Article Text

Abstract
Background: A study was undertaken to investigate the relationship between inflammatory cells and structural changes in the mucosa of the airways in an epidemiological sample of a group of asymptomatic smokers (smokers who had never sought medical attention for respiratory problems) and in non-smoking subjects.
Methods: Bronchial biopsy specimens were taken from 29 smokers and 16 never smokers and stained with monoclonal antibodies HNL, EPO, AA1, CD68 in order to identify neutrophils, eosinophils, mast cells, and macrophages, respectively. The biopsy specimens were also stained with monoclonal antibodies to the cytokines interleukin (IL)-1β and IL-8. Structural changes were identified by staining the biopsy specimens with antibodies to tenascin and laminin and by evaluating the condition of the epithelial layer.
Results: The numbers of all inflammatory cells and of cytokine staining cells were significantly increased in smokers. The thickness of the tenascin and laminin layers was increased in the smoking group and the integrity of the epithelial layer was significantly reduced. In smokers the epithelial integrity was negatively correlated with the number of eosinophils and macrophages. The thickness of the tenascin and laminin layers was positively correlated with AA1 and EPO positive cells only.
Conclusion: High numbers of inflammatory cells are present in the bronchial mucosa of asymptomatic smokers which have a clear relationship with the impaired epithelial integrity. The increased thickness of the laminin and tenascin layers in these subjects was strongly related to the presence of eosinophils and mast cells, suggesting a role for these cells in tissue remodelling of the airways of smokers.
- smoking
- bronchial biopsies
- inflammatory cells
- basement membrane markers
Statistics from Altmetric.com
Smoking causes an increase in free radicals, reactive nitrogen and oxygen, and cigarette smoking is associated with increases in the incidence and severity of several diseases including cancer and chronic obstructive pulmonary disease (COPD).1 It is also known to be associated with an infiltration of inflammatory cells into the airway mucosa and increased numbers in peripheral blood and bronchoalveolar lavage (BAL) fluid.2–4 Increased infiltration of the airway wall with inflammatory cells such as eosinophils, neutrophils, macrophages and lymphocytes has also been shown,2,5,6 with increased numbers on the epithelial surface, within the epithelium, and in the subepithelial zone.7,8 Similar to asthma,9 chronic bronchitis in smokers is associated with structural changes in the airway mucosa and loss of alveolar attachments.10 Current concepts suggest that inflammatory cells can induce protease-antiprotease and/or oxidant-antioxidant imbalance(s) which may damage the alveolar and interstitial structures of the normal lung. These studies have all investigated the pattern in smokers with chronic bronchitis, and the few studies that have compared the inflammatory responses in non-bronchitic smokers and non-smokers have reported both differences and similarities.3
This study was undertaken to investigate whether asymptomatic smokers—that is, smokers who have never sought medical attention for respiratory problems—and never smokers had differences in the cellular patterns of airway inflammation and whether such differences might be related to structural differences in the airway epithelium. We have quantified cellular involvement and structural changes by immunohistochemical examination of tissue obtained from asymptomatic smokers and compared the findings with those from a group of never smokers.
METHODS
Study population
The subjects were recruited from a population study of men born in Göteborg in 1933.11,12 The sampling procedure has been described in detail in a previous paper.12 All subjects who had sought medical attention for any airways disease (including asthma), congestive heart failure, angina pectoris, or any other severe disease were excluded. The smokers are described as “asymptomatic”. Thirty smokers and 18 never-smokers (all men) agreed to undergo a bronchoscopic examination; 29 smokers (mean pack years 32, range 9–56) and 16 never smokers produced evaluable biopsy specimens from the main carina of the bronchial tree (table 1). Asthma was excluded by questionnaire and/or doctor’s assessment.
