Article Text

Abstract
Recent developments in the detection of pre-invasive lesions of the large airways by fluorescence bronchoscopy are reviewed and the clinical and biological implications discussed.
- lung cancer
- fluorescence bronchoscopy
Statistics from Altmetric.com
Despite the considerable advances that have occurred in the management of many malignant diseases, the outlook for lung cancer sufferers remains depressingly poor. In the UK the prospects of surviving 5 years persist at only 5%, while the annual death rate exceeds the death rates for cancers of the breast, colon, and prostate combined.1 Although surgery for early stage lung cancers offers a relatively good prospect of cure,2 the majority of patients (80%) already have advanced and inoperable disease when they present to their doctors.3 In an attempt to improve the outlook, considerable interest is now being focused on the development of sensitive methods for detecting clinically silent lung cancers at very much earlier stages when treatment is more likely to be curative.4
Fluorescence bronchoscopy represents one of several initiatives in this field of early lung cancer detection. By exploiting differences in the fluorescence properties of normal and abnormal bronchial mucosa, it has become possible to detect pre-invasive lesions and early micro-invasive carcinomas involving the large airways, which would otherwise have gone undetected by more conventional white light bronchoscopy.5 The ultimate aim is to detect premalignant lesions and then eradicate them before they have become invasive. Although this approach has exciting potential in lung cancer management, it has exposed important gaps in our understanding of the natural history of early lung cancers and poses major clinical dilemmas as to how early lesions should be managed. This review will summarise the recent developments in fluorescence bronchoscopy and consider the important clinical and biological questions which it raises.
CLINICAL RELEVANCE OF PRE-INVASIVE LESIONS
Auerbach first highlighted the possible clinical relevance of pre-invasive bronchial epithelial lesions in a necroscopic study in 1956.6 His group conducted a systematic microscopic examination of serial sections from the tracheobronchial tree and found a relationship between smoking history and the prevalence of carcinoma in situ.6,7 He also noted that pre-invasive lesions of different grades of severity were associated with tumours of squamous histology, and these findings led to the hypothesis that squamous cell carcinoma arose from these pre-invasive changes.8,9
Since pre-invasive lesions are rarely visible macroscopically,10,11 it has been impossible to conduct large confirmatory longitudinal studies. However, indirect evidence has been obtained which is often used to support this hypothesis. Most frequently cited is the work of Saccomanno and colleagues12,13 who investigated uranium workers at high risk for lung cancer by collecting sputum samples at intervals for cytological analysis. They found cells with increasingly malignant features in sequential sputum specimens from miners who subsequently developed lung cancer. Longitudinal studies of squamous cell carcinoma at other sites such as the cervix14 and oral cavity15 have shown that tumours develop from pre-invasive lesions of increasing histological abnormality, contributing to the expectation that those of the lung develop through a similar pathway. Animal studies mimicking human carcinogenesis16,17 have provided further indirect evidence, supporting the hypothesis that squamous cell carcinoma of the lung develops along the pathway: squamous metaplasia → dysplasia → carcinoma in situ → invasive carcinoma.
Very occasionally, carcinoma in situ is visible bronchoscopically in patients without lung cancer, enabling the disease course to be followed by direct observation.18 Satoh et al19 described four visible advanced pre-invasive lesions in three patients that developed into invasive disease. This study provided the first direct proof in patients that squamous cell carcinoma develops from pre-invasive lesions. This conclusion was supported by a larger study with a longer follow up period involving biopsy samples taken from predetermined sites, in which 10 of 22 pre-invasive lesions progressed to invasive carcinoma within 4 years of follow up.20
These studies, although important, involved a small number of patients using an unreliable method of lesion detection, and underlined the need for a more sensitive imaging modality. The advent of fluorescence bronchoscopy has addressed this need and revived interest in the elucidation of the natural history of lung cancer development, as it provides the opportunity to undertake large scale longitudinal studies of the pathogenesis of squamous cell lung cancer.4
DEVELOPMENT OF FLUORESCENCE BRONCHOSCOPY
It has long been known that neoplastic tissues can be distinguished from surrounding normal tissues by their properties of fluorescence when exposed to blue light.21,22 More recently, studies of bronchial mucosa have shown that invasive carcinomas and pre-invasive lesions such as dysplasia and carcinoma in situ exhibit slightly weaker red and much weaker green fluorescence than normal tissues.23 The reasons for this difference are not fully understood, but may be due to differences in epithelial thickness, blood flow and concentrations of fluorophores.24,25 Although these differences in fluorescence are not visible to the naked eye, they may be visualised with the use of computer enhanced imaging and optical filters.
