Article Text

Abstract
Background: The Boston Early-Onset COPD study showed that current or ex-smoking first degree relatives of severe early onset COPD probands have significantly lower forced expiratory volume in 1 second (FEV1) and FEV1/forced vital capacity (FVC) values than current or ex-smoking control subjects, which suggests the existence of genetic risk factors for the development of COPD in response to cigarette smoking. We hypothesised that first degree relatives of early onset COPD probands may also have lower values of spirometric parameters such as forced expiratory flow at the mid-portion of forced vital capacity (FEF25–75) and FEF25–75/FVC.
Methods: Using generalised estimating equations, FEF25–75 and FEF25–75/FVC were analysed in 333 first degree relatives of probands with severe early onset COPD and 83 population based controls; analyses were also performed on data stratified by smoking status. Narrow sense heritability estimates were calculated using a variance component approach.
Results: Significantly lower FEF25–75 and FEF25–75/FVC were observed in smoking (FEF25–75: β −0.788 l/s (95% CI −1.118 to −0.457), FEF25–75/FVC: β −20.4% (95% CI −29.3 to −11.6, p<0.0001 for both phenotypes) and non-smoking (FEF25–75: β −0.357 l/s (95% CI −0.673 to −0.041, p = 0.0271), FEF25−75/FVC: β −9.5% (95% CI −17.1 to −1.9, p = 0.0145)) first degree relatives of early onset COPD probands. Narrow sense heritability estimates for FEF25–75 (h2 = 0.38) and FEF25–75/FVC (h2 = 0.45) were similar to those for FEV1 and FEV1/FVC.
Conclusion: Lower values of FEF25–75 and FEF25–75/FVC in non-smoking first degree relatives of early onset COPD probands than in controls suggest a genetic susceptibility to develop obstructive lung disease, independent of smoking, which is magnified by exposure to deleterious environments as suggested by the further decrements in FEF25–75 and FEF25–75/FVC seen in smoking first degree relatives. FEF25–75 and FEF25–75/FVC have high heritability and are important intermediate phenotypes for inclusion in genetic epidemiological studies of COPD.
- chronic obstructive pulmonary disease
- smoking
- genetics
- lung function
- FEF25–75, forced expiratory flow at the mid-portion of forced vital capacity
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
Statistics from Altmetric.com
- FEF25–75, forced expiratory flow at the mid-portion of forced vital capacity
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
Chronic obstructive pulmonary disease (COPD) is one of the leading causes of morbidity and mortality in the United States. Although cigarette smoking is the major risk factor for COPD, the variable development of COPD in smokers and the occasional development of COPD in non-smokers suggest that influences other than cigarette smoking are probably important. Genetic contributions to pulmonary function have been supported by both studies in the general population1 and twin studies.2–4
Familial aggregation of and genetic contributions to COPD, a disease characterised by obstructive abnormalities in pulmonary function, have been extensively investigated. Several early studies showed an increased prevalence of airflow obstruction in first degree relatives of individuals with COPD compared with control subjects.5–7 More recently, our group has investigated the risk of airflow obstruction in first degree relatives of probands with severe early onset COPD.8 An overall decrement in forced expiratory volume in 1 second (FEV1) was seen in current and ex-smoking first degree relatives of probands compared with control subjects, with no statistically significant difference in FEV1 among non-smokers. McCloskey et al investigated the risk to siblings of COPD probands for the development of COPD, with similar findings.9 However, there is limited information on the heritability of flow related spirometric characteristics such as forced expiratory flow at the mid-portion of forced vital capacity (FEF25–75) and FEF25–75/FVC in first degree relatives of individuals with COPD. These spirometric measures may be decreased in the presence of airway abnormalities (such as those secondary to inflammation or fibrosis) or alterations in elastic recoil; alternatively, they may indicate the presence of dysanaptic lung growth.
