Article Text

Abstract
Background: Written asthma action plans based on personal best peak expiratory flow (PEF) consistently improve health outcomes, whereas those based on predicted PEF do not. Guidelines state that personal best PEF should be assessed over 2–3 weeks during good asthma control, but it is unclear how long to wait after commencing or changing treatment.
Methods: Electronically recorded spirometric data from 61 subjects with initially poorly controlled asthma from a 72 week budesonide study were analysed. For each week, average morning pre-bronchodilator PEF was calculated and personal best PEF was determined as the highest PEF in the previous 2 weeks. The time to plateau was defined as the week beyond which no further improvement occurred.
Results: At baseline, average morning PEF was 61% predicted and personal best PEF was 87% predicted. Personal best PEF from twice daily monitoring increased to a plateau of 95% predicted (p<0.0001) after only 3 weeks of budesonide treatment. However, average morning PEF continued to improve for 3 months and “as needed” reliever use for 7 months.
Conclusions: Personal best PEF is a useful concept for asthma self-management plans when determined as the highest PEF over the previous 2 weeks. With twice daily monitoring, personal best PEF reaches plateau levels after only a few weeks of corticosteroid treatment.
- asthma
- asthma action plan
- peak expiratory flow
- patient education
- personal best
Statistics from Altmetric.com
Written asthma action plans are part of effective asthma self-management.1 In action plans based on peak expiratory flow (PEF), a change in treatment is indicated at “action points” which, for simplicity, are usually percentages of predicted or personal best PEF.2 A recent review showed that written action plans based on personal best PEF resulted in improvements in hospital admissions, emergency room visits and PEF, whereas those based on predicted PEF improved only hospital admissions.3
Asthma guidelines define personal best PEF as the highest value achieved over 2–3 weeks of twice daily pre- and post-bronchodilator monitoring during a period of good asthma control.2 However, many patients only present for review when their asthma is poorly controlled, and some measures of asthma control improve for many months after commencement of inhaled corticosteroids.4 To examine the time at which personal best PEF stabilises after initiation of inhaled corticosteroids, we analysed electronically recorded data from a long term budesonide study.4
METHODS
Data were obtained from a 72 week high dose budesonide study reported elsewhere.4 Ethical approval was obtained and all subjects gave written informed consent. Eligible subjects were aged 18–75, non-smokers, and had symptoms and β2 agonist use consistent with poorly controlled asthma with inhaled corticosteroid permitted up to 1200 μg/day. Exclusion criteria were a smoking history of >10 pack-years, other lung disease, recent asthma exacerbation, or long acting β2 agonist use. After a 2–4 week run-in period, subjects were randomised to 1600 or 3200 μg budesonide per day with down-titration over weeks 17–72. Subjects used electronic DiaryCard spirometers (MicroMedical, Rochester, Kent, UK) twice daily, upon waking and in the evening, before β2 agonist if possible.
The highest PEF was selected from each set of three spirometric manoeuvres, and flow-volume loops were reviewed if PEF or forced expiratory volume in 1 second (FEV1) was >1.5 standard deviations from the 4 week mean. For each study week, average morning pre-bronchodilator PEF was calculated and personal best PEF was determined as the highest PEF in the previous 2 weeks. Data from all subjects were combined for analysis as there was no significant difference in PEF between randomisation groups.4 The rate of change in PEF variables each week was calculated for each patient as the difference between the average of the values for the previous 4 weeks and the average of those for the subsequent 4 weeks (including that week). During the first 4 weeks, 2 week averaging periods were used. The overall mean of the differences was calculated for each week and the plateau was determined as the week beyond which the 95% confidence interval of the mean difference included zero (Analyse-It Software, Leeds, UK)—that is, the point beyond which the rate of change was not significantly different from zero. Group data for bronchodilator use were highly skewed; the plateau for this variable was therefore determined, using 4 week averages for each patient, as the week in which pairwise comparisons with subsequent 4 week averages became non-significant, tested by Wilcoxon’s signed rank sum test. All available data were used up to completion/withdrawal. The length of time from baseline to achieving a plateau for each variable was reported in weeks.
RESULTS
At baseline (week 0) the 61 subjects had characteristics of poorly controlled asthma with reliever use 3.0 occasions/day (interquartile range (IQR) 1.9–4.4). Average morning pre-bronchodilator PEF was 340 l/min (61% predicted, 95% confidence interval (CI) 57 to 66).5 Within-session PEF reproducibility was 19 l/min (IQR 14–25).6 Overall, 42 590 spirometric manoeuvres were recorded (69% of potential total manoeuvres over 72 weeks); screening excluded 0.03% of PEF values as artefactual.