There are presently three commercially available fluorescence bronchoscopy devices. The best known is the Light Induced Fluorescence Endoscopy (LIFE) device, which was designed by Lam et al in Vancouver and which employs a helium-cadmium laser to illuminate the bronchial tree with 442 nm light.26,27 The resulting red and green fluorescence is collected by the imaging bundles of the bronchoscope, and their relative intensities are measured and used to create a computer enhanced pseudo-image in which areas of abnormal fluorescence are displayed on a monitor as brown areas against a normal green background.
Storz and Pentax have independently developed systems which use conventional blue light (440–480 nm) emitted by a xenon arc lamp. The Storz system employs an optical filter incorporated within the eyepiece of the bronchoscope to transmit red and green wavelengths, together with a narrow band within the excitation wavelength which allows visualisation in conditions of low fluorescence.28 Fluorescence images can be viewed directly through the eyepiece or displayed on a monitor, abnormal tissues appearing as red/brown areas against a normal grey/blue background (fig 1). The Pentax system measures the intensity of green fluorescence and displays areas of abnormally low green fluorescence on a monitor as “cold spots” on a green background.29

Bronchoscopic appearance of carcinoma in situ using the Storz system: (A) white light bronchoscopy; (B) autofluorescence mode. The pre-invasive lesion (arrowed), difficult to detect using conventional white light bronchoscopy, is clearly demonstrated using the autofluorescence mode. In addition, the greater extent of the lesion is shown.
Fluorescence bronchoscopy is usually conducted with topical anaesthesia under sedation, as for conventional white light bronchoscopy.30 Standard white light bronchoscopy is normally undertaken before fluorescence bronchoscopy, although the order of the procedures can be varied and does not affect the final results of the investigation.31 Care is taken to avoid unnecessary trauma to the bronchial mucosa as bruising and bleeding undermine the fluorescence images.32 All abnormal areas noted under both white and blue light are biopsied. It has been estimated that the addition of fluorescence imaging to white light bronchoscopy prolongs the bronchoscopic procedure by an average of 12 minutes.18
Several studies have now been published which compare the efficacy of fluorescence bronchoscopy with white light bronchoscopy in the detection of pre-invasive lesions.33–35 In the majority, examination under white light is conducted before blue light; the abnormal areas are carefully documented using each modality and then biopsied at the end of the two examinations. The ability of the two imaging systems to detect pre-invasive lesions is then assessed from the results of histological examinations which are evaluated independently by a pathologist with no knowledge of the bronchoscopist’s findings. The vast majority of studies have concluded that fluorescence bronchoscopy significantly enhances the detection of moderate to severe dysplasia and carcinoma in situ by 1.5–6.3 fold.26,27,30–36 In a recent overview of published studies using the LIFE device, the detection of these lesions was increased by an average of twofold compared with white light bronchoscopy.5
The specificity of fluorescence bronchoscopy has been found to be low, with up to one third of areas of abnormal fluorescence being found to be false positives.36 However, it has been suggested that up to 50% of the biopsies obtained from these areas carry molecular genetic lesions associated with malignancy, despite their normal histological appearance.37 Although it is well documented that histologically normal bronchial mucosa in heavy smokers may harbour molecular genetic damage associated with malignancy,38 a study from the MD Anderson hospital has suggested that fluorescence bronchoscopy is unlikely to have this degree of sensitivity.39 In this study, the results obtained with the LIFE device were compared with those obtained using white light bronchoscopy alone in a matched group of controls. The detection of metaplasia and dysplasia was not significantly increased in the LIFE group, while areas judged to be normal by the LIFE device yielded a similar number of metaplastic and dysplastic lesions as areas judged to be abnormal. However, the apparent discrepancy between the findings of the MD Anderson study and other studies has been attributed to the lower prevalence of severe dysplasia and absence of carcinoma in situ in the study group recruited into the MD Anderson study.40 It therefore seems likely that fluorescence bronchoscopy has sufficient sensitivity to detect moderate to severe dysplasia and carcinoma in situ but is less capable of reliably detecting milder degrees of dysplasia and metaplasia.
