Article Text

Abstract
During the last decade several long term studies of interventions in patients with COPD have been published. This review analyses the potential of these interventions to alter the progression of the condition. The only treatment that has unequivocally been shown to reduce the rate of decline in FEV1 is smoking cessation. Active psychological intervention in combination with pharmacotherapy is required. Other treatments may have an effect on the rate of decline in FEV1 but this appears to be very small, at most. Several treatments affect the exacerbation rate and therefore might affect the progression of the disease. Further studies are warranted to examine this effect.
- COPD, chronic obstructive pulmonary disease
- FEV1, forced expiratory volume in 1 second
- FRC, functional residual capacity
- ICS, inhaled corticosteroids
- LAAC, long acting anticholinergics
- LABA, long acting β2 agonists
- 6MWD, six minute walking distance
- NAC, N-acetylcysteine
- ROS, reactive oxidant species
- chronic obstructive pulmonary disease
- progression
- smoking cessation
- treatment
- rehabilitation
Statistics from Altmetric.com
- COPD, chronic obstructive pulmonary disease
- FEV1, forced expiratory volume in 1 second
- FRC, functional residual capacity
- ICS, inhaled corticosteroids
- LAAC, long acting anticholinergics
- LABA, long acting β2 agonists
- 6MWD, six minute walking distance
- NAC, N-acetylcysteine
- ROS, reactive oxidant species
During the last years insight into the progression of chronic obstructive pulmonary disease (COPD) has increased considerably. This insight is largely derived from four large scale and long term studies on the effects of inhaled corticosteroids,1–4 and from large scale 1 year studies with tiotropium5,6 and with the combination of long acting β2 agonists and inhaled corticosteroids.7,8 These studies have unravelled a number of methodological problems associated with large scale long term studies which form the basis of the accompanying paper on assessment of progression of COPD.9 They also provided important information on the treatment of COPD and, as such, form the basis of current treatment and the widely used GOLD guidelines.
The effects of several treatments on the natural course of COPD have been examined in a number of large scale trials. Although the outcome of these has been negative in terms of affecting the progression of COPD, these trials have substantially enhanced our understanding of the natural evolution of the disease and the potential for effects of treatments. These trials unfortunately focused on patients with irreversible COPD, which was an important bias against observing an effect. Moreover, although the outcomes were largely negative in terms of affecting the progression of COPD as estimated by the annual decline in forced expiratory volume in 1 second (FEV1), there are several indications that treatments may affect variables that may be related to or affect the progression of COPD. They may therefore form the basis of research addressing this important question in the future.
The purpose of this paper is to review the potential of several treatment options available to patients with COPD to alter the natural course of the disease. The assessment of progression of COPD has been dealt with in a separate paper.9 This review will deal with the effects of intervention on the progression of COPD and discuss all the interventions that have been studied during the last decade. These include smoking cessation, long acting β2 agonists, long acting anticholinergic agents, inhaled steroids, combination products, antioxidants, and rehabilitation. For each of the treatments the potential of affecting the progression of COPD as discussed in the accompanying paper9—in terms of affecting the annual decline in FEV1, decline in health status, exacerbation rate, and mortality—will be highlighted. Effects on decline in functional status will only be discussed with rehabilitation as no data are currently available with other treatments. Effects on the increase in healthcare costs will not be discussed as at present only scanty data are available in this field.
Most of the effects shown by treatments are related to an effect on exacerbation rate. As discussed in the accompanying paper,9 exacerbations are really central to the progression of COPD. They are related to the decline in FEV1,10 progressive decline in health status,11,12 increased costs and hospitalization,9 and decline in functional status.13 As COPD worsens, the frequency and severity of exacerbations might increase.12 As will be discussed in this review, several treatments have been shown to have an effect on exacerbation rate.
