Article Text

Abstract
The case history of a patient admitted to the ICU with interstitial lung disease deteriorating to respiratory failure is presented. Problems in distinguishing between infection and disease progression are discussed and the role of transplantation in ventilated patients is examined.
- critical care
- interstitial lung disease
Statistics from Altmetric.com
CASE REPORT
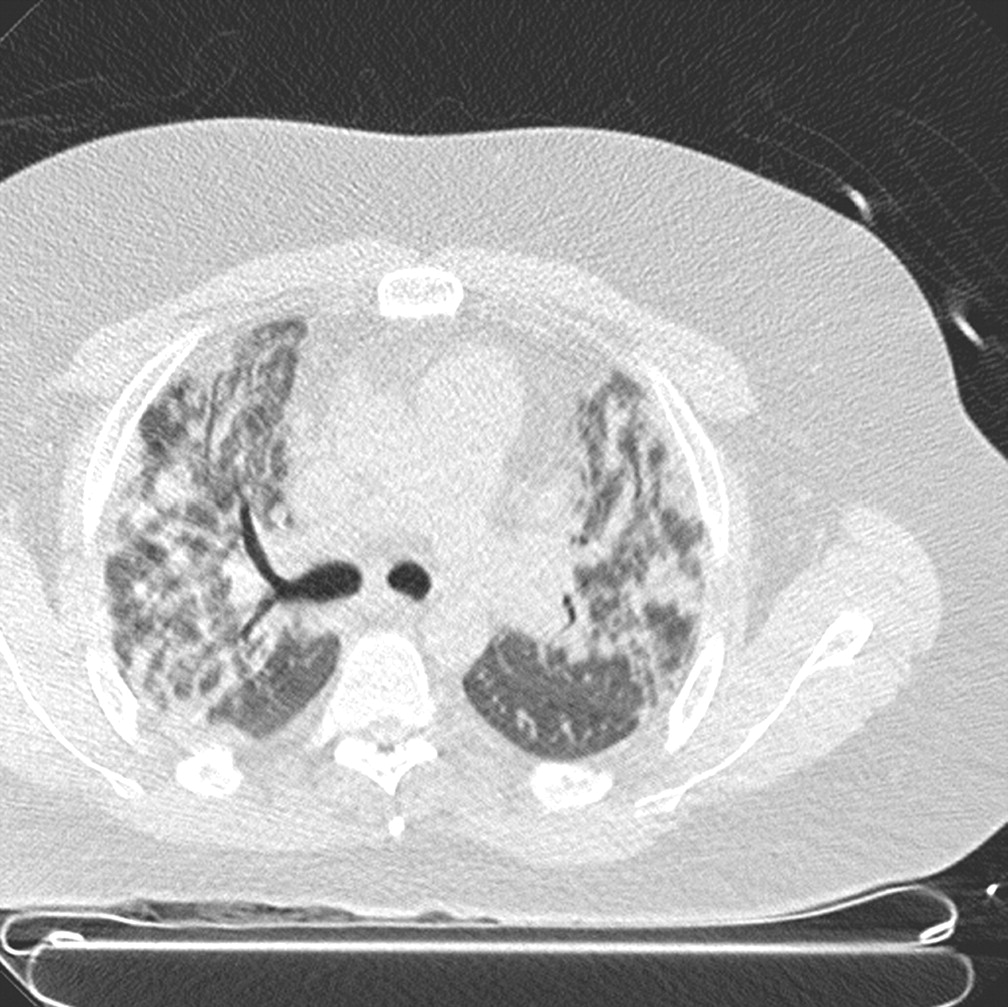
A 31 year old man with a 5 month history of Jo-1 negative dermatomyositis was admitted to the intensive care unit (ICU) with respiratory failure. Five months previously he had developed severe myositis which responded to corticosteroid treatment (prednisolone 1 mg/kg) with symptomatic improvement and a fall in creatine kinase. Six weeks later he developed chest radiographic infiltrates, extensive ground glass opacification on high resolution computed tomographic (HRCT) scanning (fig 1), and hypoxaemic respiratory failure despite maintenance treatment with prednisolone 20 mg daily. He deteriorated despite antimicrobial and increased corticosteroid treatment, requiring mechanical ventilation. A thoracoscopic biopsy specimen taken while on the ventilator disclosed diffuse alveolar damage admixed with organising pneumonia. Intravenous methylprednisolone (750 mg daily for 3 days) allowed weaning from ventilatory support and eventual discharge from hospital on prednisolone (0.5 mg/kg) and azathioprine (200 mg once daily). One month later he was readmitted with increasing dyspnoea and was treated for cytomegalovirus (CMV) pneumonitis diagnosed on the basis of a positive urinary detection of early antigen fluorescent foci (DEAFF) test and bronchoalveolar lavage (BAL) immunofluorescence. After a good initial response, progression of interstitial lung disease became evident radiologically and a single dose of intravenous cyclophosphamide (1.4 g) was administered.

