Article Text

Statistics from Altmetric.com
We would like to congratulate Janssen-Heijnen et al1 on their well performed study and on their significant contribution to resolving the problem of treatment in patients with non-small cell lung cancer (NSCLC) and co-morbidity. However, we could not find a description of the surgical approach used and would like to ask the authors to provide details of the surgical procedures adopted and the accompanying survival rates. We think,2 in agreement with other authors3 that, for patients with early stage NSCLC and co-morbidity, a less invasive surgical approach should be used. This view is supported by studies in elderly patients or in patients with co-morbidity showing that a less invasive approach does not influence survival rates. Only the recurrence rate seems to be increased by a less invasive surgical approach such as segmentectomy or pulmonary wedge resection.3–5
Several factors determine whether conservative or invasive resection should be used for NSCLC. We think that a less invasive approach should be chosen as the first therapeutic step, even for early stage NSCLC, and that elderly patients should be treated less aggressively than younger patients.
References
Authors’ reply
We agree with Sortini and colleagues that the type of surgical procedure may influence survival. Several studies have shown that less invasive resections might be a good alternative for the elderly and those with co-morbidity because postoperative mortality and complications are rather high in these patients.1–5 We did not present survival rates for the different surgical approaches because the numbers of patients in the subgroups were rather small, especially for the less invasive resections like sleeve resection, segmentectomy, and wedge resection. However, at the request of Sortini and colleagues, we here present the results for the different surgical approaches.
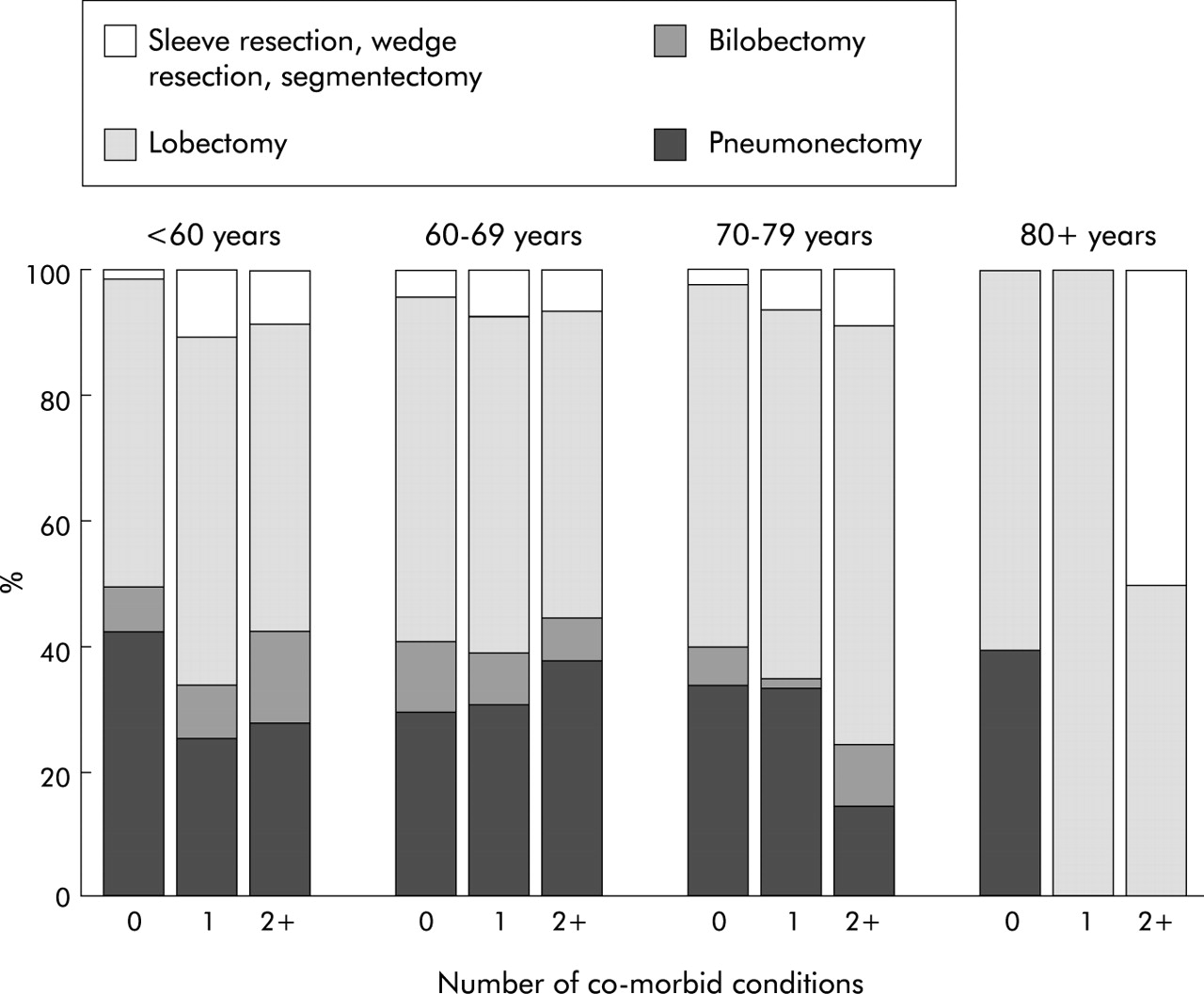
Figure 1 shows the proportional distribution of surgical approaches in resected patients with stage I and II NSCLC according to age and number of co-morbid conditions. Elderly patients received a pneumonectomy less often, while the proportion of lobectomies and less invasive resections increased with age. In age groups <60 years and 70–79 years patients with co-morbidity received pneumonectomy less often and a lobectomy/less invasive resections more often than those without co-morbidity. In patients older than 80 years the number of patients was too small to draw any conclusions.

{kind=link}
Surgical approach for surgically resected localised NSCLC according to age and co-morbidity.
In the multivariate survival analysis of resected stage I and II NSCLC patients, those treated with bilobectomy (HR = 0.70, p = 0.08) or lobectomy (HR = 0.70, p = 0.003) had a significantly better survival than those treated with pneumonectomy, adjusted for age, sex, tumour size, histological subtype, and co-morbidity. Survival in patients treated with less invasive resections was not significantly different. The absence of a difference might be explained by the small number of patients in this subgroup (n = 47).
We want to emphasise that this is an observational population based study and not a randomised controlled trial. Among the elderly, probably only the fittest patients were selected for surgery. Although we adjusted for the above mentioned patient related and tumour related factors in the multivariate survival analysis, other selection factors for surgery such as performance status, ASA score, forced expiratory volume in 1 second, and patient’s choice might have confounded the results.
Since the recurrence rate has been shown to be higher in patients who underwent less invasive surgery (such as wedge resection), lobectomy or pneumonectomy remain the surgical approaches of first choice in patients who are fit enough to undergo invasive surgery.4 Since it is still not clear what assessment is necessary in order to assess whether an older patient is fit enough for invasive surgery, future studies should focus on this topic.