Article Text

Abstract
The case histories are presented of two patients in whom breathlessness developed following surgery to an anatomically distant site. Respiratory muscle testing demonstrated diaphragm weakness in both patients.
- diaphragm paralysis
- neuralgic amyotrophy
- respiratory muscles
Statistics from Altmetric.com
Diaphragm weakness due to medical intervention most commonly occurs as a result of physical trauma to the phrenic nerves or diaphragm muscle. Recognised examples include head and neck surgery or central venous catheterisation,1,2 as well as neuropraxia caused by the use of ice slush during cardiothoracic surgery.3
Postoperative brachial plexus neuropathy may occur in the absence of direct surgical trauma and it is recognised that the phrenic nerves may also be involved.4 However, isolated phrenic neuropathy following anatomically distant surgery has not been previously described. Here we present two patients in whom breathlessness developed following surgery to an anatomically distant site. Respiratory muscle testing demonstrated diaphragm weakness in both patients.
METHODS
The following common diagnostic techniques were used.
Spirometry
Forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) were recorded using a wedge bellows spirometer (Vitalograph, Buckinghamshire, UK).
Respiratory muscle tests
Global inspiratory and expiratory muscle strength was assessed with techniques described in the ATS/ERS joint statement on respiratory muscle testing5 using standard laboratory apparatus previously described elsewhere.6 In brief, maximum static inspiratory (MIP) and expiratory (MEP) mouth pressure were measured using a flanged mouthpiece attached to a short rigid tube with a two-way valve incorporating a 2 mm leak to prevent glottic closure. MIP was measured from residual volume (RV) and MEP from total lung capacity (TLC). Diaphragm strength was assessed as transdiaphragmatic pressure measured during a maximal sniff and by anterolateral magnetic phrenic nerve stimulation. This was performed using a Magstim 200 HP stimulator (Magstim Co, Whitland, UK) with a 45 mm coil placed over each phrenic nerve in turn to assess the strength of each hemidiaphragm and then bilaterally. Subjects rested for 20 minutes before stimulation to minimise twitch potentiation, then supramaximal stimulations were delivered at 100% power output while the patient was relaxed at FRC with the mouth closed and wearing nose clips. At least three satisfactory twitches were recorded for each patient.
Patient 1
A 46 year old man had an uncomplicated sigmoid colectomy for benign adenoma. Postoperative recovery was uneventful but 2 months later he became breathless and wheezy on exertion. The dyspnoea was particularly worse when lying on his back or immersed in water. He had no medical history of note and was a mild smoker. Chest radiography showed a raised right hemidiaphragm (see online supplement available at http://www.thoraxjnl.com/supplemental). No preoperative chest radiograph was available as a baseline for comparison, but a radiograph taken in the immediate postoperative recovery period shows the right hemidiaphragm to be normally positioned (image available in online supplement at http://www.thoraxjnl.com/supplemental).
Patient 2
A 58 year old woman was admitted to hospital for a clinically suspected pulmonary embolus. Ventilation-perfusion scanning showed a high probability for pulmonary embolism. She had had polio as a child but had not required respiratory support and 1 year before her admission she had had a normal chest radiograph. As part of the work-up for her pulmonary embolism she underwent ultrasound scanning of the abdomen. This revealed a tumour in the superior pole of the right kidney. She had a heminephrectomy 3 months later and histological examination confirmed renal cell carcinoma. Postoperatively she complained of breathlessness which was attributed to her anaesthetic. This breathlessness persisted and, as a result, she underwent CT pulmonary angiography and fibreoptic bronchoscopy. Neither of these investigations found a cause for her dyspnoea. One year later she still complained of shortness of breath on exercise, lying flat or bending forward. Physical examination showed paradoxical abdominal motion. A chest radiograph revealed an elevated left hemidiaphragm which was not present preoperatively (see fig 1 and online supplement).