Mean (range) characteristics of study patients
In all subjects spirometric tests, single breath nitrogen test, and carbon monoxide transfer factor measurements were performed. Forced expiratory volume in 1 second (FEV1) and vital capacity (VC) were measured on a water sealed regularly calibrated bell spirometer. The slope of the phase III was obtained by the single breath nitrogen method.13 Carbon monoxide transfer factor (Tlco) was assessed by the single breath method using standard equipment (SensorMedics 2200, SensorMedics Co, Bilthoven, The Netherlands). The European Respiratory Society reference values14 were used for spirometric tests and data from Sixt et al15 were used for the single breath nitrogen test. For Tlco and (Tlco/VA) we used the reference values of Salorinne.16
Fibreoptic bronchoscopy and sample collections
Premedication was given with 5 mg diazepam orally and 0.5 ml morphine-scopolamine intramuscularly. In cases of kidney or gall bladder disease, pethidine 75 mg intramuscularly and atropine 0.5 mg subcutaneously were given. Additional diazepam (2.5–5.0 mg) intravenously could also be given. All study subjects were given nebulised terbutaline 0.25 mg/dose 2 × 3 before bronchoscopy. Local anaesthesia was given initially with 1% tetracaine spray in the mouth and laryngeal tract. Additional anaesthesia for the lower respiratory tract was given via the bronchoscope (Olympus). The subjects were examined in the supine position by one experienced bronchoscopist. Oxygen saturation was measured during the bronchoscopy and the subjects were given supplemental oxygen (2–3 l/min) via a nasal catheter.
All bronchoscopic examinations were performed between 08.00 and 10.00 hours. Peripheral bronchial biopsy specimens (3–4 per subject) were taken with an alligator forceps from the main carina between the right and left lung. The biopsy specimens were gently removed from the forceps and immediately placed in a sterile and moistened chamber and transported to the laboratory for further processing; 29 of the 30 biopsies from the smokers and 16 of 18 from the never smokers were evaluable.
Immunohistochemistry
Eosinophils, neutrophils, and mast cells were identified with monoclonal antibodies on frozen sections. To ensure a reliable count of neutrophils, antibodies to human neutrophil lipocalin (HNL) were used for identification. Six different primary monoclonal antibodies to HNL17 were obtained from Pharmacia Diagnostics AB (Uppsala, Sweden) and added as a cocktail at a final concentration of 0.02 mg/ml for each frozen section. The specificity of these antibodies had been tested by ELISA and confirmed using BIAcore (Biosensor AB, Uppsala, Sweden). The monoclonal antibodies against eosinophil peroxidase (EPO) (Pharmacia Diagnostics AB) were used for the identification of eosinophils in a working concentration of 0.02 mg/ml for frozen sections. Antitryptase antibody 1 (AA1; M 7052, Dako, Glostrup, Denmark) for the identification of mast cells was used at a final concentration of 0.00315 mg/ml. For the localisation of macrophages the monoclonal antibody CD68 (M 0814, Dako, Glostrup, Denmark) was used at concentration of 0.0082 mg/ml in frozen sections. Monoclonal antibodies to interleukin (IL)-1β (clone 6E10, Biogenesis, Poole, UK) were used on frozen sections at a concentration of 0.005 mg/ml and the monoclonal mouse anti-IL-8 (Pharmacia Diagnostics AB) was used at a concentration of 0.0025 mg/ml. Monoclonal antibodies to laminin (M 0638) and tenascin (M 0636; Dako) were used on frozen sections at concentrations of 0.0065 mg/ml and 0.047 mg/ml, respectively.
The bronchial biopsy specimens taken from the main carina were frozen immediately in melting propane previously cooled in liquid nitrogen. Frozen biopsy specimens were kept in liquid nitrogen until sectioned. The samples were attached to the specimen holder of a cryostat microtome (Microm, HM 500 M, Heidelberg, Germany) in a drop of OCT compound (Tissue-Tek, Miles, Elkhart, IN, USA) and cut in sections with a thickness of 4 μm. After drying in air at room temperature, the sections were wrapped in aluminium foil and stored at −70°C until they were used for immunohistochemistry.
