE LUNGS OF BRONCHIECTASIS PATIENTS WITH PSEUDOMONAS AERUGINOSA IS NOT STRONGLY RELATED TO SMOKING OR SEVERITY OF DISEASE
M. Pasteur1, Z. Pond1, O. Twentyman1, A. Jones2. 1Norfolk and Norwich University Hospital, Norwich, Norfolk; 2University of East Anglia, Norwich, UK
Introduction: Factors influencing colonisation of the lungs of bronchiectasis patients with Pseudomonas aeruginosa (Pa) are poorly understood. A correlation between Pa and poor lung function has been identified.1 This study aimed to assess the role of smoking and disease severity in predicting colonisation with Pa.
Methods: Consecutive adult patients with bronchiectasis were seen in the outpatient clinic where demographic data, smoking history and disease severity (FEV1 % predicted, number of lobes involved on HRCT and number of decades with symptomatic bronchiectasis) were recorded. Patients were asked to provide three sputum specimens for culture and case records were examined for previous microbiology data. Colonisation with Pa was defined as two positive isolates out of a minimum of three satisfactory specimens. Patients were identified as smokers if there was a >1 pack year history of smoking overlapping with bronchiectasis symptoms. Data were analysed with non-parametric statistical tests using SPSS.
Results: 266 patients were identified (mean age 64.0 years, male = 94). 226 had satisfactory microbiology data of whom 55 were colonised with Pa. 37 smokers were identified but this was not associated with Pa colonisation (p = 0.54). Univariate logistic regression analysis showed a significant but weak association between number of lobes involved and Pa colonisation (p = 0.94 at 90% level). Significant association was found between FEV1 (p = 0.012 at 95% level) and duration of disease (p = 0.01 at 95% level). However numbers of lobes on CT, disease duration, and FEV1 each only explain around 5% of the variation in colonisation. Multivariate modeling did not strengthen any association due to co-linearity of variables and lack of statistical power.
Conclusions: Colonisation with Pa in bronchiectasis is not associated with smoking and only weakly associated with markers of disease severity. Other host or environmental factors may have more importance.
1
P205 A RAPID TEST FOR MYCOPLASMAL PNEUMONIA
J. H. K. Hull, A. C. Miller. Mayday University Hospital, London Road, Croydon, UK
Mycoplasma pneumoniae (MP) is a common cause of community acquired pneumonia. The clinical and radiological manifestations may mimic a number of other pneumonic illnesses, potentially leading to misdiagnosis and inappropriate investigation and management. Currently there is no simple, inexpensive bedside test to facilitate rapid diagnosis and definitive serological confirmation is usually only possible retrospectively.
Autoantibodies that agglutinate human erythrocytes at 4 degrees (cold agglutinins) have been found in up to 76% of patients with MP. In 1958, Garrow described a simple bedside test for the rapid detection of cold agglutinins. He recommended that an equal amount of blood be added to citrate solution (as available in standard prothrombin tubes) and cooled to <5°C. If positive, there is floccular agglutination (see fig) which disappears when the tube is hand warmed. A subsequent study found that the test has 100% sensitivity and 97% specificity for the laboratory based detection of agglutinins (at titre ⩾1:64) and a 70% positive predictive value for MP.

Sample pre (A) and post (B) cooling. Arrow indicates positive result.
During the winter of 2004/2005 we diagnosed seven cases of MP using this test. The cases included a doctor working in intensive care with clinical and radiographic changes suggestive of pulmonary tuberculosis, two middle aged patients with respiratory failure and a 65 year old man with acute confusion. A rapid diagnosis in all these cases considerably assisted immediate management.
Although the value of this test was highlighted by Macfarlane1 and Neale in 1979, it is our experience that many trainees and specialists are unaware of its existence, simplicity, and value.
1
P206 INPATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE AND ACINETOBACTER POSITIVE CLINICAL ISOLATES
I. K. Tailor1, A. Bentall1, L. Stannard1, D. Thomas1, S. Connell1, M. Gill1, S. Gompertz1. 1University Hospital (Selly Oak), Birmingham, UK
Introduction: Acinetobacter can cause hospital acquired infection and is of increasing concern because of its resistance to commonly-used antibiotics. We retrospectively identified 29 patients with clinically diagnosed chronic obstructive pulmonary disease (COPD) and Acinetobacter positive isolates and describe their demographic and microbiological characteristics.
Methods and Results: 29 patients admitted with an exacerbation of COPD, who had positive isolates for Acinetobacter, were identified from the relevant clinical and microbiological databases (March 2003–January 2005). Fifty nine per cent (17/29) were male. Mean age (SD) was 71 years (10.6). Of the 13 patients with recent spirometry, nine had severe and four had moderate COPD (NICE 2004). Mean FEV1 (SD) in these individuals was 0.70 (0.27) l; FEV1 %predicted 30.8 (8.3) % and FEV1/VC 31.8 (12.7) %. Twelve patients died during their admission (12/29; 41%), seven (24%) were admitted to ITU, and mean (SD) hospital stay was 25 (20) days. Seven per cent (2/29) of patients had a previous history of Acinetobacter infection or colonisation.
Acinetobacter was isolated from: sputum, 16 patients (55%); blood cultures, 10 (35%); or both sputum and blood, three patients (10%). Eighty six per cent (25/29) of patients acquired infection nosocomially, while 14% (4/29) of patients had community acquired infection.
The isolates from 93% (27/29) of patients were sensitive to Meropenem. One of the Meropenem resistant Acinetobacters was sensitive to Amikacin and Tobramycin; the other was multiresistant (including to Tazosin, Ceftazidime, Amikacin, and Tobramycin). None of the isolates was sensitive to Ciprofloxacin, Gentamicin, Ampicillin, Cefuroxime, Cefotaxime, Chloramphenicol, or Trimethoprim. More than two thirds of patients had Acinetobacter isolates sensitive to Tobramycin and Amikacin (72% and 82% respectively). Ten per cent (3/29) were sensitive to Tazosin while only 3% (1/29) were sensitive to Ceftazidime.