Thin section CT image through the upper lobes showing patchy consolidation, some of which is peribronchial. There is a generalised non-specific increase in attenuation of the lung parenchyma. The consolidation could represent autoimmune organising pneumonia associated with connective tissue disease (in view of its bronchocentric distribution), but an infective cause for the changes (or a coexisting infective component) cannot be excluded. Poor quality images are also a major constraint in the patient with severe dyspnoea at rest. Some of the ground glass attenuation may be technical.
One week later he developed increasing dyspnoea associated with increasing oxygen requirements and a low grade fever, but there were no major changes in chest radiographic abnormalities or inflammatory indices which were only mildly increased. Broad spectrum antibiotic treatment was instituted with cotrimoxazole to cover pneumocystis pneumonia (PCP) and intravenous ganciclovir to cover recrudescence of CMV pneumonitis. However, all cultures, including specific testing for CMV antigen, were negative. Continued deterioration prompted transfer to the ICU 48 hours after admission.
Examination of bronchoalveolar lavage (BAL) samples revealed no evidence of infection. Having failed to identify an infective agent and in the presence of broad spectrum antimicrobial treatment, the patient’s continued decline was treated with three further daily doses of intravenous methylprednisolone and a further dose of intravenous cyclophosphamide. The transplantation investigation protocol was initiated and cyclosporin was added in the hope of decreasing steroid requirements. However, intermittent non-invasive support was increasingly necessary and tracheal intubation and mechanical ventilation were required 7 days after admission to the ICU. Despite vasopressor support, adjustment of antimicrobial treatment (including the empirical addition of liposomal amphotericin), and the use of granulocyte colony stimulating factor to treat pancytopenia, he continued to deteriorate and died 30 days after admission to the ICU. No clear evidence of underlying infection was obtained. Overall, the balance of probability strongly favoured inexorable progression of underlying interstitial lung disease.
MANAGEMENT OF PATIENTS WITH DIFFUSE INTERSTITIAL LUNG DISEASE IN THE ICU
Use of diagnostic techniques
This case illustrates important management difficulties in patients with diffuse interstitial lung disease (DILD) who progress to respiratory failure. Clinically, the differential diagnosis usually consists of deterioration of the underlying disease demanding increased immunosuppression, and infection requiring antimicrobial treatment and a reduction in immunosuppressive treatment. The distinction is important, whatever the likely outcome. Young patients with connective tissue disease may have an excellent long term outcome if they survive an acute episode—be it infective or due to inflammatory DILD—and prolonged aggressive intervention is appropriate. By contrast, major progression of fibrotic disease generally denotes a very poor outcome once mechanical ventilation has been instituted in idiopathic and connective tissue disease alike; prolonged ventilation is inappropriate.
Unfortunately, in most connective tissue diseases and other forms of DILD no serological marker correlates closely with pulmonary disease activity. The distinction between the onset of infection and progression of disease is complicated by the marked similarities in clinical presentation (fever, cough, increased breathlessness, and increased radiographic shadowing). Similarly, laboratory indices of infection (white blood cell count, erythrocyte sedimentation rate, C reactive protein) lack sensitivity or specificity as all may be influenced by the underlying pulmonary inflammation or systemic disease activity. The development of organ dysfunction or nosocomial infection in patients requiring intensive care may add to the diagnostic difficulties. Ideal markers that distinguish between infection and inflammation in patients requiring critical care and in those with autoimmune disease are not yet available for routine clinical use.1,2
Chest radiography is often unhelpful in discriminating between infection and progression of DILD in patients requiring critical care.3 HRCT scanning is central to the diagnosis and management of DILD4 and is a safe means of obtaining clinical and physiological information in critically ill patients.5 It may be diagnostic in advanced DILD,6 obviating the need for invasive investigation. When it is inconclusive diagnostically, CT may define the optimal site for surgical biopsy. However, although fairly accurate in the exclusion of ventilator associated pneumonia in ARDS,7 CT scanning has not been evaluated as a diagnostic test for opportunistic infection in the ventilated patient with DILD. As illustrated by the present case, the interpretation of ground glass opacification on the CT scan is not always straightforward, especially in connective tissue diseases where opportunistic infection may coexist with a number of primary pulmonary disease processes. In this setting, invasive or semi-invasive investigation is often required. In the present case there was a compelling need to define the underlying interstitial lung disease and an immediate diagnostic surgical lung biopsy (SLB) was performed, obviating semi-invasive less definitive procedures. However, in cases in which the underlying diagnosis is known and the problem is one of distinguishing between infection and disease progression, a more calibrated approach is usually appropriate including BAL and transbronchial biopsy (TBB) before SLB (fig 2).

