Article Text

Statistics from Altmetric.com
Mycobacterium kansasii is the second most common non-tuberculous mycobacterium associated with lung disease in the United States.1 Diseases are almost always cavitary, involving the upper lobes with fibrosis and infiltrations. Underlying pulmonary diseases associated with M kansasii infection include pneumoconiosis, chronic obstructive lung disease, AIDS and malignancy. To our knowledge, M kansasii has never been reported in the English literature in the aetiology of infected pulmonary sequestration. We report a case of intralobar sequestration complicated by infection with M kansasii.
A 33 year old man was previously healthy. An abnormal finding on the chest radiograph had been noted at a routine health check 1.5 years earlier. He had no history of medical illness and no risk factors for HIV infection. No symptoms attributed to his respiratory system, such as cough, haemoptysis or dyspnoea, were noted. Constitutional symptoms including malaise, fever, night sweats, anorexia, or weight loss were lacking. Physical examination revealed systolic bruit at the left basal lung. There was neither cyanosis nor digital clubbing. Oxygen saturation by pulse oximetry was 99% while breathing room air. Blood laboratory studies disclosed a white blood cell (WBC) count of 7.4×109/l (neutrophils 60.7%, lymphocytes 13.6%), and the level of carcinoembryonic antigen (CEA) was 1.33 ng/ml (reference value <3 ng/ml). Sputum acid-fast stain and mycobacterial cultures were all negative. Bronchoscopic examination showed no endobronchial abnormality. A chest radiograph taken at admission and a computed tomographic scan showed a patchy consolidation over the left basal lung. Magnetic resonance imaging (MRI) and angiography of the chest showed that an aberrant bronchial artery had arisen from the left side of the thoracic aorta and crossed the territory of the consolidation patch, but the venous drainage could not be visualised clearly (fig 1).

Magnetic resonance imaging (MRI) and angiography of chest showing the aberrant bronchial artery (arrow) arising from the thoracic aorta crossing the consolidation.
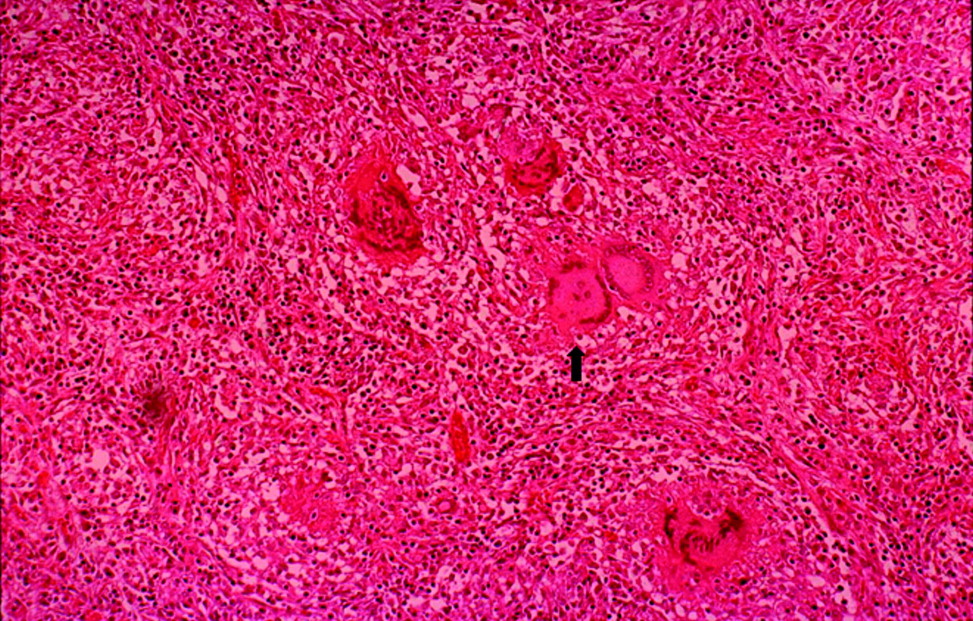
The patient underwent lobectomy of the left lower lobe by video-assisted thoracoscopic surgery (VATS). A 14×10 cm area of consolidation over the left lower lobe was noted and cystic formation and profuse sputum were found within the lesion. The three feeding arteries from the aorta at the level of the 10th thoracic spine were seen. Microscopically, the parenchyma revealed bronchiolitis and microabscess formation. Granulomatous inflammation was also present, but no organisms were identified by acid fast and Grocott’s methenamine silver (GMS) stains (fig 2). The biopsy tissue was ground and inoculated onto Lowenstein-Jensen slant (BBL Microbiology Systems, Cockeysville, MD, USA) and cultured at 35°C in a CO2 incubator. After 19 days of incubation the culture yielded a photochromogen which was later identified as M kansasii using conventional biochemical methods. The patient had an uneventful postoperative course and was discharged soon after operation. No anti-mycobacterial regimen was administered after the diagnosis was made and the patient’s clinical status remained uneventful at the 3 month follow up.
{kind=link}
{kind=link}
Microscopic section of the lung parenchyma showing microabscesses and granulomatous inflammation (arrow).
Pulmonary sequestration is a congenital malformation characterised by the presence of lung tissue with abnormal or absent communication with the bronchial tree and arterial blood supply from the systemic circulation. Despite the high frequency of infection, few data are available regarding specific infecting organisms. Acute infections due to bacteria such as Staphylococcus and Pseudomonas have been reported,2 and some chronic infections due to Aspergillus3 and Nocardia4 have also been described. Infected pulmonary sequestration due to mycobacteria including M tuberculosis5 and M avium-intracellulare6 have been reported only rarely. In our case, M kansasii was the first organism thought to be responsible for the infection of pulmonary sequestration in the absence of other pulmonary or extrapulmonary involvement. It is assumed that the organism reaches the sequestration through Kohn’s pore without causing evident disease in the normal lung parenchyma.
The combination of isoniazid, rifampin, and ethambutol was recommended for treatment of M kansasii pulmonary disease.1 However, surgical removal should be advocated in both asymptomatic and symptomatic cases of pulmonary sequestration and the benefit of a period of preoperative antimicrobial treatment in infected pulmonary sequestration has been debated.7 Our patient simply underwent a surgical resection and did not receive any anti-mycobacterial agents.
We have reported the unique occurrence of pulmonary sequestrartion with M kansasii infection. Surgical resection allows establishment of the exact diagnosis and immediate removal of the infectious focus, thus preventing complications related to the infection or to the malformation itself.