Article Text

Abstract
Background: Chronic Pseudomonas aeruginosa infection is a major cause of morbidity and mortality for individuals with cystic fibrosis (CF). P aeruginosa cross infection outbreaks have recently been reported at CF holiday camps and specialist centres. The mechanism of cross infection is unknown. A study was performed to look for the presence of epidemic strains of P aeruginosa in the environment of a CF centre during a cross infection outbreak and to examine their potential modes of spread between patients.
Methods: Microbiological sampling of the environment of the CF facility was performed, including room air sampling. Individual P aeruginosa strains were identified by bacterial fingerprinting. The typing patterns were compared with those of epidemic strains responsible for cross infection among the patients.
Results: Epidemic P aeruginosa strains were isolated from room air when patients performed spirometric tests, nebulisation, and airway clearance, but were not present in other areas of the inanimate environment of the CF centre.
Conclusions: Aerosol dissemination may be the most important factor in patient-to-patient spread of epidemic strains of P aeruginosa during recent cross infection outbreaks at adult CF centres.
- cystic fibrosis
- cross infection
- Pseudomonas aeruginosa
Statistics from Altmetric.com
Pseudomonas aeruginosa is an aerobic Gram negative bacterium that is widely distributed in nature. It may be recovered from water, soil, plants and the general environment, including domestic and hospital locations. It is an opportunistic pathogen for humans and causes chronic pulmonary infection in individuals with cystic fibrosis (CF). Once chronic infection is established, it is virtually impossible to eradicate, even with intensive antibiotic therapy. Chronic P aeruginosa infection is associated with an increase in morbidity and mortality for individuals with CF.1–3
Most patients with CF have developed chronic infection with P aeruginosa by adulthood.2 While CF siblings often share the same strain of P aeruginosa, the majority of unrelated patients typically harbour unique isolates.4,5P aeruginosa cross infection outbreaks have recently been documented in CF holiday camps6,7 and CF centres,8,9 including the Manchester Adult CF Centre. We identified two epidemic strains of P aeruginosa associated with a cross infection outbreak at our CF centre—a novel strain9 and another also known to have been responsible for epidemic spread at another UK CF centre.8
The source and mechanism of acquisition of sporadic P aeruginosa infection in individuals with CF is poorly understood. Most patients who successfully eradicate early P aeruginosa infection subsequently become re-infected with different strains.10 Similarly, the mechanism of P aeruginosa cross infection during epidemic spread is unknown. We carried out a study to look for the presence of epidemic strains of P aeruginosa within the environment of our CF centre during a cross infection outbreak and to explore the potential mechanism of spread of P aeruginosa between CF patients.
METHODS
The Manchester Adult CF Centre is housed in a modern purpose built facility. All patients have single bedrooms. All treatment, including nebulisation and airway clearance, is performed in the patient’s own room with the door closed. All nebulisers are single patient use only. At the time of a P aeruginosa cross infection epidemic the following sampling was performed.
Inanimate surfaces
Environmental samples were taken from locations in the CF centre inpatient ward and outpatient facility, including patient rooms and communal areas. Particular attention was paid to moist areas such as washbasins, taps, showers, baths, and soap dispensers, where P aeruginosa is known to proliferate. Door handles and objects in communal areas such as the television remote control unit were also sampled. Samples were taken using sterile moistened PROBACT swabs (Technical Service Consultants Ltd, Heywood, UK) which were smeared directly onto selective Pseudomonas isolation agar (CM559/SR102, Oxoid Ltd, Basingstoke, UK). The same swabs were transferred to sterile selective broth (CM559/SR102, Oxoid Ltd) and subcultured to the selective agar as described.
Spirometers
Patients perform spirometric tests at each outpatient visit and at least twice weekly during inpatient stays using a dry bellows spirometer (Vitalograph, UK). The exterior and interior surfaces of the spirometer tubing, spirometer head, and exterior surface of the spirometer were sampled between patients using the same technique as described above. Disposable mouthpieces with one way valves are used for spirometry. These were not sampled as they are known to become heavily contaminated during spirometric testing (J R W Govan, unpublished data) and therefore are single use and changed by the staff between each patient.