The sections were thawed and then fixed with undiluted Ortho Permeafix (Ortho Diagnostics, Raritan, USA) for 40 minutes at room temperature before incubation with antibodies to eosinophil, neutrophil, and mast cell markers. In preliminary experiments it was found that fixation and permeabilisation with the commercial reagent Ortho Permeafix produced comparable results in immunocytochemistry to the paraformaldehyde saponin method, but resulted in improved structural preservation. Sections were incubated with monoclonal antibodies at room temperature in a humid chamber for 30 minutes and incubation was terminated by washing in Tris saline buffer (TBS). The antigen-antibody complex was visualised by using APAAP (alkaline phosphatase anti-alkaline phosphatase) kit with fast red substrate (K670, Dako), according to the manufacturers’ instructions. In the negative controls the primary antibody was omitted. After washing, the samples were counterstained with Mayer’s haematoxylin (Merck, Darmstadt, Germany) for 6 minutes. The cover glasses were mounted with Dako fluorescence mounting medium.
Frozen sections were thawed and fixed in acetone at −20°C for 10 minutes before the addition of the monoclonal antibodies to tenascin and laminin. Sections were incubated with monoclonal antibodies at room temperature in a humid chamber for 30 minutes until terminated by washing in TBS. The sections were counterstained and mounted as described above. In the negative control the primary antibody was omitted.
Microscopic evaluation of sections
All the specimens were coded and examined by the microscopist without any knowledge of the current smoking habits of the subjects. Microscopic evaluation of two separate sections was carried out with a Nikon ECLIPSE E800 microscope. Fuji 200 film was used for colour prints. The number of cells in the mucous membrane was counted and the data were converted to an area of 1 mm2 of tissue. The cell counting was performed throughout the whole section. Variation in cell counts and estimation of structural changes between the two microscopic sections varied between 9% and 18% (% coefficient of variation).
The epithelial integrity of the bronchial wall of the subjects from the different groups was assessed by light microscopy using 4 μm thick frozen sections stained with Mayer’s haematoxylin. Epithelial integrity was estimated using a ×10 objective and sidearm light microscopic attachment that allowed the image of the section to be projected onto a computer screen. Measurements were carried out with a Bit Pad Two data tablet (Summagraphics Corp, Seymour, CT, USA) with a Synoptics (Cambridge, UK) synapse framestore and software package after calibration with the aid of a stage micrometer. The total length of the basement membrane and the length of intact epithelium in the section through each biopsy was determined. The total length of intact epithelium was expressed as a percentage of the total length of basement membrane present in each biopsy specimen.
Measurement of the thickness of the tenascin and laminin layers (in μm) was performed in 4 μm thick immunolabelled frozen sections using a ×40 objective and a computerised image analysis system as described above.
Statistical analysis
All statistics were calculated using non-parametric tests. Comparisons between the asymptomatic smokers and never smokers were performed using the Mann-Whitney U test. Spearman’s rank correlation test was used for within group correlations. Multiple linear regression analysis was applied using the backward stepwise selection model to select out the factors that independently and significantly explained loss in epithelial integrity and the increased thickness in laminin and tenascin layers. All calculations were performed on the PC using the statistical package Statistica for Windows Version 5.5 from Statsoft (USA).
RESULTS
There were statistically significant differences between asymptomatic smokers and never smokers in terms of lung function (table 1).
Inflammatory and cytokine positive cells
Asymptomatic smokers had a higher number of neutrophils (HNL positive cells), eosinophils (EPO positive cells), mast cells (AA1 positive cells), and macrophages (CD68 positive cells) in the mucosa than never smokers (figs 1 and 2).

Comparison of the number of inflammatory cells (A) HNL positive cells, (B) EPO positive cells, (C) AA1 positive cells, (D) CD68 positive cells, (E) IL-1β positive cells, and (F) IL-8 positive cells per mm2 in bronchial biopsy specimens from asymptomatic smokers and never smokers evaluated by immunohistochemical methods.

Cryostat sections of bronchial biopsy specimens for HNL in (A) asymptomatic smokers and (B) never smokers (×320). Many HNL positive cells are present in the tissue of asymptomatic smokers while only a few are present in the tissues of never smokers. Immunohistochemical staining for EPO in (C) asymptomatic smokers (×160) and (D) never smokers (×320). Many EPO positive cells are present in the tissue of the asymptomatic smokers while there are only a few in the tissues of never smokers. Stain: Mayer’s haematoxylin.
