Article Text

Statistics from Altmetric.com
A 74 year old man presented to hospital after waking with chest discomfort and haemoptysis, and left lung collapse was seen on the chest radiograph (fig 1). Twelve years earlier he had undergone laryngectomy and postoperative radiotherapy for laryngeal squamous cell carcinoma and had a permanent stoma. He had a smoking history of 35 pack years. New endobronchial malignancy was suspected, but bronchoscopy revealed the cause of his left sided airway obstruction to be a 4 cm beetle (fig 2)! Chest radiographs taken after removal of the beetle demonstrated lung re-expansion. The beetle was later identified as a Passalid beetle, species aulacocyclus, a species that resides in rotting logs.

Chest radiograph on presentation.

{kind=link}
{kind=link}
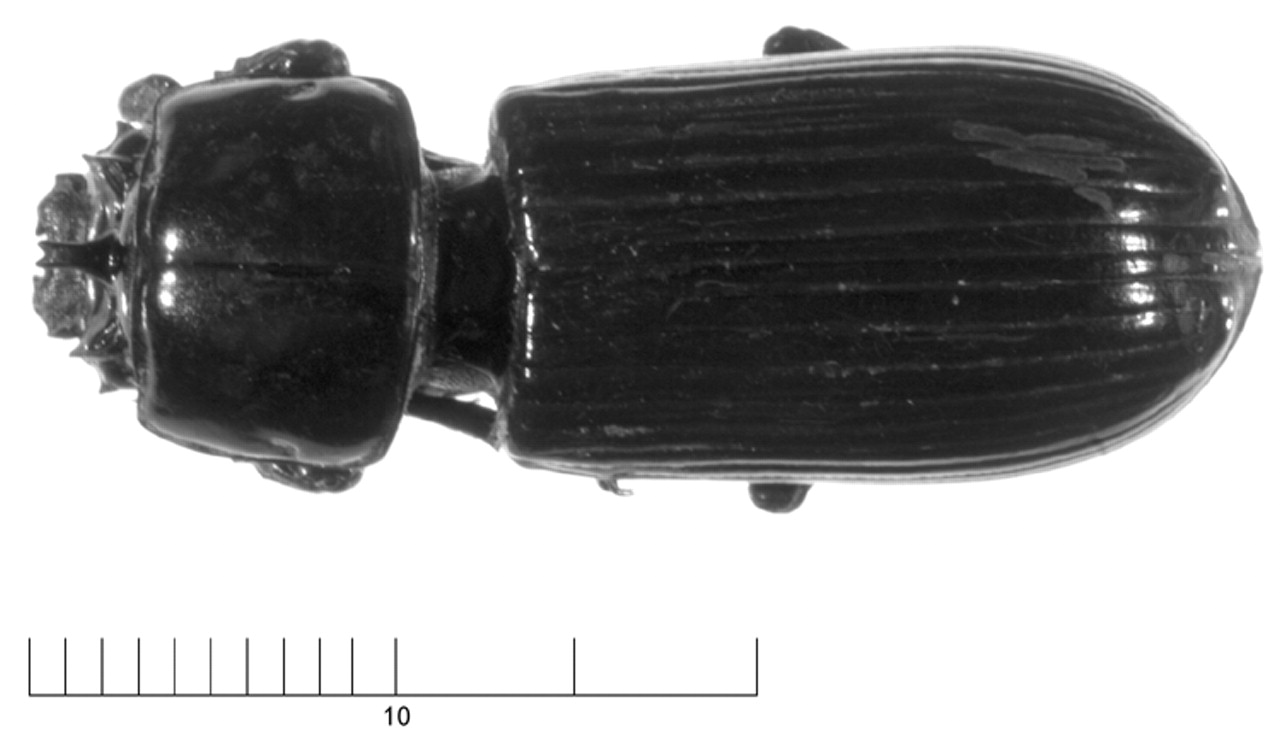
Passalid beetle.
During the day preceding his symptoms the patient had been working in his yard, chain sawing trees. It is likely that the beetle became attached to his clothing and that night crawled through his open tracheostomy while he was sleeping, becoming wedged in his left main bronchus. He subsequently awoke with the sensation of “something scratching in my chest”, a description only fully appreciated in retrospect.
Learning points
-
Foreign body inhalation in adults is rare, and even rarer when occurring via a permanent tracheal stoma.
-
Patients require education about the importance of ensuring adequate tracheal stoma care, even whilst asleep.
Despite the direct access provided to the tracheobronchial tree by a stoma, there are fewer than 10 reports of stomal foreign body inhalation.1 Inhalation through the more conventional oral route is also rare in adults and is usually related to underlying predisposing factors such as neurological impairment of protective airway mechanisms.2
Patients require education about the importance of ensuring adequate stoma care, even while asleep. Our patient has been advised to cover his stoma while sleeping. Although further unexpected Passalid beetle inhalation is highly unlikely, there are many other “creepy-crawlies” to beware in subtropical Australia!