Article Text

Abstract
Background: Inhaled steroids are the most commonly used anti-inflammatory agents for asthma and are increasingly recognised as having a more rapid onset of action than was previously thought. We have investigated the effect of a single dose of inhaled steroid on nocturnal worsening of asthma.
Methods: Ten patients with steroid naive moderate asthma and nocturnal asthma participated in a randomised, double blind, placebo controlled, crossover trial. Participants spent three nights in the laboratory, one week apart. On each night they underwent spirometric testing at 16.00 hours and received one of the three treatments (placebo, beclomethasone 1000 μg, or fluticasone 1000 μg) delivered by metered dose inhaler. Spirometric tests were repeated at 04.00 hours the following morning.
Results: Following placebo administration the mean (SE) overnight fall in FEV1 was 0.65 (0.27) l compared with –0.02 (0.13) l following fluticasone (p=0.019) and 0.23 (0.12) l following beclomethasone (p=0.048 v placebo).
Conclusion: A single dose of inhaled steroid (within the therapeutic range) reduced the fall in FEV1 in patients with nocturnal asthma when administered at 16.00 hours. Nocturnal worsening of asthma is a useful model for testing inhaled steroid activity in a single night study.
- asthma
- circadian rhythm
- inhaled corticosteroids
Statistics from Altmetric.com
Nocturnal worsening of asthma is a common and potentially fatal complication of asthma, and there is accumulating evidence that the inflammatory airway response is also increased at night. Studies on the ability of corticosteroids to block circadian recruitment of inflammatory cells have shown that a single dose of prednisone at 15.00 hours resulted in a significant pancellular reduction in bronchoalveolar lavage cytology at 04.00 hours and a reduction in the overnight fall in forced expiratory volume in 1 second (FEV1). Studies of the pathophysiology of nocturnal asthma therefore support a collaborative cellular mechanism of inflammation that is steroid sensitive but dependent on timing in addition to dosage.1–3
Inhaled steroids are the most commonly used anti-inflammatory agents for asthma and are increasingly recognised as having a more rapid onset of action than was previously thought.4 They have been shown to be of modest benefit in acute asthma5 and, moreover, single doses of inhaled steroids have a protective effect on the bronchial response to exercise6 and to allergen challenge.7
We have investigated the inhibition of nocturnal worsening of asthma by a single high dose of inhaled steroid as a model for detecting the rapid effect of inhaled steroids using a highly active drug (fluticasone 1000 μg), a less potent drug (beclomethasone 1000 μg), and placebo.
METHODS
Subjects
Ten patients aged 19–45 years with a history of asthma were recruited from the general population. All had steroid naive moderate asthma with nocturnal worsening. They met the diagnostic criteria for asthma, with a concentration of <8 mg/ml methacholine provoking a fall in FEV1 of 20% or more (PC20), and/or improvement in FEV1 by inhaled β2 agonist (200 μg albuterol) of >15% in the previous 6 months. Nocturnal asthma was defined as a fall in peak expiratory flow of >15% from bedtime to morning on at least four nights over a seven day period of testing. Patients were atopic with a positive skin prick test. Exclusion criteria were smoking history, other pulmonary disease, use of medication other than bronchodilator, and anti-inflammatory asthma therapy in the 4 weeks before entry into the study. In those with upper respiratory tract infection enrolment to the study was postponed for 6 weeks.
Study design
This was a randomised, double blind, placebo controlled, crossover trial to test the effects of a single 1000 μg dose of inhaled steroids on the nocturnal worsening of asthma. The study medications were fluticasone propionate and beclomethasone dipropionate. Both drugs and placebo were administered with the aid of a spacer and MDI.
The study consisted of three nights in the laboratory. One week was allowed between tests to prevent carryover effects. Patients were asked to withhold all asthma medications for 24 hours before study measurements. On each occasion the patient arrived at the hospital at 15.30 hours and underwent spirometric tests before and after administration of an inhaled β2 agonist (200 μg albuterol). At 16.00 hours one of the three treatments was given. No medications were taken between 16.00 and 04.00 hours, and the night was spent in the hospital. Spirometric tests were repeated at 04.00 hours.
Statistical analysis
The primary outcome was the fall in nocturnal FEV1 which was calculated from the pre-bronchodilator (pre-BD) measurement using the formula:
Fall in FEV1 (l) = pre-BD FEV1 (16.00 hours) – pre-BD FEV1 (04.00 hours)
Repeated measures analysis of variance (ANOVA) was used to compare the effects of the treatments. Data were expressed as mean (SE) values. A p value of <0.05 was considered significant.
RESULTS
The 10 subjects (six men) were of mean (SD) age 34 (3) years with FEV1 74.3 (5.1)% predicted and a bronchodilator response of 22.7 (10.1)%. All were receiving an inhaled β2 agonist; seven were also on a long acting β2 agonist and two were on ipratropium bromide. No subject was taking theophylline.