Hand samples
Two methods were used to sample the hands of staff. Method 1: Moistened PROBACT swabs were smeared across the palm and fingers. Swabs were taken from each hand and the presence of P aeruginosa investigated as previously described. Method 2: Hands were also placed into sterile gloves containing 30–40 ml of maximum recovery diluent (Public Health Laboratories, UK) and all parts of the hands, fingers, and nail areas were massaged for 1 minute. Separate samples were taken from both hands. The solution was then streaked onto the selective agar as described above.
Air samples
Air samples (900 l over 5 minutes) were obtained from a surface air system sampler (Cherwell Laboratories, Bichester, UK) using Pseudomonas isolation agar plates. The air sampler was positioned approximately 500–1000 cm from the patient. Sampling was performed immediately after spirometry, nebulisation, and airway clearance. Samples were also taken in the clinical and communal areas occupied by CF patients.
Patients
We continued to survey the P aeruginosa strain types harboured by the patients and including cases of new acquisition of P aeruginosa.
Bacterial isolates
All plates were incubated for a minimum of 72 hours at 37°C. All Gram negative species were further identified using the API 20 NE system (BioMerieux, Basingstoke, UK). Different colonial morphotypes on the same plate were investigated individually. Each isolate was typed using the pyocin typing method for P aeruginosa11 and by genomic fingerprinting by pulsed field gel electrophoresis (PFGE; CHEF-DRII System, BioRad, Hemel Hempstead, UK) following total bacterial DNA digestion with endonuclease XbaI.8 Typing patterns were compared with P aeruginosa isolates cultured from the sputum of CF patients attending the Manchester Adult CF Centre.
RESULTS
Inanimate surfaces
306 specimens were taken from the inanimate environment of the CF ward and outpatient department, excluding spirometers and room air samples. The following organisms were isolated from the ward environment: P aeruginosa (n=5), other Pseudomonas species (n=23), Alcaligenes xylosoxidans (n=11), Enterobacter cloacae (n=3), Morganella morgani (n=1), and Citrobacter freundi (n=1). These organisms were all isolated from damp areas such as washbasins, showers, and baths. None of the environmental P aeruginosa isolates had the same typing profile as the strains of P aeruginosa responsible for the cross infection outbreak.
Spirometer samples