Identifying intermediate phenotypes other than FEV1 and FEV1/FVC for genetic linkage and association studies of COPD may provide further understanding of risk factors for lung function decline and genetic influences on obstructive pulmonary disease. In this study we have assessed FEF25–75 and FEF25–75/FVC in first degree relatives of a cohort of individuals with severe early onset COPD (without severe α1-antitrypsin deficiency) and population based control subjects. We hypothesised that decrements in FEF25–75 and FEF25–75/FVC may represent spirometric changes that identify individuals with an inherited susceptibility for COPD. Some of the results presented here have been reported in the preliminary form of an abstract.10
METHODS
Probands with severe early onset COPD were enrolled from pulmonary clinics at Brigham and Women’s Hospital, Massachusetts General Hospital, and the Brockton/West Roxbury VA Hospital. Probands were defined as having a physician’s diagnosis of COPD, FEV1 <40% predicted, age <53 years, and no evidence of severe α1-antitrypsin deficiency. Potential participants were excluded from the analysis if they underwent lung transplantation before enrolment in the study. After medical record review, 84 subjects who met the enrolment criteria were contacted by letter and enrolled as probands. First degree relatives from 77 pedigrees included parents, siblings, and children of probands with severe early onset COPD; first degree relatives were unavailable in seven other pedigrees. A more extensive description of the selection of the current cohort has been published elsewhere.8,11 The present analysis excluded subjects with pulmonary function tests from outside sources.
Controls were recruited from population based studies as previously described.8,12,13 169 letters were sent to subjects of similar age and sex as the study probands. Forty responses were obtained, with 33 control “probands” willing to participate. Of the 33 potential control probands, 11 were excluded because of mild smoking history and two because of scheduling difficulties. This resulted in the inclusion of 20 age, sex and smoking matched control probands, 54 of their first degree relatives and nine spouses, giving a total of 83 control individuals. Pulmonary function was not considered as part of the selection criteria for participation by controls, so all 83 controls were included in the analysis.
All participants provided written informed consent and completed a protocol that included a questionnaire, spirometric tests, and a blood specimen. The protocol was completed in the participants’ homes or at the Outpatient General Clinical Research Center at Brigham and Women’s Hospital. The protocol was approved by the Human Research Committee of Partners/Brigham and Women’s Hospital and the Veterans’ Administration Institutional Review Board.
Questionnaire
Each participant completed a modified version of the 1978 American Thoracic Society/ Division of Lung Diseases Epidemiology Questionnaire, as previously described.8 An “ever smoker” was defined as an individual who had smoked more than 20 packs of cigarettes in a lifetime or at least one cigarette a day for at least 1 year. A current smoker was defined as someone who answered “yes” to smoking at any time in the month before the interview. Non-smokers were classified as those who answered “no” to the question “Have you ever smoked cigarettes?” Pack years of cigarettes smoked were calculated as the product of the duration of smoking in years and the average number of cigarettes smoked per day, divided by 20 to convert to packs. Race was assessed by questionnaire (white, black, other).
Pulmonary function testing
Spirometric tests were performed for first degree relatives and control subjects with a Survey Tach spirometer (Warren E Collins, Braintree, MA, USA) as previously described.8 The manoeuvres were performed in accordance with ATS criteria, with all subjects seated and wearing nose clips.14 Participants were asked to desist from using inhaled bronchodilators for 4 hours before testing, if possible. The values presented for FEV1 represent the highest value for any effort, and FEV1/FVC, FEF25–75 and FEF25–75/FVC represent values from the best test effort, defined as the manoeuvre with the highest sum of FEV1 plus FVC. Height was measured in stocking feet. Percentage predicted values were calculated using prediction equations as defined by Hankinson and colleagues.15 Pre- and post-bronchodilator (180 μg albuterol) spirometry was performed.