Conclusions: Inpatients with COPD who culture Acinetobacter have a high mortality and/or prolonged hospital stay. It is necessary to adhere to strict control measures to prevent transmission in hospital and outbreaks of resistant strains.
P207 HOW GOOD ARE WE IN IMPLEMENTING BTS GUIDELINES IN THE MANAGEMENT OF ADULT COMMUNITY ACQUIRED PNEUMONIA?
A. Khan. Royal Devon and Exeter Hospital (Wonford), Devon, UK
Background: CURB-65 is a simple severity assessment tool recommended by the British Thoracic Society (BTS) guidelines published in 2001 and updated in 2004 in the management of adult community acquired pneumonia (CAP).This is a 6 point scale (0–5)—one point for each of Confusion, Urea >7 mmol/l, Respiratory rate ⩾30/min, low systolic (<90 mm Hg) or diastolic (⩽60 mm Hg) Blood pressure, and age ⩾65 years. We evaluated the use of CURB-65 score in hospital practice for the purpose of this retrospective audit.
Methods: We looked at adult immunocompetent patients diagnosed with community acquired pneumonia (symptoms and signs consistent with lower respiratory tract infection associated with radiographic shadowing) admitted over six month period to Derriford hospital serving a population of 450 000. Data were obtained from hospital clinical coding system and thorough analysis of medical records of individual patient. All base line demographics, clinical, laboratory, and radiological data were recorded at the initial hospital presentation. Specific search was made to identify documentation of CURB-65 components in medical records.
Results: Eighty four (84) patients were identified who were diagnosed with community acquired pneumonia in six month period between 23/10/2003 to 22/04/2004. Thirty nine (39) were males, median age was 72.2 years (range 19–96) and 45 were non-smokers. Fifty two (52) were referred by their general practitioner and the rest were admitted via accident and emergency department. The specialist respiratory clinicians managed 30/84 (35%). We found that there were no documented record for mental confusion in 68 patients (81%), urea in three (3%), respiratory rate in 29 (35%), and blood pressure in two (2%). Sixty (60) patients were discharge from the hospital with a mean stay of six days. Twenty four (24) patients died because of their illness and 20 of this group (83%) were not risk stratified according to CURB criteria. The mortality was high in the elderly (average age 80 years, range 69–95) age group.
Conclusions: This audit highlights the fact that BTS pneumonia guidelines were not followed according to CURB-65 score in substantial number of patients. Documentation for mental confusion was particularly scanty and recording the respiratory rate in significant number of patient was missing. We recommend that every acute trust should locally adopt BTS CURB-65 risk stratification of CAP. This should be made available to the junior staff in their induction programmes. This topic should be regularly audited and The BTS audit tool for community acquired pneumonia on their website is certainly a very useful tool in this regard.
P208 THE ROLE OF PLASMA DNA CONCENTRATION AS A PREDICTOR OF MORTALITY AND SEPSIS IN CRITICALLY ILL PATIENTS
S. J. Wort2, A. Rhodes1, H. Thomas1, R. Pearse1, P. Collinson1, E. D. Bennett1. 1Intensive Care Unit, St Georges’s Hospital, London SW17 0QT, UK; 2Department of Respiratory Medicine, Hammersmith Hospital, London W12 0HS, UK
Introduction: Risk stratification of severely ill patients remains problematic, resulting in increased interest in potential circulating markers, such as cytokines, procalcitonin, and brain natriuretic peptide. Recent reports have indicated the usefulness of plasma DNA as a prognostic marker in various disease states such as trauma, myocardial infarction, and stroke. To our knowledge there are very few studies examining the role of plasma DNA in the setting of the critically ill patient in the intensive care setting.
Methods: 52 consecutive patients were studied in a general intensive care unit. Blood samples were taken on admission and stored for further analysis. Plasma DNA levels were estimated by a polymerase chain reaction (PCR) method using primers for the human b-haemoglobin gene. Patients were followed up to three months.
Results: Seventeen patients of the 52 patients investigated died within three months of sampling. 19 of the 52 patients developed either systemic inflammatory response syndrome (SIRS), sepsis, or severe sepsis. Plasma DNA concentrations were found to be significantly different between patients who died and those who survived. The medians and interquartile ranges (IQR) for both groups were as follows: non-survivors; median = 321.4 ng/ml, IQR = 245.3: survivors; median = 70.7 ng/ml, IQR = 67.1 (Mann-Whitney U test, p = 0.0003). In addition, plasma DNA concentrations were found to be significantly different between patients who developed a sepsis state and those who did not. The medians and interquartile ranges for both groups were as follows: septic patients, median = 192.1 ng/ml, IQR = 298; non-septic patients, median = 73.8 ng/ml, IQR = 110.6 (Mann-Whitney U test, p = 0.03). Furthermore, plasma DNA levels were higher in patients who needed 24 hours or more of inotropic support (median = 246 ng/ml, IQR = 350.4 v 69.6 ng/ml, IQR = 107.2; Mann-Whitney U test, p = 0.007) but not 24 hours or more ventilation (79.33 ng/ml, IQR = 259.01 v 81.04 ng/ml, IQR = 110.41; Mann-Whitney U test, p = 0.27) nor in those who needed 24 hour or more of renal support (224 ng/ml, IQR = 353.6 v 78.8 ng/ml, IQR = 191.4; Mann-Whitney U test, p = 0.08). In addition, receiver operator characteristic (ROC) curves were calculated for the use of plasma DNA as a predictor of death and of sepsis (in comparison to the SOFA score).
Conclusions: The results presented here demonstrate that plasma DNA may be a useful prognostic marker of mortality and sepsis in intensive care patients. Further research is clearly needed in the use of this novel marker in the intensive care setting and into the possible mechanisms of release/clearance of plasma DNA in disease states.