SMOKING CESSATION
It has been clear for almost half a century that the main cause of COPD is smoking. It has become evident in the last decade that the most efficient treatment against COPD progression is smoking cessation. Two studies are of pivotal importance in this field. The first is the study by Doll et al on British doctors published in 1994 after 40 years of observation.14 The second is the Lung Health Study (LHS),15 a 5 year randomised trial which started in the US in 1986. This massive multicentre trial (nine US and one Canadian centres) enrolled 5887 adult smokers with mild to moderate COPD (FEV1 55–90% of predicted). Two thirds of the original participants were offered an intensive 12 week smoking cessation intervention. The British survey showed us the natural history of smoking in a selected population and the American trial demonstrated the effects of a specific smoking cessation intervention on the history of COPD among smokers who quit, tried to quit, or never quit. The study by Doll et al has shown that, besides lung cancer, smoking caused COPD and reduced life expectancy among doctors.14
This was shown to be true for less selected people as well. Fletcher et al16 showed that up to 26% of heavy smokers developed COPD among workers in London. Moreover, as the prevalence of smoking is rising in women and slightly decreasing among men, the sex distribution of COPD has shifted from 19% women in 1970 to 38.5% in 199317 and almost 50% in 2000.18,19
The Lung Health Study I (LHS I) has extensively demonstrated the efficacy of an intensive smoking cessation programme. This multi-component approach20 consisted of a cognitive-behavioural strategy including stimulus control, avoidance, role playing, assertiveness, training, reinforcement and relaxation techniques. The intervention group also received polacrilex nicotine 2 mg gum. The number of pieces of gum used by ex-smokers was 8–11 and less than 8 by continuing smokers. No cardiovascular illness or other serious side effects were reported.21 The validated (exhaled carbon monoxide and/or salivary cotinine level) 5 year sustained cessation rate was 22% in the intervention group compared with only 5% in the usual care group.22 Ipratropium bromide had no effect on the decline in FEV1.23
A follow up study at 11 years24 showed that 93% of participants who refrained from smoking throughout the LHS were still abstinent after this long period. At that time, 38% of continuing smokers had an FEV1 less than 60% of predicted compared with 10% of sustained quitters. The subgroup of intermittent smokers/quitters was also evaluated. Surprisingly, those who made several attempts to quit smoking had a smaller decline in lung function at comparable cumulative doses of cigarettes than those who continued to smoke.25 The fall in FEV1 was 0.23% predicted (27 ml) per year for quitters, 0.91% predicted (48 ml) per year for intermittent smokers, and 1.29% predicted (60 ml) per year for continuing smokers. Analysis by sex in the LHS showed that, among those with mild COPD, women appeared to benefit more from smoking cessation than men.26
The results of the LHS showed that smoking cessation is an effective way of altering the progression of COPD. Moreover, it is the only treatment that does this, in contrast to bronchodilators and inhaled corticosteroids (see below). We may assume from the LHS that any psychological and/or pharmacological approach of smoking cessation that gives a ±22% smoking cessation rate at 1 year among patients with mild to moderate COPD would achieve the same effects on lung function. The number of randomised studies on smoking cessation in patients with COPD is small; the results can be extrapolated from general population trials.
PHARMACOLOGICAL TREATMENT
Long acting β2 agonists
Bronchodilators are effective in the symptomatic treatment of COPD, and the main classes for maintenance treatment are anticholinergic agents and long acting β2 agonists (LABA). It is well established that LABA decreased symptoms such as breathlessness and daytime as well as night time symptoms in COPD.27–29 In addition, LABA have shown improvement in health status in some studies.30 Surprisingly, there was no clear dose-response effect.28,30 In recent studies where LABA have been compared with combination treatment there is some evidence that LABA as a single treatment may have a positive effect on health status.7,31 Studies on exercise capacity have also shown some evidence of improvement, but in long term studies the effect was small and often not significant. Surprisingly, a recent study with formoterol showed an inverse dose-response effect on exercise capacity.32
Whether LABA might affect disease progression is unclear. Firstly, there are no long term data showing an effect on mortality in COPD. Soriano and coworkers33 compared salmeterol treatment with a reference treatment in patients from general practices in the UK and found no indication of an effect on mortality. In contrast, inhaled corticosteroids as well as inhaled corticosteroids in combination with LABA were associated with a significantly lower mortality rate.33 Secondly, an effect on the long term decline in FEV1 has not been shown with LABA, but no studies have specifically addressed this question. There are few data comparing regular treatment with β agonists with on demand treatment showing that, in a 4 year perspective, these treatments did not differ in their effect on the decline in FEV1.34 One year trials with outcomes other than the decline in FEV1 have not shown any reduction in deterioration with LABA treatment.7,8,31
The question then arises whether it is theoretically possible that LABA could have a long term effect on the progressive deterioration in COPD. There are in vitro data indicating that LABA has anti-inflammatory effects, and no effect has so far been shown on the neutrophilic inflammation typical of COPD.35 An anti-oedema effect with LABA has been described in guinea pigs.36 Furthermore, salmeterol was shown to increase mucociliary clearance in normal subjects and in patients with bronchitis.35 However, at present none of these effects have been clearly shown to be present in patients with COPD and no effect on outcome variables has been seen in these patients.