The number of cells expressing cytokines in the two patient groups is shown in fig 1. Asymptomatic smokers had significantly more cells expressing IL-1β and IL-8 than never smokers. In asymptomatic smokers IL-1β was predominantly expressed in macrophages but was also present in some other cells. IL-8 was expressed predominantly in neutrophils, but also in bronchial epithelial cells (fig 1E, F).
In asymptomatic smokers all inflammatory cells were positively correlated with each other. IL-1β positive cells correlated with the numbers of neutrophils, eosinophils, and macrophages, and IL-8 positive cells correlated with the numbers of neutrophils and eosinophils (table 2). The cytokine positive cells were also significantly correlated (r=0.77, p<0.001).
Correlations between different inflammatory cells in asymptomatic smokers
Epithelial damage and structural changes
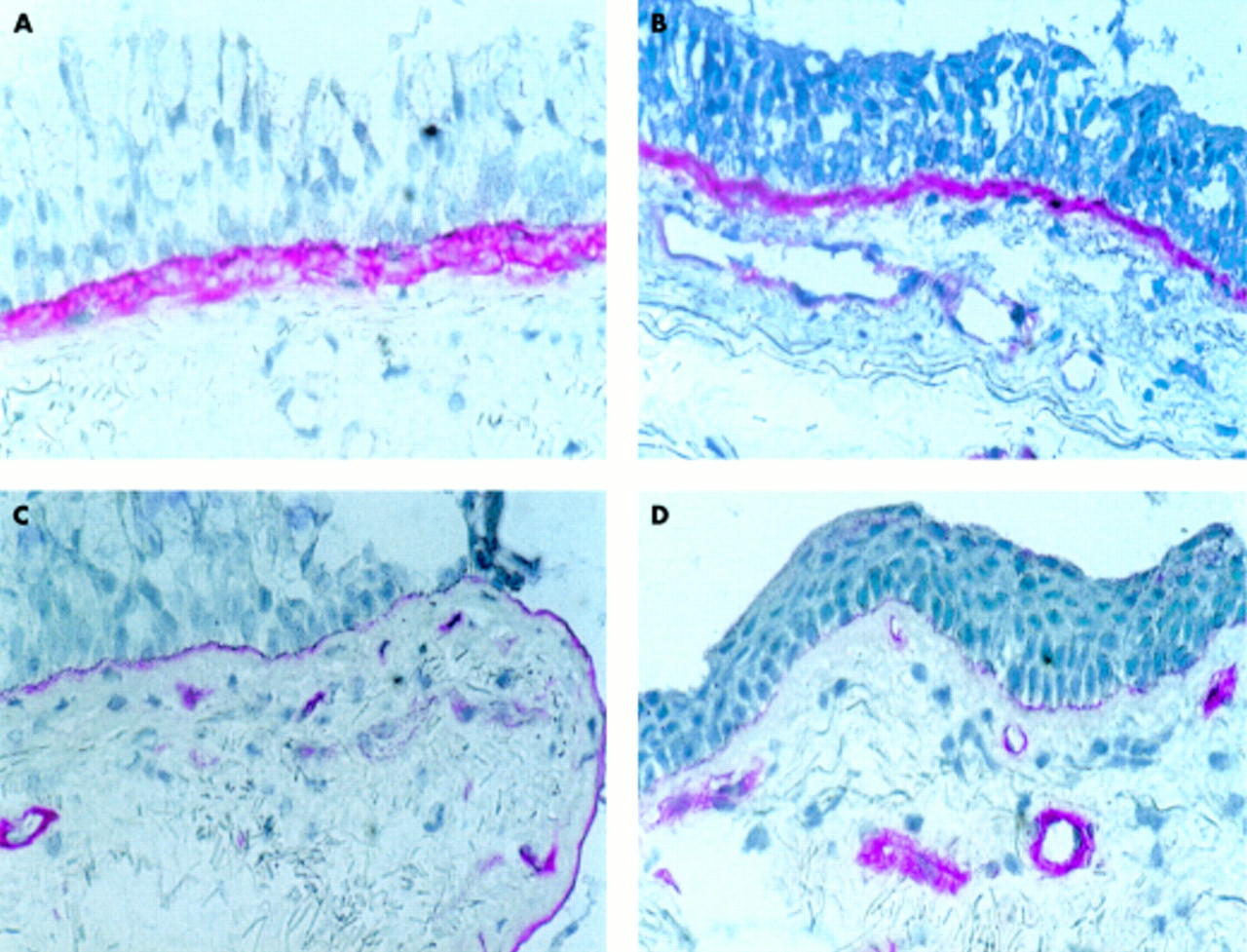
The epithelial integrity was lower in asymptomatic smokers than in never smokers (fig 3 and fig 4C, D). In the damaged area the cylindrical ciliated epithelial cells were absent while the layer of cuboidal basal cells was often intact. Eosinophils were frequently found in the area of epithelial damage (fig 2A). The tenascin positive and laminin positive layers in asymptomatic smokers were thicker than in never smokers (fig 4A–D, fig 5A, B).

Comparison of epithelial integrity (length of basal membrane with intact epithelium divided by the total length of the membrane) in asymptomatic smokers and never smokers.

Cryostat sections of bronchial biopsy specimens in asymptomatic smokers and never smokers. Light microscopic examination of the thickness of the tenascin layer in (A) asymptomatic smokers and (B) never smokers, and of the thickness of the laminin layer in (C) asymptomatic smokers and (D) never smokers. Stain: Mayer’s haematoxylin. Original magnification ×320.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of structural changes in the airways of smokers and never smokers as indicated by the thickness of (A) the tenascin layer and (B) the laminin layer in the subepithelium.
Correlations between the numbers of inflammatory cells and structural changes in the epithelium
