Article Text

Abstract
Tumour necrosis factor α (TNFα) antagonists are an established therapeutic option in Crohn's disease and rheumatoid arthritis. In recently published studies these agents have been used with great success, but little is known about any side effects or long term consequences. They increase the frequency of infections with mycobacteria, where TNFα is thought to be an important host defence factor. We describe one patient who was treated with TNFα antagonists and later developed pulmonary granulomas with caseating necrosis without detection of mycobacteria or any other pathogens. Possible mechanisms involved in this newly recognised side effect are discussed.
- pulmonary granulomas
- tumour necrosis factor α antagonist
Statistics from Altmetric.com
Since tumour necrosis factor α (TNFα) plays a significant role in inflammation, genetically engineered antibodies against human TNFα (infliximab) and TNFα receptors (D2E7, etanercept) have been generated.1 Although the use of these agents has been successful in rheumatoid arthritis and Crohn's disease, the long term effects of TNFα blocking agents are not yet known. Recent publications report that treatment with infliximab is associated with an increased frequency of mycobacterial infection. TNFα is thought to be essential for host defence in such infections.2 We describe a patient treated with D2E7 who developed bilateral pulmonary granulomas where no infectious pathogens were detected. Possible mechanisms involved in this newly recognised side effect are discussed.
CASE REPORT
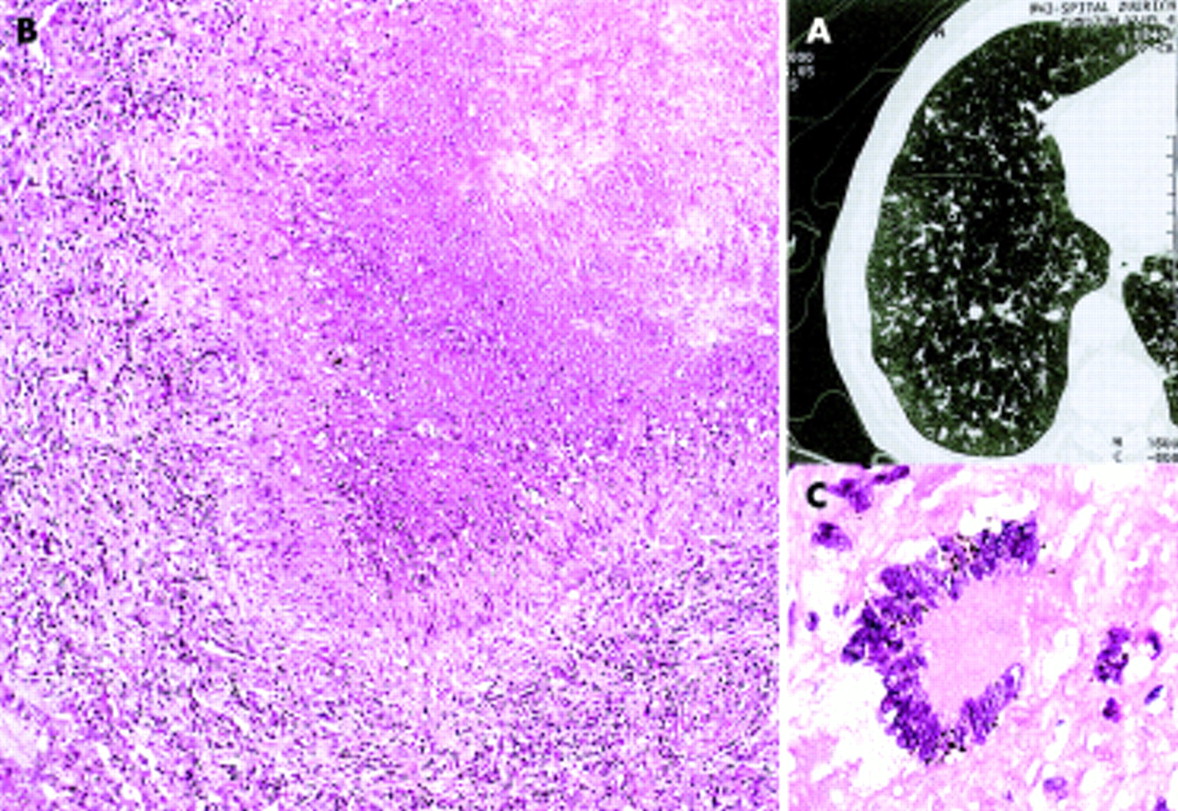
A 73 year old patient had suffered from seropositive rheumatoid arthritis for 15 years and had been treated unsuccessfully with different disease modifying drugs. Twelve months before admission he was treated with D2E7 (Cambridge Antibody Technology, UK/BASF, Germany), 40–80 mg/week, with limited success. After admission to hospital because of cough and weight loss of 4 kg during the previous 6 months, treatment with D2E7 was stopped. The chest radiograph and CT scan showed bilateral nodular infiltrates (fig 1A) that had not been present on a control radiograph taken before treatment with D2E7. A diagnostic bronchoscopic examination with lavage was performed. Cultures for bacteria and mycobacteria remained negative as well as an eubacterial polymerase chain reaction (PCR) and amplified mycobacterial tuberculosis direct test (MTD). The open lung biopsy specimen is shown in fig 1B and C. The lesion was most consistent with tuberculosis, but mycobacterial and eubacterial PCRs were negative as were Ziehl-Neelsen and Gram stains and bacterial and mycobacterial cultures. In spite of the negative bacteriological findings, antituberculous treatment was administered for 6 months. The pulmonary lesions showed no regression with this treatment and remained clearly visible after more than 1 year.