P209 KL-6 AS A MARKER OF ALVEOLAR INFLAMMATION IN PATIENTS WITH ARDS
N. Nathani, G. Perkins, N. Murphy, M. Manji, B. Tunnicliffe, D. Thickett. Lung Injury and Fibrosis Treatment Programme, University of Birmingham, UK
KL-6 is expressed on the surface of alveolar type II cells and elevated KL-6 in plasma and epithelial lining fluid levels have previously been shown to correlate with the severity of disease and survival in ARDS. The relation between alveolar inflammation and KL-6 has not been ascertained. We hypothesised that the increase of KL-6 in ARDS is dependent upon the severity of neutrophilic inflammation. Furthermore we were interested in the relation between significant alveolar infection and KL-6 levels.
Plasma arterial samples were collected from ARDS patients at day 1 and when possible at day 4 along with bronchoalveolar lavage (BAL) samples on the same day (plasma n = 61, matched plasma and BAL, n = 37). Bacterial growth in the BAL was determined by quantitative cultures (significant at >1×104). KL-6 and IL-1 were measured by ELISA. Data were analysed using unpaired t tests. Data are presented as mean (SD).
Plasma KL-6 of ARDS patients were elevated (mean 548 (SD 295.10) U/ml) compared to at risk (274 (SD 185.17) U/ml, p = 0.005) and normal control (204 (SD 166.81) U/ml, p = 0.004). Plasma Kl-6 correlated with correlated with lung injury scores (r = 0.4891, p = 0.0021). In non-survivors the plasma KL6 levels increased significantly at day 4 (p = 0.03) when compared to day 1.
BAL Kl-6 was detectable in all ARDS patients (BAL KL-6 = 589 U/ml). BAL-KL-6 levels correlate with the plasma levels (r = 0.3260, p = 0.04). BAL KL-6 also correlated with the BAL myeloperoxidase (MPO) activity (r = 0.3417, p = 0.044) and the BAL cell count/ml (r = 0.3991, p = 0.0237) and BAL IL-1 (r = 0.4045, p = 0.029).
BAL KL-6 of ARDS patients (day 0/1 and day 4) with significant pathogenic growth were similar (659 U/ml, n = 14) compared to those without significant infection (481 U/ml, n = 24, p = 0.246). Plasma results did not show any difference.
This study has demonstrated for the first time that BALF KL-6 is increased in patients with ARDS. BALF KL-6 correlated with plasma KL-6 and was related to the severity of neutrophilic inflammation. Alveolar infection does not seem to determine the levels of KL-6 in either BALF or plasma. In conclusion, we suggest that KL-6 may represent a useful marker of alveolar type II cell dysfunction in ARDS as levels reflect the severity of lung injury and neutrophilic inflammation but not alveolar infection.
Asthma: basic mechanisms
P210 PROTEOMIC COMPARISON OF BRONCHOALVEOLAR LAVAGE AND INDUCED SPUTUM
A. R. Horsley1,2, M. Imrie1,2, R. Gray1,2, D. Noble2, A. P. Greening1,2, J. A. Innes1. 1Molecular Medicine Centre, Western General Hospital, Edinburgh EH4 2XU; 2Department of Respiratory Medicine, Western General Hospital, Edinburgh EH4 2XU, UK
Introduction: Induced sputum (IS) offers the possibility of non-invasively sampling the biochemical composition of airway lining fluid. To investigate the contribution of the lower airway to IS, we have used mass spectrometry to compare the proteomic profiles of IS and lower airway samples obtained by bronchoalveolar lavage (BAL).
Methods: Saliva and IS were obtained on patients immediately before undergoing bronchoscopy for clinical indications. Bronchoalveolar lavage (BAL) was obtained by injecting and aspirating 4×30 ml 0.9% saline from a bronchoscope wedged in the right middle lobe, unless directed otherwise by site of pathology. Samples were stored on ice and processed within two hours. Sputum plugs were harvested from IS and processed in DTT. SELDI analysis: Samples were pipetted onto a Ciphergen CM10 chip and analysed by SELDI-TOF mass spectrometry. Paired analysis of spectra between 5 and 15 kDa was performed by computer and manually verified. Mass spectrometry peaks were scored as present or absent and those peaks representing multiple charges of the same protein were excluded.
Results: Results are currently available for the initial seven patients (final diagnosis respiratory tract infection ×2, sarcoid ×1, malignancy ×2, nothing found ×2). A total of 160 protein peaks were detectable in the BAL samples. Of these, 111 (69%) were also detectable in IS. A total of 173 protein peaks were identified in IS. Of the 62 peaks in the sputum samples that were not present in BAL, 37 (60%) were also not detectable in saliva.
Conclusions: These results suggest that IS contains a composite mix of protein from the distal airway (common to BAL) and the central airway (unique to IS) with some salivary components admixed. The presence of proteins unique to BAL suggests that the two techniques for sampling the lower airway are complementary rather than wholly interchangeable. Despite this, the majority of BAL proteins can also be detected in induced sputum. Further work required to characterise the BAL proteome in different disease states is ongoing.
P211 THE EFFECTS OF NEBULISED BRONCHODILATORS ON METOBONOMIC PROFILE OF EXHALED BREATH CONDENSATE FROM HEALTHY SUBJECTS
G. Frazer1, J. Miller1, J. Barr2, O. Beckonert3, P. Phillips3, I. Kilty3, W. MacNee1. 1University of Edinburgh, UK; 2Royal Infirmary of Edinburgh, UK; 3Pfizer Global Research & Development, UK
Introduction: Metabonomic analysis of exhaled breath condensate (EBC) samples has the potential to distinguish between subjects with chronic obstructive pulmonary disease (COPD) and controls based on differences in nuclear magnetic resonance (NMR) spectra. In order to determine whether this may be confounded by drug effect we undertook a study to examine the effects of nebulised salbutamol and ipratropium bromide on the metabonomic profile in EBC in healthy volunteers.
Subjects: Six healthy volunteers without a current or past history of a clinically significant atopic/allergic disorder or chronic upper or lower respiratory tract disease were recruited. All were non-smokers or ex-smokers with <5 year pack years of tobacco exposure and aged between 18 and 60.
