Article Text

Abstract
Background: Proinflammatory cytokines stimulate osteoclast activity and this could lead to increased bone resorption in patients with cystic fibrosis. The aim of this study was to determine whether markers of systemic inflammation are related to changes in bone mineral content (BMC) in adults with cystic fibrosis.
Methods: Total body BMC was assessed by dual energy x ray absorptiometry in 100 patients (54 male) of mean (SD) age 25.6 (7.1) years and forced expiratory volume in 1 second (FEV1) 61.8 (24.1)% predicted on recruitment to the study and 1 year later. Blood was also taken at these time points to measure markers of systemic inflammation.
Results: After 1 year BMC had reduced by 16.1 (62.1) g, p = 0.01; (0.6 (2.8)%). The change in BMC was related to mean levels of interleukin (IL)-6 (rs = −0.39, p<0.001) and C reactive protein (rs = −0.34, p = 0.002), intravenous antibiotic use (rs = −0.27, p = 0.006) and oral corticosteroid use (rs = −0.20, p = 0.045). Urinary markers of osteoclast activity were also related to IL-6 (rs = 0.27, p = 0.02). Multiple linear regression revealed that IL-6 (coefficient –2.2 (95% CI –3.4 to –1.0) per pg/ml, p = 0.001), colonisation with Burkholderia cepacia (coefficient –46.8 (95% CI –75.5 to –18.1), p = 0.002), and annual change in BMI (coefficient 15.4 (95% CI 3.6 to 27.2) per kg/m2, p = 0.011) were independently significant predictors of annual change in BMC.
Conclusions: These data suggest a pathophysiological mechanism by which chronic pulmonary infection results in bone loss in patients with cystic fibrosis.
- BMC, bone mineral content
- BMD, bone mineral density
- BMI, body mass index
- BSAP, bone specific alkaline phosphatase
- CRP, Creactive protein
- FEV1, forced expiratory volume in 1 second
- IL-6, interleukin 6
- cystic fibrosis
- bone mineral content
- cytokines
- interleukin-6
Statistics from Altmetric.com
- BMC, bone mineral content
- BMD, bone mineral density
- BMI, body mass index
- BSAP, bone specific alkaline phosphatase
- CRP, Creactive protein
- FEV1, forced expiratory volume in 1 second
- IL-6, interleukin 6
Low bone mineral density (BMD) is prevalent in adults with cystic fibrosis.1–,4 The aetiology of low BMD in the cystic fibrosis population is multifactorial,5 but a consistent correlate of low BMD is cystic fibrosis disease severity.2–,4 The pathophysiology of this relationship is poorly defined but could be related to high circulating levels of proinflammatory cytokines. Concentrations of immunoreactive interleukin-6 (IL-6) are increased in patients with cystic fibrosis secondary to chronic pulmonary infection6,7 and this and other proinflammatory cytokines influence bone homeostasis.8,9 Work by Ionescu and colleagues in 22 adults with cystic fibrosis showed that BMD was related to forced expiratory volume in 1 second (FEV1) and to levels of IL-6 and tumour necrosis factor-α soluble receptors.10 These findings were supported by Aris and colleagues who found a temporal relationship between changes in inflammatory and bone metabolic markers during antibiotic treatment in 17 adults with cystic fibrosis.11 These studies suggest that pulmonary infection provokes an inflammatory response sufficient to affect bone metabolism in patients with cystic fibrosis. However, the pathophysiological mechanism for bone loss has not been explored longitudinally in a large cohort of patients.
The aim of this study was to determine whether markers of systemic inflammation are related to biochemical markers of bone turnover and changes in bone mineral content (BMC) over a 1 year period in adults with cystic fibrosis.
METHODS
Patients
The study population was derived from a cohort of 151 adults with cystic fibrosis who were participating in a prospective study documenting the natural history of cystic fibrosis related bone disease.2,12 Of the 123 patients who attended for measurements of total body BMC on recruitment to the study, 100 patients (54 male) re-attended for further BMC measurements a median (25–75% interquartile range (IQR)) of 12.0 (12.0–12.8) months later. The mean (SD) baseline total body BMC in patients with follow up BMC measurements was 2133 (390) g compared with 2086 (424) g in patients without follow up BMC measurements (p = 0.61). Of the 23 patients who were not rescanned, eight had died, four had received a double lung transplant, and 11 (9%) had chosen to withdraw from the study. The study was approved by the South Manchester research ethics committee and each patient provided informed written consent.