{kind=link}
(A) High resolution computed tomographic scan of the chest showing multiple bilateral mostly centrilobular infiltrates 12 months after treatment with D2E7. (B) Thoracoscopic lung biopsy specimen showing necrotising granulomatous inflammation consisting of necrosis rimmed by histiocytes, epithelioid cells, lymphocytes, and scattered multinucleated giant cells (stain: haematoxylin and eosin, original magnification ×60). (C) Multinucleated giant cell at the border of a necrotising granuloma (stain: haematoxylin and eosin, original magnification ×200).
Similar granulomas developed in a patient with angioimmunoblastic lymphadenopathy treated with etanercept, also without proof of mycobacteria despite the use of sensitive techniques such as eubacterial PCR. However, the concomitant use of chemotherapy made it difficult to establish a clear link between inhibition of TNF and the development of granulomas.
DISCUSSION
Surprisingly few side effects have been described with TNFα antagonists. Among the most common are hypersensitivity reactions and minor upper respiratory tract infections. Increased risks of infection associated with TNFα antagonists have been described for pathogens such as mycobacteria2 and aspergillosis.3 The mycobacterial infections in patients treated with infliximab and the pattern of tuberculous disease were unusual.2 It is known that the hallmark of infections with Mycobacterium tuberculosis and atypical mycobacteria is granuloma formation. Granulomas function both to limit the spread of infection and to provide an environment of activated macrophages which, through autocrine and paracrine stimulation, kill mycobacteria.4 The formation of a protective granuloma involves the orchestrated production of host chemokines and cytokines (e.g. TNFα) which coordinate the recruitment, migration and retention of cells to and within the granuloma.5 It was shown in a recent study that TNF receptor p55 gene deficient (TNFRp55–/–) mice succumb to infection with Mycobacterium avium because of a deranged T cell macrophage interaction which results in fatal granuloma.6 Most patients with tuberculosis are relatively resistant to M tuberculosis and mount an effective cell mediated immune response to it. With new and sophisticated treatments such as TNFα receptor antagonists these cell mediated immune responses are bound to fail. This has become particularly evident in TNF lymphotoxin-α deficient mice where the recruitment and activation of mononuclear cells in response to BCG infection are significantly delayed and reduced, resulting in immature granulomas allowing uncontrolled fatal infection.7
The granuloma formation we observed in our patients after treatment with TNFα antagonists could have been caused by an as yet unidentified infectious agent. Alternatively, it may have resulted from the possible interference in cross talk between T cells and macrophages, even in the absence of an infectious agent. It appears that TNFα antagonists, especially infliximab, could cause reactivation of or increases in susceptibility to a newly acquired infection with mycobacteria. As we could not detect any pathogen in our case, even with very sophisticated methods, we believe that the granulomas in our patient after treatment with D2E7 might represent the effect of the drug interfering with the TNF receptor. This difference may reflect the different ways in which the two agents—infliximab and D2E7—neutralise TNFα. According to the manufacturers, granuloma formation was not observed in preclinical animal studies.
We conclude that atypical granuloma formation may be a long term side effect of this new class of drugs, either due to an immunological mechanism or to an unknown infectious agent undetectable even by very sensitive molecular techniques. This serves as a reminder that our understanding of the risks of inhibiting TNFα is still incomplete.