Methods: Subjects were asked to refrain from caffeinated beverages for 312 hours and from strenuous exercise for 324 hours before taking part in the study. All subjects gave a 20 minute EBC sample at baseline. Spirometry and exhaled carbon monoxide were then assessed. Subjects were then given 5 ml of salbutamol and 0.5 ml of ipratropium bromide by nebuliser. EBC collections were repeated at 30 minutes and two hours post the completion of the nebuliser. All EBC samples were stored at −80°C until analysed. Samples were prepared in either 150 μl D2O (>99.9%) including 0.03 mM TSP and 3 mM NaN3 or 150 μl containing phosphate buffer (D2O:0.2M phosphate buffer = 2:1), TSP (0.03 mM) and NaN3 (3 mM). Metabonomic analysis was carried out using NMR.
Results: A number of peaks in the spectra were observed in pre-bronchodilator samples, with increased spectra complexity with the phosphate buffer. No significant changes were seen after nebulised salbutamol and ipratropium bromide (see figs 1 and 2).

Metabonomic profile of EBC pre and post nebulised bronchodilator.

{kind=link}
{kind=link}
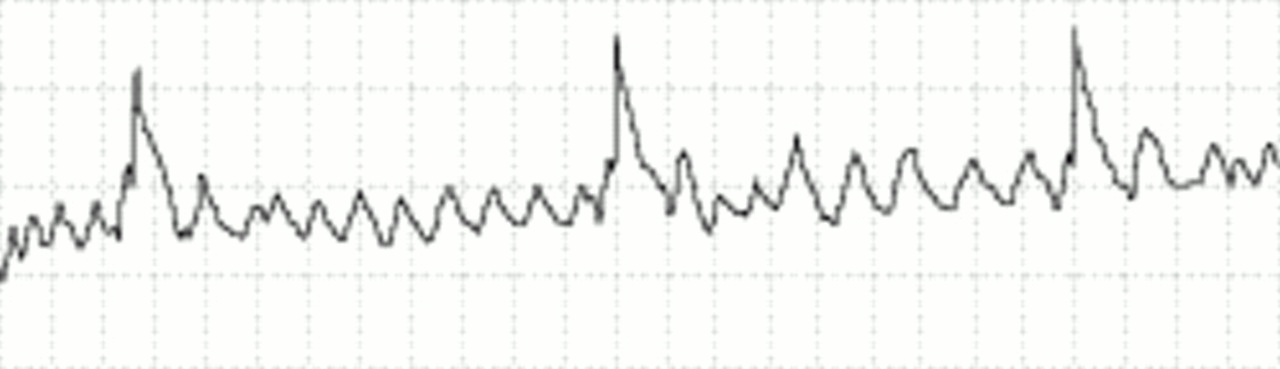{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
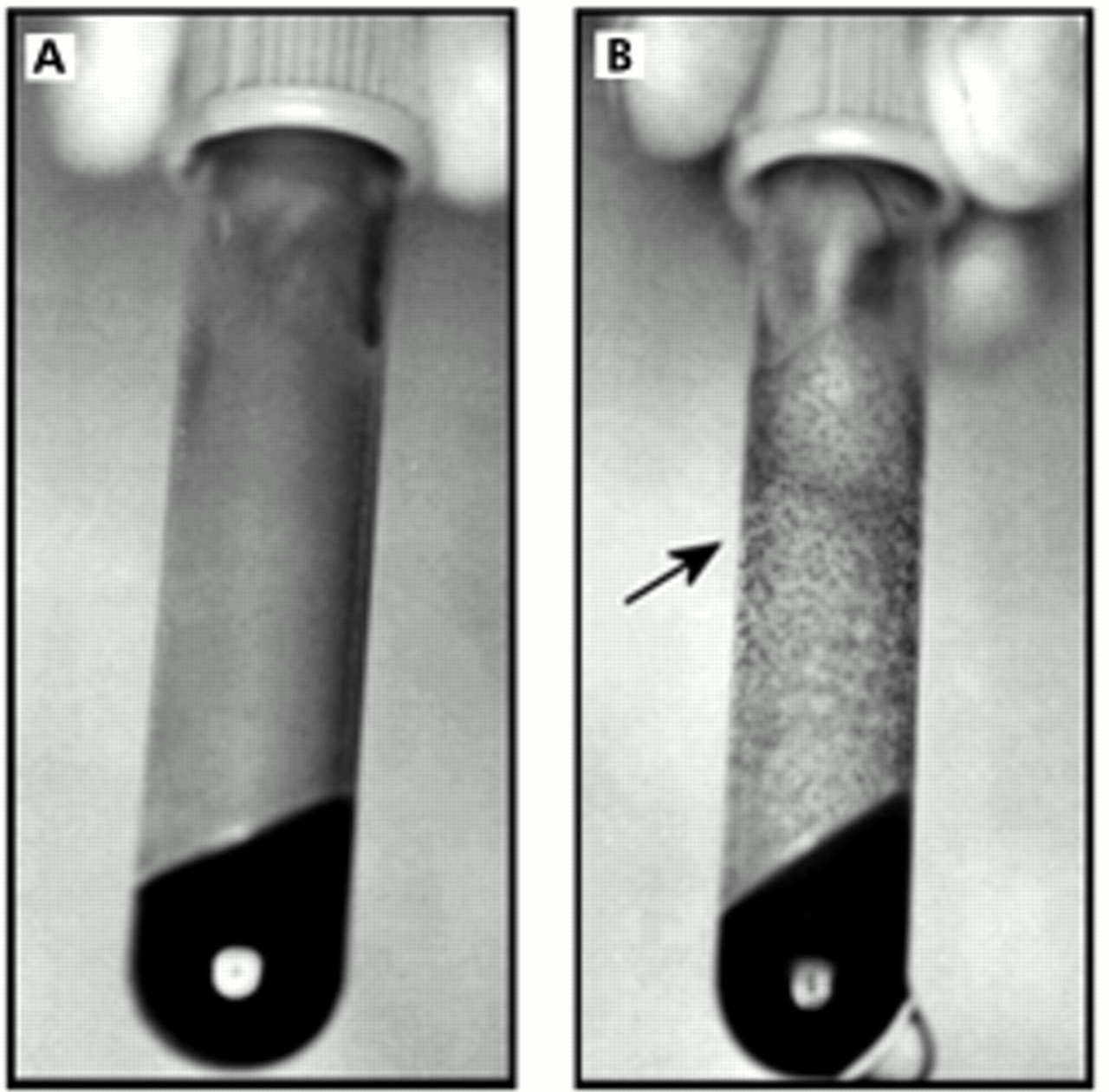{kind=link}
{kind=link}
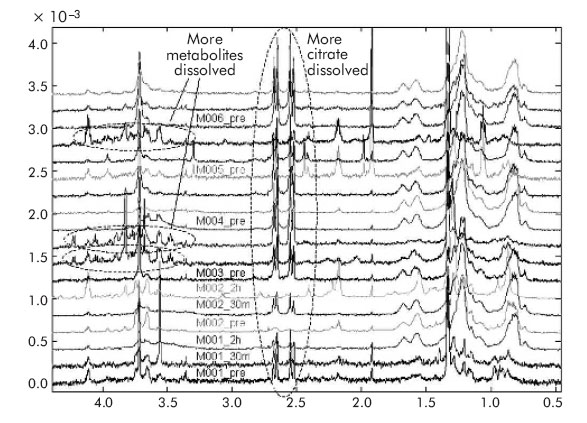{kind=link}
Effect of phosphate buffer on metabonomic profile of EBC pre and post nebulised bronchodilator.