Bone mineral content measurements
Total body BMC was measured on recruitment to the study and at follow up by dual energy x ray absorptiometry (QDR 4500 Acclaim densitometer, Hologic, Bedford, Mass, USA). The short term precision for the total body BMC measurement, expressed as the coefficient of variation, was 0.92%. The BMC results were expressed as absolute values (in grams) from which the annual change and annual percentage change in BMC were calculated.
Biochemical measurements
Morning blood and urine samples were taken from patients on recruitment to the study and at follow up, at a time when their lung disease was stable—that is, not prescribed oral or intravenous antibiotics for the treatment of a pulmonary exacerbation. Urine samples were not necessarily first void as participants attended as outpatients from all over the North West region. Plasma IL-6 levels were measured using Quantikine immunoassays (R&D Systems Europe Ltd, Abingdon, UK) and the intra- and inter-assay coefficients of variation were 2.6% and 4.5%, respectively. The sensitivity of the assay was 0.7 pg/ml (range 3.1–300). Serum concentrations of C reactive protein (CRP), osteocalcin, bone specific alkaline phosphatase (BSAP), and urinary deoxypyridinoline crosslinks were measured as described previously.2
Clinical assessment
The best recorded FEV1, weight, and height in the 4 months before the recruitment and follow up visits were used to calculate the percentage predicted FEV113 and body mass index (BMI). Sputum microbiology and prescriptions of inhaled corticosteroids, oral corticosteroids, nebulised antibiotics and intravenous antibiotics were recorded throughout the study as these factors could modify the inflammatory response to infection. Levels of physical activity were assessed using the Baecke questionnaire which scores levels of physical activity from a minimum of 3 to a maximum of 15, as described previously.2
Statistical analysis
Data were analysed using SPSS version 9.0 (SPSS Inc, Chicago, IL, USA) and variables were summarised using the mean (SD) or median (25–75% IQR). The annual change in BMC was calculated for each patient to correct for the varying time between recruitment and follow up. For the biochemical indices of bone turnover together with CRP and IL-6, the mean value of the two readings obtained from each individual was used for statistical analysis. A one sample t test was used to determine whether the annual change in BMC was significantly different from zero. The independent samples t test or the Mann Whitney U test was used to determine differences between patient groups. Spearman’s rank correlations were performed to explore the relationship between markers of systemic inflammation, markers of bone turnover, and the change in BMC over 1 year. Linear regressions (single and multiple variables) were used to characterise the relationship between the annual change in BMC (dependent variable) and the following predictors: age at baseline, sex, B cepacia colonisation, daily prednisolone use, annual antibiotic use, annual change in BMI, annual change in FEV1, and mean concentrations of IL-6, CRP, deoxypyridinoline crosslinks, osteocalcin, and BSAP. Forward and backward selection methods were used to identify independent predictors in the multiple variable model. Residuals were examined to check for normality.
RESULTS
Patient characteristics
None of the patients included in this analysis were taking any specific bone sparing agents and none had received a transplant. Four patients were pancreatic sufficient and all pancreatic insufficient patients were prescribed 22.5 μg (900 IU) of oral vitamin D (calciferol) daily, but seven patients admitted to not taking their vitamin supplements on a regular basis. Sixty one patients were homozygous for the delta F508 genotype, 31 patients were heterozygous for the delta F508 genotype, and eight patients had another genotype.
On recruitment to the study the mean (SD) age, percentage predicted FEV1, BMI, and physical activity score of the patients were 25.6 (7.1) years, 61.8 (24.1)%, 21.3 (2.3) kg/m2 and 7.8 (1.3), respectively. Over the follow up period the mean (SD) annual change in FEV1 and BMI were –2.1 (8.2)% predicted (p = 0.01) and 0.2 (1.1) kg/m2 (p = 0.05), respectively. There was no significant change in the physical activity score over the follow up period.
Seventy three patients were colonised with Pseudomonas aeruginosa, 22 patients were colonised with B cepacia and five patients were colonised with Staphylococcus aureus, Haemophilus influenzae or no organism. Of the 73 patients colonised with P aeruginosa, 38 were prescribed daily nebulised antipseudomonal antibiotics (colomycin or gentamicin). In the whole group over the follow up period the median (25–75% IQR) intravenous antibiotic usage was 23 (0–58) days per year. Twenty six patients received no intravenous antibiotic therapy and, in the remaining 74 patients, the median (25–75% IQR) intravenous antibiotic usage was 38 (19–71) days per year.