Forty seven samples were taken from the spirometers. P aeruginosa was grown from a sample taken from the exterior surface of the spirometer tubing; this isolate had a different bacterial fingerprint from those of the epidemic P aeruginosa. None of the remaining spirometer samples (n=46) yielded growth of Pseudomonas species.
Hand samples
One hundred and two samples were taken from the hands of staff, 48 using method 1 and 54 using method 2. Pseudomonas putida was grown from the left and right hands of the same member of staff. All other staff hand samples were negative for growth of Pseudomonas species.
Room air samples
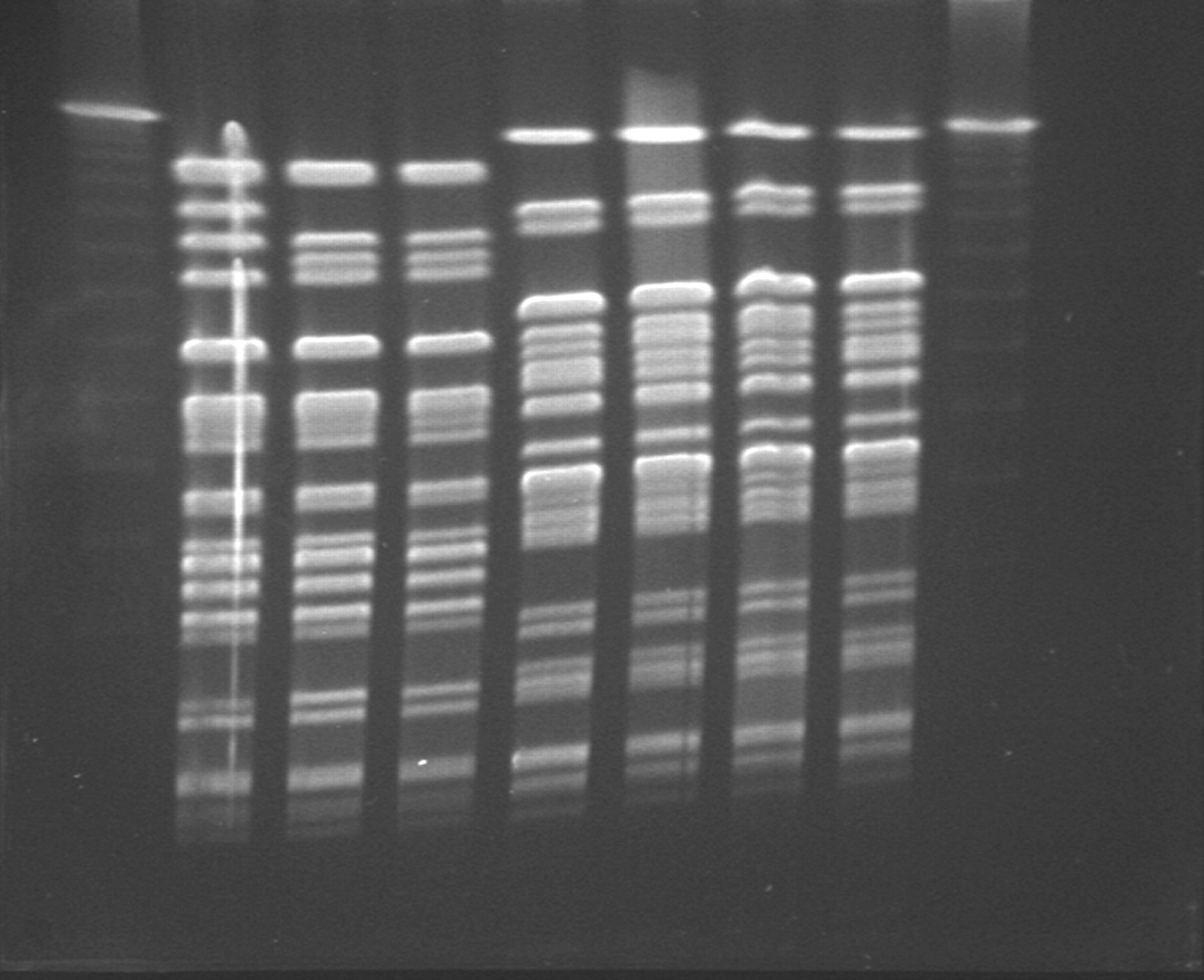
Fifty eight air sampling plates were taken from the CF outpatient (n=22) and inpatient (n=36) facilities. P aeruginosa was isolated from seven of the 58 plates (12.1%), 4/26 immediately after spirometry, 1/9 after air clearance techniques, 1/14 after nebulisation, and 1/9 in a communal waiting room. Typing confirmed the isolates on three plates (one after airway clearance with 1 colony forming unit (CFU) P aeruginosa/m3 air, one after spirometric testing with 1 CFU/m3, one after nebulisation with 2 CFU/m3) as epidemic strains of P aeruginosa (fig 1).
{kind=link}
Genomic typing of P aeruginosa. Chromosomal DNA was digested with endonuclease XbaI and separated by pulsed field gel electrophoresis. Lanes 1 and 9=DNA markers (lambda ladder markers); lanes 3–5=P aeruginosa epidemic strain MA isolated from room air (lane 2) and CF patient sputum (lanes 3–4); lanes 6–8=P aeruginosa epidemic strain AH isolated from room air (lanes 5–6) and CF patient sputum (lanes 7–8).
Patients
At the same time as the environmental sampling was being carried out, a previously “Pseudomonas naïve” CF patient resident on the ward developed infection with a multiresistant strain of P aeruginosa. This patient had been resident on the ward for 4 weeks before P aeruginosa was isolated. All previous sputum cultures had been negative for P aeruginosa. Typing confirmed the isolate to be an epidemic strain (P aeruginosa strain MA). Six other patients who were also resident on the CF ward at the same time are now known to harbour this particular strain of P aeruginosa.
DISCUSSION
Extensive microbiological screening of the inpatient and outpatient environment has identified a number of Pseudomonas and other Gram negative species; however, we failed to find an environmental reservoir or environmental contamination for the epidemic strains of P aeruginosa. Epidemic P aeruginosa could, however, be isolated from room air in the presence of CF patients known to harbour these strains.