Summary: Nebulised bronchodilators did not cause any change in the metabonomic profile of EBC from six healthy volunteers. This suggests that any difference in metabonomic profile observed between COPD subjects and controls will not be due to the effects of these drugs. Further studies are needed to investigate the utility of metabonomics for EBC analysis in COPD subjects.
Supported by Pfizer Global Research & Development (Sandwich, Kent).
P212 METACHOLINE INDUCED REGIONAL VENTILATORY ABNORMALITIES IN NORMAL SUBJECTS
P. W. Ind, N. A. Marks, W. E. Svensson, A. M. Al-Nahhas. NHLI, Hammersmith Campus, Imperial College, London, UK
Krypton-81m scanning has long been known to show patchy ventilatory abnormalities in obstructive lung disease. We have examined the effect of induced bronchoconstriction on regional ventilation in healthy subjects.
Eight normal subjects (5 female, aged 22–50 years) with normal lung function (mean FEV1 107 (SD 10.4) %predicted, KCO 107 (SD 18.5) %pred) no clinical features of asthma and minimal smoking history (six never smokers, 2<10 pack years) were studied. All showed reduction in FEV1 after high dose nebulised metacholine (MCh) (>20% at 64 mg/ml n = 1 or >15% 128 mg/ml n = 7). Mean fall in FEV1 was 11 (SD 4) % at MCh 32 mg/ml. Seated anterior and posterior Kr-81m ventilation scans were carried out, <5 minutes after nebulised saline or MCh, on two separate days, in single blind, randomised order. Scans were graded normal (grade 0) or abnormal: minor (1), moderate-diffuse (2), severe (3), analysed blind by two observers (
). Discrepancies (all of 1 grade; 7 of 16) were resolved by a third opinion (WE; Consultant in Nuclear Medicine). Following saline, mean fall in FEV1 was 2 (SD 2) % baseline and all subjects had normal ventilation scans. After MCh, mean reduction in FEV1 was 27 (SD 10)% baseline. Kr-81m scans in three showed no or subtle changes, in four moderate ventilatory defects, and in one severe, patchy defects. There was no correlation between bronchoconstriction (decrease in FEV1) and severity of scan grade.
We conclude that Kr-81m scans demonstrate significant regional ventilatory defects resembling asthma on induced bronchoconstriction in normal subjects. The technique, which has the advantages of being quick and of low radiation dose, may be useful in assessment of obstructive lung disease.
Abstract P212
P213 HUMAN LUNG MAST CELLS ADHERE TO HUMAN AIRWAY SMOOTH MUSCLE, IN PART VIA TUMOUR SUPPRESSOR IN LUNG CANCER-1
W. Yang1, D. Kaur1, Y. Okayama3, A. Ito2, A. J. Wardlaw1, C. E. Brightling1, P. Bradding1. 1Institute for Lung Health, Department of Infection, Immunity and Inflammation, University of Leicester; 2Division of Surgical Pathology, Kobe University Graduate School of Medicine, Japan; 3RIKEN Yokohama Institute, Yokohama, Japan
Mast cells infiltrate the airway smooth muscle (ASM) of patients with asthma, an event which is likely to be a key factor in the development of this disease. Adhesion is a fundamental mechanism facilitating cellular cross-talk. We have demonstrated previously that HLMC adhere avidly to ASM through an undefined mechanism, which is partially Ca2+ dependent. In mice, mast cells express the tumour suppressor named tumour suppressor in lung cancer-1 (TSLC-1) (also known as SgIGSF, IGSF-4, RA175, SynCAM-1, and Necl-2). This molecule mediates the adhesion of mouse mast cells to fibroblasts and nerves through a heterophilic Ca2+-independent mechanism. In this study we have tested the hypothesis that human mast cells express TSLC-1 and that this mediates the Ca2+independent adhesion of human mast cells to human ASM. HLMC were dispersed from macroscopically normal lung obtained within one hour of resection for lung cancer. The enzymatically dispersed cells were purified using immunomagnetic affinity selection with final mast cell purity >99%, and viability >98%. The human mast cell line HMC-1 was also studied. TSLC-1 gene expression was analysed using gene arrays (GeneChip, Affymetrix, Santa Clara, CA, USA), and surface protein expression measured by flow cytometry. To monitor adhesion, mast cells and confluent human ASM were co-cultured for 30 minutes then non-adherent mast cells were removed by centrifugation. The histamine content of adhered mast cells was measured and used as an index of relative mast cell number adhering. HLMC expressed both TSLC-1 mRNA (12.9% of GAPDH control) and surface TSLC-1 protein (mean 78.5 (SD 1.5) % HLMC positive, n = 3 donors, p = 0.0007). Blocking chicken antihuman TSLC-1 mAb reduced HLMC adhesion by 22.3 (SD 3.0) % (p = 0.004, n = 7). Similar results were seen with the HMC-1 cell line. The effects of inhibiting adhesion with EDTA and anti-TSLC-1 were additive, indicating that TSLC-1 contributes to the Ca2+-independent adhesion pathway. ASM did not express TSLC-1 indicating that TSLC-1 acts as a heterophilic adhesion molecule. In summary, HLMC adhere avidly to ASM in part via TSLC-1, and in part via an as yet undefined Ca2+ dependent pathway. This supports the hypothesis that adhesion is important in the recruitment and retention of HLMC by the ASM in asthma, and for the functional interaction of these cells.