CLINICAL DILEMMAS POSED BY THE DETECTION OF SEVERE DYSPLASIA AND CARCINOMA IN SITU
The ability to detect pre-invasive lesions, which are thought to be at high risk of progressing to invasive carcinoma, raises the important clinical question as to how these lesions should be managed. Some groups have opted to manage severe dysplasia and carcinoma in situ with either surgery,41 radical external radiotherapy,42 or endobronchial treatment,43,44 whereas others have argued that such aggressive management is not justified when there is no certainty that some or all of these lesions will progress to invasive malignancy.4
Surgery undoubtedly provides the most effective method for eradicating pre-invasive lesions. However, it carries an appreciable perioperative risk45 and may not be feasible in patients with poor cardiorespiratory fitness and/or multifocal disease. It should also be appreciated that patients with pre-invasive lesions have a substantial risk of developing separate invasive lung cancers with the result that prior surgery may render them unfit for curative treatment.46
Endobronchial treatment is not as effective as surgery in eradicating pre-invasive lesions but has the advantages of preserving lung tissue and carrying less operative risk.47,48 Photodynamic therapy has been used most extensively43,49 and is claimed to eradicate carcinoma in situ in up to 80% of lesions, although it is unlikely to be successful in eliminating large lesions of more than 2 cm in their longest dimension.50 Other groups have managed carcinoma in situ with the NdYAG laser,44 electrocautery,51 cryotherapy,52 and endobronchial radiotherapy.53
The rationale for treating severe dysplasia and carcinoma in situ is that it may prevent the development of an aggressive invasive carcinoma. However, it is impossible to judge whether treatment is effective in this respect when the natural history of pre-invasive lesions is so poorly understood. In addition, this approach may not be practical if the prevalence of these lesions is as high as that suggested by the necroscopic studies of Auerbach—for example, carcinoma in situ was found within the tracheobronchial trees in 75% of heavy smokers.8
An alternative strategy is to maintain careful surveillance with fluorescence bronchoscopy and offer treatment at the earliest signs of progression to invasive disease. Although the clinical distinction between a pre-invasive lesion and an early micro-invasive carcinoma may be difficult with the result that the treatment of an invasive carcinoma may be delayed, this approach has the advantages of avoiding unnecessary treatment in patients who do not progress to invasive disease and of providing important information on the natural history of pre-invasive lesions.
INSIGHTS INTO THE NATURAL HISTORY OF SQUAMOUS CELL CARCINOMA FROM FLUORESCENCE BRONCHOSCOPY
Three studies have now been published reporting on the surveillance of pre-invasive lesions using fluorescence bronchoscopy.54–56 Although they are limited by small numbers of patients and by their relatively short duration of follow up, they show that severe dysplasia and carcinoma in situ have the capacity to progress and regress spontaneously. In the largest of these studies severe dysplasia was more likely to regress (17/22 lesions) than carcinoma in situ (5/32 lesions).54 The mechanisms by which these lesions regress is not understood, although it has been suggested that some are so small that they may actually be removed when biopsied.57 The proportion of carcinoma in situ lesions that progressed to invasive carcinoma in these studies was 1/4,56 5/9,55 and 0/3254; however, these figures are extremely difficult to interpret as high grade pre-invasive lesions were treated if they persisted for 3–6 months.54,55