A significant negative correlation was found in the asymptomatic smokers between epithelial integrity and eosinophil, mast cell, and macrophage numbers. There was no correlation between epithelial integrity and IL-1β or IL-8 positive cells (table 3). Linear multiple regression analysis including data on all four cells and the two types of cytokine staining cells as independent variables indicated that the numbers of eosinophils and macrophages together independently and significantly contributed to the loss in epithelial integrity (r2=0.47, p=0.00026).
Correlation coefficient (r value) between inflammatory cell numbers and structural changes
In the asymptomatic smokers a positive correlation was found between the thickness of the tenascin layer and the numbers of eosinophils and mast cells. Linear multiple regression analysis including data on all four cells and the two types of cytokine staining cells as independent variables indicated that the numbers of mast cells together with IL-1β staining cells independently and significantly contributed to the thickness of the tenascin layer (r2=0.38, p=0.0064). In the asymptomatic smokers a significant positive correlation was found between the thickness of the laminin layer and eosinophils and mast cell numbers (table 3). Linear multiple regression analysis including data on all four cells and the two types of cytokine staining cells as independent variables indicated that the numbers of eosinophils together with IL-1β staining cells independently and significantly contributed to the thickness of the laminin layer (r2=0.38, p=0.0018).
In smokers, epithelial integrity was significantly and negatively correlated with the thickness of both the laminin and tenascin layers (r=0.56, p=0.003 and r=0.77, respectively, p=0.001). In never smokers IL-8 positive cells were significantly correlated with the thickness of both the tenascin and laminin layers (table 3).
DISCUSSION
The main findings of this study are the differences in inflammatory and structural characteristics of asymptomatic smokers and never smokers. The cellular pattern of inflammation in the central airways in asymptomatic smokers was characterised by increased numbers of neutrophils, eosinophils, mast cells, macrophages, and cytokines. Epithelial damage was mainly found in asymptomatic smokers. Furthermore, we found that the tenascin and laminin containing layers in the airways were thicker in asymptomatic smokers than in never smokers.