P214 COOPERATIVE ROLES OF TOLL-LIKE RECEPTORS IN THE INDUCTION OF ANTIVIRAL RESPONSES IN COCULTURES OF AIRWAY SMOOTH MUSCLE CELLS AND LEUKOCYTES
G. E. Morris1, M. K. B. Whyte1, C. E. Brightling2, P. Bradding2, S. K. Dower1, I. Sabroe1. 1Academic Unit of Respiratory Medicine, Division of Genomic Medicine, University of Sheffield; 2Institute for Lung Health, Department of Infection, Inflammation and Immunity, Leicester-Warwick Medical School and University Hospitals of Leicester, UK
Viral infection induces specific patterns of host defence and activates proinflammatory cytokine production from airway smooth muscle cells (ASMCs). Toll-like receptor 3 (TLR3) responds to double stranded viral RNA, and we found that this receptor was expressed intracellulary in airway smooth muscle. Activation of ASMCs with poly(I:C) resulted in the generation of cytokines including IL-8, IL-6, and IP-10, an effect enhanced by costimulation with cytokines such as IL-1. Activation of ASMCs by poly(I:C) also caused the upregulation of ICAM-1. We have previously shown that LPS-activated monocytes caused the generation of cytokines from ASMCs through the production of IL-1 by the monocytes, and in keeping with these data, coculture of ASMCs with monocytes (which do not express TLR3), poly(I:C) and LPS resulted in a further induction of IP-10 production, with the potential to regulate mast cell recruitment to ASMC. In contrast, we found no evidence of expression of TLR7 and TLR8 by ASMCs, but agonists of TLR7 and TLR8 could induce cytokine production from ASMCs by indirect activation of PBMCs in ASMC/PBMC cocultures. These data indicate compartmentalised regulation of antiviral responses in the lung, and provide a mechanism by which environmental endotoxin may synergise with viral activation of leukocytes and lung tissue cells to cause inflammation relevant to asthma and viral induced wheeze.
P215 α SMOOTH MUSCLE ACTIN EXPRESSION BY HUMAN AIRWAY SMOOTH MUSCLE CELLS IS UPREGULATED IN CO-CULTURE WITH MAST CELLS
L. Woodman, D. Kaur, A. Sutcliffe, P. Bradding, C. E. Brightling. Institute for Lung Health, Leicester, UK
Background: Mast cells have been found to be microlocalised within the airway smooth muscle (ASM) bundles of asthmatic patients. This interaction is a key factor in the development of variable airflow obstruction and airway hyperresponsiveness. We hypothesised that mast cell-ASM interactions promote ASM differentiation.
Methods: To test our hypothesis we incubated ex vivo human ASM with human lung mast cell (HLMC) lysates. ASM was microdissected from large airway specimens obtained at lung resection surgery. The ex vivo ASM cells were characterised for α-smooth muscle actin expression by immunofluorescence and were used between passages 2–6. HLMC were also obtained at lung resection surgery using immunomagnetic affinity purification and lysates were prepared with 0.0625, 0.125, 0.250, and 0.50×106 cells. ASM (five donors) was grown to confluence in T75 flasks, growth arrested in serum free ITS medium and co-cultured with and without the HLMC lysates for 1, 3, and 7 days. The expression of α-smooth muscle actin was assessed at each time point for each condition by flow cytometry.
Results: The HLMC lysates significantly increased α-smooth muscle actin expression after 7 days, but not after 1 or 3 days (see table).
Abstract P215 Fold change (95% CI) in geometric mean fluorescence intensity of α-smooth muscle actin expression after stimulation with HLMC lysates from 0.0625–0.50×106 compared to control
Conclusion: Mast cell derived mediators promote ASM expression of α-smooth muscle actin supporting the view that interactions between these cells are important in the immunopathogenesis of asthma.
Supported by Asthma UK and DoH Clinician Scientist Award.