{kind=link}
{kind=link}
An algorithm for the management of patients with diffuse interstitial lung disease (DILD) and acute respiratory failure (ARF). BAL=bronchoalveolar lavage; TBB=transbronchial biopsy; SLB=surgical lung biopsy.
In a case where pulmonary infiltrates are associated with immunosuppressive therapy, BAL makes a crucial contribution to the detection of opportunistic infection.8,9 The spectrum of likely infective organisms depends on a variety of factors including the presence of neutropenia,10 the nature of the underlying disease process and immunosuppressive therapy,11,12 the prior administration of antimicrobial treatment,13 and the timing of the BAL relative to hospital admission and the onset of ventilation.14,15 Bacterial pathogens are isolated most commonly, but staining and cultures should be undertaken to exclude fungal, mycobacterial, and viral infections. In addition, non-infectious causes of diffuse radiographic shadowing including malignancy and alveolar haemorrhage may be identified. New diagnostic techniques applicable to BAL fluid include antigen detection (e.g. Aspergillus spp, Cryptococcus neoformans, Legionella pneumophilia), antibody detection (e.g. antipneumolysin for pneumococcal pneumonia), special methods for culture (BACTEC radiometric culture for mycobacteria), and techniques from molecular biology such as the polymerise chain reaction. However, the appropriate use of new diagnostic tests is often difficult to rationalise; their clinical usefulness is likely to be heavily dependent upon the quality of specimen, BAL technique, and population studied.16 It is advisable for clinicians to seek microbiological advice before performing BAL if the use of novel diagnostic procedures is contemplated.
BAL is generally safe in immunosuppressed patients including those with haematological dysfunction17 and in critically ill patients requiring mechanical ventilation.18,19 However, deterioration in respiratory mechanics and gas exchange is well recognised and may be clinically significant.20,21 Thus, BAL should be performed in the ICU in high risk patients; occasionally it is appropriate to institute mechanical ventilation before BAL is undertaken.
The diagnosis of CMV pneumonitis was unexpected but illustrates the diagnostic usefulness of BAL. CMV pneumonitis is probably rare outside transplant patients and those infected with HIV.22–24 In patients infected with HIV the clinical significance of positive CMV serological testing is uncertain.24 There are few data in other patient groups25 but CMV pneumonitis is associated with a high rate of mortality (>80%) if treatment is delayed.26,27 Serological evidence of previous CMV infection is common in adults, especially after the age of 40. As CMV pneumonitis typically presents with fever, dyspnoea and diffuse infiltrates on the chest radiograph, it may be very difficult to make the crucial distinction between infection and progression of disease.28 Diagnostic viral cytopathic changes in TBB or open lung biopsy specimens tend to occur in advanced infection by which time antiviral treatment may be less efficacious, reinforcing continued interest in non-invasive techniques that promise rapid diagnosis.24,25
The added value of TBB in patients undergoing BAL remains contentious. In a retrospective study of immunosuppressed patients TBB was more sensitive than BAL (77% v 48% in HIV disease, 55% v 20% in haematological malignancy, 57% v 27% in renal transplant recipients) and there were few serious complications.29 In patients with HIV infection it has been argued that a negative BAL result should prompt a repeat BAL with TBB at the most abnormal site; this approach has a diagnostic yield of 90% for nodules or focal infiltrates.30 In a retrospective study of mechanically ventilated patients, TBB was diagnostic in 35% of cases and led to a change in management in 60% of “medical” patients and in 25% of patients following lung transplantation.31 The frequency of pneumothorax was higher (10.4%) than is generally reported in non-ventilated subjects (5%), but there were no serious complications. At subsequent open lung biopsy or necroscopic examination there was a concordance of 85% with TBB findings. The authors argue that TBB is safe in mechanically ventilated patients with undiagnosed pulmonary infiltrates and may obviate the need for SLB.