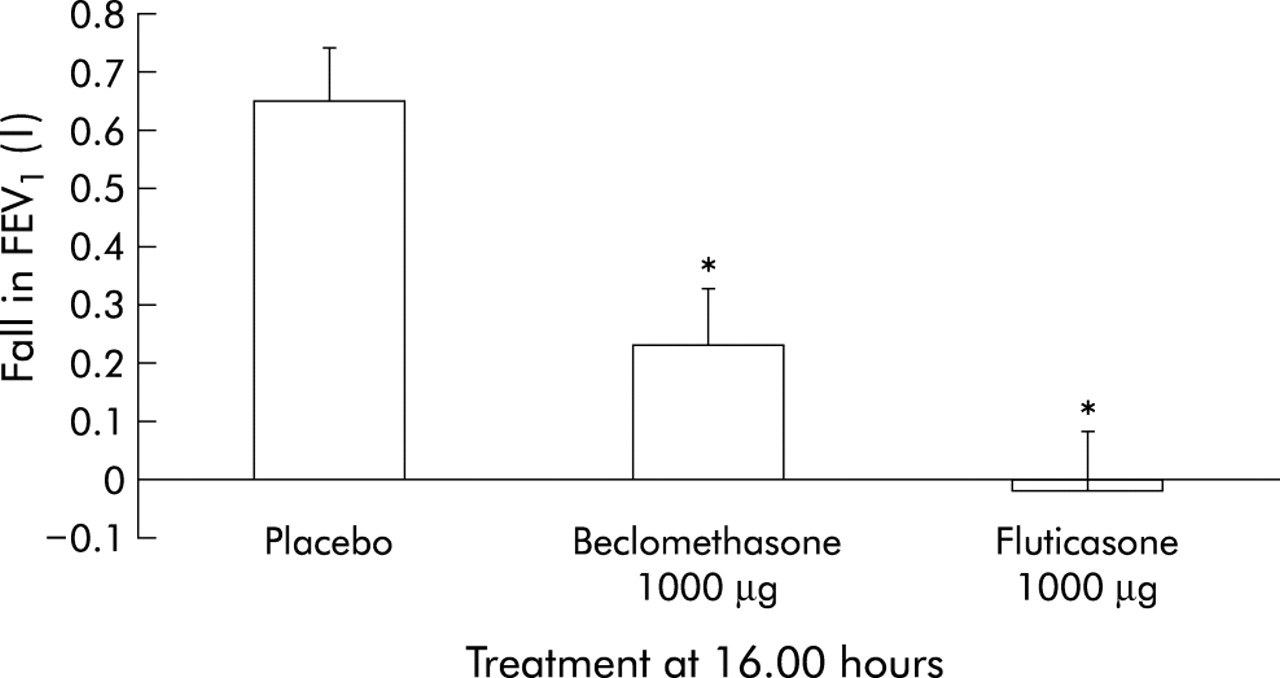
The overnight fall in FEV1 from 16.00 hours to 04.00 hours on each night is shown in fig 1. In the night following placebo administration the mean overnight fall in FEV1 was 0.65 (0.27) l compared with –0.02 (0.13) l following fluticasone (p=0.019 v placebo; 95% CI 0.135 to 1.208) and 0.23 (0.12) l following beclomethasone (p=0.048 v placebo; 95% CI 0.003 to 0.847). The effect of beclomethasone was not significantly different from that of fluticasone (p=0.053; 95% CI –0.005 to 0.498). The negative value for the mean fall in FEV1 on the night of fluticasone treatment indicates an increase in FEV1 from 16.00 hours to 04.00 hours.
{kind=link}
Overnight fall in FEV1 following a single dose of inhaled beclomethasone (1000 μg), fluticasone (1000 μg), or placebo at 16.00 hours. The fall in FEV1 was calculated from the formula: fall in FEV1 (l) = pre-BD FEV1 (16.00 hours) – pre-BD FEV1 (04.00 hours). Negative values indicate a nocturnal increase in FEV1. *p<0.05 v placebo.
DISCUSSION
A single dose of inhaled steroid reduced the fall in FEV1 in patients with nocturnal asthma; both beclomethasone and fluticasone were tested with equivalent doses on a per mg basis. Since the potency of fluticasone is twice that of beclomethasone, we in fact evaluated two unmatched doses, one being half the other.8 Both inhaled steroids were different from placebo. The borderline statistical significance of the difference between the drugs is likely to relate to the small sample size. The study was not designed to distinguish between the two treatments because the medications may differ in their time response effects and the maximum effect of treatment was not investigated. A single dose of inhaled steroid (within therapeutic range) is therefore enough to prevent nocturnal worsening of asthma when administered at 16.00 hours.
An inflammatory events cascade occurs in asthmatic patients with nocturnal asthma which has its onset in the afternoon, making this a predictable phenomenon.3 Nocturnal asthma therefore offers a unique model for investigating the pathophysiology and treatment of asthma. The protocol described here can be used in various studies on inhaled steroids—for example, to test for side effects on the hypothalamic-pituitary-adrenal axis, to determine the site of action, and to compare potency. Moreover, acute effects of inhaled steroids have been shown to correlate with long term effects,9 which strengthens the relevance of this model.
There is evidence that the reported effect of steroids is derived from direct action in the lungs rather than from systemic activity. Currie et al10 showed that fluticasone 1000 μg/day did not cause significant suppression of overnight urinary cortisol. Although the study was not designed as a large therapeutic trial, our data support the acute protective effect of a single dose of inhaled steroid on nocturnal asthma. We conclude that nocturnal worsening of asthma is a useful model for testing the activity of inhaled steroids.
Footnotes
-
Supported by grants 00/04284-3 and 98/10382-6 from the S. Paulo State Government (FAPESP), Brazil.