Exacerbations are important in COPD and have a slight influence on the long term development of deteriorated airway function, together with a clear impact on the health status of the patients. Table 1 provides an overview of the effects of different treatments on the annual exacerbation rate in COPD. There is evidence that LABA could decrease the number of exacerbations. This is quite well shown for mild exacerbations but the evidence is scarce for an effect on severe exacerbations—that is, exacerbations leading to intervention with other treatment.7,8,31,37 The TRISTAN study showed an effect with salmeterol alone with a significant decrease of 20%. The effect was more pronounced in the more severe group with FEV1 below 50% predicted.8 No clear explanation for these observations is available. A potential explanation could be that LABA have a protective effect against damage in the mucosa by bacterial toxins.38 Together with inhaled corticosteroids, salmeterol has been shown to have a synergistic effect with fluticasone on bacterial colonisation.39 Formoterol also has a pro-inflammatory inhibitory effect in combination with a corticosteroid.40
Percentage reduction in annual exacerbation rate in major studies
Long acting anticholinergics
The long acting anticholinergic (LAAC) tiotropium bromide has recently become available. Two long term studies (1 year) of tiotropium versus placebo5 and ipratropium,6 respectively, have shown clinically beneficial effects on pulmonary function (without tolerance/tachyphylaxis developing), dyspnoea scores, use of rescue short acting β agonists, health related quality of life, COPD exacerbations, and hospital admissions for exacerbations (table 1). The additional costs of substituting tiotropium for ipratropium to achieve these favourable outcomes were estimated at €180 per patient per year.41 Currently, a 4 year maintenance treatment study comparing tiotropium with placebo in COPD patients (the UPLIFT study) is being conducted to assess its effect on the long term decline in lung function as well as on the morbidity and mortality rates. There are at least three indirect indications that signal the potential of tiotropium as a disease modifying agent. In the 1 year trials the decline in trough FEV1 was around 40 ml/year in the placebo group compared with about 10 ml/year in the tiotropium group.6 This may be due to residual bronchodilation lasting longer than 24 hours as the difference was substantially smaller if postbronchodilator FEV1 was considered. Tiotropium was shown to reduce the exacerbation rate and—in as much as exacerbations are related to the annual decline in FEV111,42—a reduction in the latter may be expected. Finally, the rate of deterioration in health status after an initial improvement appeared less with tiotropium than with ipratropium.5
Inhaled steroids
Data from early studies on the effects of inhaled corticosteroids (ICS) on the decline in FEV1 are limited and leave much room for different interpretations. Kerstjens et al43 showed an effect on both FEV1 and exacerbations. Less distinction between asthma and COPD was made than would be considered right according to present COPD guidelines. Distinction between asthma and COPD was more obvious in the smaller study by Renkema et al44 from 1996. Their study showed some effect of ICS on FEV1 but the power of the study was too limited. A pooled study by van Grunsven et al45 of the patients from the studies by Kerstjens et al43 and Renkema et al,44 together with a study published only as an abstract,46 has been published. This analysis showed an estimated 2 year difference in pre-bronchodilator FEV1 between subjects treated with ICS and placebo of 34 ml/year. This was statistically significant in spite of the fact that approximately one third of the originally included patients were excluded from the pooled analysis.45 The effect on post-bronchodilator FEV1 was less impressive and the time course of FEV1 did not fit with our general understanding of the time course of the decline in FEV1 in COPD. In a smaller Canadian study of 77 patients with COPD irreversible to systemic corticosteroids, Bourbeau et al47 found no effect of inhaled budesonide 1600 μg daily on FEV1, dyspnoea, or exercise capacity.