P216 REGULATION OF HUMAN LUNG MAST CELL ION CHANNELS BY ADENOSINE
S. M. Duffy, G. Cruse, P. Bradding. Department of Infection, Immunity & Inflammation, Institute for Lung Health, University of Leicester, UK
Mast cells play a pivotal role in the pathogenesis of asthma. Human lung mast cells (HLMC) express the Ca2+ activated K+ channel IKCa1, which is opened following IgE dependent activation, and which promotes Ca2+ influx and secretion. We have previously shown that IKCa1 in HLMC is suppressed by b2 adrenoceptor agonists via a Gas mediated pathway. Adenosine has dual effects on HLMC activation, potentiating IgE-dependent activation at around 106 M, and markedly inhibiting it at around 10−3 M. In asthmatic subjects in vivo, adenosine concentrations are increased, and adenosine is a potent bronchoconstrictor, an effect mediated in part via mast cell degranulation. In this study we have used the patch-clamp technique to measure ion channel function in isolated HLMC in response to adenosine. IKCa1 was opened using the specific opener, 1-EBIO. In resting cells, adenosine at 10−6 M had no effect. In cells in which IKCa1 was activated by 1-EBIO, 10−6 M adenosine also had no effect, but showed a dose dependent suppression of IKCa1 at higher concentrations. Adenosine suppressed IKCa1 in approximately 90% of HLMC that expressed IKCa1. Addition of 10−4 M adenosine reduced membrane current from 178.0 (SD 19.0) to 95.8 (SD 16.9) pA (p<0.001, n = 32) with a corresponding change in reversal potential from −63.1 (SD 1.5) to −33.2 (SD 5.2) mV (p<0.001). Suppression of IKCa1 by adenosine was reversible and reproducible. The selective A2A adenosine receptor agonist GCS21680 also suppressed IKCa1 (123.1 (SD 26.8) to 105.8 (SD 22.9) pA by 10−6 M CGS21680 (p = 0.011, n = 8). Conversely the A2A adenosine receptor antagonist ZM241385 antagonized the suppression of IKCa1 by 10−4 M adenosine (22.8 (SD 8.3) pA post adenosine, 70.9 (SD 25.1) pA post 10−6 M ZM241385 (p = 0.05, n = 10). In addition, adenosine at concentrations >10−4 M consistently opened a transient strongly outwardly rectifying current in approximately 70% of resting HLMC. Thus 10−3 M adenosine increased membrane current measured at +100 mV from 13.0 (SD 3.4) to 153 (SD 27.0) pA (p<0.001, n = 15) with a corresponding change in reversal potential of the induced current from −14.4 (SD 3.4) to +5.9 (SD 9.8) mV (p<0.001), suggesting it is either carried by Cl− or mixed cations. This transient outward current was still induced by adenosine in the presence of the A2A receptor antagonist ZM241385, and was not induced by the A2A agonist CGS21680, suggesting that it is mediated via the A2B receptor. In summary, adenosine suppresses IKCa1 through the Gas coupled A2A receptor, consistent with our previous observations with the b2 adrenoceptor. This may explain in part how adenosine inhibits HLMC secretion at high concentrations. In addition, adenosine opens a novel outwardly rectifying current, probably via the Gas coupled A2B receptor. The nature of this current requires further electrophysiolgical characterisation, and it will be important to determine its role in secretion.
Funding: Wellcome Trust.
P217 MAST CELLS EXPRESS IL-13Rα1 AND PRIMING HUMAN LUNG MAST CELLS WITH IL-13 INCREASES FCεRI EXPRESSION AND PROLIFERATION
D. Kaur1, F. Hollins1, L. Woodman1, N. Neale1, W. Yang1, P. D. Monk2, R. May2, P. Bradding1, C. E. Brightling1. 1Institute for Lung Health, Leicester, UK; 2Cambridge Antibody Technology, Cambridge, UK
Background: The Th2 cytokine interleukin (IL)-13 is implicated in the development of asthma. Its receptor, IL-13Rα1, is expressed on most leukocytes, except T cells. Evidence to support its expression by mast cells is limited.
Methods: We investigated: (1) IL-13Rα1 expression by primary human lung mast cells (HLMC), HMC-1 and LAD-2 cells; (2) the number of IL-13Rα1+ bronchial submucosal mast cells in subjects with asthma and normal controls, and (3) the effect of IL-13 priming on the mast cell expression of the high affinity IgE receptor (FcεRI) and stem cell factor receptor (CD117) by flow cytometry, histamine release by radioenzymic assay, proliferation by cell counts, and thymidine incorporation and survival by nuclear morphology assessment.
Results: IL-13Rα1 was highly expressed by primary HLMC, human mast cell lines and bronchial submucosal mast cells. However, there was no difference in expression between asthmatics and normal controls. Following priming with IL-13 for five days the geometric mean (log SEM) fluorescence intensity for FcεRI staining on HLMC (n = 6) was 79 (0.09) compared to control cells cultured in SCF alone 65 (0.08) (1.2-fold increase; 95% CI 1.11 to 1.34; p = 0.003). IL-13 priming also increased histamine release following IgE/anti-IgE activation the mean (SEM) percentage histamine release above spontaneous secretion by HLMC (n = 3) was 13.2 (3) % and increased after priming with IL-13 to 20.4 (4.7) % (56 (9.8) % increase v IgE/anti IgE alone; p = 0.03). Priming also increased proliferation of HLMC (1.5-fold increase in cell number after IL-13 priming compared to SCF alone, 95% CI 1.2 to 1.8; p = 0.003) and LAD-2, but not HMC-1 without affecting cell survival or CD117 expression. The IL-13 specific neutralising antibody CAT-354 inhibited all these IL-13 mediated effects.
Conclusion: HLMC express IL-13Rα1 and activation of this receptor mediates upregulation of FcεRI and cell proliferation. These data support the view that targeting IL-13 may be beneficial in the treatment of asthma.
Supported by: DoH Clinician Scientist Award & Cambridge Antibody Technology.
P218 THE CCR7 LIGAND, CCL19, IS EXPRESSED BY MAST CELLS AND IS CHEMOTACTIC FOR HUMAN AIRWAY SMOOTH MUSCLE CELLS
R. Saunders, D. Kaur, L. Woodman, A. J. Wardlaw, P. Bradding, C. E. Brightling. Institute for Lung Health Leicester, UK
Background: Increased airway smooth muscle (ASM) mass is a feature of asthma. We hypothesised that smooth muscle hyperplasia in asthma is in part due to migration of ASM cells or precursors, mediated through activation of chemokine receptors. Mast cells are microlocalised to the ASM bundle in asthma and are therefore a potential source of these chemokines. We have found that ex vivo ASM in culture and ASM in bronchial mucosal biopsies express CCR7. In addition we have reported that ex vivo human lung mast cells express CCL19, one of the CCR7 ligands, and that the number of CCL19+ cells was increased in bronchial biopsy specimens of asthmatic compared to normal patients. Thus we have now investigated the role of CCL19 in ASM cell migration.
Methods: ASM was microdissected from large airway specimens obtained at lung resection surgery. The ex vivo ASM cells were characterised for a smooth muscle actin and used between passages 2–6 (n = 5). ASM cells were plated onto 8-well plates coated with 10 μg/ml fibronectin at a density of 250 000 per well. The cells were serum deprived in ITS medium for 24 hours before experimentation. Chemotaxis was assessed toward a gradient of CCL19 (25–200 ng/ml), impregnated onto blotting paper. HMC-1 cells 1.6×106 cells (n = 3) were lysed and the CCL19 concentration measured by ELISA and ASM migration towards HMC-1 lysates was also assessed.
