Article Text

Abstract
A 66 year old man had inhaled cotton fibre for 50 years at his workplace. He did not have any respiratory symptoms. Chest CT scans revealed diffuse centrilobular and peribronchovascular interstitial thickening. Lung biopsy specimens confirmed the presence of string-like foreign bodies as well as granulomas and fibrosis in the peribronchial region. Infrared spectrophotometry confirmed that the foreign bodies were composed of natural cellulose. This is the first study to show directly by examination of biopsy samples that cotton fibre inhalation can cause diffuse lung disease. The clinical features of the disease were entirely different from those of byssinosis.
- cotton
- byssinosis
- diffuse lung disease
- cellulose
Statistics from Altmetric.com
Byssinosis is a disease caused by the inhalation of cotton, flax, and hemp fibres while working. It is the general term for a syndrome and the clinical description is well established.1,2 This report describes a new type of diffuse lung disease caused by cotton inhalation which was confirmed pathologically and had marked differences from byssinosis.
CASE REPORT
A 66 year old man underwent chest radiography during a health check and diffuse infiltrative opacities were detected in the bases of both lungs. He had no respiratory symptoms, including cough, sputum, or dyspnoea. He was an ex-smoker (6 pack-years) who had stopped smoking about 30 years earlier. The patient had been involved in the manufacture and repair of futons for 50 years, working at a small futon shop since he was 16 years old. Although cotton fibres were often floating freely in the atmosphere of the workroom, no respiratory protection for the dust was provided. On examination he had fine inspiratory crackles in the bilateral lower lung fields.
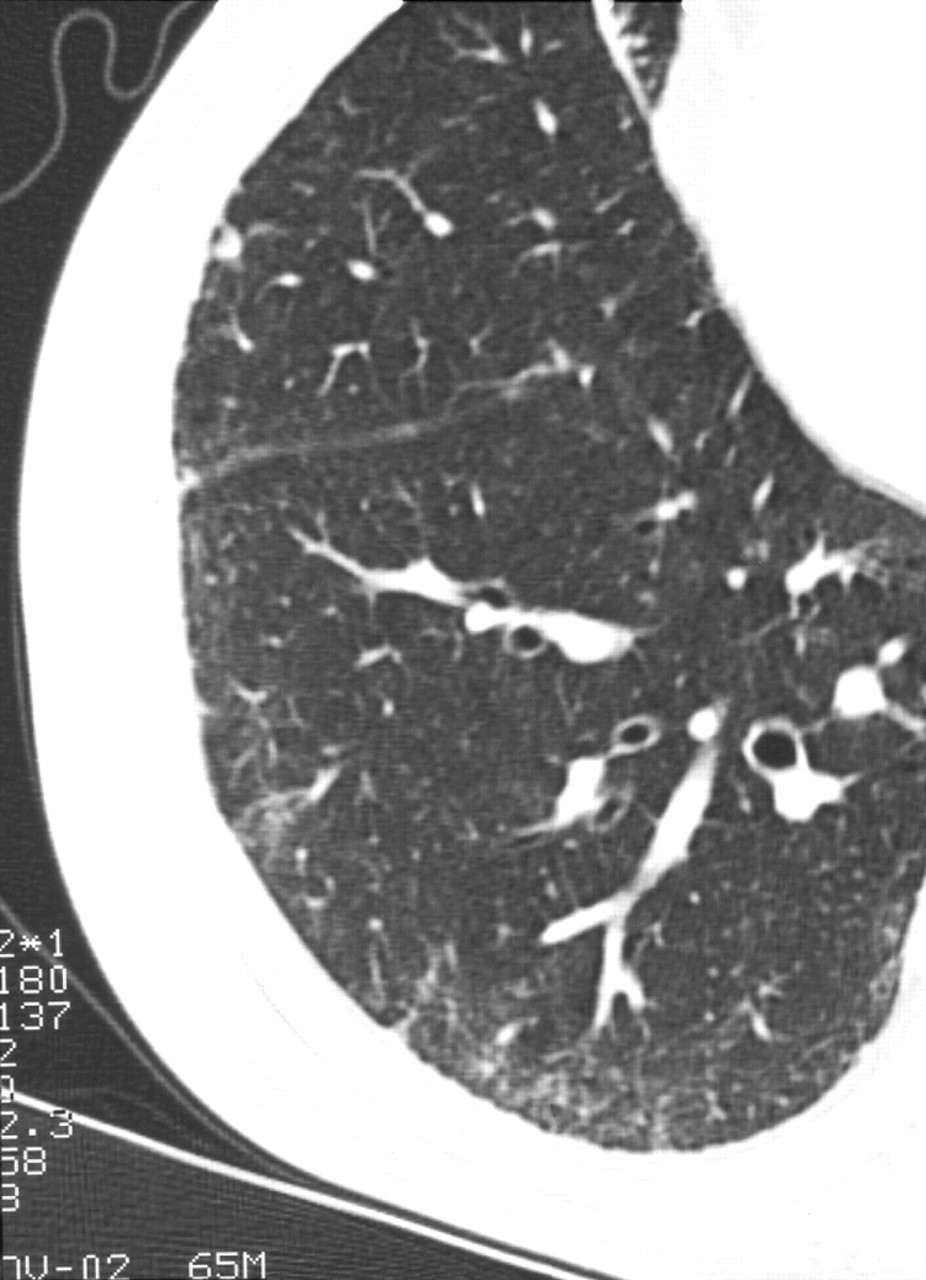