Four large placebo controlled trials of ICS in COPD have been conducted. The Copenhagen City Lung Study (CCLS)2 included 290 subjects with predominantly mild COPD from an ongoing epidemiological study. Patients were non-asthmatic subjects with a ratio of FEV1 to vital capacity (VC) of <0.7, irreversible to oral prednisolone and inhaled terbutaline. A total of 290 patients were randomised to either budesonide (800+400 μg daily for 6 months followed by 400 μg twice a day for 30 months) or placebo for 36 months. The study drug and placebo were given in the Turbuhaler. The mean age was 59 years, mean FEV1 was 2.37 litres (86% of predicted), 40% were women, and 77% were present smokers. The main outcome parameter was decline in FEV1, and crude declines in FEV1 turned out to be slightly smaller than expected (42 ml/year in the placebo group and 45 ml/year in the budesonide group). Using a regression model in the intention-to-treat population, patients in the placebo group had a decline in FEV1 of 49 ml/year compared with 46 ml/year in the budesonide group; the estimated difference 3.1 ml/year (95% confidence interval −12.8 to 19.0) was both statistically and clinically insignificant (p = 0.70). There was no initial rise in FEV1 in the budesonide group. No effect was seen on exacerbation rate.
The European Respiratory Society Study on Chronic Obstructive Pulmonary Disease (EUROSCOP)1 was a multicentre European study. EUROSCOP included patients with mild COPD who continued to smoke in spite of a 3 month smoking cessation programme including nicotine gum. A total of 1277 current smokers were randomised to either budesonide 400 μg twice daily or placebo, both given by Turbuhaler. The mean age was 53 years, 73% were men, and the mean post-bronchodilator FEV1 was 80% of predicted. There was a significant initial effect of inhaled budesonide on lung function. In the first 6 months the placebo group experienced a rapid decline in FEV1 of 81 ml/year, whereas the budesonide group had an increase in FEV1 of 17 ml/year. From 9 to 36 months both groups had a decline in FEV1: 69 ml/year in the placebo group and 57 ml/year in the budesonide group; the difference was not statistically significant (p = 0.39). After substratification according to pack-years of smoking there was a tendency towards an effect of budesonide in subjects with ⩽36 pack-years but the difference in decline from 9 to 36 months still did not reach statistical significance. No effect was seen on exacerbation rate.
The Inhaled Steroids in Obstructive Lung Disease in Europe (ISOLDE) study3 is the only one which has included patients with moderate to severe COPD, the mean FEV1 being 50% of predicted. A total of 751 patients were included and randomised to either fluticasone 500 μg or placebo in a metered dose inhaler via a Volumatic spacer twice daily. After randomisation all patients were immediately offered 2 weeks of treatment with oral prednisolone, 0.6 mg/kg once daily. The main effect parameter was decline in FEV1 and the secondary effect parameters were exacerbations, symptoms, and health status evaluated using the St George Respiratory Health Questionnaire (SGRQ). Only 219 patients in the fluticasone group and 182 in the placebo group completed the study; patients with more than three exacerbations within a 3 month period were excluded and this led to significantly more patients being excluded from the placebo arm. The course of lung function over the 3 years was almost similar to that seen in the EUROSCOP study except for the short term effect of oral prednisolone; the modelled declines in FEV1 were 50 ml/year in the fluticasone group and 59 ml/year in the placebo group. There was an overall reduction in number of exacerbations from 1.32 to 0.99 per year (p = 0.03, table 1). Most significantly, the gradual loss in health status was slower in the fluticasone group: 3.2 units per year in the placebo group compared with 2.0 units per year in the fluticasone group (p = 0.004). This decline, however, may not be representative of the normal decline which occurs in patients with COPD because it was preceded by an oral steroid trial, and it has been shown that such a trial substantially enhanced health status.50 Hence, the decline after a steroid trial will at least be partly due to withdrawal of steroids.