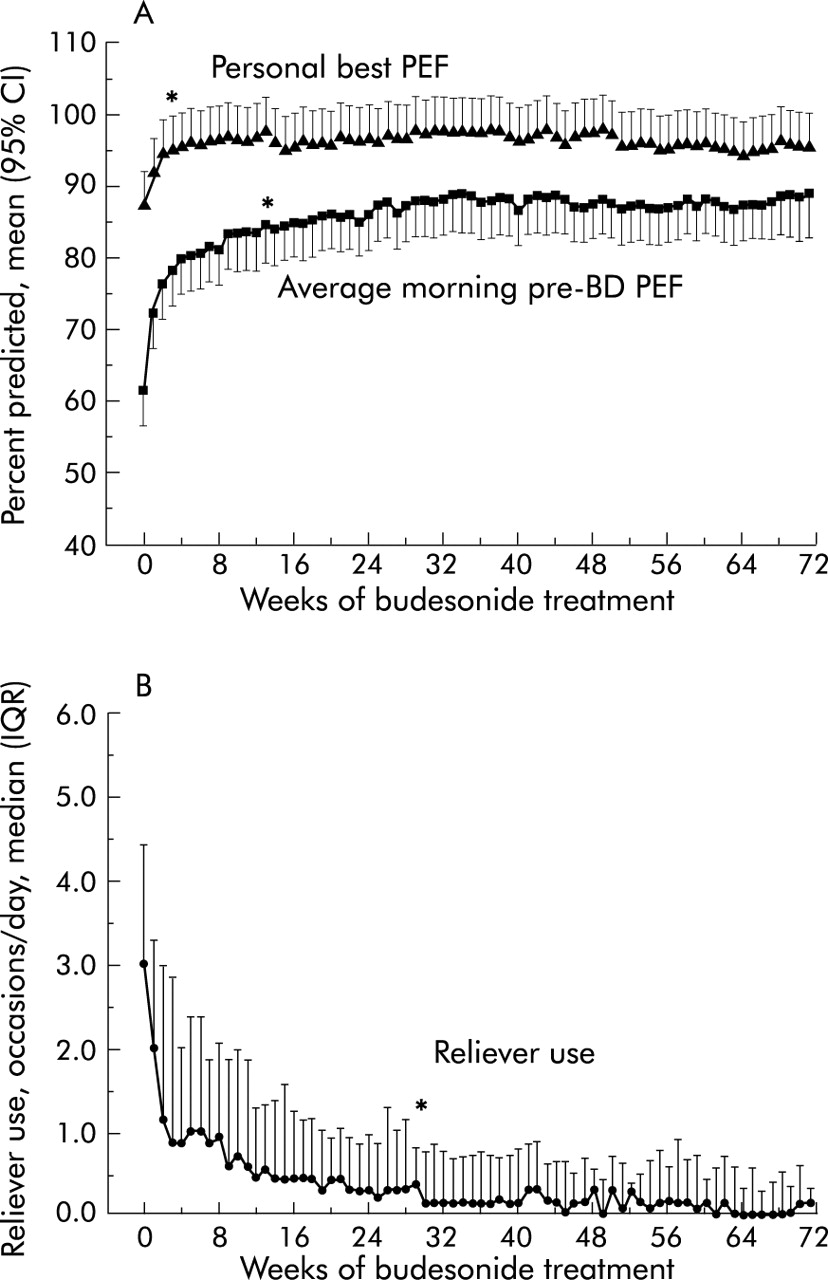
Personal best PEF improved from 484 l/min (87% predicted, 95% CI 82 to 92) at baseline to a plateau of 527 l/min (95% predicted, 95% CI 90 to 100, p<0.0001; fig 1). The plateau in personal best PEF based on twice daily PEF measurements was reached after only 3 weeks of treatment when reliever use was still 0.9 occasions/day (IQR 0.3–2.9). The plateau in personal best PEF was delayed to 8 weeks if once daily (morning) PEF values were analysed. Average morning pre-bronchodilator PEF continued to improve to week 13 (467 l/min, 84% predicted, 95% CI 79 to 90) and reliever use to week 30 (0.1 occasions/day, IQR 0.0–0.8); p<0.0001 compared with week 3 for each.

{kind=link}
(A) Personal best PEF, determined as the highest morning or evening pre- or post-bronchodilator (BD) PEF from the previous 2 weeks, and average morning pre-bronchodilator PEF, calculated for each week of the study and shown as percentage predicted PEF.5 Plot shows mean with 95% confidence intervals. (B) As needed short acting β2 agonist use in occasions/day (1 occasion = 2 puffs). Plot shows median and IQR. Asterisks show the week after which no further statistical improvement occurred (plateau).
DISCUSSION
This study showed that personal best PEF from 2 weeks of twice daily measurements reached a plateau very early after initiation of high dose budesonide in patients with poorly controlled asthma. These findings indicate that the action points for a PEF based action plan can be assigned after only a short period of inhaled corticosteroid treatment, without waiting until other markers of asthma control such as average PEF or symptoms have stabilised.