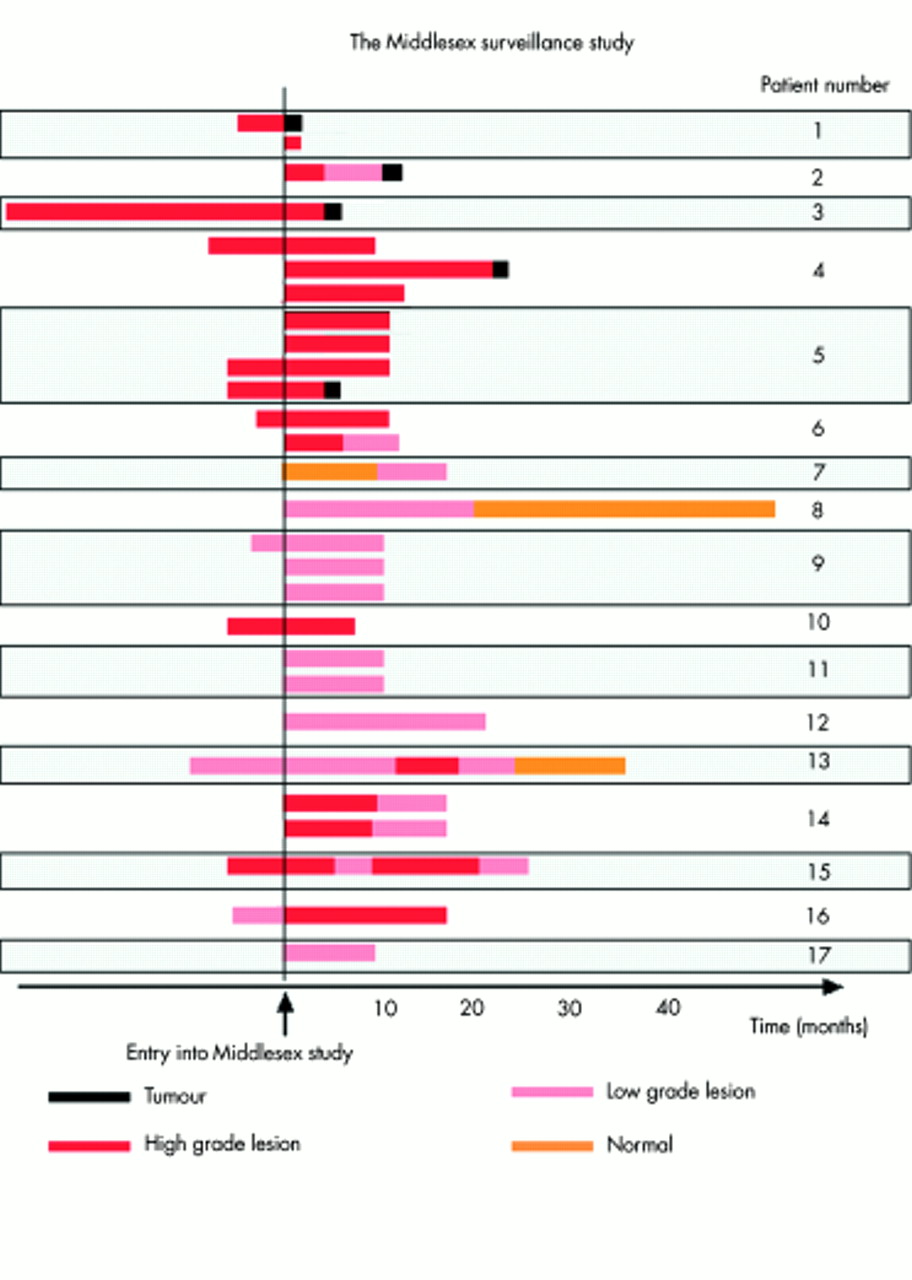
As part of the Middlesex Surveillance Study we perform fluorescence bronchoscopies on patients referred for routine bronchoscopy if they are at high risk of developing lung cancer, and on patients referred from other hospitals who have been found to have pre-invasive lesions. We have identified 17 patients with pre-invasive lesions but no histological or radiological evidence of invasive disease, and have followed them with serial fluorescence bronchoscopies for 6–48 months (fig 2). Five patients have subsequently developed an invasive squamous cell carcinoma, usually from carcinoma in situ in one of their multiple lesions, and have then been promptly treated. Lesions in the other 12 patients have remained pre-invasive for up to 4 years. Our data are consistent with the other published studies54–56 in that they show that the progression of high grade pre-invasive lesions to invasive carcinoma, although frequent, is not inevitable, with the proviso that follow up times have been 24 months or less.

Diagram illustrating the progress of patients with pre-invasive lesions under fluorescence bronchoscopic surveillance at the Middlesex Hospital. Each bar represents the sequence of histological findings of a lesion under follow up in an individual patient. The left side of the diagram shows bronchoscopic and histological results obtained elsewhere before attendance at the Middlesex Hospital surveillance programme.
The fluorescence bronchoscopy studies to date confirm the multifocal nature of pre-invasive lesions first discovered by the work of Auerbach. The question he highlighted in 1957 remains unanswered: “why some carcinomata in situ go on to frank carcinoma and why the majority fail to do so”.58 At that time this question was academic as effective detection and treatment strategies did not exist. The ability to detect pre-invasive lesions offered by fluorescence bronchoscopy and newer endobronchial treatment strategies now requires this question to be answered.
FUTURE DIRECTIONS
Somatic molecular genetic changes underlie and drive tumour progression.59 Concurrent bronchial epithelial lesions of various grades obtained from specimens resected for carcinoma of the bronchus have been examined for genetic changes known to be characteristic of lung tumours.60 Genetic loss on the short arms of chromosomes 3 and 9 have been found in early pre-invasive lesions56,61,62; p53 mutations are typically first seen in dysplasia; 5q deletions are detected in tumours more frequently than carcinoma in situ.56 These observations have been used to propose a pattern of sequential cumulative somatic genetic damage underlying the pathway to development of squamous cell carcinoma.4 Longitudinal studies using fluorescence bronchoscopy will be able to confirm the sequence of genetic changes, particularly for more advanced pre-invasive lesions.