When BAL and TBB are non-diagnostic, SLB may be warranted. Although widely accepted in DILD in general,4 the role of SLB has been questioned in ventilated subjects because of a perception of higher risk and reduced benefit in critically ill patients. However, it can be argued that diagnostic accuracy in this patient group (which is central to confident management) justifies the increased incidence of perioperative complications. The diagnostic yield of SLB in ventilated patients has varied from 46% to 100%,32–35 but the influence of diagnosis on management is not always easy to quantify. In one study the attainment of a definitive diagnosis resulted in continuation of existing treatment in 33% of patients, increased immunosuppression in 26%, initiation of immunosuppression in 22%, and a change in antimicrobial treatment in 19%.32 In ventilated patients the mortality rate with SLB may be as high as 10% and operative complications, occurring in approximately 20%, may influence survival.32–35 However, mortality after the initial postoperative period is probably largely ascribable to progression of the underlying condition rather than to the surgical procedure, although controlled clinical data are lacking. Factors predicting mortality in ventilated patients with pulmonary infiltrates undergoing SLB have included an immunocompromised status at the onset of respiratory failure or current immunosuppressive treatment, severe hypoxia, multiorgan failure, and older age.33–35
In immunocompromised patients in the ICU, high inpatient and 1 year mortality rates (50% and 90%, respectively) are often cited to suggest that SLB adds little to the management provided that broad spectrum antibiotic cover (including cotrimoxazole to cover PCP) and a trial of corticosteroid treatment are instituted.36,37 However, “patient benefit” is not always synonymous with eventual survival. Inappropriate immunosuppressive therapy may be associated with infective complications. SLB may identify irreversible disease, allowing inappropriate support to be minimised33,34 and withdrawal of care issues to be discussed definitively with the relatives.38,39 Finally, immunocompromised patients with underlying DILD can be viewed as “special cases” with regard to the performance of SLB because of the unique difficulties in distinguishing between infection and progression of the primary disease.
Role of lung transplantation
Mechanical ventilation is widely regarded as a strong relative contraindication to lung transplantation because of the high risk of pneumonia due to airway microbial colonisation, severe muscular deconditioning due to immobility, and other complications such as sepsis, deep venous thrombosis, gastrointestinal haemorrhage, altered gut motility, and nutritional problems.40 The International Society of Heart Lung Transplantation/United Network for Organ Sharing has documented a threefold increase in 1 year mortality in mechanically ventilated patients compared with those who are non-ventilated.41 However, in small populations from selected centres, outcomes have been similar to those in non-ventilated recipients. In a recent report of 21 patients who were transplanted while being mechanically ventilated, six developed acute allograft dysfunction and all died within a year with three not surviving the postoperative period.42 However, there were no postoperative deaths among the remaining 15 patients and their long term survival (40%) did not differ from non-ventilated patients undergoing transplantation. Thus, mechanical ventilation should not be viewed as an absolute contraindication to transplantation. In our patient the factors favouring attempted transplantation included his age, relatively brief history (minimising severe muscular deconditioning), and the lack of evidence of relentless systemic disease activity.
Non-invasive ventilation decreases the need for tracheal intubation and increases the likelihood of successful weaning from mechanical ventilation, both resulting in a lower incidence of nosocomial infection.43 The successful use of non-invasive ventilation as a bridge to transplantation in patients developing respiratory failure has been reported.44,45 In view of the general scarcity of donor organs, the indications for transplantation in patients receiving mechanical ventilation are necessarily imprecise and controversial. Decisions should not be subject to generic guidelines but must be individualised, taking into account such factors as the presence of reversible superimposed processes (with a realistic chance of bridging to surgery with treatment) and the likelihood of expeditious transplantation. Immediate transplantation during an acute episode is seldom practicable.
CONCLUSIONS
In patients with interstitial lung disease who deteriorate to respiratory failure, the distinction between infection and progression of disease is often difficult and sometimes, as in the presented case, the two may coexist. Accurate management requires BAL which is best performed in the ICU in those with borderline respiratory failure; TBB may be a useful adjunct. In selected cases SLB may be invaluable both diagnostically and as an aid to confident management. Although seldom justifiable, transplantation of a ventilated patient is not absolutely contraindicated, especially in young non-deconditioned patients.