Article Text

Statistics from Altmetric.com
Globally, the tuberculin skin test (TST), smear microscopy, and culture remain central to the diagnosis of tuberculosis (TB) because of the cost and ease of performance. However, TST has poor specificity and reduced sensitivity in settings including HIV and advanced TB,1 smear microscopy lacks sensitivity, and TB culture (the diagnostic gold standard) takes weeks and is positive in only two thirds of treated cases.2 TB pleuritis and peritonitis can be particularly difficult to diagnose due to paucity of bacilli and often need invasive or open procedures. In this setting, assays measuring interferon γ (IFN-γ) production by lymphocytes in response to TB antigens may be useful. While most studies have used blood based assays, more clinically relevant information may exist in local fluids such as bronchoalveolar lavage (BAL) fluid and pleural fluid in which much higher responses have been achieved.3–5
We investigated a 32 year old Somali man, resident in Britain for 2 years, who presented with a 3 week history of vomiting, diarrhoea, anorexia, and abdominal pain. On examination he was febrile (38.5°C), tachycardic, and tachypnoeic. No lymph nodes were palpable. A BCG scar was noted. He had signs of a right pleural effusion and ascites with peritonism.
A full blood count showed lymphopenia (0.26 × 106/l), normal neutrophils (3.6 × 106/l), hypochromic microcytic anaemia (Hb 10.7 g/dl), and a normal platelet count. Hyponatraemia (129 mmol/l (normal range 135–145)), hypoalbuminaemia (28 g/l (normal range 35–50), and mild hepatitis (aspartate transaminase 121 U/l (normal range 5–40)) were noted. Inflammatory markers were increased as follows: C reactive protein 280 mg/l; erythrocyte sedimentation rate 75 mm/h. An HIV antibody test was negative. A tuberculin skin test was not performed. The CT scan showed a moderate right pleural effusion and small left pleural effusion, small bowel dilation with mesenteric induration, large volume ascites, and small (<1 cm) mediastinal but no abdominal lymph nodes. On abdominal paracentesis, a leucocytosis of 640 cells/ml (75% lymphocytes) with 55 g/l protein and 3.8 mmol/l glucose was found but no organism was identified. The pleural fluid had a protein level of 36 g/l and a glucose level of 6.4 mmol/l.
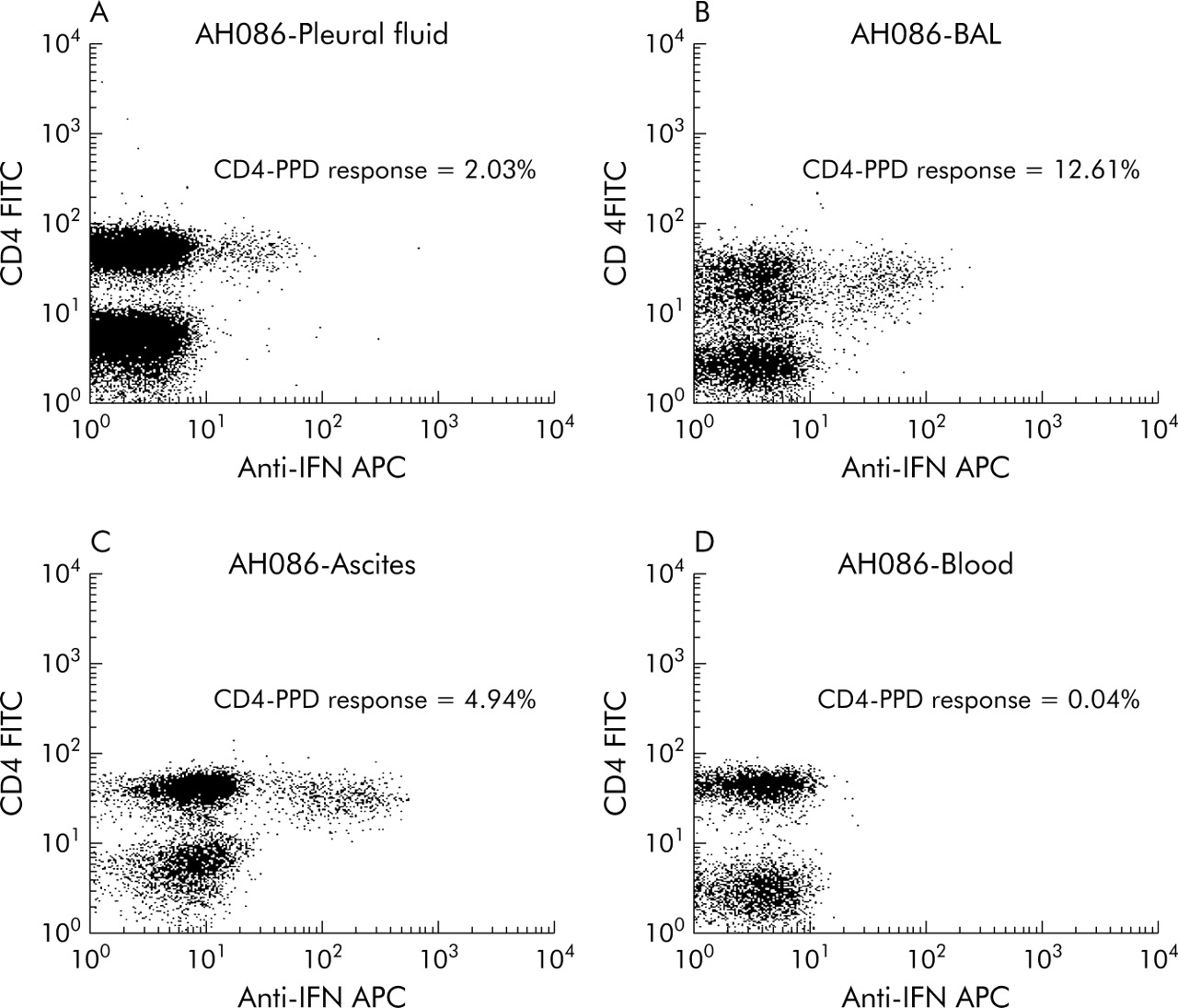
Bronchoalveolar lavage was performed. Auramine staining of sputum and ascitic, pleural, and BAL fluids was negative. Molecular assays (TB strand displacement assay) were negative from all sites. TB cultures were negative at 8 weeks. The pleural fluid, ascitic fluid, BAL fluid, and peripheral blood were examined for absolute leucocyte and lymphocyte numbers by flow cytometry, as well as lymphocyte phenotypes. The frequency of lymphocytes synthesising