Written asthma action plans are an essential component of asthma self-management education, and their use has been associated with significant improvements in health care utilisation, morbidity, and quality of life.1 In Australia, although written action plans have been recommended in asthma guidelines for 15 years, the proportion of patients possessing a plan declined by almost half between 1996 and 2001 to only 22%.7 Confusion for clinicians may have contributed to this decline as, despite general advice to individualise the plan to each patient, asthma guidelines contain few specific instructions about how this should be done. A recent review of the critical components of action plans found additional benefits when they were based on personal best rather than predicted PEF.3 However, the need to standardise the assessment and recording of personal best PEF has been highlighted by a study of 104 patients presenting with acute asthma.8 At presentation, only 30 patients knew their personal best PEF and, of these, 10/22 recorded a higher PEF over the next 24 days.
Current guidelines state that personal best PEF should be determined during good asthma control. However, some patients only present when their asthma is uncontrolled and do not return after they have completely recovered, leaving no opportunity to reassess their personal best PEF during good asthma control. This problem could be avoided by basing the action plan on predicted PEF, but such plans show fewer benefits.3 As patients are less likely to follow medical instructions which are discordant with their own lay beliefs,9 adherence may be poorer with a plan that specifies action at a PEF which the patient considers to be too high or too low. The present study shows that personal best PEF can be determined long before symptoms and reliever use have stabilised, when the patient may still be motivated to return for review.
Because the present study was based on the analysis of outlying values, rigorous quality control analysis was undertaken.6 Within-session reproducibility of PEF, FEV1 and FVC was well within guidelines for supervised spirometry. Data falsification was eliminated by electronic monitoring, and the use of spirometric rather than PEF manoeuvres may have contributed to the low rate of artefactual PEF values. Although long term adherence with monitoring using mechanical PEF meters and paper diaries is notoriously poor, the present recommendations should be applicable to conventional monitoring as adherence is reasonable over shorter periods. The chance of inappropriate changes in medication will be reduced by ensuring correct PEF technique, and by re-establishing personal best every few years or if the PEF meter is changed. This advice will be particularly important in Europe with the imminent introduction of non-linear PEF scales. It is of interest that, despite the known limitations of conventional PEF monitoring, significant health benefits have been found with the use of action plans based on this type of monitoring.3
Previous studies have examined the time course of changes in average morning PEF4,10 but not personal best PEF. It is predictable that maximum PEF would improve more rapidly than average morning PEF, as inhaled corticosteroids reduce PEF variability and improve lung function. The present study was carried out in patients with very poorly controlled asthma at entry who were started on inhaled corticosteroid treatment. The recommendations should be more widely applicable as the time course of improvement in asthma outcomes is even shorter for patients with milder asthma.10 An earlier plateau in personal best PEF would also be expected with use of long acting β2 agonists, given their more rapid onset of effect than inhaled corticosteroid alone.11 One limitation of the present study is that patients were excluded if they experienced a viral respiratory infection during the run-in period; however, because of the observed reduction in PEF during viral exacerbations (mean 10 days),12 it would appear advisable to delay determination of personal best PEF until after clinical resolution of a respiratory infection.
The prolonged improvement in bronchodilator use in the present study4 is of interest. The time course of improvement for asthma symptoms was similar (data not shown), suggesting that reliever medication was not just being used habitually. This prolonged improvement may instead reflect a reduction in predisposition to bronchoconstriction, associated with continuing improvement in airway hyperresponsiveness over 18 months despite down-titration of inhaled corticosteroids.4 Preliminary results from the GOAL study indicate that patients treated with fluticasone/salmeterol combination also have a gradual reduction in bronchodilator use over many months.13 The findings from these studies suggest that action plans based on reliever use may need revision after several months of inhaled corticosteroid or combination treatment.
The phrase “personal best” is already familiar to the general public through sports reports which commonly refer to an athlete’s “PB”—that is, their “best ever” time/height/distance. The distinction between the sports definition of PB as “best ever” and the guidelines based definition of personal best PEF as “best in the last 2 weeks” is important, as additional analysis of the present data showed that “best ever” PEF continued to rise for 39 weeks from baseline, compared with the plateau at 3 weeks for personal best defined according to the guidelines. “Best ever” PEF for individual patients would therefore vary substantially, depending on how long they had been monitoring. By contrast, personal best PEF defined as “best in the last 2 weeks” is standardised to a consistent short duration of monitoring and is thus better suited to the real life situation of intermittent monitoring. To avoid any confusion with lay use of “PB”, patients should be shown that their personal best PEF is calculated from 2 weeks of twice daily data, and manufacturers of electronic devices which can store many months of PEF data should be made aware of this distinction.
The concept of “personal best” PEF is particularly appropriate for asthma self-management because it reminds patients of the individualised nature of their action plan and reinforces the aim of maintaining best lung function. Patients presenting with poor asthma control can be asked to carry out twice daily monitoring for the first few weeks after initiating or changing inhaled corticosteroid treatment, and can then be issued with a written action plan based on personal best PEF to help reduce the risk of re-presentation.
Footnotes
-
This work was supported by the Asthma Foundation of NSW, the National Health and Medical Research Council of Australia, AstraZeneca Sweden and AstraZeneca Australia.