Statistical methods
All computations were performed with the SAS statistical package (SAS Statistical Institute, Cary, NC) on a SUN server running the UNIX operating system. The Student’s t test was used to compare the mean values between first degree relatives and controls for unadjusted and percentage predicted pulmonary function parameters. Unadjusted values for pulmonary function parameters were considered in multivariate regression models that included age, age2, sex, height, height2, race, and pack years of smoking. As a number of individuals were included from each early onset COPD family and each control family, generalised estimating equation (GEE) models were used for regression. GEE models account for the positive correlation between family members within a familial cluster. Since age is an important contributor to pulmonary function outcomes, regression analyses were performed on the overall group of participants and a subset that excluded individuals 18 years or younger. Heritability estimates were computed using all individuals from the early onset COPD pedigrees. Narrow sense heritability estimates (h2) were calculated using a variance component approach in the SOLAR program;16 this estimate represents a ratio of the phenotypic variance due to additive genetic effects divided by the total trait phenotypic variance. The heritability estimates were calculated with inclusion of age, sex, race, height, pack years of cigarettes, pack years2, age2, and height2 as covariates.
RESULTS
Demographic and spirometric data of first degree relatives stratified by smoking status
As previously reported, the probands with early onset COPD had severe airflow obstruction11 (mean FEV1 among probands of 16.1% predicted for men and 17.5% predicted for women). Most of the early onset COPD probands were female (71%).11 In the current analysis, 55.6% of the first degree relatives of early onset COPD probands and 56.6% of the controls were female (table 1). There were no differences in mean ages between the first degree relatives and control group stratified by smoking status. The age range of the first degree relatives extended from 7.8 to 80 years for non-smokers and from 15.1 to 87 years for smokers. Exclusion of 22 non-smokers and two smokers aged 18 years or younger resulted in more comparable age ranges between the first degree relatives and controls.
Baseline demographic and pulmonary data stratified by smoking status
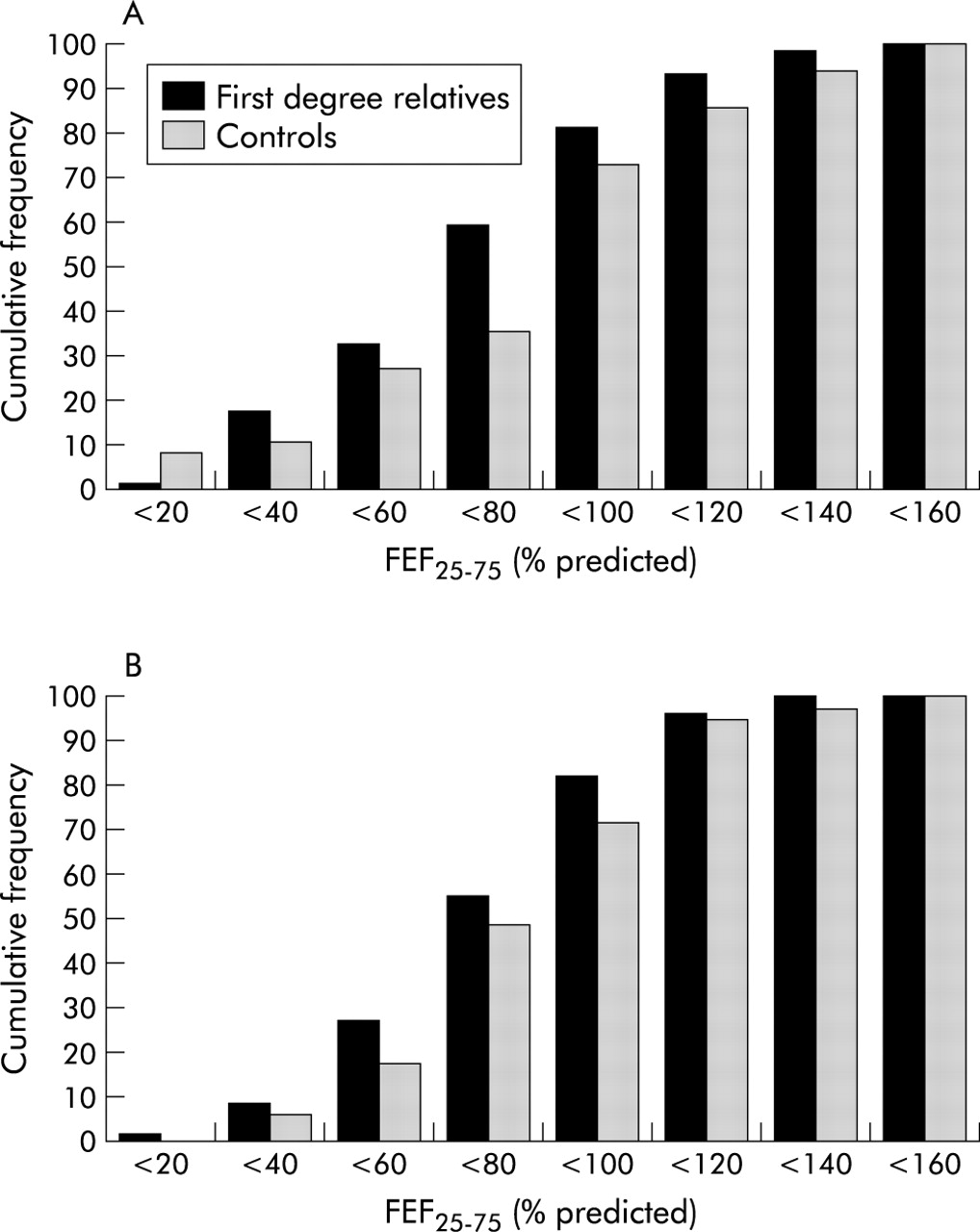
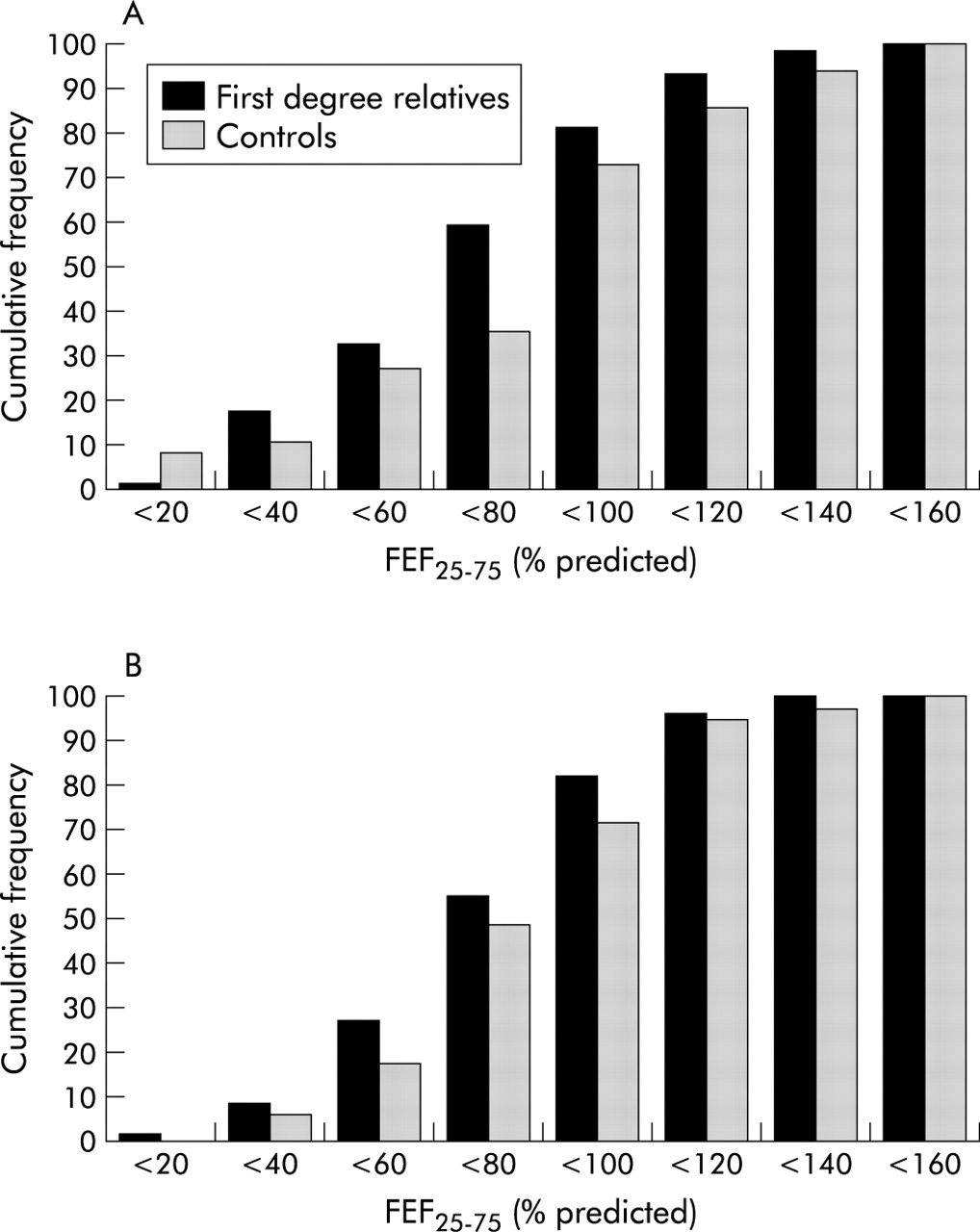
Among the smokers, despite similar ages and mean pack years of smoking, first degree relatives had lower mean percentage predicted FEV1 and FEF25–75 values; among the smokers the unadjusted values (not shown) for FEV1/FVC, FEF25–75 and FEF25–75/FVC were also significantly lower in first degree relatives of early onset COPD probands. No significant differences in the mean values for unadjusted or percentage predicted FEV1, FVC, FEV1/FVC, FEF25–75, or FEF25–75/FVC values were seen in non-smoking first degree relatives compared with controls (not shown), although there was a trend towards lower values of FEF25–75 percentage predicted and FEF25–75/FVC in first degree relatives of early onset COPD probands. When individuals aged 18 years or younger were removed, percentage predicted FEF25–75 and FEF25–75/FVC were significantly lower in first degree relatives than controls. Frequency histograms for FEF25–75 for smoking and non-smoking first degree relatives and controls demonstrate these trends (fig 1).
{kind=link}