Nine patients were prescribed long term continuous oral corticosteroids (prednisolone 5–15 mg daily) during the follow up period, three for allergic bronchopulmonary aspergillosis and six for unstable lung disease. In the whole group the median (25–75% IQR) oral corticosteroid usage during the follow up period was 0.6 (0.0–2.3) mg prednisolone per day. Thirty six patients received no oral corticosteroid therapy and in the remaining 64 patients the median (25–75% IQR) oral corticosteroid usage was 1.6 (0.7–4.3) mg/day. Sixty eight patients had been prescribed inhaled glucocorticoid therapy (budesonide 200–400 μg twice daily or fluticasone propionate 250–500 μg twice daily).
Biochemical results
Blood and urine samples were taken at the recruitment and follow up visits from 75 of the 100 patients who re-attended for dual energy x ray absorptiometry. There was no significant difference in baseline BMC between patients with (2136 (399) g) and without biochemical data (2121 (371) g, p = 0.87). Due to the inherent variability of the inflammatory and bone biochemical markers, averaged values from the recruitment and follow up visits were calculated. The median (25–75% IQR) concentrations of these variables were: IL-6 5.5 (2.6–11.5) pg/ml (normal range 0.2–2.9 pg/ml, fig 1⇓), CRP 10.3 (5.0–26.8) mg/l (normal range <15 mg/l), BSAP 18.3 (15.3–24.4) U/l (normal range 10.0–23.0 U/l), osteocalcin 9.5 (7.1–11.6) ng/ml (normal range 3.4–10.0 ng/ml), and deoxypyridinoline crosslinks 6.1 (4.7–8.2) nM/mM (normal range 2.3–7.4 nM/mM).

Mean interleukin-6 concentrations in 75 adults with cystic fibrosis (mean value for each patient calculated from the baseline and follow up measurements; dashed lines denote the upper and lower limits of the normal range).
The urinary excretion of crosslinks was positively related to IL-6 (rs = 0.27, p = 0.02) but was not related to any other clinical or biochemical indices of systemic inflammation. Bone formation, as measured by bone specific alkaline phosphatase and osteocalcin, was not related to any of the indicators of inflammation.
Median (25–75% IQR) levels of IL-6 were significantly higher in patients colonised with B cepacia (9.5 (5.2–19.5) pg/ml) than in those colonised with P aeruginosa (4.7 (1.9–9.0) pg/ml), p = 0.01. However, there was no significant difference in the CRP, annual intravenous antibiotic use, oral corticosteroid use, levels of physical activity, change in FEV1, or change in BMI between these microbiological groups (table 1⇓).
Biochemical markers of systemic inflammation, clinical characteristics, and annual change in bone mineral content in cystic fibrosis patients infected with Pseudomonas aeruginosa and Burkholderia cepacia
Men had significantly higher median (25–75% IQR) levels of IL-6 (7.2 (4.1–13.6) pg/ml) than women (3.9 (1.8–6.4) pg/ml, p = 0.007). Men also had significantly higher levels of CRP (20.0 (7.5–28.0) mg/l) than women (5.5 (5.0–23.5) mg/l, p = 0.01). However, there was no significant difference in annual intravenous antibiotic use, oral corticosteroid use, levels of physical activity, change in FEV1, or change in BMI between men and women (table 2⇓).
Biochemical markers of systemic inflammation, clinical characteristics, and annual change in bone mineral content in men and women with cystic fibrosis
Bone mineral content results
The mean (SD) total body BMC on recruitment to the study was 2133 (390)g in the whole group, 2311 (367)g in male patients and 1919 (303)g in female patients. The mean (SD) annual change in total body BMC was –16.1 (62.1) g in the whole group (p = 0.01), −22.5 (75.1) g in men (p = 0.03) and –8.4 (41.2) g in women (p = 0.18). The mean (SD) annual percentage change in total body BMC was –0.6 (2.8)% in the whole group (p = 0.03), −0.8 (3.3)% in men (p = 0.07) and −0.4 (2.2)% in women (p = 0.21).
The mean (SD) annual reduction in BMC was significantly greater in patients colonised with B cepacia (−64.7 (67.6) g) than in those colonised with P aeruginosa (−3.0 (54.0) g), p<0.001. In the patients colonised with P aeruginosa there was no difference in the annual change in BMC between those prescribed and those not prescribed nebulised antibiotics. In the whole group there was no significant difference in the annual change in total body BMC between patients prescribed oral corticosteroids or inhaled corticosteroids and those not.
The percentage predicted FEV1 (rs = 0.21, p = 0.04) and BMI (rs = 0.32, p = 0.001) at the time of recruitment to the study were significantly related to the baseline total body BMC, which confirms the cross sectional relationship between clinical markers of cystic fibrosis disease severity and BMC. The annual change in BMI was weakly related to the annual change in BMC (rs = 0.20, p = 0.05) but there was no relationship between the annual change in FEV1 and the annual change in BMC (rs = −0.05, p = 0.65).