Since somatic genetic changes occur at the pre-invasive stage of the development of lung cancer, they may serve as markers for the early detection of the disease—for instance, through the analysis of material exfoliated from the airways. However, no genetic marker has yet been identified which indicates which patients with pre-invasive disease will progress to tumour. Although p53 mutations are indicative of high risk,20,63 somatic genetic damage to 17p13, the location of the p53 gene, has been found in bronchial epithelium in a substantially higher proportion of smokers (18%) than can be expected to develop lung cancer.38 Thus, neither histological features nor somatic genetic changes found in pre-invasive lesions currently have the power to predict which patients will develop lung cancer.
Our approach to the search for useful markers for early lung cancer detection is to focus on the transition from carcinoma in situ to tumour. The collection and storage of bronchial biopsy specimens from patients undergoing fluorescence bronchoscopy provides a unique opportunity to compare molecular changes in abnormal lesions before and after invasion. In addition, as patients present with multifocal pre-invasive disease, this approach allows us to compare anatomically distinct carcinoma in situ which follow up indicates were either “indolent” or “aggressive”. This will provide insights into the molecular events which control the invasion process in the hope that detectable changes can be developed as markers of early disease. Markers that predict the future behaviour of an individual lesion may be developed from this strategy.
Tissue sections of bronchial biopsy specimens from abnormal lesions are microdissected using laser capture microdissection. This separates the lesion from the underlying stroma and thus provides a virtually pure population of cells (fig 3). Molecular analyses can compare somatic genetic differences or epigenetic changes caused by changes in gene expression. We are currently analysing the former using loss of heterozygosity (LOH) and comparative genome hybridisation (CGH). LOH provides information on specific loci related to lung cancer such as those on 3p, 9p, etc64,65 and CGH produces a “fingerprint” of total genomic damage.66

{kind=link}
{kind=link}
{kind=link}
Photomicrograph of laser capture microscopy dissection of a bronchial lesion (A) before dissection and (B) after dissection. The pre-invasive lesion (A) is identified and removed from the slide using the dissection system. The accuracy of the technique is demonstrated in (B). The lesion is completely excised, providing virtually pure populations of cells for genetic analysis (×4 magnification).
However, our expectation is that the transition from carcinoma in situ to invasive tumour is more likely to be driven by changes in gene expression than by somatic genetic changes. Gene expression studies require RNA as a starting material. Fluorescence bronchoscopy pinpoints endobronchial abnormalities, allowing biopsy specimens to be obtained and immediately frozen making them suitable for RNA isolation and subsequent analysis. Several methods for comparing gene expression repertoires are currently available.67–69 cDNA microarray analysis is particularly attractive because of its proven ability to distinguish tumours of identical histological appearance but different prognosis, treatment response, and behaviour.70–72 When improved technology allows the very small amounts of RNA from biopsies to be used in the analysis, this may be the method of choice for identifying molecules associated with tumour invasion which could lead to markers of early lung cancer detection.
CONCLUSIONS
Fluorescence bronchoscopy is now providing valuable insights into the natural history of pre-invasive lesions and early lung cancers and promises to facilitate the identification of reliable and sensitive markers of invasive carcinoma. If sensitive screening tests can be developed using these markers, fluorescence bronchoscopy will provide an ideal method for locating lesions within the large airways of individuals with positive screening results.
However, it should be appreciated that many important questions still remain unresolved before the clinical value of fluorescence bronchoscopy can be established. Firstly, there is no evidence that fluorescence bronchoscopy has the ability to detect precursor lesions of other lung cancer cell types such as adenocarcinoma and small cell carcinoma, so it is likely that these other cancers will continue to escape detection early in their development. Secondly, it remains to be seen whether pre-invasive lesions, detectable by fluorescence bronchoscopy, are clinically significant and likely to shorten the patient’s life if left untreated, even if they can be shown to be pre-malignant. Similar questions were raised by the NCI lung cancer screening trials in which clinically silent early stage central lung cancers were detected with sputum cytology and then treated but without any apparent reduction in lung cancer mortality.73,74 Finally, the establishment of an early lung cancer detection and treatment programme will inevitably add to the costs and workload of our healthcare services and will be difficult to justify without evidence of a significant reduction in lung cancer mortality. We therefore believe that it will first be necessary to demonstrate the benefits of these approaches in large randomised controlled trials before they can be incorporated into routine clinical practice.
Acknowledgments
We would like to thank Karl Storz for the loan of their D-Light autofluorescence bronchoscope and for their invaluable technical support. We are also indebted to the Ellerman Trust and to the University College London Hospitals Charitable Foundation for financial support towards Dr Anindo Banerjee’s research fellowship. We also thank Nicola Foster for figure 3.