One clear distinction between asymptomatic smokers and never smokers in the present study was the finding of increased numbers of neutrophils in the asymptomatic smokers. The increased number of neutrophils in asymptomatic smokers is in agreement with previous studies on BAL, in which counts of neutrophils were significantly higher in smokers than in non-smokers.18 The failure of other studies3 to corroborate these findings may have methodological reasons; we fixed our biopsy specimens with Permeafix which has been shown in other studies to be a superior fixation agent for most cellular antigens.9 Some other studies have not found differences in the numbers of neutrophils between smokers with bronchitis and healthy non-smokers.2,19 The consequence of the increased presence of neutrophils in the lungs of asymptomatic smokers is uncertain, since none of our calculations seemed to relate neutrophils to the structural alterations found in the mucosa of the central airway of the lungs in these subjects, despite the fact that neutrophils are highly destructive cells containing an abundance of cytotoxic and proteolytic molecules. Indeed, the activity of the neutrophil has been implicated in the development of advanced smoking related diseases such as chronic bronchitis and emphysema and neutrophil granule proteins were found in BAL fluid from subjects with subclinical emphysema.10,20,21
The number of eosinophils (EPO positive cells) was higher in the asymptomatic smokers than in the never smokers. This is in agreement with the findings of Lams and co-workers who reported an increase in eosinophils in the subepithelium in asymptomatic smokers.8 Our results are also in accordance with results from an epidemiological study in which asymptomatic smokers were found to have higher levels of serum eosinophil cationic protein (ECP) and higher numbers of blood and BAL eosinophils than never smokers.22 Increased numbers of eosinophils in bronchial biopsy specimens, sputum, and BAL fluid of smoking patients with chronic bronchitis, with or without obstruction, have been found in most studies, but not all,2 and have been related to increased sensitivity to corticosteroid treatment.23,24
Overall, the number of mast cells was increased in asymptomatic smokers. Increases in epithelial mast cells, but not in the lamina propria, were shown in a previous report on patients with chronic bronchitis25 but were not found by others.2 The number of epithelial mast cells was shown to be increased in the bronchioli of smokers with airflow limitation, suggesting a role in the development of COPD.5 Whether differences between our findings and those of others are due to differences in fixation procedures as discussed above is at present not known. The number of macrophages was increased in asymptomatic smokers. Our findings are not in agreement with some previous reports,26 although large numbers are regularly found in BAL fluid of smokers even without symptoms.12,22
We found a more or less parallel increase in the numbers of all four inflammatory cells studied in the bronchial mucosa of asymptomatic smokers. As mentioned above, these findings were supported by some previous studies but were in contrast to others in which no increments in inflammatory cells were observed. The reasons for these seemingly discrepant results are not clear, but could be due to differences in patient selection and the definition of non-smokers. In our study we have included only never smokers in the group of non-smokers. Assuming that they have not been exposed to excessive air pollution and/or passive smoking, our never smoking group of subjects should be as free from pollution as it is possible to be in a westernised society. Many previous studies have also included only a limited number of non-smoking controls and our study seems to be one of the most extensive in this regard. It is therefore our strong belief that our results, together with other similar results, correctly reflect the consequences of smoke exposure to the lung mucosa, and that smoking induces a general inflammatory response seen even in seemingly healthy and asymptomatic smokers.
In a previous report we found IL-1β and IL-8 levels to be significantly raised in the BAL fluid of asymptomatic smokers.12 IL-8 was closely related to neutrophil markers, which is also seen in this study. This may be explained by the fact that most IL-8 staining cells were neutrophils, although other cells such as epithelial cells also stained for IL-8. These results are in accordance with our findings in atopic and non-atopic asthmatics.9 Thus, the major source of the neutrophil chemoattractant IL-8 in the lung may actually be the neutrophil itself. Others have shown that the mRNA for IL-8, as well as for ICAM-1, is turned on in lung cells of smokers and that these alterations may be involved in the attraction of neutrophils to the lungs of smokers.27 In our previous study the concentrations of soluble IL-1β were used to reflect macrophage activity.12 This seems to be partly true, since macrophages in general stained for IL-1β. It is, however, also clear from this study that IL-1β originates from several other sources as well, in particular monocytes and T lymphocytes. IL-1β may have a role in the activation of B cells and in the generation of B cell surface adhesion molecules28 but, together with other cytokines such as tumour necrosis factor α (TNFα) and interferon γ (IFNγ), it has also been shown to cause damage to bronchial epithelial cells cultivated in vitro.29 This observation could have some relevance to our findings of a reduction in epithelial integrity in asymptomatic smokers.