Finally, the Lung Health Study II has been published and confirms the findings of the previous studies.4 A total of 1116 patients with mild to moderate COPD were randomised to either triamcinolone 1200 μg or placebo in this multicentre trial including 10 clinical centres in the USA and Canada. As in the previous studies, no effect of inhaled steroids was seen on the decline in FEV1 (mean (SD) decline of 47 (3) ml/year in the placebo group and 44 (2.9) ml/year in the triamcinolone group). The effect increased somewhat with increasing compliance. The exacerbation rate was not considered specifically but there were fewer unscheduled visits to doctors in the triamcinolone group.
Three recent 1 year studies7,8,31 have included a placebo arm and an arm receiving ICS. All have included patients more or less comparable to those included in the ISOLDE study. They have all been too short to provide data on the decline in FEV1, but an effect on the exacerbation rate was seen in all three studies of the order of 15–35% depending on the severity of the exacerbations. All the studies were too short to examine decline in health status.
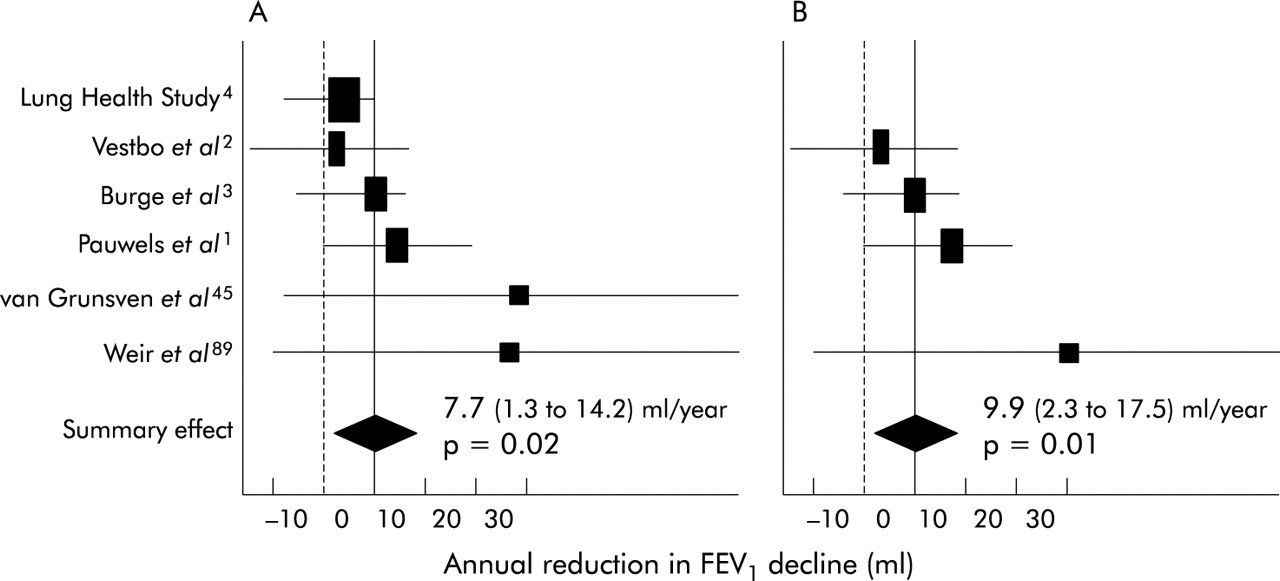
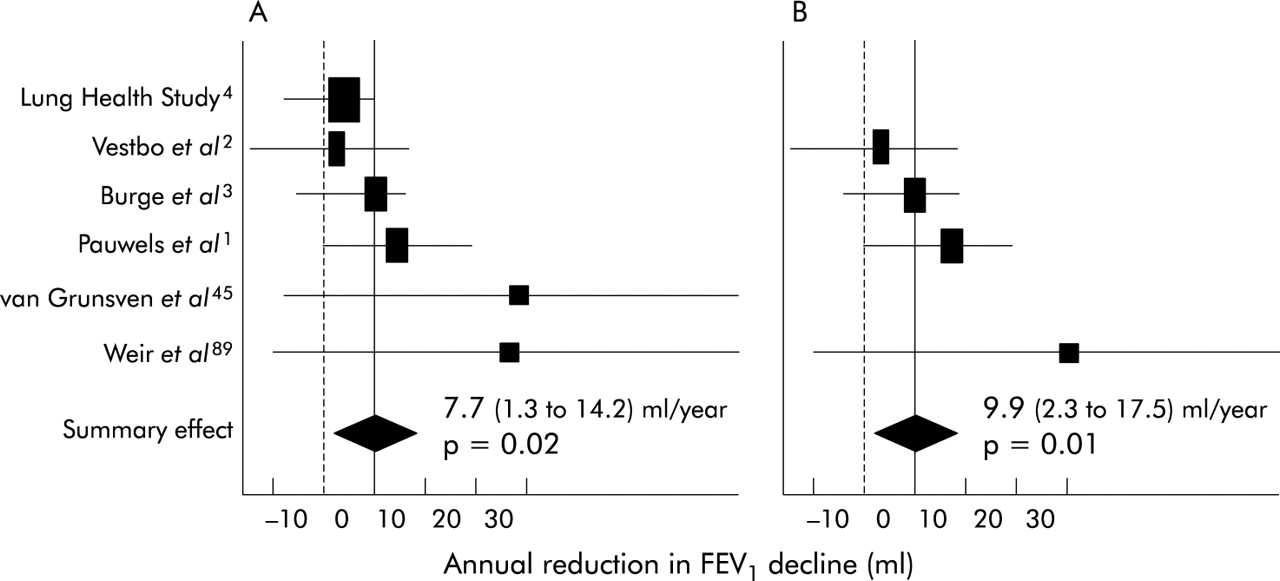
Three meta-analyses of ICS in COPD have been published and, although more or less based on the same studies, they come to somewhat different conclusions.48–50 The first of these studies found no statistically significant effect of ICS on FEV1 whereas the most recent meta-analysis50 showed that ICS reduced the rate of decline in FEV1 by 7.7 ml/year (95% CI 1.3 to 14.2). In high dose studies the effect was even larger: 9.9 ml/year (95% CI 2.3 to 17.5). Figure 1 summarises the results of this meta-analysis. Differences in values chosen for the analyses may explain some of the differences as the observed declines differ from the modelled declines in several studies. Would a true difference of 7.7 ml/year matter? Probably, in itself, this difference is small; all large studies conducted to date have arbitrarily chosen 20 ml/year as the minimal relevant difference. However, given the heterogeneity of COPD, an overall difference of 7.7 ml/year would indicate that groups of patients may experience a larger effect. Given the possible link between exacerbations and excess decline in FEV142,43 and the effect of ICS on exacerbation rate in patients with at least moderate COPD, it seems reasonable that the GOLD guidelines51 recommend ICS in patients with FEV1 <50% predicted and documented exacerbations.