Laboratory tests revealed the following: white blood cell count 5300/μl; lactate dehydrogenase 241 IU/l (normal ⩽220); KL-6 607 U/ml (normal ⩽500); surfactant protein A 57.7 ng/ml (normal ⩽43.8); surfactant protein D 224 ng/ml (normal ⩽110); C reactive protein 0.6 mg/dl (normal ⩽0.3). Serological tests showed no evidence of collagen disease. Arterial blood gas analysis revealed a pH of 7.452, Paco2 of 35.5 mm Hg, and Pao2 of 76.2 mm Hg. Lung function tests gave the following results: vital capacity 2.78 l (87% of predicted), forced expiratory volume in 1 second/forced vital capacity (FEV1/FVC) 75%, peak expiratory flow 7.53 l/min (104% of predicted), and carbon monoxide transfer factor (Tlco) 12.7 ml/min/mm Hg (86% of predicted). As indicators of small airway function, maximal mid expiratory flow was 1.42 l/s (49% of predicted) and 25% forced expiratory flow was 0.49 l/s (31% of predicted). Analysis of bronchoalveolar lavage fluid revealed a cell count of 2.2 × 105/ml with 15% lymphocytes (CD4/CD8 ratio of 4.65) and 85% macrophages. A high resolution CT (HRCT) scan of the lungs showed subpleural ground glass opacities and an interface sign at the surface of the visceral pleura, while centrilobular and peribronchovascular interstitial thickening were identified as the inverted Y and V sign (fig 1).

HRCT scan of the lung showing subpleural ground glass opacities, an interface sign at the surface of the visceral pleura, and centrilobular and peribronchovascular interstitial thickening.
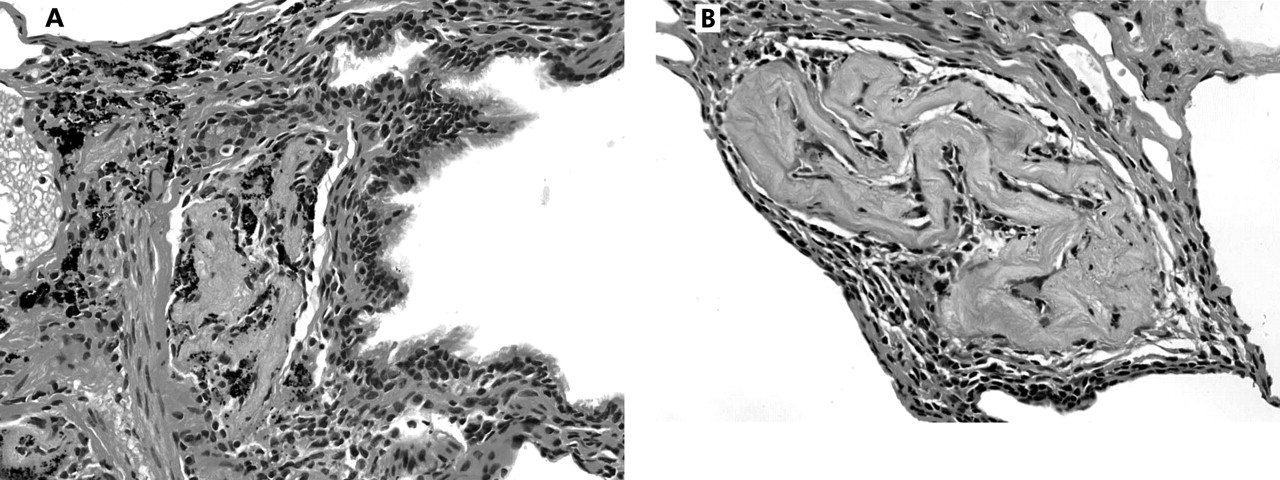
Transbronchial lung biopsy was performed but failed to provide a pathological diagnosis. A video-assisted thoracoscopic biopsy was therefore undertaken with the patient’s informed consent and three biopsy specimens were obtained. All three specimens had similar histological features of tiny granulomas and fibrous thickening of the peribronchiolar interstitium (fig 2). Scattered eosinophilic string-like foreign bodies were detected within the areas of peribronchiolar fibrosis (fig 3A and B). These string-like foreign bodies were 20–30 μm thick and were surrounded by histiocytes that formed granulomas with an overall size of 100–150 μm. It was unclear whether or not the foreign bodies had a hollow oval structure on cross section (a characteristic feature of cotton fibres).