Epithelial shedding and loss of integrity are recognised features in the biopsy specimens of asthmatic patients.9 The degree of epithelial damage was higher in asymptomatic smokers than in never smokers. The thickness of the tenascin and laminin positive layers was also increased in smokers. Previous studies have shown increased thickness in the layers expressing tenascin9,30 and laminin9,31 in patients with seasonal and occupational asthma, but to our knowledge no previous reports have investigated the thickness of the tenascin and laminin layers in smokers.
Epithelial damage by activated eosinophils has been proposed as one of the major pathophysiological mechanisms in asthma.32,33 Activated eosinophils release cationic granule proteins which are highly toxic to the respiratory epithelium.34 When MBP or ECP were applied in vitro to human epithelial cells, they were found to cause direct damage to the cells in a dose and time dependent manner.35,36 In the present study we found a correlation between the number of eosinophils and epithelial integrity in the asymptomatic smokers, which supports this notion. We also regularly found accumulation of eosinophils in areas of epithelial damage. It should, however, be emphasised that the extent of epithelial damage was less than that seen in patients with allergic asthma.9
The increased thickness of the tenascin layer was correlated with the numbers of both mast cells and eosinophils. However, in the multivariate analysis mast cells seemed to be the major independent factor together with IL-1β, suggesting a role for these components in this process. Similar findings were also obtained in patients with allergic asthma, and the activities of mast cells have been implicated in the development of fibrotic disorders.37 IL-1β has been shown to induce tenascin production by fibroblasts.38 In a previous study snuff and smoking were shown to cause an increase in tenascin expression in oral mucosa,39 results which may have a bearing on our findings. The thickness of the laminin layer was also correlated in univariate analysis with eosinophils and mast cells but, in contrast to the data on tenascin, multivariate analysis indicated that the eosinophils were the major independent factor with IL-1β as one minor but independently contributing factor. Many different cell types may produce laminins, but the type studied in this report (laminin 1) is predominantly produced by epithelial cells in the lungs. Our findings could indicate that tenascin and laminin production are governed by partly different mechanisms, with the mast cell involved above all in fibroblast production of tenascin and the eosinophil predominantly involved in epithelial production of laminin. It is possible, however, that mast cells and eosinophils cooperate in these processes, as eosinophil products such as ECP and transforming growth factors have been shown to interfere with fibroblast growth and the production of matrix proteins.40,41 The strong correlations between epithelial integrity on the one hand and laminin and tenascin on the other suggest that anchoring of epithelial cells may be impaired, possibly as a result of inadequate production of adhesion molecules.
In conclusion, the cellular patterns for eosinophils, neutrophils, mast cells, macrophages, and cytokines differed between asymptomatic smokers and never smokers. In asymptomatic smokers the airway inflammation was characterised by increased numbers of neutrophils, eosinophils, mast cells, macrophages, and cytokines in both the surface epithelium and in the subepithelium. There were also distinct structural alterations in the airway mucosa in asymptomatic smokers that were not found in never smokers. The increased thickness of the laminin and tenascin layers in these subjects was strongly related to the presence of eosinophils and mast cells, suggesting a role for these cells in the tissue remodelling of the airways of smokers.
Acknowledgments
This study was supported by grants from the Care and Allergy Foundation (Vårdalstiftelsen), the Swedish Heart and Lung Foundation, the Swedish Allergy and Asthma Foundation, and the Swedish Medical Research Council.
REFERENCES
Linked Articles
- Airwaves