{kind=link}
Meta-analysis of the effect of inhaled corticosteroids on the rate of decline in FEV1 in (A) all trials and (B) trials in which a high dose of inhaled steroids was given. From Sutherland et al.50
Treatment with the combination of LABA and ICS (LABA/ICS) improves symptoms and lung function and reduces exacerbations in patients with COPD (table 1). All three 1 year studies7,8,31 on the effect of LABA/ICS on FEV1 show that the initial improvement is maintained over the year. The duration of the studies is insufficient to judge the effect of this combination therapy on the long term decline in FEV1. The results of longer term studies such as the TORCH study will have to be awaited before any firm conclusion can be made in this respect.
Combination treatment has a long term beneficial effect on health related quality of life. In the TRISTAN study7 only the combination group (salmeterol/fluticasone) showed a clinically significant improvement in SGRQ total score by week 52. There were statistically significant differences in SGRQ total score with the combination compared with both placebo and fluticasone alone assessed over the 52 weeks. These differences and the difference with placebo at the end of the trial were small and did not reach the minimal clinically significant difference. In the study by Szafranski et al7 the combination of formoterol/budesonide significantly improved the SGRQ total score. The difference with placebo just failed to reach the clinically meaningful level of four points. In the study by Calverley et al31 patients were initially treated with oral corticosteroids and formoterol before being randomised to four study treatments. At the end of the 12 month treatment period the SGRQ total score was 7.5 points lower in the formoterol/budesonide group than in the placebo group. This difference, however, is at least in part determined by the oral steroid trial performed before randomisation (see above).