Cumulative frequency histograms for FEF25–75 percentage predicted in (A) current and ex-smoking first degree relatives of severe early onset COPD probands and controls and (B) non-smoking first degree relatives of severe early onset COPD probands and controls. (A) Approximately 59% of first degree relatives had percentage predicted FEF25–75 of less than 80% compared with 35% for controls. (B) Approximately 55% of first degree relatives had percentage predicted FEF25–75 less than 80% predicted compared with 48% for controls.
Multivariate regression models for pulmonary function outcomes
To assess familial aggregation of FEF25–75 and FEF25–75/FVC in smokers, multivariate regression was performed using the unadjusted spirometric values in GEE models which included the usual covariates for which pulmonary function measures are adjusted (height, age, race, sex). When multivariate models were analysed with pulmonary function phenotypes as continuous outcomes in all subjects (not stratified by smoking status), first degree relatives of early onset COPD probands had lower values than controls for FEV1, FEF25–75, and FEF25–75/FVC (table 2); there was no significant difference for adjusted FVC. In current or former cigarette smokers there were also statistically significant decrements in FEV1, FEF25–75, and FEF25–75/FVC among the first degree relatives (table 2). Inclusion of current smoking status in the model did not alter the trend of these findings (data not shown). In non-smokers there were no differences between first degree relatives and controls for FEV1 and FVC. However, FEF25–75 and FEF25–75/FVC were significantly reduced among non-smoking first degree relatives compared with non-smoking controls (table 2). Residual analysis confirmed the robust nature of these findings (data not shown). A sensitivity analysis excluding individuals aged 18 years or younger did not alter the overall significance of these findings in non-smokers (table 2).