Low power histological view of video-assisted thoracoscopic biopsy specimen showing fibrous thickening of peribronchiolar interstitium. H&E staining, magnification ×4.
{kind=link}
{kind=link}
{kind=link}
(A) High power view of the same specimen as in fig 2 showing an eosinophilic string-like foreign body in the bronchiolar wall. (B) A foreign body in the other portion. H&E staining, magnification ×40. Spectral analysis by infrared spectrophotometry showed that the foreign bodies had an identical pattern to that of cellulose.
Two additional tests were conducted to identify the string-like foreign bodies. The samples were heated to 300°C and, since this did not melt them, it was concluded that they were natural fibres. Spectral analysis of the foreign bodies with an infrared spectrophotometer (IRμs Molecular Microanalysis System, Spectra-Tech Inc, USA) showed that the foreign bodies had a similar spectral pattern to that of cellulose. Based on the results of these tests and the patient’s occupational exposure to cotton inhalation, the cellulose fibres were concluded to be cotton.
Electron microscopy was also performed but we were unable to identify the foreign bodies because they were sparsely distributed in the biopsy specimens.
DISCUSSION
This patient had been engaged in the manufacture and repair of futons for 50 years, during which period he had been exposed to cotton dust without respiratory protection. The futon is a traditional Japanese style of bedding made of cotton packed inside a cloth bag, and is similar to the mattress used on a western bed. Byssinosis is a well known disease caused by the inhalation of cotton and is the general term applied to various acute and chronic conditions that afflict workers who process cotton, flax, and hemp fibres.1,2
However, the patient described here did not have any of the recognised symptoms of byssinosis (cough, wheeze, or Monday morning fever) and lung function tests did not show the relevant abnormalities (no reduction in FEV1 but small airway disturbance). He did not have any of the histopathological features characteristic of byssinosis such as mucus gland hyperplasia and infiltration of neutrophils into the bronchi.3,4 There was also no eosinophilic infiltration (reflecting allergy) in the biopsy specimens. Since cellulose fibres were found in the lungs of our patient and a foreign body tissue reaction to cellulose was confirmed, it was concluded that he suffered from a condition that could be called cotton dust pneumoconiosis.
There have been only a few reports of pulmonary fibrosis and pneumoconiosis due to organic dust.5,6 Sano investigated the pathogenesis of organic dust pneumoconiosis, showing that rats developed mild fibrosis and granulomas in the lungs after endotracheal infusion of saline containing organic dust, but this report has only been published in Japanese.5 In addition, one post-mortem study has suggested that cotton fibres cause pulmonary fibrosis in humans.7 The fibrosis observed in our patient was characterised by a peribronchiolar distribution and occupied the central area of the secondary lobules, developing around the string-like foreign bodies which we identified as inhaled cotton fibres. There was no evidence of honeycombing. These findings were similar to the histological distribution of interstitial lung disease associated with nylon flock.8 We therefore conclude that the fibrosis in our patient was causally related to the inhalation of cotton.
This is the first histological evidence that cotton fibre inhalation may be related to a granulomatous reaction and peribronchial fibrosis in the lungs. Our findings support the possibility that, like inorganic dust, organic dust can also cause pneumoconiosis. The pulmonary opacities seen in our patient were predominantly localised at the lung bases, so it was difficult to distinguish this condition from idiopathic pulmonary fibrosis on plain chest radiographic films. A diagnosis of cotton dust pneumoconiosis may be suggested by occupational exposure, a bronchiolocentric distribution of lung changes on the HRCT scan, and detection of string-like foreign bodies in lung biopsy specimens. The huge number of workers in industries handling cotton around the world should therefore be more careful about exposure to inhalation of cotton fibres.