Abstract P218 The number of cells that moved toward the CCL19 gradient per high powered field (HPF) of view after six hours
Results: ASM migration towards recombinant CCL19 followed a bell-shaped dose response curve as shown in the table. The response to 100 ng/ml CCL19 was blocked using an anti-CCL19 antibody. The concentration of CCL19 in HMC-1 lysates was 163 (20) pg/1.6×106 cells. HMC-1 lysates were chemotactic for ASM.
Conclusion: Therefore, CCL19 is chemotactic for ASM cells and mast cells have the potential through CCL19 activation of CCR7 to mediate ASM migration. This has important implications for the role of mast cell-ASM interactions in the immunopathogenesis of asthma.
Supported by: Asthma UK and DoH Clinician Scientist Award.
P219 CCL19 IS EXPRESSED BY ASM IN SEVERE ASTHMA: IMPLICATIONS FOR CHRONIC WOUND REPAIR AND AIRWAY REMODELLING
S. H. Siddiqui, R. Saunders, D. Kaur, S. Saha, N. Neale, A. J. Wardlaw, P. Bradding, C. E. Brightling. Institute for Lung Health Leicester, UK
Background: Airway smooth muscle (ASM) hyperplasia and hypertrophy are features of asthma, but are particularly prominent in more severe disease. One possible explanation for this increased ASM mass is that ASM cells or their precursors migrate to the ASM bundle under the influence of chemokines. In support of this view we have described that ex vivo ASM expresses functional CCR7 and that mast cells microlocalised within the ASM bundle may be an important source of the CCR7 ligand CCL19. In addition CCR7+ marrow derived mesenchymal stem cells have recently been shown to undergo chemotaxis towards CCL19. Therefore, we hypothesised that ASM itself may also express CCL19.
Methods: The expression of CCL19 by ASM in bronchial biopsies with asthma was assessed in 12 subjects with asthma (GINA I = 6, III = 3, and IV = 3) and five normal controls by immunohistochemistry. We investigated the role of CCL19 in an ex vivo model of wound repair with and without the addition of exogenous CCL19 (50–200 ng/ml) and CCL19 (5 μg/ml) neutralising antibody. ASM was microdissected from large airway specimens obtained at lung resection surgery. The ex vivo ASM cells were characterised for α smooth muscle actin and used between passages 2–6 (n = 3). The expression of CCL19 on ASM cells was assessed by flow cytometry and immunofluorescence. Wounds were scratched into a monolayer of ASM cells, seeded onto 8-well plates coated with fibronectin (10 µg/ml) at a density of 250 000 per well. The wounded ASM cells were photographed at 0 hours and 6 hours and the number of cells that moved into the wound after six hours were blind counted.
Results: In vivo ASM expressed CCL19 in the three subjects with severe asthma, but not in those with mild-moderate disease or normal controls. CCL19 was expressed in 43.5 (7.7) % of ex vivo ASM. Exogenous CCL19 did not enhance wound healing, but inhibition of CCL19 with a neutralising antibody, significantly reduced wound healing, in the presence or absence of CCL19 (see table).
Abstract P219 The number of cells that moved into the wound per high powered field (HPF) of view after six hours
Conclusion: Therefore, CCL19 is expressed constitutively by ASM in severe asthma and by primary ASM in culture. Autocrine activation of CCR7 by ASM-derived CCL19 may be an important wound repair mechanism in severe asthma.
Supported by: Asthma UK and DoH Clinician Scientist Award.
P220 EXPRESSION OF TRPM7 AND TRPM2 CHANNELS IN HUMAN LUNG MAST CELLS
R. C. E. Wykes1,2, E. P. Seward2, P. Bradding1. 1University of Leicester, UK; 2University of Sheffield, UK
Mast cells play an important role in many diverse diseases including asthma and pulmonary fibrosis. There is great interest in the role ion channels play in the regulation of mast cells. Recently transient receptor potential (TRP) proteins have been identified as a superfamily of ion channels important in regulating cation influx into cells. The physiological function and cellular roles of the TRPM family of ion channels are poorly understood. We have previously reported the identification of a non-selective but Ca2+ permeable cation channel in human lung mast cells (HLMC) and the human mast cell line model, LAD2 (BTS winter meeting 2004), which shares many of the biophysical characteristics of the cloned TRPM7 channel. RT-PCR confirmed that HLMC and LAD2 cells contain transcripts for TRPM7. The aim of the present work was to continue our characterisation of the TRPM7-like current and to examine these cells for the presence of further TRPM family members using RT-PCR. In our original whole cell patch experiments we used a simplified pipette solution (145 mM NaCl, 10 mM HEPES, 10 mM EGTA). Under these conditions the resting [Ca2+]i is decreased. We wished to examine whether [Ca2+]i influenced the amplitude or biophysical characteristics of the recorded current. To do this we used a pipette solution designed to buffer [Ca2+]i to about 100 nM. This recording solution would also allow us to determine whether our original currents were contaminated by a Ca2+ release activated Ca2+ current (ICRAC), as this current has been reported to be activated in rat basophilic leukaemia (RBL) cells when strong intracellular calcium chelation is used and suppressed when [Ca2+]i is buffered to about 100 nM. The size of the mean inward currents measured at −85 mV were not significantly different between the two pipette solutions (see table). Other parameters, such as the currents reversal potential, its sensitivity to block by La3+, inhibition by [Mg2+]i, cation selectivity, and augmentation under divalent-free external solution were also unaltered between the two pipette solutions. Thus recording TRPM7 in HLMC with strong Ca2+ chelation is unlikely to lead to a significant contamination of the current by ICRAC in contrast to the findings in RBL cells. This again demonstrates important differences between rodent model mast cells and primary human lung mast cells.
Abstract P220
RT-PCR experiments determined that LAD2 cells express transcripts for TRPM2, but not for TRPM1 or TRPM3-6. TRPM2 was also detected in HLMC. As TRPM2 channels have been shown to play an important role in the activation process of neutrophil granulocytes, this channel may be important for mast cell function. We are presently performing patch-clamp experiments to determine whether a TRPM2 current can be activated in HLMC.