At the same time as the environmental sampling was performed, an inpatient acquired infection with an epidemic strain of P aeruginosa. Six other patients resident on the CF ward at the same time are now known to harbour this strain. Patient-to-patient spread is suggested by our failure to culture the epidemic P aeruginosa from the inpatient and outpatient environment at this time. The isolation of epidemic P aeruginosa from room air in the presence of CF patients raises the possibility that there may be airborne spread of epidemic P aeruginosa strains between patients with CF.
The Manchester Adult CF Centre is housed in a modern purpose built facility with single bedrooms for all patients and close attention is paid to infection control techniques. Although we were unable to isolate the epidemic P aeruginosa strains from the environment of the CF facility, we did isolate a number of Gram negative organisms. This level of contamination with P aeruginosa at our CF centre is less than might be expected from previous studies of P aeruginosa contamination in hospital environments,12,13 but is similar to more recent studies.14,15 These differences may reflect changes in cleaning methods and use of modern cleaning agents. In addition to hospitals, such organisms can be found in domestic areas including patients’ homes.16 A previous study has shown that some CF patients harboured P aeruginosa strains that were also present in the hospital environment.17 However, it is difficult to know whether this merely represents secondary contamination of the environment by patients with chronic P aeruginosa infection. This study and most previous studies have shown that CF patients harbour different strains of P aeruginosa from those found in the environment of specialist centres.14,15,18 Importantly, it should be emphasised that regular attendance at CF specialist centres is associated with better health for individuals with CF,19 even at the time of cross infection outbreaks.20
If nebuliser equipment is inadequately cleaned, it can become contaminated with Pseudomonas and other Gram negative species.21,22 Nebulisation equipment should be single patient use and be cleansed and dried thoroughly after each use. On our unit there is no patient sharing of nebuliser equipment, so nebulisers are unlikely to be a source of cross infection. However, sampling of the room air detected P aeruginosa immediately after patients had used their nebuliser. Based on these new data, we recommend that CF patients should not use nebulisers in the same room as other patients with CF. Similarly, when individuals with CF perform airway clearance, other patients should not be present in the same room as epidemic strains of P aeruginosa can be isolated in room air at this time.
There is concern that spirometers are a potential source for cross infection, although this is partly dependent on the type of spirometer used.23 We use dry bellows spirometers with disposable single use mouthpieces fitted with one way valves. We isolated P aeruginosa on one occasion from the exterior surface of the proximal tubing. This was a different strain from that associated with the cross infection outbreak at our centre. An epidemic P aeruginosa strain was isolated from room air after a patient had performed spirometric tests. Although the risk of cross infection from spirometry equipment is minimal provided it is properly cleaned and maintained, spirometry associated airborne spread may present a risk of cross infection to other CF patients if they are present in the same room.
P aeruginosa was not recovered from the hands of staff in the present or previous studies at other CF centres.14,15,24 Neither contamination of the environment nor a breakdown in simple infection control practices has played a role in the P aeruginosa cross infection outbreak at this CF centre. The isolation of epidemic strains of P aeruginosa from room air suggests that aerosol dissemination may be the most important factor in patient-to-patient spread during the recent cross infection outbreaks. Air sampling was done at a distance of 500–1000 cm, which suggests that close contact may be important for cross infection. The duration of airborne contamination following spirometric testing, nebulisation, and airway clearance was not determined in this study but warrants further investigation. The required level of exposure necessary for acquisition is unknown and cannot be identified by ethical experimentation.
In conclusion, in our clinic the reservoir for epidemic multiresistant strains of P aeruginosa is not the inanimate environment of a CF facility but the patients. It seems likely that cross infection by epidemic strains of P aeruginosa between individuals with CF is by airborne dissemination. To control the spread of P aeruginosa in CF centres we recommend that patients should have single rooms to enable spirometric tests, airway clearance techniques, and nebulisation to be performed without risk to other patients, and cohort segregation of patients who harbour epidemic strains of P aeruginosa should be introduced.
REFERENCES
Footnotes
-
Conflict of interest: none.
-
Unfunded study.