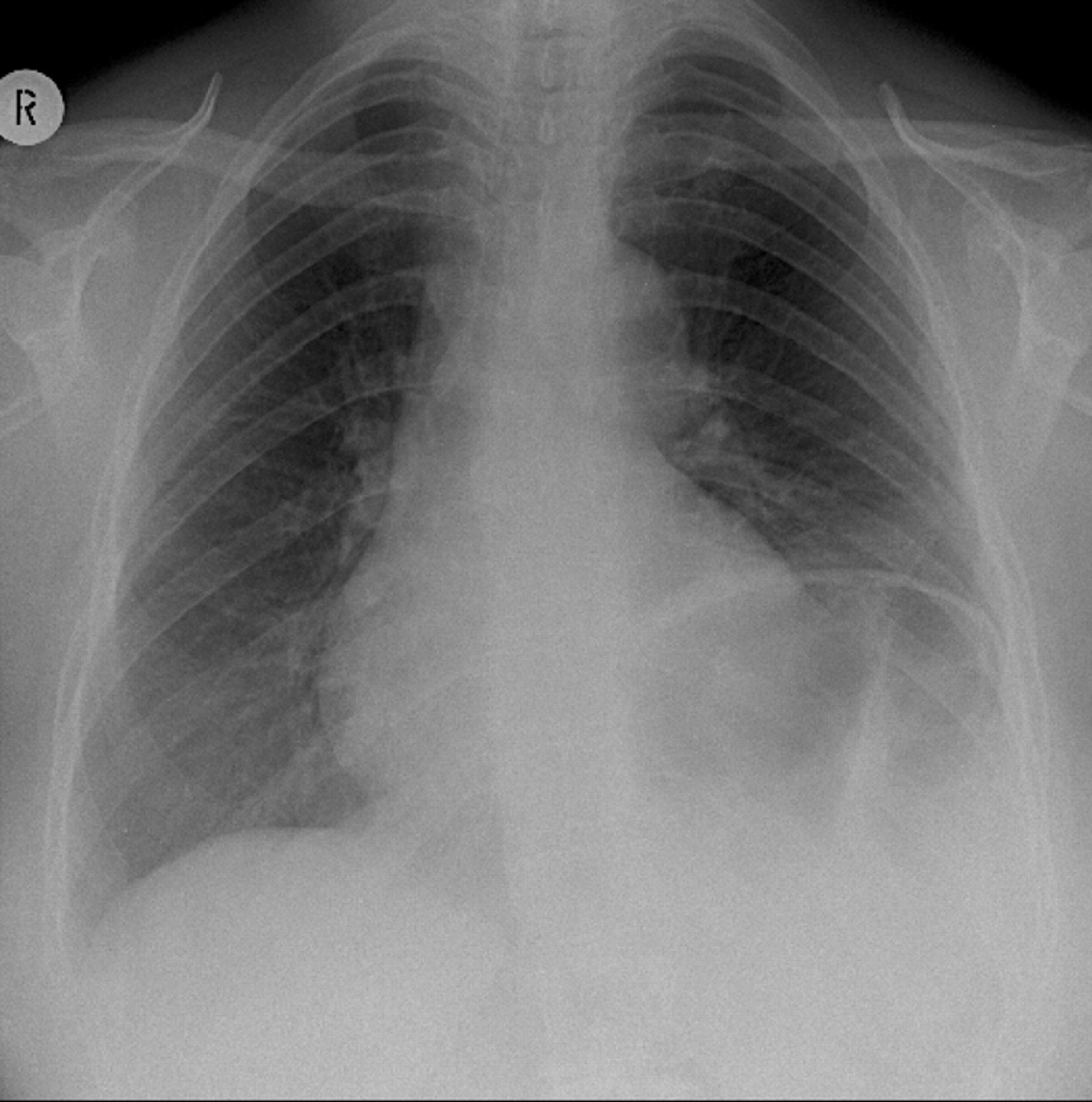
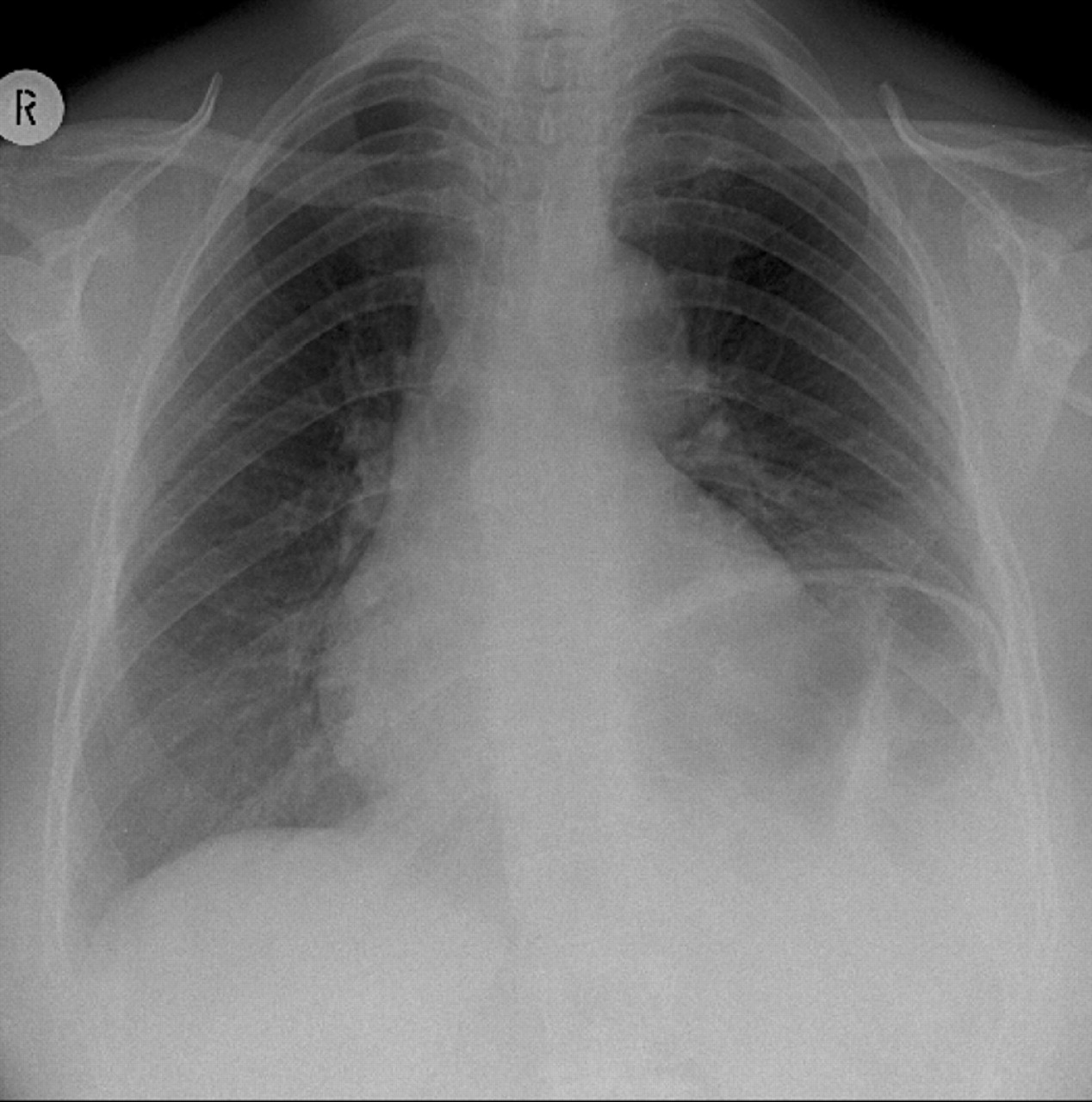{kind=link}
Raised left hemidiaphragm in patient 2.
RESULTS
Data for both these patients are shown in the tables in the online supplement available on the Thorax website at http://www.thoraxjnl.com/supplemental. The baseline characteristics and spirometric parameters are shown in table S1 and the results of respiratory muscle testing in table S2.
In addition to the radiograph in fig 1, the online supplement also contains a series of additional images. The first (fig S1) shows the raised hemidiaphragm in patient 1. In order to compare this and the chest radiograph of patient 2 (fig 1) with a “baseline”, three further radiographs are included as control images, one for patient 1 (fig S2) and two for patient 2 (figs S3 and S4).
