Article Text

Statistics from Altmetric.com
In 2001 the US National Heart, Lung and Blood Institute (NHLBI) and the World Health Organization announced guidelines for the diagnosis, management, and treatment of COPD (Global Initiative for Chronic Obstructive Lung Disease, GOLD).1 One key aspect of these guidelines is that COPD is classified by severity into five stages which constitute the basis of treatment recommendations. However, to date there has been little evidence for the usefulness of these severity stages.
We retrospectively reviewed 1000 patients with COPD diagnosed clinically in 2001; 500 patients originated from a pulmonary rehabilitation hospital. Patients’ symptoms (based on a standardised interview), findings of a standardised lung examination, lung function data, and chest radiographic findings are routinely documented in a database. The inclusion criteria were symptoms of COPD (chronic cough with chronic sputum production for more than 2 years) and radiographic findings of COPD (hyperinflation, diaphragmatic flattening). Patients with a history of asthma (variability of spirometric parameters, improvement in forced expiratory volume in 1 second (FEV1) of >20% after inhalation of β2 agonists, symptoms predominantly at night, seasonal allergies, allergic rhinitis, or eczema) were excluded from the study, as were those in whom FEV1 and forced vital capacity (FVC) differed by more than 5% according to the American Thoracic Society (ATS) guidelines2 and patients with an abnormal chest radiograph or chronic cough caused by a disease other than COPD.
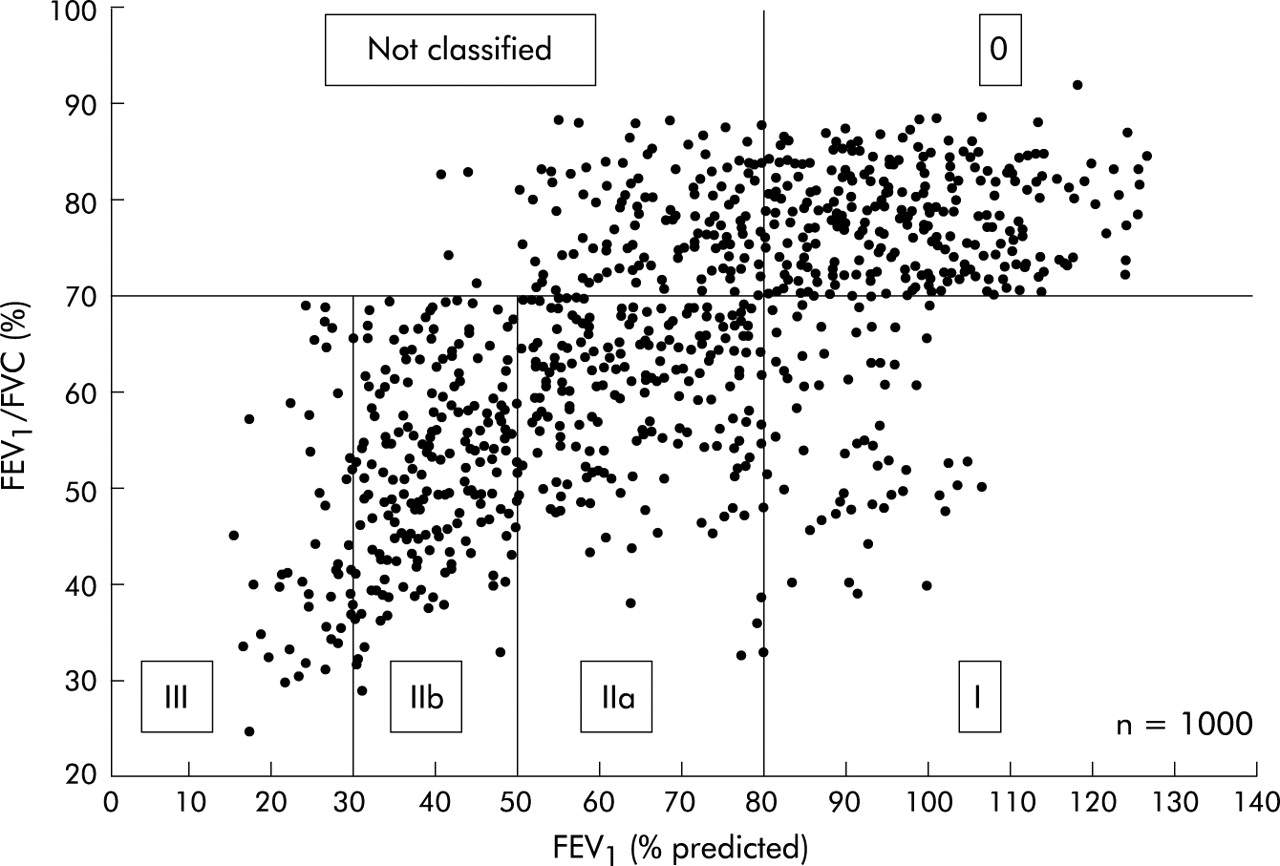
FEV1 and FEV1/FVC were determined three times. The predicted values for FEV1 were taken from the European Respiratory Society (ERS) guidelines.3 The individual values of FEV1 and FEV1/FVC for all patients are shown in fig 1. Almost 14% of patients clinically diagnosed as having COPD could not be classified because they had an FEV1/FVC ratio of >70%, despite having a reduced FEV1 (<80% predicted). This combination is not represented in the GOLD classification. Less than 5% of all patients were classified as GOLD stage I.
The finding that the GOLD classification missed an important subgroup of patients with mild COPD challenges any proposed advantage of this classification scheme over existing guidelines from the ATS4 and ERS.5 Only six patients not classified as having COPD by GOLD were missed using the ATS criteria (stage I: FEV1 ⩾50%) and ERS criteria (mild: FEV1 ⩽70% and FEV1/VC >88% for men and >89% for women). Obviously, any arbitrary classification of a continuous variable such as FEV1 and FEV1/FVC results in a borderline group of patients. The GOLD classification, however, provides no guidance as to the further diagnosis of the unclassified subgroup (fig 1). Our results also show that stage I disease (FEV1/FVC <70% and FEV1 >80% predicted) was very rare, constituting only 4–5% of the patients. This indicates that the distribution of the stages, especially stage I, is inhomogeneous.
Despite its retrospective design, this study was strengthened by the fact that lung function data, chest radiographic findings, and the results of a standard clinical examination were available for all patients. It therefore offers the chance to investigate the clinical impact of the GOLD classification, especially in patients with mild COPD.
Our study therefore suggests that GOLD criteria miss an important subgroup of patients with clinically diagnosed COPD, which reduces its usefulness as a clinical tool.

{kind=link}
Plot of % predicted forced expiratory volume in 1 second (FEV1) against the ratio of FEV1 to forced vital capacity (FVC) (%) of the total population (n=1000).