A retrospective analysis of the UK General Practice Research Database has suggested that treatment with the combination of salmeterol/fluticasone might improve survival in patients with COPD.33 The ongoing TORCH study is investigating prospectively whether this combination therapy has an effect on all cause mortality in COPD.
Antioxidants
Oxidative stress has been implicated in the pathogenesis and progression of COPD.52–55 Both reactive oxidant species (ROS) from inhaled cigarette smoke and endogenously formed ROS by inflammatory cells constitute an increased intrapulmonary oxidant burden. Attenuation of oxidative stress would be expected to result in reduced pulmonary damage and a decrease in local infections, thus contributing to attenuation of the progression of COPD. At present the only antioxidant widely available for treatment in patients with COPD is N-acetylcysteine (NAC). Its antioxidant properties and their relevance in relation to COPD have been recently reviewed.56
In an open observational survey in Sweden the decline in FEV1 in patients with COPD who took NAC for 2 years was less than in a reference group on usual care.57 This favourable effect was particularly apparent in patients over 50 years of age (annual decline in FEV1 of 30 ml) compared with the reference group (annual decline of 54 ml). After 5 years the decline in FEV1 in the NAC group was less than in the reference group (Lundbäck B et al, personal communication, 1993). Clearly, it should be noted that the nature of the study design precludes firm conclusions on the effect of NAC on lung function decline in COPD. In a multicentre, randomised, placebo controlled study (BRONCUS) in 523 patients, Decramer et al58,59 did not find an effect of NAC on the annual decline in FEV1 (54 (6) v 46 (6) ml/year) but, after 3 years, functional residual capacity (FRC) was decreased in the NAC group (−374 ml) but was slightly increased in the placebo group (+8 ml, p = 0.008). The significance of this effect on FRC, possibly related to a mucolytic effect on the small airways, still remains unclear. NAC did not affect the rate of decline in health status.
In a recent systematic review by Stey et al,60 data on prevention of exacerbations, improvement in symptoms, and adverse effects were extracted from original reports. The relative benefit and number needed to treat were calculated for both individual trials and combined data. Thirty nine trials were retrieved; 11 (2011 analysed patients) published between 1976 and 1994 were regarded as relevant and valid according to preset criteria. Except for one study, these were placebo controlled, randomised trials. In nine studies 351 of 723 (48.5%) patients receiving NAC had no exacerbation compared with 229 of 733 (31.2%) patients receiving placebo (relative benefit 1.56 (95% CI 1.37 to 1.77); number needed to treat 5.8 (95% CI 4.5 to 8.1)). There was no evidence for any effect of study period (12–24 weeks) or cumulative dose of NAC on efficacy. In five trials 286 of 466 patients (61.4%) receiving NAC reported improvement in their symptoms compared with 160 of 462 patients (34.6%) receiving placebo (relative benefit 1.78 (95% CI 1.54 to 2.05), number needed to treat 3.7 (95% CI 3.0 to 4.9)).
These findings are in line with the outcomes of two previous meta-analyses using a less precise selection of studies61,62 and confirm that NAC has a clinically significant effect on the number and impact of exacerbations (table 1). It should be pointed out that the majority of the abovementioned studies were performed before ICS were widely used in COPD. In the abovementioned randomised study the annual exacerbation rate was not influenced by NAC but it decreased significantly by 22% in patients not taking ICS (p = 0.0396).58,59 No effect was seen in patients taking ICS, indicating that the effects on the exacerbation rate do not appear to be additive. This is in line with the compilation of literature data shown in table 1. As can be seen, the maximal effects possible appear to be around 25% and most interventions produce similar effects. No additive effects were observed between LABA and ICS, or between ICS and NAC.