The respiratory muscle tests for patient 1 showed global inspiratory and expiratory muscle strength within normal limits but sniff transdiaphragmatic pressure (SnPdi) was low at 43.4 cm H2O (normal >80). Magnetic phrenic nerve stimulation demonstrated right hemidiaphragm weakness with a right twitch transdiaphragmatic pressure (TwPdi) of 1.6 cm H2O (normal >7). The response to magnetic stimulation on the left was normal with a TwPdi of 10.5 cm H2O (normal >8).
Patient 2 had evidence of bilateral diaphragm weakness. Measurements of her global respiratory muscle strength were reduced and SnPdi was greatly reduced at 16.8 cm H2O. Magnetic stimulation of her phrenic nerves revealed a TwPdi on the left of 2.8 cm H2O and on the right of 1.7 cm H2O (normal ranges as above).
DISCUSSION
Both patients have shown clear evidence of a phrenic neuropathy and diaphragm weakness which was unilateral in patient 1 and bilateral in patient 2. The sites of the surgery were anatomically distant from the diaphragm so direct trauma to the diaphragm or the phrenic nerves was unlikely, and the weakness persisted long after the perioperative period when electrolyte disturbance7 or the administration of drugs with negatively inotropic properties8 might have contributed.
Occasionally diaphragm paralysis can occur following central venous cannulation. The immediate postoperative chest radiograph for patient 1 (fig S2) shows a right internal jugular catheter in situ. The diaphragm was normally positioned at this time, however, and symptoms did not appear until 2 months after this. We do not therefore believe that this line caused phrenic nerve injury and this impression is supported by such literature as is available which suggests that phrenic nerve damage occurs after difficult or traumatic central venous cannulation or where multiple attempts are made to locate the internal jugular, and that symptoms occur at the time of insertion.9,10
The control chest radiographs for patient 2 were taken at a time before her admission to hospital with a pulmonary embolism and after this admission for a pulmonary embolism. The first figure (fig S3) shows no evidence of a raised hemidiaphragm and thus, as a baseline image, it suggests that her history of polio as a child, which spared the respiratory muscles, had not affected her phrenic nerves. The second baseline radiograph (fig S4) was taken after the pulmonary embolism and shows evidence of a small pleural effusion in keeping with this diagnosis. Diaphragm paralysis is not associated with pleural effusions and therefore we believe it reasonable that the paralysis occurred after her surgery.
Neuralgic amyotrophy, however, is a condition which may account for the symptoms and signs seen in both patients after their surgery. It is a self-limiting condition of unknown aetiology characterised by a brachial neuropathy. Commonly, but not invariably, it is associated with pain in the shoulder region of sudden onset followed by weakness and wasting of the arm muscles in the distribution of the long thoracic, suprascapular, axillary and radial nerves.11 The phrenic nerves can become involved in neuralgic amyotrophy,4,12 but this is usually in conjunction with the “shoulder girdle” syndrome of pain described above. Rarely, isolated phrenic nerve involvement can occur, but anatomically distant surgery has not been previously described as a trigger for the condition.
In their original series which described brachial plexus neuralgic amyotrophy, Parsonage and Turner noted that nearly half the patients were already in hospital with other conditions.13 These included infections (such as malaria) and traumatic conditions (such as gunshot wounds). A minority of these, however, were patients recovering from surgery and, of those patients who did have a surgical trigger (12 of 136 cases), all had had anatomically distant surgery (usually hernia repair). As with our patients, neuralgic amyotrophy developed after surgery and diaphragm involvement was not noted in that series.
Patients with isolated phrenic neuropathy often initially present to chest physicians. Recovery of diaphragm strength is more variable than recovery of upper limb function and typically takes 2–5 years.12 Although no treatment is known to hasten recovery, identification of the condition is worthwhile if only to spare the patient unnecessary investigations. Plain chest radiographic appearances are a poor guide to diaphragm function and, where the diagnosis is suspected or in patients in whom a cause for breathlessness is difficult to discern, we recommend phrenic nerve stimulation be conducted to quantify diaphragm strength.