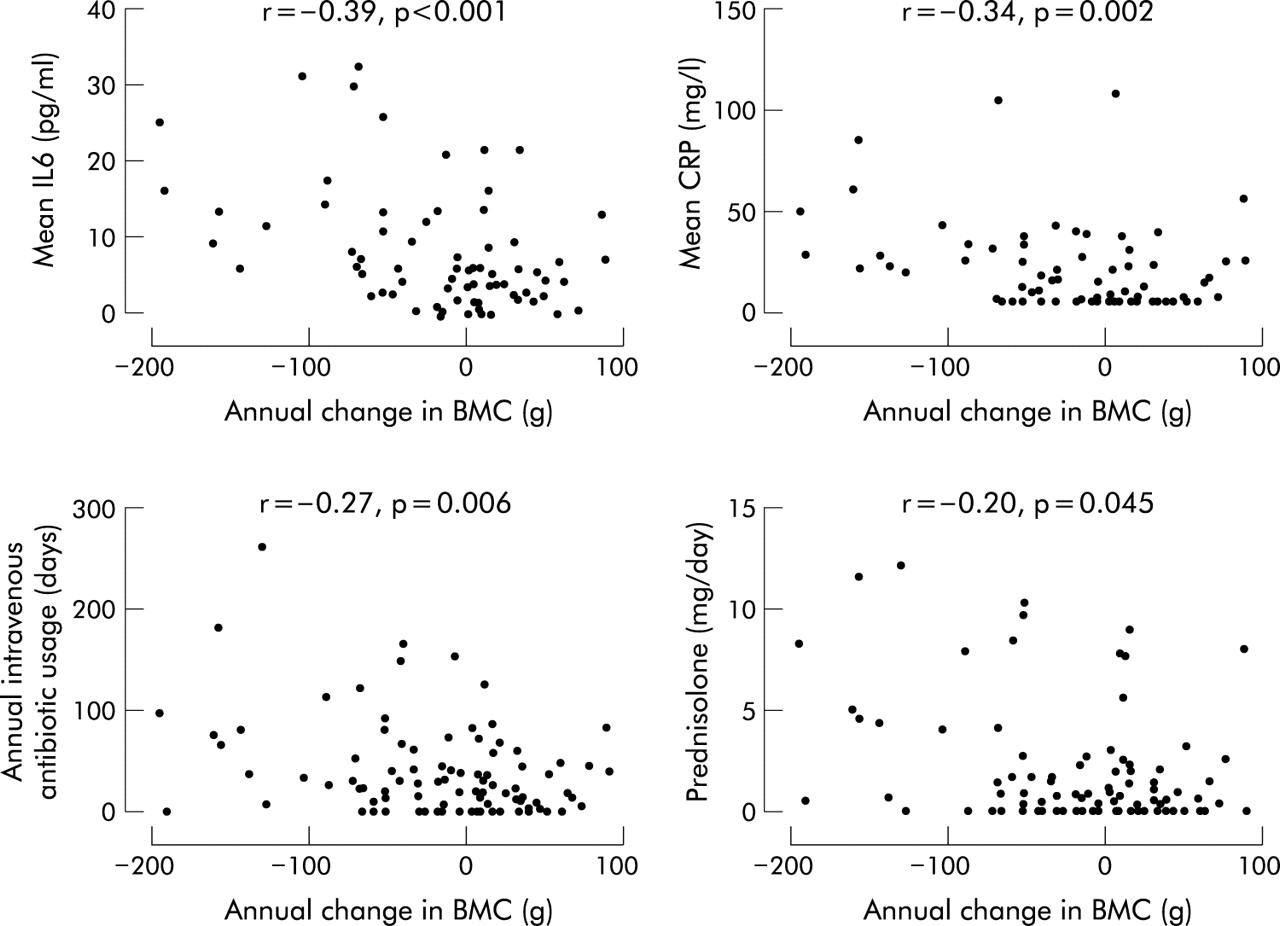
There were significant relationships between the change in total body BMC and the markers of systemic inflammation (fig 2⇓). In the univariate analysis there was a significant negative relationship between change in total body BMC and mean levels of IL-6 (rs = −0.39, p<0.001) and CRP (rs = −0.34, p = 0.002). There was also a significant negative relationship between change in total body BMC and the clinical indicators of systemic inflammation—namely, days of intravenous antibiotic use (rs = −0.27, p = 0.006) and oral corticosteroid use (rs = −0.20, p = 0.045). Mean levels of physical activity were not related to change in total body BMC. When multiple linear regression analysis was used to allow for the interrelationships between variables, IL-6 (coefficient −2.2 (95% CI –3.4 to –1.0) per pg/ml, p = 0.001), colonisation with B cepacia (coefficient −46.8 (95% CI −75.5 to −18.1), p = 0.002), and the annual change in BMI (coefficient 15.4 (95% CI 3.6 to 27.2), p = 0.011) were independently significant predictors of annual change in BMC. Sex was not a significant predictor of annual change in BMC.

