Article Text

Statistics from Altmetric.com
Pulmonary manifestations of systemic lupus erythematosus (SLE) include acute lupus pneumonitis, chronic interstitial pneumonitis, diaphragmatic dysfunction, atelectasis, pulmonary vascular disease, upper airway dysfunction, and bronchiolitis obliterans.1 Pneumonia due to infection also develops because infection is a major cause of death of patients with SLE.2,3 Here, we report a patient with SLE who suffered from an ambulatory lung consolidation devoid of pathogens.
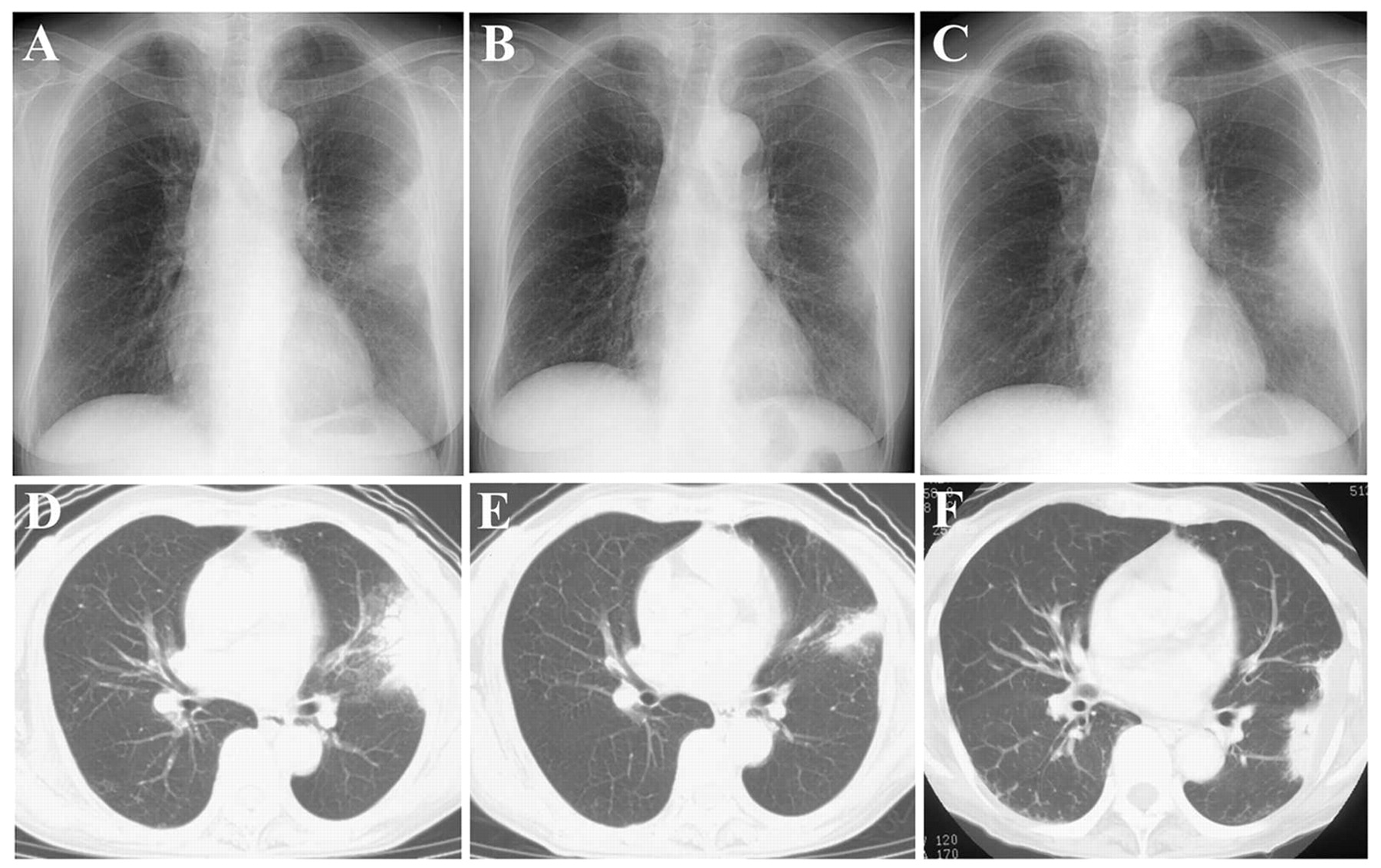
A 61 year old woman with SLE had been treated with 10 mg prednisolone every other day since 1990 without deterioration in the disease. She had complained of cough, non-purulent sputum, and fever once or twice a month since September 1998 which resolved spontaneously within a few days. In October 1999 she was first admitted to hospital with a lung consolidation and an ambient faint infiltrate over the left S4 and S6b on the chest radiograph and computed tomographic (CT) scan (fig 1A, D). She had pancytopenia, increased levels of C reactive protein and LDH, a high titre of anti-double strand DNA antibody, and decreased levels of complement titres. Analysis of bronchoalveolar lavage fluid and histopathological examination of transbronchial lung biopsy specimens showed an increased number of lymphocytes with a low CD4/CD8 ratio. The presence of neither microorganisms nor granulomas was confirmed. She was discharged because the consolidation was reduced (fig 1B, E). In March 2000 she had another bronchoscopic examination because of deterioration of the consolidation (fig 1C, F) but the results were the same as in 1999. For the purpose of further examination we conducted a partial lung resection. The affected lung tissue histopathologically showed a non-specific inflammatory nodule which consisted of lymphocyte dominant inflammatory cell infiltration, lymph follicle formation, fibrosis, fibrin exudation, a thickened alveolar septum, and collapsed alveoli without infectious microorganisms or malignant cells. Removal of the affected lung tissue resulted in improvement in symptoms and abnormal data.
Non-specific inflammatory nodules might occur as a complication of SLE, and a surgical intervention should be considered to diagnose and treat the disease.
{kind=link}
Chest radiograph and CT scan on first admission (A, D), at partial improvement (B, E), and on second admission (C, F) showing deterioration and improvement of a fan shaped patchy shadow on the pleura.