Multivariate regression models for predicting pulmonary function in all subjects and after excluding those aged 18 years or younger
Heritability of spirometric phenotypes
Heritability estimates were obtained for 576 individuals in the Boston Early-Onset COPD Study pedigrees for all spirometric parameters (table 3). Probands and all extended family members who participated in this study were included in the analysis. The heritability estimates for FEF25–75 and FEF25–75/FVC were at least equal to those values for FEV1 and FEV1/FVC, with narrow sense heritability estimates for FEF25–75 and for FEF25–75/FVC calculated as 0.38 and 0.45, respectively.
Heritability estimates for spirometric parameters
DISCUSSION
The phenotypic expression of COPD is under both genetic and environmental influence. As a complex human disease, COPD is heterogeneous in presentation, with variable severity and anatomical distribution. To date, the only known genetic risk factor for COPD is severe α1-antitrypsin deficiency, and research efforts are ongoing in an attempt to localise the other genetic influences on this complex disease. From an environmental perspective, cigarette smoke exposure is an established risk factor. Probands with severe early onset COPD were culled in an effort to define other genetic factors relevant to the heritability and expression of COPD. This cohort of individuals with severe early onset COPD has disease out of proportion to age and smoking histories, suggesting the presence of an underlying susceptibility that is under genetic influence and subject to modification of phenotypic expression due to gene × environment interactions.
Familial aggregation has previously been reported for COPD and for spirometric measures of pulmonary function. Most of the earlier investigations have focused on FEV1 and FEV1/FVC. The current investigation of first degree relatives of early onset COPD probands provides further insight into the familial aggregation of spirometric phenotypes. A previous analysis of spirometric phenotypes in the first 44 pedigrees of this early onset COPD cohort showed that current and ex-smoking first degree relatives had reduced FEV1 and FEV1/FVC compared with control subjects of similar age and smoking history.8 No increased risk for decrements in FEV1 or FEV1/FVC was seen in non-smoking first degree relatives. Identification of phenotypic characteristics that differentiate non-smokers is important as this may point to intermediate phenotypes of COPD that are under strong genetic control, as well as being potentially indicative of a susceptibility to develop clinically significant disease in the setting of an appropriate environmental exposure.
This current analysis in the Boston Early-Onset COPD Study extends the previous analysis to the flow related measures FEF25–75 and FEF25–75/FVC, and identifies these flow parameters as potential indicators of genetic susceptibility to develop COPD. Cohen et al17 have suggested familial aggregation of phenotypes related to abnormalities in forced expiration, finding differences in Vmax for lifetime non-smokers together with decrements in Vmax, V50, and V25 flow related measures among first degree relatives who smoked.17 Our findings are potentially suggestive of a heritable abnormality in airways development that may predispose to disease susceptibility later in life. Since these decrements are manifest in non-smokers and are of a larger magnitude in first degree relatives who smoke, our results suggest both a baseline genetic predisposition for lower FEF25–75 and FEF25–75/FVC as well as a potential gene × smoking interaction that accentuates the decrements in FEF25–75 and FEF25–75/FVC. These findings remained robust after the exclusion of individuals with low FEV1, suggesting that the observations in smokers and non-smokers are not being driven by individuals who already have low lung function. There was no change in the findings of lower spirometric measures among the smoking first degree relatives compared with controls, regardless of how smoking was considered as a covariate (current smoking, ever smoking, pack years smoked). This suggests that differential inflammatory effects of current smoking at the time of spirometry are not the explanation for our results. This study did not quantify the amount of childhood exposure to smoke experienced by first degree relatives; assessment of childhood smoke exposure is subject to potential recall bias. Adding childhood tobacco smoke exposure as a yes/no variable to our multivariate models did not change the results among the smokers or non-smokers.