{kind=link}
{kind=link}
Univariate relationship between change in total body bone mineral content (BMC) and the mean concentration of interleukin (IL)-6, mean concentration of C reactive protein (CRP), annual intravenous antibiotic use, and oral prednisolone use.
DISCUSSION
The results of this 1 year prospective study suggest that bone loss is related to systemic inflammation in adults with cystic fibrosis. Although the aetiology of low bone mass in this patient population is multifactorial,5 the inverse relationship between change in BMC and the mean concentrations of IL-6 and CRP strongly supports the inflammatory hypothesis of bone loss in cystic fibrosis. The significant positive relationship between IL-6 and the urinary excretion of deoxypyridinoline crosslinks suggests that IL-6 stimulates osteoclastic bone resorption in patients with cystic fibrosis, thereby providing a pathophysiological mechanism by which chronic pulmonary infection results in bone loss in this patient population.
The relationship between low BMC and cystic fibrosis disease severity could be explained by other factors such as corticosteroid use and immobility. However, the relatively weak association in the univariate analysis between the annual change in BMC and oral corticosteroid use suggests that this was not the major factor. There was also no significant relationship between mean levels of physical activity and change in total body BMC. Regression analysis showed that mean levels of IL-6 and change in BMI were significant predictors of change in total body BMC, and these findings are consistent with those of Ionescu, who showed that patients with high concentrations of immunoreactive IL-6 had low fat free mass.10 This suggests that the systemic inflammatory response to infection adversely effects muscle mass as well as skeletal mass in patients with cystic fibrosis.
Patients colonised with B cepacia had a greater inflammatory load and sustained a greater loss of bone mass than patients colonised with P aeruginosa. Furthermore, B cepacia colonisation was an independent predictor of the annual change in BMC. These data indicate that adult patients with B cepacia have a particularly high risk of developing osteoporosis. Male patients had higher inflammatory indices than female patients and there is no clear explanation for this as there were no sex differences in baseline FEV1, change in FEV1, or intravenous antibiotic use. However, this unexpected finding might explain the trend towards a higher rate of bone loss in male patients within this cohort.12
The longitudinal changes in total body BMC suggest that bone turnover is abnormal in patients with cystic fibrosis and these data are consistent with our previous findings documenting site specific changes in BMD in the lumbar spine and proximal femur.12 As peak bone mass is normally achieved between the middle and end of the third decade of life, the 0.6% annual reduction in total body BMC in this young adult cohort suggests that patients with cystic fibrosis reach peak bone mass at a younger age. This is likely to be a causative factor in the increased fracture rate documented in patients with cystic fibrosis.1,4
Although we have shown that mean levels of IL-6 are related to markers of bone resorption and change in BMC over a 1 year period, we have not proved a causal relationship between systemic inflammation and bone loss. Furthermore, we have only assessed levels of systemic inflammation at two time points which may not accurately reflect the level of systemic inflammation throughout the year. However, we have studied a large number of patients and found biologically meaningful results which support and extend the findings of previous studies investigating the inflammatory hypothesis of bone loss in patients with cystic fibrosis.10,11 IL-6 has also been implicated in the pathophysiology of several other diseases characterised by increased osteoclastic bone resorption including rheumatoid arthritis,14 inflammatory bowel disease,15 hyperparathyroidism,16 and Paget’s disease.17
In conclusion, the mean concentration of immunoreactive IL-6 was significantly related to biochemical markers of osteoclastic bone resorption and to the change in total body BMC over 1 year. These data provide a pathophysiological mechanism by which chronic pulmonary infection results in bone loss in this patient population. The 0.6% annual reduction in total body BMC suggests that peak bone mass is achieved at an earlier age than normal in patients with cystic fibrosis. The concentration of IL-6, colonisation with B cepacia, and change in BMI were independent predictors of bone loss over 1 year.
Acknowledgments
The authors thank S Hill for performing the cytokine assays, E B Mawer’s laboratory for performing the bone turnover marker assays, and D Ledgeton, M Hodgkinson, C Alsop and R Larder for performing the bone densitometry measurements.
REFERENCES
Footnotes
This study was funded by the Cystic Fibrosis Trust.
Linked Articles
- airwaves