IFN-γ in response to purified protein derivative of Mycobacterium tuberculosis (PPD) was then measured as described previously.4 The percentage of lymphocytes in BAL fluid, ascitic fluid, and pleural fluid was 10.5%, 79.2%, and 91.1%, respectively. In CD3+ T cells the CD4/CD8 lymphocyte ratios in BAL fluid, ascitic fluid, pleural fluid, and blood were 1.5, 7.7, 2.7, and 2.1, respectively. In the CD4+ T cell populations the frequency of PPD specific IFN-γ positive lymphocytes in BAL fluid, ascites, pleural fluid, and blood was 12.61%, 4.94%, 2.03%, and 0.04% (fig 1).

{kind=link}
Proportions of interferon (IFN)-γ synthetic CD4+ T cells in response to purified protein derivative (PPD) after 16 hours of incubation in (A) pleural fluid, (B) bronchoalveolar lavage fluid, and (C) ascitic fluid of a patient with acute TB. These cells are virtually absent in the peripheral blood (D). In these flow cytometric assays the CD3+ T lymphocytes are gated and shown in the histograms. Of these, the CD4+ populations contain the IFN-γ positive cells (upper left quadrants) while the CD4− (CD8+) T cells are IFN-γ negative.
A presumptive diagnosis of tuberculous peritonitis was made. The patient was too unwell for exploratory surgery. Empirical antituberculosis treatment with rifampicin, isoniazid, ethambutol, and pyrazinamide was commenced with adjunctive corticosteroids which resulted in rapid resolution of his symptoms and signs. Corticosteroids were tailed off over a few weeks. He continues on rifampicin and isoniazid and remains well.
Although we were unable to obtain histological or microbiological confirmation of the diagnosis in this case, clinical and radiological evidence combined with the treatment response were highly suggestive of TB. The patient had marked lymphopenia which, in HIV negative TB patients, has been associated with advanced TB as well as decreased rates of smear positivity, an increased rate of extrapulmonary disease, and an attenuation of skin test reactivity.6 Hence, in a setting where traditional diagnostic tools are least effective, blood based immune assays are also likely to be suboptimal due to low CD4 counts and diminished response to antigens. The demonstration of high frequency lymphocyte responses in BAL fluid, pleural fluid and ascitic fluid, despite a negligible response in the blood as observed in our patient, is therefore of great clinical importance. We believe that this case highlights the potential usefulness of immune assays in TB with tissue fluids other than blood. Investigation of a larger patient cohort is warranted to delineate the responses seen in different stages of infection (such as latent and treated TB) and to determine clinically relevant cut off points which will allow these assays to be used as a diagnostic tool.