Our analysis has several important limitations. The Boston Early-Onset COPD Study cohort is predominantly white, so generalisability of these findings to individuals and families of other races may be limited. The rate of recruitment among the controls was low; only 20 control probands and 83 total controls were recruited from letters sent out to individuals who had been previous participants in population based studies from our laboratory.8 The size of the control group is an important consideration as we interpret our findings, and a larger control group would strengthen the interpretability and generalisability of our results. Despite the potentially increased measurement related variability in FEF25–75 and FEF25–75/FVC, the fact that there was any difference between the non-smokers suggests that these phenotypes are important to consider in genetic epidemiology studies, even if the absolute magnitude of our findings may be influenced by the small size of our control group. The sensitivity analyses performed by removing the younger individuals suggest that our results are not being driven by a small number of younger individuals in the early onset COPD pedigrees. FEF25–75 is a more variable measure than FEV1, but the same technique and spirometric equipment were used to measure this parameter in all subjects, which may contribute to increased accuracy of measurement of these phenotypes. Lastly, we do not have longitudinal follow up data to assess the development of COPD in the first degree relatives, nor do we have radiographic correlates assessing the presence of emphysema in the first degree relatives or controls. Longitudinal investigation and confirmation of these findings in an independent cohort is a goal of future studies.
Abnormalities in FEF25–75 have been considered as evidence for small airways disease,18 although other investigators have suggested that this measure does not provide information beyond FEV1/FVC for characterising small airway disease.19–21 Alternatively, decrements in FEF25–75/FVC may represent variations in lung elastic recoil or other acquired/inherited abnormalities in airway function, variability in genetically programmed responses to oxidative and proteolytic stress in the lungs, or may be the result of airway/lung parenchyma dysanapsis. FEF25–75/FVC has been used as a measure of dysanaptic lung growth, the physiologically normal but non-isotropic lung growth that occurs between the airways and lung parenchyma. Tager and colleagues have shown that FEF25–75/FVC is highly correlated with Mead’s earlier measures of dysanapsis (as measured by the ratio of maximal flow at 50% vital capacity × static recoil pressure of the lung at 50% vital capacity).22,23 Dysanaptic lung growth may predispose to the development of obstructive lung disease24,25 and may also predict airway hyperresponsiveness.26 Chen and colleagues27 have recently investigated whether dysanaptic lung growth has a genetic component.27 They investigated Vmax50/FVC using segregation analysis and suggested that dysanaptic growth of the lung airways to parenchyma is under major gene control.
Although we do not currently have longitudinal follow up data on the first degree relatives of early onset COPD probands to assess the development of lung disease, it is our hypothesis that the first degree relatives of individuals with severe early onset disease who demonstrate reduced levels of spirometric flow parameters have increased susceptibility to develop airflow obstruction later in life. The decrements of FEF25–75 and FEF25–75/FVC in non-smoking first degree relatives suggest a phenotypic difference from population based controls. This finding may be related to a baseline susceptibility to develop lung disease in families of probands with early onset COPD, with an increased risk to develop airflow obstruction in the setting of gene × environment (smoking) interactions. Importantly, we have shown significant heritability estimates for FEF25–75 and FEF25–75/FVC similar to those for FEV1 and FEV1/FVC. These findings suggest the importance of including these additional spirometric measures as intermediate phenotypes in studies of the genetic epidemiology of COPD.
In summary, investigation of the spirometric characteristics of first degree relatives of probands with severe early onset COPD unrelated to severe α1-antitrypsin deficiency found reductions in FEF25–75 and FEF25–75/FVC in smoking and non-smoking first degree relatives, with heritability estimates that are comparable to FEV1 and FEV1/FVC. These findings suggest that genetic factors may be relevant to the determination of FEF25–75 and FEF25–75/FVC. Since differences between non-smokers have not been demonstrated in our cohort for FEV1 and FEV1/FVC, this suggests that FEF25–75 and FEF25–75/FVC may represent genetic effects that are manifest early in life and identify a disease susceptibility characteristic that is highly heritable. FEF25–75 and FEF25–75/FVC are important intermediate phenotypes to consider in genetic linkage and association studies of COPD.
REFERENCES
Footnotes
-
Dr DeMeo was supported by National Institute of Health (NIH) grant T32 HL0742722. The Boston Early-Onset COPD Study was supported by NIH grant R01 HL61575.