REHABILITATION
Besides airflow obstruction, COPD has been characterised as a disease with significant systemic impact.63,64 It is unknown how the systemic impact of the disease progresses over time. A few studies have looked at the decline in functional status in COPD. Three studies looked at the long term decline in walking distance. Bestall et al65 reported an annual decline in shuttle walking test of 23 m and Pinto-Plata et al66 reported a decline of 26 m in 6 minute walking distance (6MWD) in a group of patients followed up for 1.9 years. We found a decline of 25 m/year in 6MWD in patients followed up for 5.2 years.67 Consequently, it is expected that patients with COPD not submitted to rehabilitation programmes reduce their functional exercise capacity to a clinically relevant extent, 54 m every 2 years.68 This is in agreement with the reductions seen in health related quality of life, as observed in one large trial which investigated the effect of inhaled fluticasone in COPD.69 This decline, however, is likely to have been overestimated (see above).
Pulmonary rehabilitation programmes aim at tackling the systemic consequences of COPD. Exercise training programmes consistently improved health related quality of life and exercise tolerance.70 These changes are probably mediated through a significant improvement in skeletal muscle function.71–74 Changes are obtained after relatively short programmes but, especially in the more severe patients, longer programmes are needed.75 Although exercise training is considered the cornerstone of pulmonary rehabilitation programmes,76 these programmes have a comprehensive and multidisciplinary approach. Patients generally receive educational sessions and may receive psychological counselling, nutritional advice, occupational therapy, and self-management strategies may be practised.77,78
The question whether pulmonary rehabilitation is capable of altering disease progression remains largely unanswered. Indeed, no studies have investigated the impact of long term rehabilitation programmes over a period of time long enough to address disease progression. In the only study in which patients were followed up for 6 years, no effects were seen of a short (8 week) pulmonary rehabilitation programme on disease progression estimated by rate of decline in lung function, exercise tolerance, health status, and mortality.78 However, pulmonary rehabilitation may, under certain conditions, theoretically impact on the disease progression.
Firstly, the decline in FEV1 is enhanced by exacerbations of COPD.42,43 Exacerbations further reduce muscle force66,79 and health related quality of life.11 Pulmonary rehabilitation has been shown to reduce exacerbations80 and their severity significantly81 (table 1). When self-management programmes are part of the rehabilitation package, hospital admissions are avoided.82 Hence, through a reduction in exacerbation rate and hospital admissions, pulmonary rehabilitation may indirectly affect disease progression.
Secondly, pulmonary rehabilitation aims at improving activities of daily living in COPD. Whether pulmonary rehabilitation is successful at achieving this goal is not well studied, but circumstantial evidence and small studies suggest that patients may have a more active lifestyle after pulmonary rehabilitation.83,84 Since inactivity is one of the important contributors to skeletal muscle weakness64 and morbidity in COPD,85 rehabilitation programmes leading to significant “reactivation” of patients may be effective in altering disease progression. As reactivation is a behavioural modification, it is likely that this occurs only after long term interventions or regular reinforcement. Studies using long term interventions, indeed, generally show long lasting effects on health related quality of life and functional exercise capacity.71,80,86 We showed that 6 months of pulmonary rehabilitation improved 6MWD and health related quality of life and “stopped” the decline in both variables in the consecutive year of follow up.71 Shorter rehabilitation programmes lacking regular (e.g. weekly) reinforcement have, despite short term effects, more disappointing long term effects.87,88
CONCLUSIONS
The only treatment that was unequivocally shown to affect COPD progression is smoking cessation. Inhaled steroids may have a small effect on disease progression. Most treatments were clearly shown to offer symptomatic benefits. Several treatments reduce exacerbation rate by about 25% and may thus affect the progression of the disease. The effects of various treatments on exacerbation rate do not appear to be additive.
Acknowledgments
The authors acknowledge the expert secretarial assistance of Mrs C Ausseloos, Mrs E Lahousse and Mrs A Vandeborne.
REFERENCES
Footnotes
-
↵† Deceased.
-
This workshop was supported by GlaxoSmithKline-Belgium.
T Troosters is a postdoctoral fellow of the FWO-Vlaanderen.